Article Text

Abstract
Rationale Severe acute paediatric asthma may require treatment escalation beyond systemic corticosteroids, inhaled bronchodilators and low-flow oxygen. Current large asthma datasets report parenteral therapy only.
Objectives To identify the use and type of escalation of treatment in children presenting to hospital with acute severe asthma.
Methods Retrospective cohort study of children with an emergency department diagnosis of asthma or wheeze at 18 Australian and New Zealand hospitals. The main outcomes were use and type of escalation treatment (defined as any of intensive care unit admission, nebulised magnesium, respiratory support or parenteral bronchodilator treatment) and hospital length of stay (LOS).
Measurements and main results Of 14 029 children (median age 3 (IQR 1–3) years; 62.9% male), 1020 (7.3%, 95% CI 6.9% to 7.7%) had treatment escalation. Children with treatment escalation had a longer LOS (44.2 hours, IQR 27.3–63.2 hours) than children without escalation 6.7 hours, IQR 3.5–16.3 hours; p<0.001). The most common treatment escalations were respiratory support alone (400; 2.9%, 95% CI 2.6% to 3.1%), parenteral bronchodilator treatment alone (380; 2.7%, 95% CI 2.5% to 3.0%) and both respiratory support and parenteral bronchodilator treatment (209; 1.5%, 95% CI 1.3% to 1.7%). Respiratory support was predominantly nasal high-flow therapy (99.0%). The most common intravenous medication regimens were: magnesium alone (50.4%), magnesium and aminophylline (24.6%) and magnesium and salbutamol (10.0%).
Conclusions Overall, 7.3% children with acute severe asthma received some form of escalated treatment, with 4.2% receiving parenteral bronchodilators and 4.3% respiratory support. There is wide variation treatment escalation.
- paediatric asthma
Data availability statement
Data are available on reasonable request. Deidentified participant data and the data dictionary (REDCap data form) will be available for sharing from 1 July 2022. Any data access requests should be sent to SC (simon.craig@monash.edu), and should include a proposal from the individual or organisation regarding their plan for use of the data. The study team will review the request and consider the scientific merit of the proposed use of the data, and the legal, regulatory and ethical issues pertinent to the request. Presuming all constraints are addressed, the data will be shared using a secure file transfer platform.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Some children with acute asthma exacerbations require escalation of care beyond inhaled bronchodilators and oral corticosteroids; however, rates of intravenous therapy vary between 3.4% (in the UK and Ireland) to 10.5% in the USA.
To date, no large dataset has reported on both intravenous and respiratory support following first-line management for children presenting acutely to hospital with asthma.
What this study adds
This study of 14 029 New Zealand and Australian children presenting to hospital with acute wheeze or asthma demonstrates wide variation in management: 7.3% received some form of escalated treatment with 4.2% receiving parenteral bronchodilators and 4.3% respiratory support.
Severe outcomes were rare, with 243 children admitted to intensive care; 22 received non-invasive ventilation and only 4 were intubated.
How this study might affect research, practice or policy
Although large multicentre studies are required to guide future treatment, significant clinical events such as intubation, and/or use of non-invasive ventilation are too rare to be suitable for use as outcome measures in future randomised clinical trials.
Introduction
Asthma is a frequent reason for a child to attend the emergency department (ED),1 and one of the most common reasons for paediatric hospitalisation after an ED visit.2 In the USA, the rate (per population) of paediatric ED visits for asthma increased by 13.3% between 2001 and 2010,3 while in the UK, it is estimated that a child is admitted to hospital every 20 min due to an asthma exacerbation.4
Most children with asthma have mild or moderate exacerbations, and respond to first-line treatment with inhaled bronchodilator therapy and systemic corticosteroids.5 However, a proportion of children require more intensive therapies including intravenous medications, supplemental oxygen, respiratory support, endotracheal intubation and/or admission to the intensive care unit (ICU).5 6 Management of acute severe asthma is complicated by a number of challenges, including the infrequency of its occurrence, a large number of treatment options and wide variation in self-reported and actual practice.7 Acute asthma has been highlighted as a research priority by multiple paediatric emergency medicine research networks.8–10
A 2015 study from the UK found that 110 (3.4%) of 3238 children with acute asthma presenting to 24 EDs received intravenous therapy: magnesium in 2.1%, salbutamol in 1.9% and aminophylline in 1.6%. More than thirty different intravenous dosing and infusion regimens were identified in these 110 patients.6 In contrast, a study from the USA found that 10.5% of 61 854 children with acute asthma presenting to seven EDs between 2012 and 2017 received intravenous magnesium.11 No clinical characteristics explained the variation in intravenous magnesium use in the USA study, and the large difference between use of intravenous magnesium in the UK and USA studies remains unexplained. While intravenous magnesium has been found in meta-analysis to reduce both hospital admission and hospital length of stay (LOS), the quality of evidence is low, mainly due to small sample size.12
In addition to the use of intravenous bronchodilators, another management strategy that is increasing in use and supported by limited evidence is nasal high flow (NHF) therapy.13 Other management strategies similarly lack high-quality evidence, or even any evidence of effect on the key outcomes of LOS and admission into hospital. High-quality multicentre research to address these important evidence gaps is a research priority for major paediatric emergency research networks.14 15
To date, no large dataset has reported on both intravenous and respiratory support following initial management with inhaled bronchodilators and oral corticosteroids for children presenting acutely to hospital with asthma. This information is vital to understand variation in care, outcomes from care, and planning future studies in this population.
