Article Text

Abstract
Introduction COVID-19 sequelae are numerous and multisystemic, and how to evaluate those symptomatic patients is a timely issue. Klok et al proposed the Post-COVID-19 Functional Status (PCFS) Scale as an easy tool to evaluate limitations related to persistent symptoms. Our aim was to analyse PCFS Scale ability to detect functional limitations and its correlation with quality of life in a cohort of patients, 2–9 months after hospitalisation for COVID-19 hypoxemic pneumonia.
Methods PCFS Scale was evaluated in 121 patients together with quality of life and dyspnoea questionnaires, pulmonary function tests and CT scans.
Results We observed a high correlation with multiple questionnaires (Short Form-36, Hospital Anxiety and Depression Scale, modified Medical Research Council, end Borg Six-Minute Walk Test), making the PCFS Scale a quick and global tool to evaluate functional limitations related to various persistent symptoms following COVID-19 pneumonia.
Discussion The PCFS Scale seems to be a suitable instrument to screen for patients who will require careful follow-up after COVID-19 hypoxemic pneumonia even in the absence of pulmonary sequelae.
- COVID-19
- viral infection
- respiratory infection
- pneumonia
Data availability statement
Data are available upon reasonable request. The data are deidentified participant data, they are available from MK and data reuse will be allowed limited to academic research and to non-commercial use only, after evaluation of research project.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
There is a great number of patients with a wide range of clinical symptoms following COVID-19 pneumonia.
A simple and reproducible questionnaire could help the clinician to identify the ones that need intervention.
What this study adds
The Post-COVID-19 Functional Status (PCFS) Scale is a global instrument that correlates with quality of life, dyspnoea and mental health.
How this study might affect research, practice or policy
This study showed that the PCFS Scale is a suitable scale to detect functional limitations related to the various persistent symptoms following COVID-19 pneumonia.
Introduction
The consequences that result from the COVID-19 pandemic are numerous. A few studies have already highlighted both high frequency and heterogeneity of post COVID-19 symptoms.1 2 Indeed, many symptoms have been described up to 6 months after the acute phase of COVID-19,3 including asthenia, muscle weakness, anxiety, depression, sleep disorder and respiratory manifestations. If most of these symptoms are reversible,4 some last over time and significantly alter daily life.5 If not taken seriously, they could evolve towards a chronic disease with major public health and economic consequences.
Because of the vast number of patients and range of clinical symptoms, a simple and reproducible questionnaire is crucial to identify patients with functional limitations. A year ago, the ‘Post-COVID-19 Functional Status (PCFS) Scale’ was proposed by Klok et al as an easy tool to identify people with incomplete recovery.6 It focuses on daily-life limitations connected to persistent symptoms. Machado et al already described a relationship between the PCFS Scale and two scores that assess health-related quality of life (EuroQoL-5D-5L), daily life and work impairment.7 However, it was based on a population of symptomatic patients who volunteered, of whom only 5% had been hospitalised during the acute phase of COVID-19. In the present study, we assessed the PCFS Scale in a cohort of patients recovering from hypoxemic COVID-19 pneumonia and analysed its ability to detect functional limitations related to remaining symptoms and its correlation with quality of life using Short Form-36 (SF-36) and mental health and dyspnoea questionnaires.
Methods
Study design and inclusion criteria
This observational, monocentric prospective study was conducted at Nantes University Hospital, France, between June 2020 and March 2021. Patients aged between 18 and 75 years admitted with hypoxemic COVID-19 pneumonia, confirmed by reverse transcription-PCR or chest CT scan, were routinely proposed a follow-up with a pulmonologist after discharge.
Construct validity and study objectives
The PCFS was translated into French by the authors (online supplemental figure 1) and then back-translated into English by a native English speaker. Multiple self-administered questionnaires were fulfilled: French translation of the PCFS Scale, the modified Medical Research Council (mMRC) Scale, the Multidimensional Dyspnea Profile (MDP), the SF-36 questionnaire and the Hospital Anxiety and Depression Scale (HAD A and D). Patients also underwent physical examination and pulmonary functional tests. When possible, a chest CT scan and a Six-Minute Walk Test (6MWT) were performed (see online supplemental methods).
Supplemental material
The main study aim was to evaluate the validity of the French translation of the PCFS Scale to detect limitations secondary to the wide spectrum of symptoms remaining after COVID-19 pneumonia. To achieve that, we analysed its correlation with questionnaires exploring dyspnoea, quality of life and psychiatric state. The secondary aim was to verify whether the PCFS Scale could be suited to detect pulmonary sequelae. For this purpose, we analysed PCFS Scale correlation with persistent chest CT scan abnormalities, carbon monoxide transfer factor (TLco) and 6MWT. Three groups of patients were identified according to their follow-up status: (1) ‘no sequelae’ stood for no persistent dyspnoea, no chest CT scan findings and no altered TLco, (2) ‘isolated dyspnoea’ stood for patients with persistent dyspnoea with normal TLco and chest CT scan and (3) ‘pulmonary sequelae’ for chest CT scan and/or TLco abnormalities.
