Article Text

Abstract
Background Occupational exposure and increased body mass index (BMI) are associated with respiratory symptoms. This study investigated whether the association of a respiratory burden score with changes in BMI as well as changes in occupational exposure to vapours, gas, dust and fumes (VGDF) varied in subjects with and without asthma and in both sexes over a 5-year period.
Methods In a 5-year follow-up of a population-based study, 6350 subjects completed a postal questionnaire in 2013 and 2018. A respiratory burden score based on self-reported respiratory symptoms, BMI and frequency of occupational exposure to VGDF were calculated at both times. The association between change in respiratory burden score and change in BMI or VGDF exposure was assessed using stratified regression models.
Results Changes in respiratory burden score and BMI were associated with a β-coefficient of 0.05 (95% CI 0.04 to 0.07). This association did not vary significantly by sex, with 0.05 (0.03 to 0.07) for women and 0.06 (0.04 to 0.09) for men. The association was stronger among those with asthma (0.12; 0.06 to 0.18) compared with those without asthma (0.05; 0.03 to 0.06) (p=0.011). The association of change in respiratory burden score with change in VGDF exposure gave a β-coefficient of 0.15 (0.05 to 0.19). This association was somewhat greater for men versus women, with coefficients of 0.18 (0.12 to 0.24) and 0.13 (0.07 to 0.19), respectively (p=0.064). The estimate was similar among subjects with asthma (0.18; –0.02 to 0.38) and those without asthma (0.15; 0.11 to 0.19).
Conclusions Increased BMI and exposure to VGDF were associated with increased respiratory burden scores. The change due to increased BMI was not affected by sex, but subjects with asthma had a significantly larger change than those without. Increased frequency of VGDF exposure was associated with increased respiratory burden score but without statistically significant differences with respect to sex or asthma status.
- Asthma
- Asthma Epidemiology
- Clinical Epidemiology
- Occupational Lung Disease
- Perception of Asthma/Breathlessness
Data availability statement
Data are available upon reasonable request. The data sets generated and/or analysed during the current study are not publicly available due to privacy policy regulations but are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Asthma
- Asthma Epidemiology
- Clinical Epidemiology
- Occupational Lung Disease
- Perception of Asthma/Breathlessness
Key messages
What is already known on this topic
Increased body mass index (BMI) and occupational exposure are associated with respiratory symptoms.
It is not known if change in respiratory burden score is associated with changes in BMI and occupational exposure to vapours, gas, dust and fumes and what the potential associations between sex and asthma status are.
What this study adds
Increased BMI and occupational exposure were associated with increase in respiratory burden score.
Both associations did not differ at the level of statistical significance between sexes, but the association with change in BMI was stronger with a positive asthma status.
How this study might affect research, practice And/Or policy
Further studies are needed to confirm our findings, but this study contributes to a better understanding of how respiratory burden is affected by occupational exposure and BMI.
This knowledge may aid clinical decision-making and inform more personalised treatments in patients with asthma, obesity and occupational exposure.
Introduction
Increased body mass index (BMI) (≥25 kg/m2) and occupational exposure to vapours, gas, dust and fumes (VGDF) are associated with respiratory symptoms.1 2 Obesity is associated with exertional dyspnoea, an increased risk of asthma and reduced asthma control.1 Furthermore, patients with extremely high BMI (>50 kg/m2) show a significant lung function improvement after weight loss following bariatric surgery.3 Peralta et al4 demonstrated that a moderate and high weight gain over 20 years was associated with accelerated lung function decline (forced vital capacity and forced expiratory volume in 1 s) among adults, while weight loss improved this excessive decline. However, few studies have assessed the changes in respiratory symptoms due to weight gain or loss. Ekström et al showed that obesity is strongly associated with increased activity-related breathlessness5 and that subjects with increased BMI since their 20s had more breathlessness compared with those with stable weight.