The primary aim of this study was to describe the escalation of treatment (modalities beyond systemic corticosteroids and inhaled bronchodilators) in children presenting to hospital with acute severe asthma. Secondary aims were to (1) describe variation in escalation of treatment; (2) determine the frequency of key outcomes (such as intubation, ICU admission and death) and complications in these children; (3) identify predictors for escalation of treatment and (4) identify predictors for hospital LOS.
Methods
A multicentre retrospective cohort study of children diagnosed with asthma or wheeze was conducted in 18 Australian and New Zealand EDs associated with the Paediatric Research in Emergency Departments International Collaborative network.16 Eight hospitals had pediatric-only EDs, while the remaining EDs manage a mixture of adults and children.
Each site investigator identified a list of medical records of all children meeting inclusion criteria presenting between 1 November 2015 and 31 October 2016. The dates were chosen to avoid any confounding effects of the significant thunderstorm asthma event which occurred in Melbourne in November 2016.17 Potentially eligible records were identified using the local ED information system and hospital medical records, using the following International Classification of Diseases (ICD)-10 codes: ‘Asthma’ or ‘Childhood asthma’ (ICD-10 code: J45, J46); ‘Wheezing’ (ICD-10 code: R06.2) and ‘Acute bronchiolitis’ (ICD-10 code: J21). An ED visit was considered eligible for inclusion if the child (1) was aged between 1 and <18 years (up to but not including 18th birthday) and (2) had a final discharge diagnosis of asthma/wheeze. Children with a final diagnosis of bronchiolitis and no bronchodilator administered, and those with a diagnosis of foreign body inhalation, were excluded. Each ED presentation was eligible for inclusion, even if the child had previously been included in the study.
Data collection included (for all patients): age, sex, hospital LOS (from time of arrival in ED to the time the patient left hospital), triage category (using the Australasian Triage Scale (ATS),18 a 5-point scale which allocates patients from category 1 (should be seen immediately) to category 5 (can wait up to 120 min)), and whether or not asthma treatment was escalated beyond systemic corticosteroids and inhaled bronchodilators (short-acting beta-agonists or anticholinergic agents). For patients who had escalation of treatment (defined as any of ICU admission, invasive or non-invasive respiratory support, or parenteral bronchodilator treatment)), the following data were also collected: duration of ICU admission; intravenous bronchodilator treatment used; type of non-invasive respiratory support (continuous positive airway pressur (CPAP)/bilevel non-invasive ventilation (NIV) and NHF therapy); use of intubation and mechanical ventilation; interhospital transfer and complications (pneumothorax, hypokalaemia requiring replacement therapy, hypotension requiring an intravenous fluid bolus of at least 10 mL/kg, nausea/vomiting requiring antiemetic therapy, arrhythmias requiring ECG monitoring or antiarrhythmic therapy and death).
We followed guidance for optimal data quality in retrospective studies, including the use of defined inclusion criteria and variables, a standardised data extraction document and trained abstractors.19 Our research is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology statement.20
Data storage and analysis
Deidentified data were entered into a protected electronic database by staff at each participating hospital using Research Electronic Data Capture,21 and housed at a central data processing site at Murdoch Children’s Research Institute, Parkville, Victoria, Australia.