Results
A total of 121 patients were enrolled in the study. At a median time of 125 days (59–284) after hospital admission for severe COVID-19 pneumonia (online supplemental figure 2), only 44 patients (36.4%) had a restored pre-COVID-19 condition (online supplemental table 1). Overall, 106 patients (88%) had a PCFS Scale Score at 0, 1 or 2, indicating no symptom (0) or symptom persistence without (1) or with minor (2) limitation (table 1). Overall, 92% of patients scored the PCFS Scale easy or very easy to fill in (online supplemental table 2).
Patient characteristics according to their PCFS Scale Score
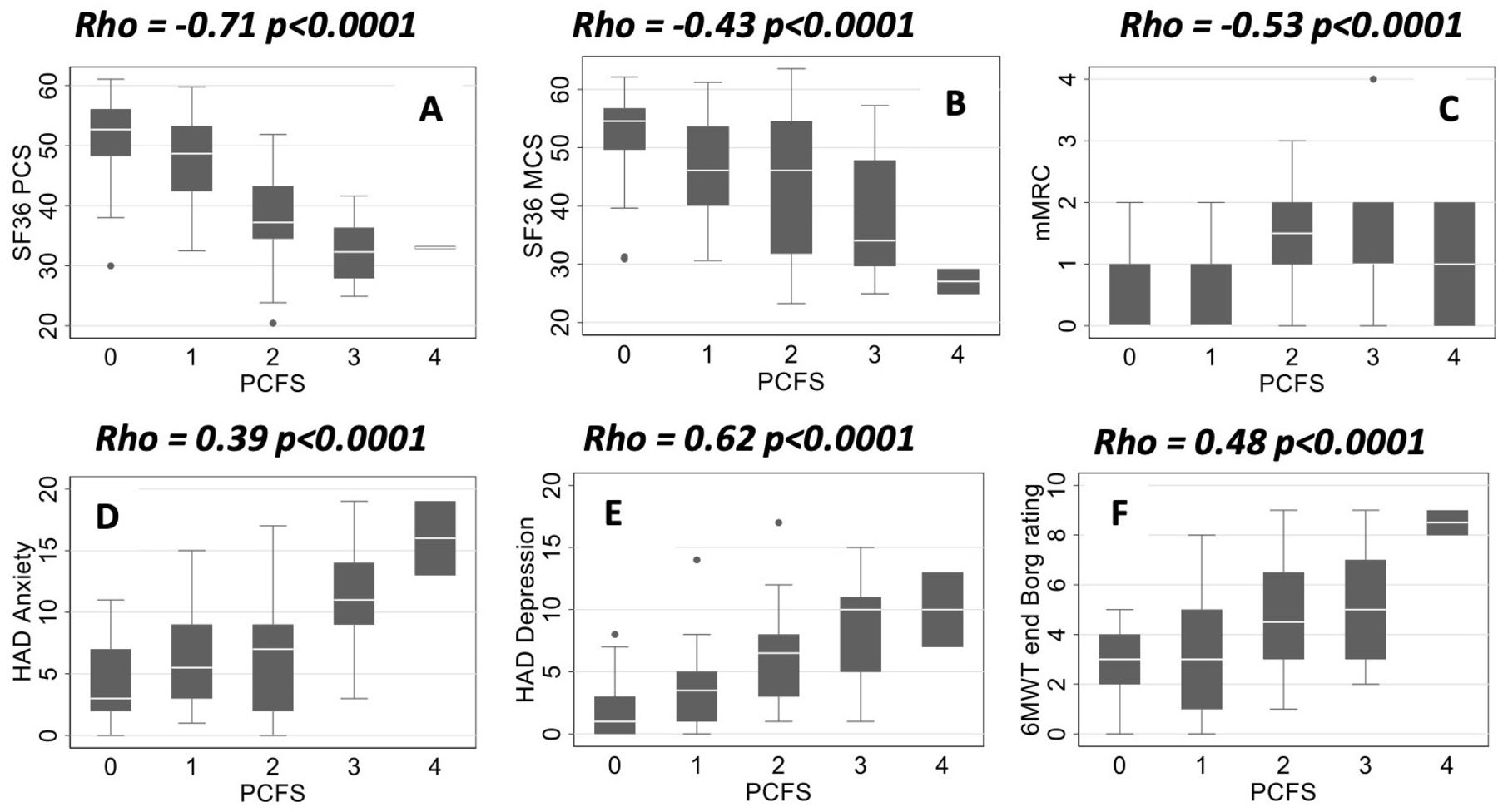
The PCFS Scale significantly correlated with all SF-36 questionnaire subgroups, including the physical composite score (rho=−0.71; p<0.0001, figure 1A) and the mental composite score (rho=−0.43; p<0.0001, figure 1B). The PCFS Scale also correlated significantly with the mMRC (rho=0.53; p<0.0001) (figure 1C), all subgroups of the MDP (data not shown) and both the HAD anxiety (rho=0.39; p<0.0001) and depression scale (rho=0.62; p<0.0001) (figure 1D,E). The PCFS Scale also correlated with the 6MWT end Borg dyspnoea rating (rho=0.48; p<0.0001) (figure 1F). Significant correlation was neither found between the PCFS Scale and TLco results nor with persistent lung abnormalities on chest CT scan (online supplemental figure 3). However, the PCFS Scale was significantly higher in the ‘isolated dyspnoea’ group, as well as the 6MWT end Borg rating (table 2).