Occupational exposure to VGDF is common. For instance, in Norway, it is estimated that 23% of the workers are exposed.6 Current evidence strongly suggests that exposure to VGDF can affect the airways in subjects with and without asthma.2 5 7–11 Multiple studies have shown that exposure to VGDF is associated with chronic obstructive pulmonary disease (COPD)8 and asthma,9 10 12 and that occupational exposure to VGDF can also be a risk factor for asthma exacerbation.11 13
Female sex is associated with a higher frequency of respiratory symptoms and severe asthma14 and is at an increased risk of asthma.15 16 Women exposed to dust report more shortness of breath, and in particular inorganic dust exposure is associated with asthma in women, while men only reported occasional wheezing and reduced lung function.17
Although the associations between respiratory symptoms and increased BMI and VGDF exposure are well documented, there is a lack of prospective studies on how change in BMI or VGDF exposure affects respiratory symptoms. In addition, there is a lack of knowledge on the influence of asthma status and sex over these effects. A better understanding of how changes in VGDF exposure or BMI affect respiratory symptoms, particularly in vulnerable subjects, will improve prevention and help guide personalised treatments.
The present study aimed to assess whether the association of a change in respiratory burden score with changes in BMI and occupational VGDF exposure varied with self-reported, physician-diagnosed asthma status and sex.
Methods
Study population
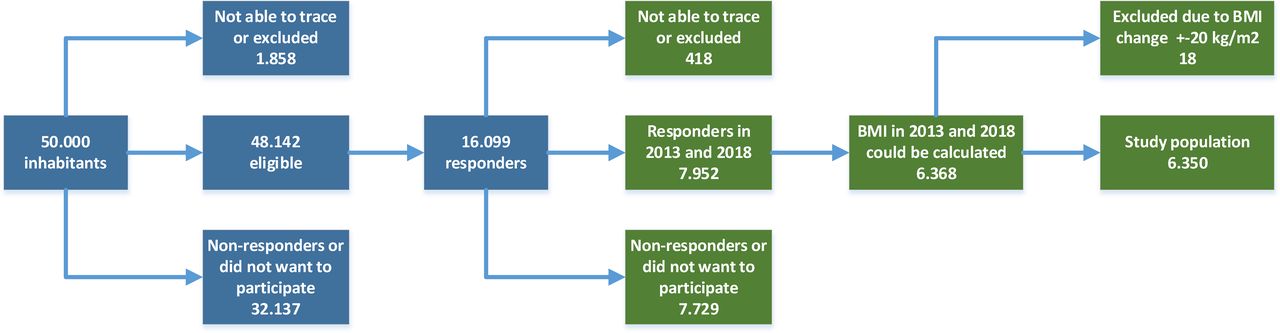
The Telemark study is a population-based survey that started in 2013 with a random sample of 50 000 inhabitants living in Telemark County, Norway, aged 16–50 years, who received a postal questionnaire. Of these, 48 142 were eligible and 16 099 responded (response rate: 33%).18 In 2018, all eligible 2013 responders (n=15 681) were invited to complete the questionnaire again. Four hundred and eighteen subjects could not be traced or were excluded. Subjects not providing height and weight and thus impeding BMI calculation at both baseline and follow-up were excluded from the present study.
Questionnaire
The questionnaire included questions regarding occupational exposure, physician-diagnosed asthma, respiratory symptoms ever and in the last 12 months, height, weight, and possible confounders. The questionnaire was based on the European Community Respiratory Health Survey questionnaire and a validated questionnaire from a similar study in Sweden.19
Exposure variables
BMI, measured in kg/m2, was calculated for each participant in 2013 and 2018 using the self-reported weight and height from the questionnaires. BMI was stratified into the following categories recommended by the WHO: normal weight (including underweight) <25.0 kg/m2, overweight 25.0–29.9 kg/m2 and obese ≥30 kg/m2, and was used as a continuous variable.20 As only 85 subjects (1.3%) were classified as underweight (BMI ≤18.5 kg/m2), they were included in the normal weight category. Change in BMI was calculated for each participant by subtracting the BMI value in 2013 from that in 2018.