Data were analysed descriptively. Binary outcomes are presented as proportions with 95% confidence intervals (CIs). For continuous outcomes, data are presented as mean and standard deviation (SD; normally distributed data) or median and IQR (Inon-parametric data). For categorical data, comparisons were made with calculation of OR (with 95% CIs), and significance determined using χ2 analysis. For non-parametric continuous data, comparisons were made using the Mann-Whitney U test (two-group comparisons) and the Kruskall-Wallis test (three-group comparisons). For normally distributed continuous data, two-group comparisons were made using independent samples t-test, while three-group comparisons were made using Analysis of Variance (ANOVA). LOS and type of escalation of treatment for the entire study population are analysed overall, and in subgroups by age: 1–5 years and 6–17 years, as we hypothesised that use of individual treatments would vary with age.
Multilevel generalised linear models were carried out to assess factors influencing LOS and escalation of treatment, clustered on hospital site. A multiple logistic model was used to assess predictors of escalation of treatment, and odds ratios (OR) and 95% CI presented. For this outcome, Triage category 5 resulted in perfect prediction (all no escalation of treatment). Therefore, we combined Triage categories 4 and 5 (non-urgent and semiurgent) and used this combination as the reference for analysis.
For the LOS outcome, count distributions were explored due to heavy skew. Overdispersion in the data ruled out Poisson distribution, so negative binomial distribution was employed. Incidence rate ratios (IRR) are calculated alongside 95% CI and p values.
Sample size
The rate of administration of intravenous treatment for children in Australia and New Zealand was unknown. Based on the rate of intravenous treatment in a UK study of approximately 3%,6 we anticipated the need to review approximately 1000 eligible charts at each site to obtain 30–40 presentations where intravenous bronchodilators were administered. This number would allow the detection of a 3%–6% difference in characteristics between those with and without escalated care.
Each site was requested to collect data on 1000 patients or 12 months of data (whichever was less). If more than 1000 eligible medical records were identified on the initial screen of medical records at lenany participating hospital, screening occurred in random order until 1000 eligible records had been identified for abstraction.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
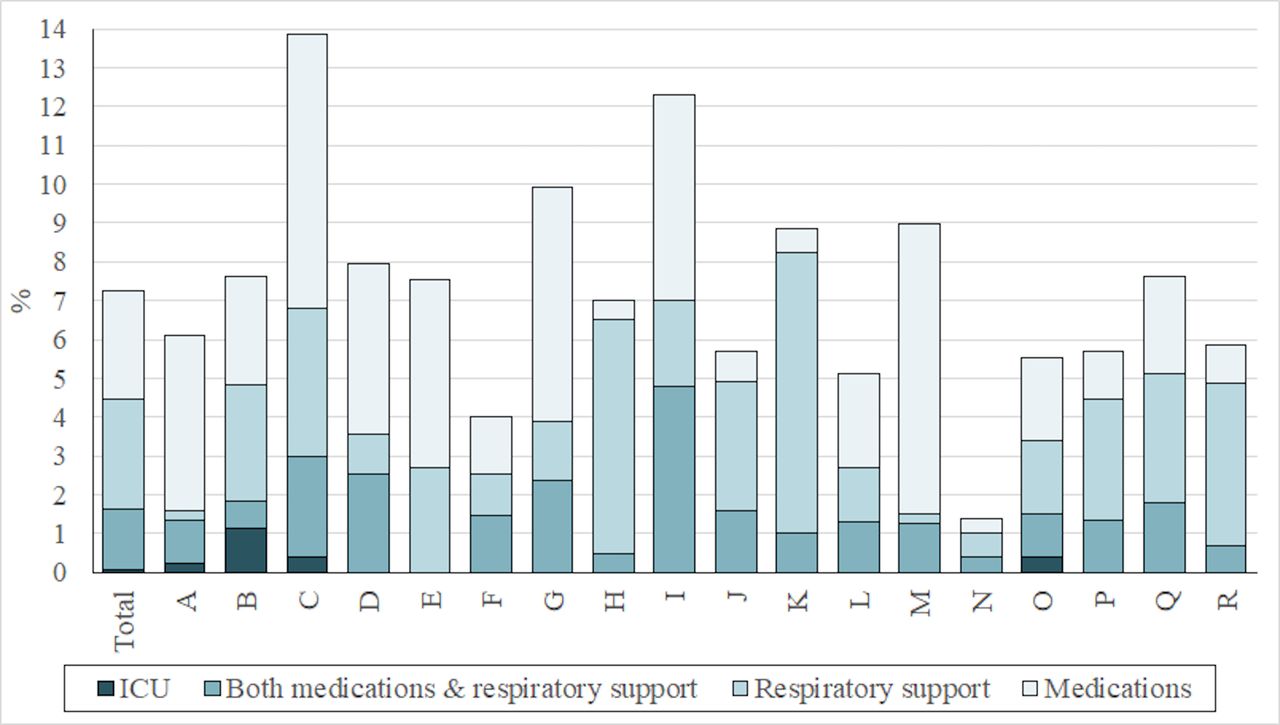
