Article Text

Abstract
Background Chronic bronchitis in childhood is associated with a diagnosis of asthma and/or bronchiectasis a few years later, however, consequences into middle-age are unknown.
Objective To investigate the relationship between childhood bronchitis and respiratory-related health outcomes in middle-age.
Design Cohort study from age 7 to 53 years.
Setting General population of European descent from Tasmania, Australia.
Participants 3202 participants of the age 53-year follow-up (mean age 53, range 51–55) of the Tasmanian Longitudinal Health Study cohort who were born in 1961 and first investigated at age 7 were included in our analysis.
Statistical methods Multivariable linear and logistic regression. The association between parent reported childhood bronchitis up to age 7 and age 53-year lung conditions (n=3202) and lung function (n=2379) were investigated.
Results Among 3202 participants, 47.5% had one or more episodes of childhood bronchitis, classified according to severity based on the number of episodes and duration as: ‘non-recurrent bronchitis’ (28.1%); ‘recurrent non-protracted bronchitis’ (18.1%) and ‘recurrent-protracted bronchitis’ (1.3%). Age 53 prevalence of doctor-diagnosed asthma and pneumonia (p-trend <0.001) and chronic bronchitis (p-trend=0.07) increased in accordance with childhood bronchitis severities. At age 53, ‘recurrent-protracted bronchitis’ (the most severe subgroup in childhood) was associated with doctor-diagnosed current asthma (OR 4.54, 95% CI 2.31 to 8.91) doctor-diagnosed pneumonia (OR=2.18 (95% CI 1.00 to 4.74)) and, paradoxically, increased transfer factor for carbon monoxide (z-score +0.51 SD (0.15–0.88)), when compared with no childhood bronchitis.
Conclusion In this cohort born in 1961, one or more episodes of childhood bronchitis was a frequent occurrence. ‘Recurrent-protracted bronchitis’, while uncommon, was especially linked to multiple respiratory outcomes almost five decades later, including asthma, pneumonia and raised lung gas transfer. These findings provide insights into the natural history of childhood ‘bronchitis’ into middle-age.
- clinical epidemiology
- respiratory infection
Data availability statement
Data are available on reasonable request. TAHS is a cohort study with data that has been prospectively collected since 1968 and will be an ongoing resource for future epidemiological analyses. Data collection protocols have been detailed in the TAHS cohort profile paper published in 2016 (Matheson et al. 2016 doi: 10.1093/ije/dyw028). The raw data have not been made widely available, but expressions of interest can be discussed with the corresponding author, JLP and/or principal investigator, SCD, on an individual basis.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Severe early childhood bronchitis manifested by recurrent episodes of protracted wet cough is associated with asthma and bronchiectasis in later childhood.
WHAT THIS STUDY ADDS
This is the first very long-term prospective study that has examined the relationship between childhood bronchitis severity with adult lung health outcomes. ‘Recurrent-protracted bronchitis’ in childhood, while uncommon, was associated with multiple respiratory outcomes in middle-age including asthma, pneumonia and raised lung gas transfer on lung function measurement.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study’s findings support the need for increased vigilance in monitoring young children who have multiple episodes of protracted bronchitis for potential asthma, pneumonia and bronchiectasis up to mid-adult life, confirmed with objective testing.
Introduction
‘Bronchitis’ implies airway inflammation. However, historically, the term bronchitis in childhood has been applied broadly to bouts of coughing without implying a specific cause or diagnosis, for example, asthma or bacterial bronchitis.1 2 Clinicians have previously believed that ‘wheezy bronchitis,‘on the other hand, signifies asthma.3 However, the terminology and understanding of the causes of paediatric cough has since evolved significantly and the paradigm has changed. It is now recognised and accepted that ‘chronic cough’ in children, that is, cough lasting >4 weeks, can be caused by a range of pathologies including protracted bacterial bronchitis (PBB), bronchiectasis, asthma and tracheo/bronchomalacia. Furthermore, wheeze and cough can be common to all of these conditions.3 4
PBB, also known as chronic bacterial bronchitis, is recognised as a discrete diagnostic entity by Respiratory Societies across Europe,5 the USA6 and Australia/New Zealand. PBB is defined as presence of a chronic ‘wet’ cough that lasts 1 month or more and resolves with 2–4 weeks of appropriate antibiotic therapy, in the absence of indicators to suggest another cause for the cough.7 8 Prospective paediatric cohort studies have described a link between PBB and both bronchiectasis and asthma, with 27% of children with PBB having an asthma phenotype 5 years later9 and 8%–10% having bronchiectasis within 2–5 years.9 10 Whether chronic bronchitis (CB) in childhood is associated with poor lung health in adulthood is unknown and represents an important research priority, with potential to improve outcomes through earlier recognition and management.5
Longitudinal cohort studies from early life to adulthood have provided important insights into lung disease development11 and are closing the gap in understanding between paediatric and adult respiratory medicine.12 While several studies have supported the role of early life exposures in adult lung function deficits and chronic obstructive pulmonary disease (COPD),13–18 the early origins of adult chronic productive cough (or CB) remain poorly understood and sparsely studied.19
Using population-based data from our Tasmanian Longitudinal Health Study (TAHS) longitudinal cohort, we aimed to investigate trends and associations between bronchitis severity at age 7 in childhood and respiratory health outcomes of asthma, CB, pneumonia and lung function in middle-age at age 53.