VGDF exposure in 2013 was defined as an affirmative answer to the question ‘Have you ever been exposed to gas, smoke, or dust at work?’ All exposed participants in 2013 were then asked to grade their average exposure in the past 5 years into one of the following categories: ‘Daily, for large parts of the working day’ (exposure=4 points), ‘Daily, but for short periods’ (exposure=3 points), ‘Weekly’ (exposure=2 points), ‘Less often’ (exposure=1 point) and ‘never’ (no exposure=0 points). In 2018, the subjects were asked the same question with the options ‘No’, ‘Yes’ or ‘Yes, in the last 12 months’, and in case of an affirmative answer in the last 12 months the participants were asked to classify the exposure into the same categories as in 2013. Exposure change was calculated by subtracting the exposure points in 2013 from those in 2018. A positive or negative number indicates that the exposure frequency increased or decreased, respectively. The analyses were restricted to subjects engaged in paid work in the last 12 months of 2013. Subjects engaged in paid work in the last 12 months in 2013 but not in 2018 were included in the analyses as unexposed in 2018. Subjects with missing data for VGDF exposure were excluded from the analyses on change in VGDF.
Outcome variable
The questionnaire enquired about seven respiratory symptoms in the last 12 months and the current use of any medication for asthma (online supplemental table 1). A missing answer was recoded as not having that symptom or not using medication for asthma. We calculated a respiratory burden score for each participant in 2013 and 2018 by adding positive answers to the questions to a maximum score of 8. We then calculated the change in respiratory burden score by subtracting the score in 2013 from that in 2018, such that a positive number represented more respiratory symptoms in 2018 than in 2013. We chose to use a respiratory burden score to better describe the total respiratory symptom burden, and because it also provides increased statistical power and better describes symptoms as a continuum.21 Although current use of asthma medication is not a respiratory symptom, we included this question in the respiratory burden score as respiratory symptoms can lead to medication usage. Similar scores based on these symptoms have been previously used in other studies on subjects with asthma.21 22
Supplemental material
Background and adjustment variables
Asthma was defined by an affirmative response to the following question: ‘Has a physician ever diagnosed you with asthma?’ Age and sex were confirmed using the Norwegian National Population Registry.
At both time points, smoking habits were classified as daily smokers, occasional smokers and former smokers in case of an affirmative answer to the following question: ‘Do you smoke every day (also applies if you only smoke a few cigarettes, cigars, or light a pipe each day)?’, ‘Do you smoke occasionally (not each day, but weekends, parties, or similar)?’ and ‘Did you used to smoke?’, respectively. Those who did not answer any of the three questions were defined as missing and those with three negative responses were categorised as never smokers. The variable for smoking habit changes between 2013 and 2018 was divided into the three following categories: same, increased or decreased.
Participants’ educational levels were categorised into the following categories: elementary education (≤10 years), upper secondary school and certificate (additional 3–4 years), and university and university college. In addition, we included a category for other education and missing data.
Statistical analyses
To compare the longitudinal changes in background variables from 2013 to 2018, we used a paired t-test for continuous variables and a McNemar’s test for categorical variables. Changes in BMI and VGDF exposure frequency were calculated by subtracting the values in 2013 from those in 2018. We used linear regression models to assess the associations between change in respiratory burden score as an outcome variable and changes in BMI or VGDF exposure frequency. In the unadjusted linear regression models, we used change in respiratory burden score as the outcome variable and changes in BMI or VGDF exposure or possible confounding variables as the exposure variable. In the adjusted models to estimate the effect of changes in BMI or VGDF exposure frequency, we adjusted for age, sex, educational category in 2013, smoking habit category in 2013, change in smoking habit, BMI category in 2013, physician-diagnosed asthma in 2013, VGDF exposure in 2013 and respiratory burden score in 2013 (full model). The models were then stratified for sex and physician-diagnosed asthma in 2013, and interaction terms were used to test differences in strata-specific effect estimates.
All analyses were performed using the statistical package IBM SPSS V.26.0. Statistical significance was set at p<0.05.