{kind=link}
PCFS Scale correlates with SF-36 scores, mMRC dyspnoea scale, HAD Scale and the 6MWT end Borg rating. (A) Correlation between the SF-36 physical composite score and the PCFS scale. (B) Correlation between the SF-36 mental composite score and the PCFS scale. (C) Correlation between the mMRC and the PCFS Scale. (D) Correlation between the HAD A and the PCFS scale. (E) Correlation between the HAD D and the PCFS scale. (F) Correlation between the end 6MWT Borg scale and the PCFS Scale. 6MWT, Six-Minute Walk Test; HAD, Hospital Anxiety and Depression; mMRC, modified Medical Research Council; PCFS, Post-COVID-19 Functional Status; SF-36, Short Form-36.
Comparison of the PCFS Scale and 6MWT end Borg rating according to the type of sequelae
Discussion
In patients having suffered from severe COVID-19 pneumonia, our data showed that the PCFS Scale correlated with SF-36, dyspnoea and mental health questionnaires, making it a global and easy tool to detect functional limitations related to the multiple aspects of post-COVID-19. Indeed, SF-36 is a lengthy questionnaire that can hardly be used in everyday practice. The strong correlation with the physical composite score suggests that the PCFS Scale could be best suited to explore the physical impact of COVID-19.
We observed no correlation between the PCFS Scale and DLCO results or chest CT scan sequelae at reassessment (online supplemental figure 3), which is consistent with the literature suggesting that the symptom burden has no correlation with the initial severity or the existence of residual lung abnormalities.8 9 Interestingly, the PCFS Scale Score was significantly higher in the ‘isolated dyspnoea’ group, as well as the 6MWT end Borg rating (table 2), suggesting that the PCFS Scale also reflected deconditioning. Determining a PCFS Scale threshold that coincides with patients’ acceptable state could be interesting to target patients requiring careful prolonged medical follow-up after COVID-19.
In our study, we showed acceptable validity of the PCFS Scale according to the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) group standards10 by comparing it with other scales. We did not test ‘responsiveness’ to analyse the PCFS Scale ability to vary with treatment, for instance, physiotherapy. However, we retrospectively analysed the PCFS status before COVID-19 and 85% patients had a PCFS Scale of 0 at that time (data not shown).
In conclusion, the PCFS Scale correlated with quality of life, dyspnoea and mental health. The growing population of patients recovering from COVID-19 with persistent and disabling symptoms calls for specific rehabilitation programmes. The PCFS Scale may be a suitable instrument to search for functional limitations related to the wide range of symptoms following COVID-19 pneumonia. Importantly, these patients with functional limitations, but for some of them without pulmonary sequelae, will require careful follow-up, including deconditioning identification and treatment.
Data availability statement
Data are available upon reasonable request. The data are deidentified participant data, they are available from MK and data reuse will be allowed limited to academic research and to non-commercial use only, after evaluation of research project.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Nantes Teaching Hospital Ethics Committee (GNEDS). Written consent was obtained for each patient enrolled in the study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NB, EE and PL contributed to the study design, patient enrolment, data analysis and writing of the report. MK and J-BH contributed to the study design and data analysis. TG, CL, DH-L, LM, A-LC, SD, CB, AC and F-XB contributed to patient enrolment and follow-up. AN, DC and RL contributed to chest CT scan acquisition and analysis. PL was the author responsible for the overall content as the guarantor.
Funding This work was supported by the Institut de Recherche en Santé Respiratoire des Pays de la Loire. The authors thank the cluster LUNG innOvatiOn (LUNG O2) for logistic support.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.