A total of 14 029 children were enrolled from 18 participating hospitals (table 1). Of these, 1020 (7.3%, 95% CI 6.9% to 7.7%) had escalation of treatment. Children with escalation of treatment had similar demographic features to those without escalation of treatment (median age 3 (IQR 1–6) years vs 3 (IQR 1–5) years; male sex 62.5% vs 63.0%) but were more likely to have a more urgent triage category. Of the total study population, 400 (2.9%, 95% CI 2.6% to 3.1%) received respiratory support alone, 380 (2.7%, 95% CI 2.5% to 3.0%) received parenteral bronchodilator treatment alone and 209 (1.5%, 95% CI 1.3% to 1.7%) received both respiratory support and parenteral bronchodilator treatment. 30 (0.14%, 95% CI 0.14% to 0.3%), all from one hospital, received nebulised magnesium: 23 received nebulised magnesium alone, while seven also received respiratory support and parenteral bronchodilators. 243 (1.7%, 95% CI 1.5% to 2.0%) were admitted to the ICU; of these eight (0.06%, 95% CI 0.02% to 0.11%) received neither respiratory support nor parenteral bronchodilator treatment (table 2). There was considerable variation between sites in the proportion of children receiving escalation of treatment, and the type of escalation of treatment used (figure 1).

Proportion of children receiving escalation of treatment, and the type of escalation of treatment used, by Hospital.
Demographic and clinical data for children with and without escalation of asthma therapy*
Details of escalation of therapy,* comparison of young (1 –5 years) and older (6 to <18 years) children
For the children receiving respiratory support, NHF therapy was used in 603 (99.0%, 95% CI 97.9% to 99.6%), with a median duration of 18.7 (IQR 6.9–38.8) hours. A total of 432/603 (71.6%) received NHF in the ward environment, and did not require ICU admission. Other forms of respiratory support either alone or in combination with NHF were used in 22/609 (3.6%, 95% CI 2.3% to 5.4%). Of all escalation interventions NHF alone accounted for 322/1020 (31.7%, 95% CI 28.7% to 34.5%). Overall only four children (0.03%, 95% CI 0.01% to 0.07%) received invasive ventilation and endotracheal intubation, and there were no deaths.
Three combinations of intravenous medication accounted for over 85% of parenteral bronchodilator usage: magnesium alone (291/577, 50.4%), magnesium and aminophylline (142/577, 24.6%) and magnesium and salbutamol (58/577, 10.0%). Children aged 6–17 years were less likely to receive respiratory support (1–5 years 484/714, 67.8% vs 6–17 years 125/306, 40.8%; OR 0.79, 95% CI 0.64 to 0.96, p=0.02), but more likely to receive parenteral bronchodilators (1–5 years 349/714, 48.9% vs 6–17 years 228/306, 74.5%; OR 2.05, 95% CI 1.73 to 2.43, p<0.001) (table 3).