Patient and public involvement
A representative from the Norwegian Asthma and Allergy Association (NAAA) was a member of the study steering committee and contributed to the development of questionnaires. NAAA representatives have also been involved in the study planning and transfer of knowledge to the patient group.
Results
Figure 1 shows a flow chart of the participant inclusion and exclusion procedures. Briefly, 7952 subjects responded to the questionnaire in both 2013 and 2018. Of these, 6368 reported weight and height on both questionnaires to allow calculation of BMI changes. All subjects with a BMI change >±20 points were excluded (n=18). This was based on a scatter plot and performed to exclude extreme values and errors in recorded weight due to automatic scanning of the questionnaires. Thus, 6350 subject questionnaires were included for further analyses.
{kind=link}
Flow chart of study subjects, including subjects excluded and the rationale for exclusion. BMI, body mass index.
Table 1 shows the characteristics of the population in 2013 and 2018.
Study population characteristics in 2013 and 2018 (N=6350)
In 2018, more subjects reported having a degree from a university, while fewer had elementary school as their highest educational level, compared with 2013. The number of subjects reporting daily or occasional smoking was significantly lower in 2018 than in 2013. In the study population, BMI significantly increased from 25.5 kg/m2 to 26.1 kg/m2 over the 5-year study period (p<0.001), and there were more overweight subjects or with obesity. The prevalence of physician-diagnosed asthma increased from 10% to 12% (p<0.001). The frequency of exposure to VGDF in the last 12 months was reduced for all exposure categories, and the ‘never exposed’ category was larger in 2018 than in 2013. In 2013, 104 (3.4%) women were exposed daily and most of the day and 207 (6.7%) were exposed daily but in shorter periods of the day. The corresponding numbers were greater for men at 188 (7.9%) and 298 (12.6%), respectively. Approximately 3% of each question about respiratory symptoms in the last 12 months were missing.
Univariable analyses (table 2) with changes in respiratory burden score as the outcome variable in a linear regression model showed a β-coefficient of 0.05 (95% CI 0.033 to 0.066) for change in BMI.
Results from a series of linear regression models with change in respiratory burden score, with a single exposure variable and also adjusted for baseline respiratory burden score
This means that a one-point change in BMI was associated with an increase of 0.05 points in respiratory burden score. There was no significant association between change in respiratory burden score and age, sex or educational level in 2013. The average respiratory burden score in 2013 was 1.12 (SD: 1.78) and was negatively associated with change in respiratory burden score (β-coefficient −0.46; 95% CI −0.48 to –0.44). Daily smoking was associated with change in respiratory burden score with β-coefficients of −0.39 (−0.52 to –0.27) in 2013 and −0.15 (−0.30 to −0.005) in 2018. Increased smoking was associated with higher respiratory burden score (β=0.21; 0.03 to 0.38), whereas a reduction was associated with reduced respiratory burden score (β=−0.30; −0.45 to –0.16) over time. Change in respiratory burden score was positively associated with change in VGDF exposure, with a β-coefficient of 0.07 (0.03 to 0.11). We found no significant associations between change in burden score and 2013 exposure frequency in the last 5 years. When adjusting for respiratory burden score in 2013, significant associations were found for daily smoking, asthma, obesity in 2013 and daily exposure to VGDF in 2013, as well as change in BMI and VGDF.
Table 3 shows the univariable and adjusted β-coefficients in linear regression models for change in respiratory burden score as an outcome variable and change in BMI or VGDF exposure as the exposure variable.
Model showing change in respiratory burden score as the outcome variable for the full model and stratified by sex and asthma status*
The models were also stratified by sex and physician-diagnosed asthma in 2013. The adjusted full regression models showed an association between change in respiratory burden score and change in BMI, with a β-coefficient of 0.05 (0.04 to 0.07). Stratified by sex, the association was 0.05 (0.03 to 0.07) and 0.06 (0.04 to 0.09) for women and men, respectively, and 0.05 (0.03 to 0.06) and 0.12 (0.06 to 0.18) for subjects without and with asthma, respectively, which differed significantly (p=0.011). The association between change in respiratory burden score and change in VGDF exposure was significant, with a β-coefficient of 0.15 (0.05 to 0.19) in the adjusted full model. In the stratified models, individually, men and women had a significant association, with β-coefficients of 0.18 (0.12 to 0.24) and 0.13 (0.07 to 0.19), respectively, but without differences between sexes. The estimate (β=0.18; −0.02 to 0.38) among subjects with asthma was higher but not significantly different from subjects without asthma (β=0.15; 0.11 to 0.19).
Discussion
In this study, we showed that change in BMI is associated with change in respiratory burden score. This effect was larger in subjects with asthma than in those without. As shown in table 3, for BMI changes, we found an adjusted β-coefficient of 0.05 for change in respiratory burden score. This means a 0.05 increase in respiratory burden score for a one-point increase in BMI. These results suggest that if a subject gains the weight equivalent to an increase in BMI of 10 points (eg, from 25 kg/m2 to 35 kg/m2), this will result in an average increase of 0.5 symptoms in the respiratory burden score. In our study, 24 subjects (0.4%) had a BMI increase ≥10 points. For patients with asthma, the average increase was 1.12 symptoms per 10 BMI points. We observed a positive association between respiratory burden score and VGDF exposure change, but this effect was not affected when stratifying for sex and asthma status. The longitudinal effect of VGDF exposure change was statistically significant, with an adjusted β-coefficient of 0.15 respiratory burden score change for both, all participants and those without asthma. The comparable estimate for subjects with asthma was 0.18 (not statistically significant). These results indicate that a person with asthma only had a slightly greater respiratory burden score increase associated with a VGDF exposure increase.
The univariable analyses (table 2) showed some surprising results; for example, daily smoking in 2013 was negatively associated with change in respiratory burden score, possibly reflecting regression to the mean. Regression to the mean is a statistical phenomenon that can make natural variation in repeated data look like real change and unusually happens when large or small measurements tend to be followed by measurements that are closer to the mean.23 When adjusting for respiratory burden score in 2013, the associations were more as expected, showing the importance of adjusting for respiratory burden scores at baseline.
In line with Ekström et al,5 we found that increased BMI was associated with increased respiratory burden score. However, as the outcomes are different (breathlessness vs burden score), it is difficult to directly compare the estimates. Unfortunately, our study did not contain any questions regarding activity-related breathlessness. Since obese subjects have an increased workload, they may report more breathlessness during activity. However, our respiratory burden score included symptoms at rest and night, indicating symptoms also at rest.
In the stratified model, the adjusted effect estimates for BMI change did not differ between sexes, but subjects with asthma had a higher estimate than those without. This is in line with a previous cross-sectional analysis from the 2013 Telemark study, where subjects with asthma and obesity had higher respiratory burden score compared with subjects with asthma and normal weight.22 Subjects with a distinct obese asthma phenotype report more respiratory symptoms and reduced asthma control and use more asthma medications.24–27 Weight loss in this group has been shown to improve respiratory symptoms and lung function.3
Studies have shown that pulmonary diseases affect sexes differently.28 There seems to be a difference in how men and women perceive respiratory symptoms, and possibly the kind of symptoms they report.29 A previous study has shown that as subjects became obese, male subjects had greater increase in wheezing without a cold, while female subjects had greater increase in asthma.30 In the present study, there was no significant difference between sexes in changes in respiratory burden score with increasing weight. We speculate that this might be attributed to the respiratory symptoms attributed to increased BMI being the same in both sexes or that, in addition, women have other symptoms not reflected in our study. The health response to air pollution has been shown to differ between male and female subjects, but whether this is a result of sex-linked biological differences or exposure pattern differences is unclear.31 Sex differences in respiratory signs and symptoms in occupational settings have been described in a review, but there is little evidence of a clear pattern of susceptibility and the results are not consistent between studies.32 In population-based studies, more consistent sex differences have been found, but whether occupational exposure exacerbates sex differences in respiratory symptoms warrants further research.32 Skorge et al33 showed that exposure to dust, fumes and gas was significantly more strongly associated with an increased incidence of respiratory symptoms in women than in men. In our study, we did not detect any sex difference (p=0.064), but the groups including exposed women were small.