Treatments administered and complications occurring in those children who received escalation in therapy,* comparison of young (1–5 years) and older (6 to <18 years) children
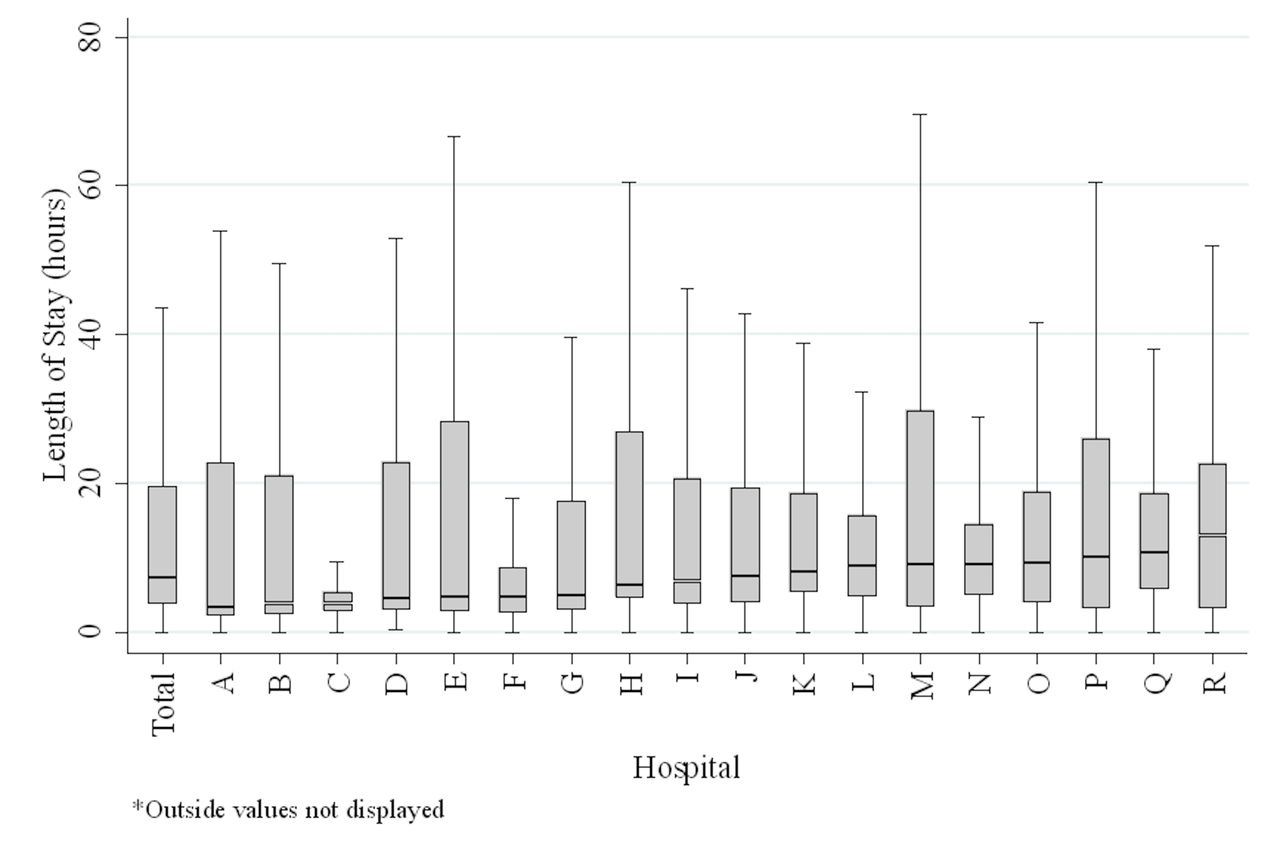
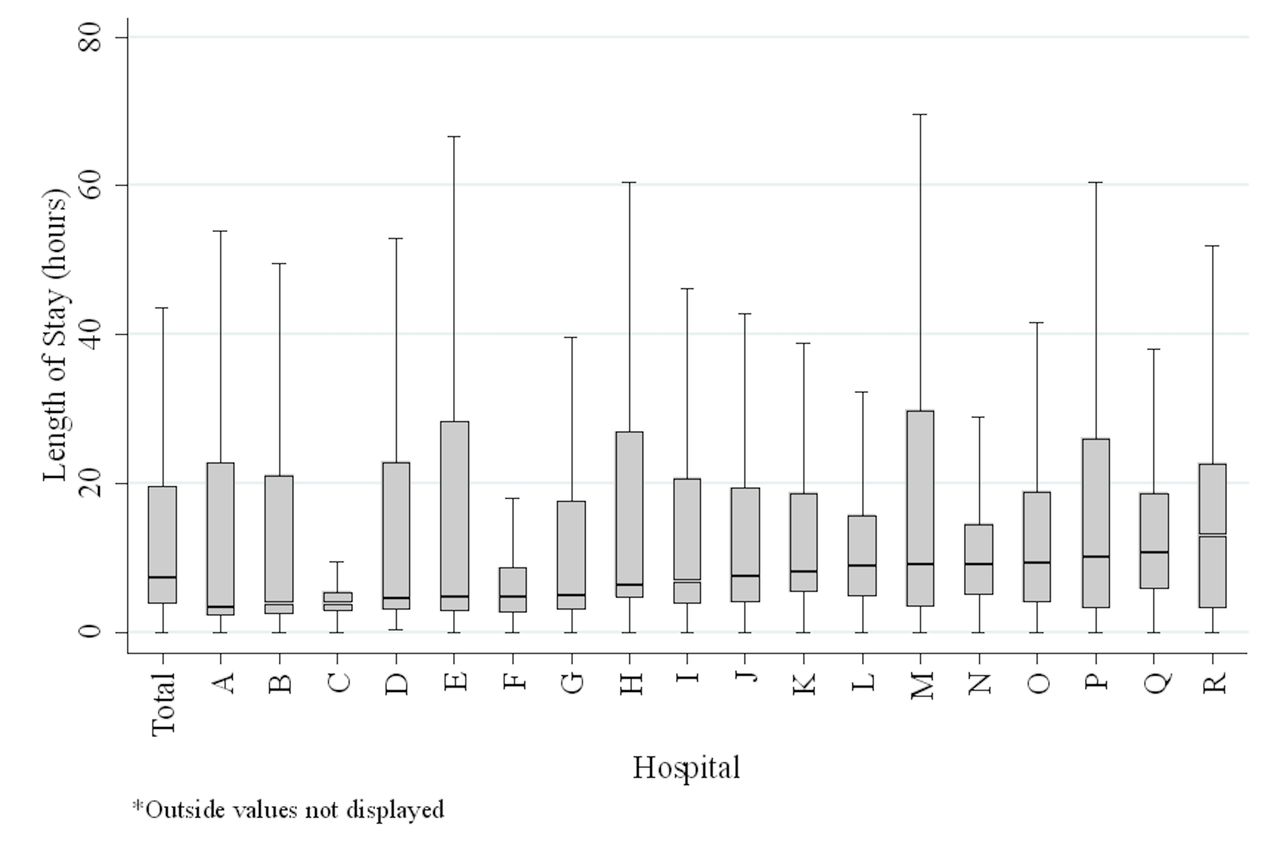
Overall the median LOS for the 14 029 children was 7.4 (IQR 3.7–19.6) hours. Children aged 1–5 years had longer LOS compared with older children (1–5 years LOS 8.2 hours, IQR 4.0 to 20.1 hours vs 6–17 years LOS 5.4 hours, IQR 3.0 to 16.5 hours; p<0.001). There was considerable variation in LOS by site (figure 2). Children with escalation of therapy had a longer LOS (children with escalation 44.2 hours, IQR 27.3–63.2 hours vs children without escalation 6.7 hours, IQR 3.5–16.3 hours; p<0.001) (table 1).
{kind=link}
{kind=link}
Hospital length of stay, by site.
Multilevel linear models (table 4) demonstrated that LOS was strongly related to a higher (more urgent) triage category (ATS 1 patients had an IRR of 2.70 (95% CI 2.24 to 3.25), p<0.001) and escalation of treatment (IRR of 3.45, 95% CI 2.93 to 4.06, p<0.001). Escalation of treatment was strongly related to a higher (more urgent) triage category (ATS 1 patients had an OR of 214 (95% CI 101 to 452, p<0.001)) and increasing age (OR 1.05 (95% CI 1.02 to 1.09), p=0.004).
Regression analysis modelling length of stay and escalated treatment
Regression analysis using hospital as an independent variable (rather than a clustering variable) demonstrated some effect of hospital site on LOS and escalation of treatment (online supplemental table 1).
Supplemental material
Of those receiving escalation of therapy, major sequelae were rare. There was no hypotension requiring intravenous fluid therapy, and no arrhythmias requiring antiarrhythmic therapy or DC-cardioversion. Only two patients had a pneumothorax; both were managed conservatively without pleural drainage (table 3). Potassium replacement (OR 2.69, 95% CI 1.89 to 3.83, p<0.001) and use of antiemetics (OR 3.81, 95% CI 2.7 to 5.37, p<0.001) were more commonly used in children aged 6–17 years than those aged 1–5 years.
Discussion
Our multicentre study of over 14 000 New Zealand and Australian children presenting to hospital with acute wheeze or asthma demonstrates wide variation in management beyond systemic corticosteroids and inhaled bronchodilators. Overall, 7.3% of children presenting to hospital with asthma and wheeze received some form of escalated treatment with 4.2% receiving parenteral bronchodilators and 4.3% respiratory support. We have identified considerable inter-hospital differences in the frequency of treatment escalation, the choice of escalation treatments and hospital LOS.