To our knowledge, few studies have investigated how changes in VGDF exposure affect respiratory symptoms in subjects without any respiratory disease. In a Polish follow-up study comparing subjects exposed to dust with those not exposed, a lower OR was found for chronic cough when removing exposure compared with continued exposure.34 Skorge et al33 conducted a follow-up study over 11 years and showed that occupational airborne exposure to dust, fumes and gas is weakly related with the incidence of respiratory symptoms, but significantly more so for women. However, this study did not describe how changes in exposures affect the incidence or prevalence of respiratory symptoms.
Previous studies have shown that VGDF exposure is associated with asthma exacerbation. In a study, severe asthma exacerbation was associated with high occupational exposure to dust, gas and fumes (relative risk (RR) 3.1, 95 % CI 1.9 to 5.1) compared with lack of exposure.11 In a Cochrane review, compared with continued exposure, reduction or removal of exposure for patients with occupational asthma was associated with improvement in symptoms.35 The reduction of exposure increased the likelihood of reporting the absence of symptoms (RR 2.65; 1.24–5.68), while for removal of exposure the RR was 2.80 (1.67–13.86). This review did not include any studies on the improvement of asthma symptoms after a reduction in exposure, while for the removal from exposure the RR was 2.47 (1.26–4.84). In the present study, reduced exposure to VGDF did not lead to a statistically significant improvement in burden score in subjects with asthma. This might be because subjects with asthma included all types of cases, not just those with occupational asthma.
To our knowledge, a well-recognised and validated respiratory burden score for subjects without asthma or other respiratory diseases is not available. However, similar scores including some of the questions in our questionnaire have been used in subjects with asthma or other respiratory diseases.21 22 We developed our score to better describe the burden of respiratory symptoms, including the use of medication, and to reflect a continuum in respiratory symptoms. Contingency table analyses with Cramer’s V test as an effect measure of the association indicated an association among the three wheezing questions, but the other questions in the score had a low level of association (data not shown). When using only one of the wheezing questions in the respiratory burden score, the estimates were as expected lower, but the associations were the same and the reliability was reduced. The respiratory burden score had good internal consistency, with a Cronbach’s alpha value of 0.83. In the 2013 survey, we did not enquire about breathlessness or dyspnoea in the last 12 months, but we included these questions in the 2018 survey. When comparing participants’ respiratory burden score in 2018 with a score including questions on breathlessness, we found that the scores showed high agreement, with an intraclass correlation coefficient of 0.91 (0.90–0.91). The Bland-Altman plot indicates that our respiratory burden score showed less agreement in high scores, probably because one of the scores included more items (symptoms).
Strengths and limitations
A strength of this study is its relatively large and unselected sample from the general population. The study was a prospective study over 5 years using the same questions at baseline and follow-up. Adjusting for important possible confounders, such as smoking, obesity and occupational exposure, is considered another strength. However, there was a significant loss to follow-up (51%) in this study. Online supplemental table 2 shows a comparison between responders (n=7952) and not responders, including those not eligible in 2018 (n=8174). Briefly, there were more men, more current smokers, more subjects with asthma or with lower educational level, and fewer employed in the last 12 months among subjects lost to follow-up compared with those included in the study. The subjects lost to follow-up were also younger and had more respiratory symptoms and current use of asthma medication. The mean BMI was not significantly different, but the distribution by BMI categories showed more overweight or obese subjects among those included. These variables were included and adjusted for in the analysis. Although the differences may have altered prevalence estimates, they were unlikely to have biased the estimates of associations, although such bias cannot be ruled out entirely.