This is the first large dataset reporting management beyond systemic corticosteroids and inhaled bronchodilators in the current era where NHF therapy has been increasingly used outside the ICU environment. Remarkably NHF was used in nearly all patients who received respiratory support and accounted for nearly one-third of all escalation of asthma treatment. There is high-quality evidence supporting NHF therapy as a rescue treatment in children <1 year with bronchiolitis.22 This may explain the increased use in younger children in our study. However, there is little evidence to guide NHF therapy in children over 1 year of age with asthma and wheeze. Small observational studies report conflicting results,23 24 while pilot randomised controlled trials (RCTs) in children25 and adults26 appear promising. The results of an ongoing large RCT of over 1500 children aged 1–4 years comparing conventional ‘low-flow’ oxygen to NHF with oxygen for hypoxic respiratory failure (including presentations characterised by airflow obstruction such as asthma/wheeze)25 is likely to provide more definitive evidence of effect in that subgroup.
In our cohort, the use of respiratory support varied ten-fold between hospitals and the use of parenteral treatment varied eight-fold. Intravenous magnesium was administered in 3.9%. This is nearly twice as frequent as reported in the UK and Ireland (2.1%)6 but less than half the rate reported in the USA (10.5%).11 Lack of high-quality evidence may contribute to this regional variation in practice. A 2016 Cochrane review of the use of intravenous magnesium for treating acute paediatric asthma in the ED found that the treatment may reduce the need for hospital admission and LOS, although this was based on limited data (admission, three studies of 115 children; LOS one study of 47 children).12 The authors concluded equipoise still exists and recommended further trials.
Similar to the UK study, we found a large number of combinations of parenteral bronchodilators were used. However, in 85% of children receiving escalated therapy with intravenous bronchodilator treatment, this was confined to just three different regimens; intravenous magnesium alone or in combination with either aminophylline or salbutamol. Once again, the lack of high-quality evidence,15 as well as inconsistent local guidelines, may contribute to this variation. While magnesium and salbutamol are listed as second-line and third-line bronchodilators for management of acute severe paediatric asthma in Australian national guidelines,27 some state-based guidelines prefer magnesium and aminophylline.28 In New Zealand, guidelines suggest consideration of all three without preference,29 while the Global Initiative for Asthma guidelines strongly recommend against aminophylline and states there is insufficient evidence to support the use of intravenous beta2-agonists.30
Cochrane reviews of advanced pharmacologic treatment of children with acute exacerbations of asthma highlight a number of knowledge gaps.15 The evidence supporting intravenous magnesium is extremely limited (including only 5 studies and 182 children),31 while only one study (showing no significant benefit) was identified regarding intravenous ketamine.32 Despite a meta-analysis of nearly 3000 patients enrolled in trials of inhaled magnesium, review authors noted that large, well-conducted trials had not shown clinically meaningful benefits.33 This finding has been reinforced by a recent large study of over 800 children demonstrating no difference in hospitalisation when nebulised magnesium was added to nebulised albuterol.34 Studies on intravenous beta2-agonists35 36 and/or intravenous aminophylline37 have not demonstrated clinically significant benefit, while there is no available Cochrane review on the utility of parenteral epinephrine for acute severe asthma in children.15
A major hurdle to determining effective management strategies following failure of systemic corticosteroids and inhaled bronchodilators in children presenting with acute severe asthma, is the lack of consistency in primary outcome measures. A systematic review of primary outcomes used in RCTs of intravenous bronchodilators in acute paediatric asthma identified 35 publications and four protocols that used 56 different primary outcomes between them, concluding that core outcome sets need to be developed for future trials.38 Large observational studies, such as our study, allow the consideration of the frequency of important outcome measures and are vital to informing the design of future comparative trials.
Of those children who had escalated treatment of some description (intensive care admission, respiratory support or intravenous bronchodilator administration), 243 (23.8%) were admitted to intensive care. However, only four received intubation and mechanical ventilation, and 22 received CPAP or Bi-level NIV. Sample size calculations for studies with 90% power and a type I error (alpha) of 0.05 to demonstrate a 50% reduction in these outcomes would require 24 078 (for intubation) and 5766 (for NIV) children with asthma requiring escalation of therapy, or 450 220 (for intubation) and 80 728 (for NIV) children attending the ED with an asthma exacerbation. It, therefore, is not feasible, even with large multicentre studies, to achieve sufficiently large sample sizes to power randomised clinical trials to address these outcomes.
Our study has a number of limitations. Our data was based on a retrospective analysis of medical records; we mitigated its inherent limitations by following published guidance19 though abstractors were not blinded. Our case definition (asthma or wheeze, aged between 1 and 17 years, administered salbutamol in the ED) was intentionally broad, and aimed to capture all children outside the traditional age range for bronchiolitis who were administered bronchodilators. Although the inclusion of a large number of preschool children raises the possibility of some overlap with bronchiolitis, the definition of bronchiolitis in the Australasian setting usually refers to those under 12 months of age.
As our focus was on describing practice in those children who received escalated asthma care, we collected limited data on those patients who did not receive treatment beyond inhaled bronchodilators and oral corticosteroids. We did not assess compliance with local or national clinical practice guidelines. Our determination of predictors of escalated therapy and hospital length of stay was therefore limited due to less data points being captured for those not receiving escalated care.
Due to the large number of charts at each site, we were unable to allocate two reviewers to independently extract the data. However, the data points requested were designed to be from unambiguous parts of the medical record (such as medication charts, triage categories, oxygen and respiratory therapy, and times of admission and discharge) rather than items which require significant interpretation such as clinical examination findings. Further, it is not routine practice in Australia and New Zealand to use a bedside asthma score, so this information was not available.
In conclusion, there is wide variation in both the frequency and nature of escalation of treatment for children with ED presentations for acute severe asthma. Overall, 7.3% of children presenting to hospital with asthma and wheeze received some form of escalated treatment with 4.2% receiving parenteral bronchodilators and 4.3% respiratory support. NHF is more likely in children aged 1–5 years, while intravenous bronchodilators, particularly magnesium, is more commonly administered in older children. Significant clinical events such as intubation, and/or use of NIV are rare and are not suitable for use as outcome measures in future studies.
Data availability statement
Data are available on reasonable request. Deidentified participant data and the data dictionary (REDCap data form) will be available for sharing from 1 July 2022. Any data access requests should be sent to SC (simon.craig@monash.edu), and should include a proposal from the individual or organisation regarding their plan for use of the data. The study team will review the request and consider the scientific merit of the proposed use of the data, and the legal, regulatory and ethical issues pertinent to the request. Presuming all constraints are addressed, the data will be shared using a secure file transfer platform.
Ethics statements
Patient consent for publication
Ethics approval
The project was approved by the Human Research Ethics Committees of Monash Health (RES-17-0000-238L) and Monash University (MUHREC 10407). Site-specific approval was obtained at each institution prior to commencement of data collection.
Acknowledgments
The authors would like to acknowledge the following people for their assistance with data extraction for this project: Perth Children’s Hospital: Dennis Chow, Lisa Properjohn, Carsten Broeze, Stephen Paull, Kathy Barton, Katie Hillam, Kareena Easton, Marie Ni Chollatain, Rickie-Lee Jackson, Natalie van Asselt, Tim Renshaw. Children’s Hospital Westmead: Deepali Thosar. Logan Hospital: Brooke Charters, Vanessa Funk. Monash Health: Natalie Sae-Rian. Queensland Children's Hospital: Eadon Seifried, Sally Gray, Angus Jones, Mark O'Grady, Ann Hinde.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SC, FB, AG, CVEP and SD identified the research question. SC was responsible for the study design and research protocol, and for drafting the manuscript. SC, JH, AK, SG, JF, BL, MB, JN, AL, CM, NW, DB, JW, CG, ER, JL, LJ and SD were responsible for data collection at their respective hospitals. All other authors contributed equally to writing, reviewing and editing the manuscript. SH and SC were responsible for the statistical analysis. All authors provided comments on the drafts and have read and approvedthe final version of the Article. All authors had full access to all the data(including statistical reports and tables) at the conclusion of the studyand take responsibility for the integrity of the data and the accuracy of thedata analysis. SC is guarantor for this paper, accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The study was part funded by a grant from the National Health and Medical Research Council (NHMRC, Centre of Research Excellence grant (GNT1058560), Canberra, Australia and the Victorian Government’s Operational Infrastructure Support program. Data collection at Logan Hospital was supported by a grant from the Emergency Medicine Foundation, Queensland. Data collection at Perth Children’s Hospital was supported by a grant from the Perth Children’s Hospital Foundation. SC has received funding from a Thoracic Society of Australia and New Zealand/National Asthma Council Fellowship and the ACEM Foundation Al Spilman Early Career Research Grant. SRD's time is funded in part by Cure Kids New Zealand. FB’s time was part funded by a grant from the Royal Children’s Hospital Foundation, Melbourne, Victoria, Australia and an NHMRC Practitioner Fellowship.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.