An important limitation of our study was the self-reported outcomes. Even though the questionnaires contained validated questions used in large epidemiological studies on respiratory health, validated questionnaires may improve response accuracy but may still introduce recall bias and random errors. A review found that subjects tend to overestimate height and underestimate weight and BMI when using self-reported data and that this bias is greater in overweight and obese subjects.36 However, the outcome variable used was the difference in BMI, and we have no reason to believe that the bias from self-reported height and weight was substantially different between the two time points. Asthma was defined as self-reported, physician-diagnosed asthma. Using our current study design, we could not verify the diagnosis. However, validation studies of self-reported, physician-diagnosed asthma have found good sensitivity (65%) and high specificity (94%).37 This question is susceptible to misclassification of asthma and COPD among older subjects. To assess this point, we also performed analyses restricted to subjects with asthma onset ≤30 years of age (n=679). The results are shown in online supplemental table 4 and were comparable with the analyses in which all subjects with asthma were included. Underweight (BMI ≤18.5 kg/m2) has been associated with more respiratory disability in other studies. In our study underweight and normal-weight subjects are merged into one category. However, only 1.3% of the subjects reported underweight and excluding underweight subjects from the analyses made minimal difference (online supplemental table 3).
Another limitation is that we did not have direct measurements of occupational exposure for each participant nor information regarding exposure between 2013 and 2017, which could lead to misclassification of exposure. The question refers to the frequency, but the exposure levels may have been reduced after implementing better ventilation, use of personal protective equipment or a change in production methods. However, the question regarding VGDF exposure is commonly used in occupational epidemiology and has been tested against a 16-item battery assessing specific inhalation exposures and a job-exposure matrix, which appears to delineate exposure risk as well as a multiple-item battery and has a modest agreement with the job-exposure matrix.38 39 In this study, we assumed equal steps between exposure frequencies, and that an increase in exposure at one point has an equal but opposite effect on the respiratory burden score as a one-point reduction in exposure. Following this approach, we might have underestimated the effect of reduction of exposure in the most exposed subjects and overestimated the effect of reduction in the least exposed subjects. Another limitation is that approximately 50% of the subjects have never been exposed to VGDF, and 5% were exposed daily and most of the day in 2013 and 7% in 2018. A larger number of subjects in these exposure categories would have contributed to narrower CIs for estimates of association. Future studies should include more respiratory symptom questions, objective measures such as spirometry and more detailed occupational exposure data.
In this study we have shown that respiratory burden in the form of respiratory symptoms and asthma medication use increases with increasing BMI and occupational exposure, but further studies are needed to estimate the clinical effect of this. Weight loss may improve respiratory symptoms by increasing pulmonary function and reducing workload and the low-grade inflammation associated with obesity.1 Similarly, reducing occupational VGDF exposure may reduce respiratory burden by reducing airway inflammation.40
In conclusion, the present study showed that BMI changes and occupational exposure to VGDF were associated with increased respiratory burden score. The change due to increased BMI was not affected by sex, but subjects with asthma had a larger change than subjects without. Increased frequency of VGDF exposure was associated with increased respiratory burden score, but stratified analyses showed no statistical difference between sexes or with respect to asthma status.
Data availability statement
Data are available upon reasonable request. The data sets generated and/or analysed during the current study are not publicly available due to privacy policy regulations but are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Regional Committee for Medical and Health Research Ethics in Norway (REC 2012/1665). Written informed consent was obtained from all study participants. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We wish to thank Gølin Finckenhagen Gundersen, Martin Veel Svendsen and Regine Abrahamsen for participating in data collection and preparation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GK drafted the paper and was involved in study design, data collection, data management, data analyses, data interpretation and accept responsibility for the overall content as guarantor. CB supervised the statistical analyses and was involved in data interpretation and critical revision of the manuscript. PKH, JK, KT and AKMF were involved in study design, data analyses, data interpretation and critical revision of the manuscript. All authors approved the final manuscript.
Funding This work was supported by internal funding from the Telemark Hospital, Norway.
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC). Mention of any company or product does not constitute endorsement by the US Government, NIOSH or CDC.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.