Methods
Study design and population
Our study sample included participants of the TAHS cohort (1968–2016) who took part in the original assessments at age 7 and were followed up at the mean age of 53 years (details published elsewhere18 20–22). Tasmania is an island State of Australia located 240 km to the south of the Australian mainland, which is the least populated and marginally the poorest state by gross product per capita, with relatively high rates of smoking and historically, less accessible healthcare facilities for a developed country. Briefly, this population-based cohort of participants essentially from European descent were born in 1961 and first studied including retrospective questionnaire data in 1968 (aged 6–7 years, n=8583), was retraced (n=7312) and resurveyed by a postal survey questionnaire in 2004 at mean age 43 years (n=5729) with further clinical testing. Subsequently, 6127 (71.4%) of the full original cohort were retraced and invited to participate in a clinical follow-up between 2012 and 2016. At mean age=53, 3609 (58.9%) respondents completed the questionnaire and 2719 (43.9%) underwent lung function testing including prebronchodilator/postbronchodilator spirometry and lung gas transfer measurements, on average 46 years later (figure 1). To minimise lost to follow-up, methods of tracing included computer linkage to the National Death Index, Commonwealth Electoral Roll, Medicare database, Tasmanian marriage records,23 and via siblings and parents who were also part of the original 1968 survey, and multiple attempts at contacting participants may have been required. Over 70% of the original participants still resided in Tasmania, with migration mainly to the East Coast of Australia and fewer than 0.5% now living overseas.
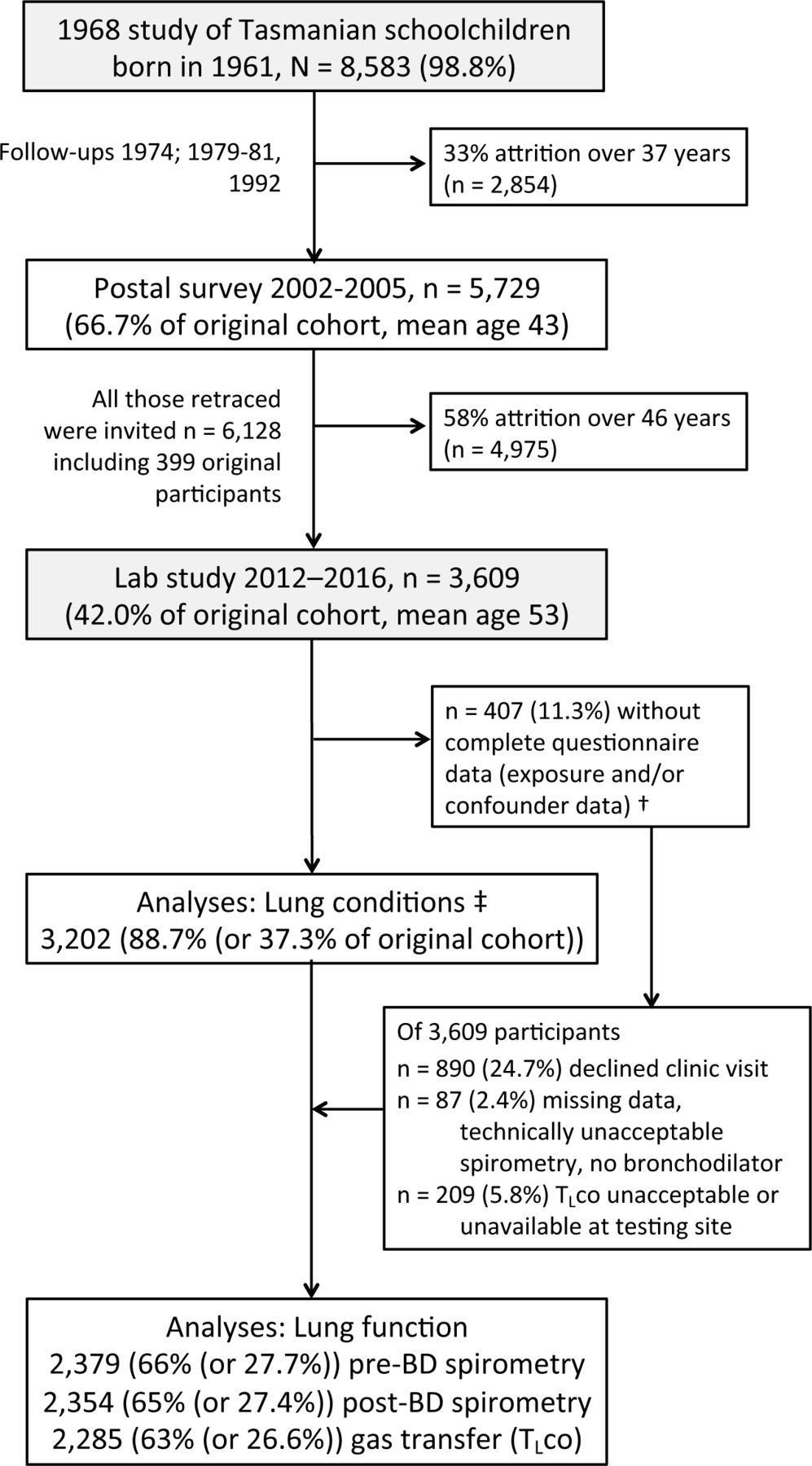
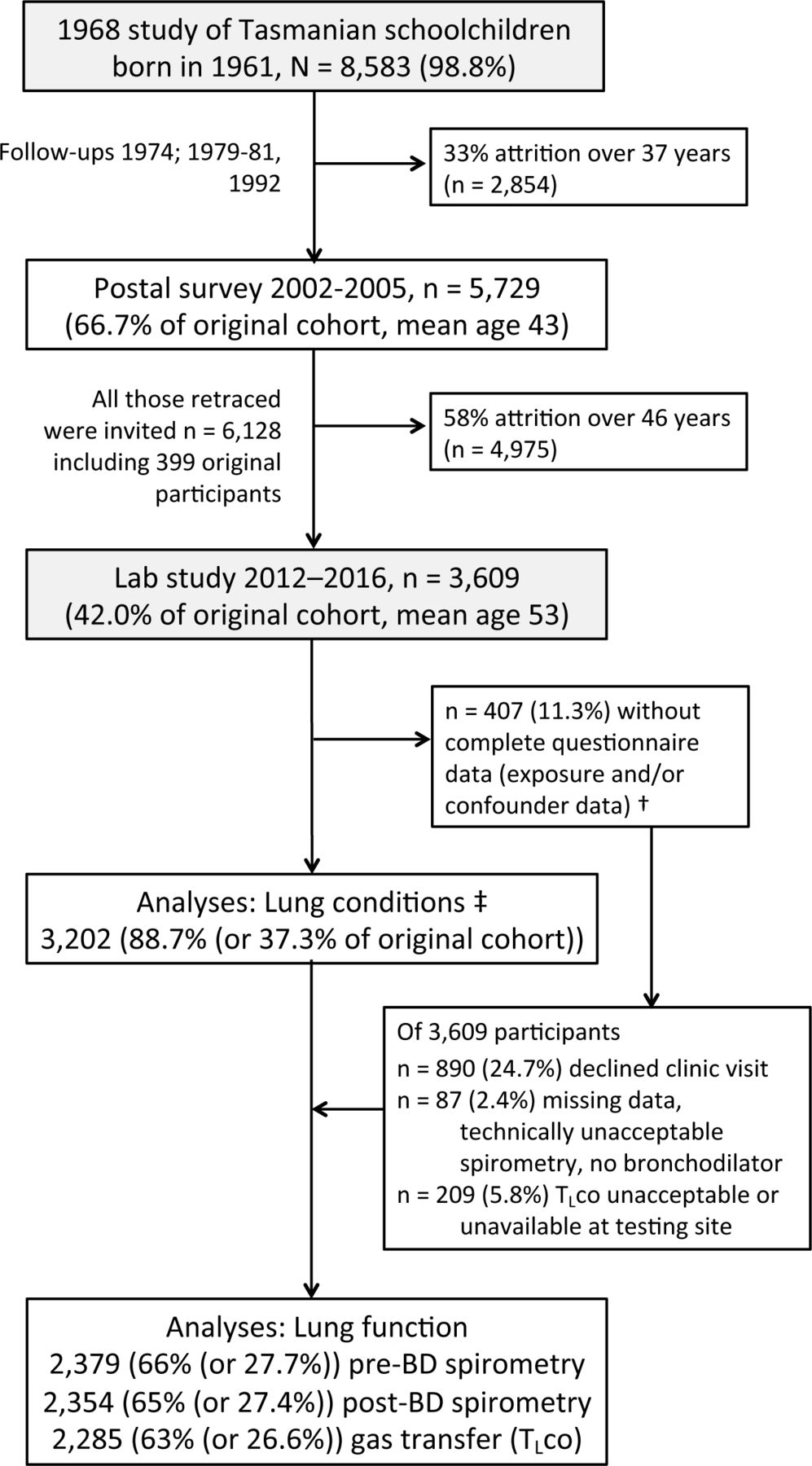{kind=link}
TAHS participants 1968–2016 study participants were those who attended both the 7 and 53 years follow-up visits and had complete questionnaire data and technically acceptable lung function measurements. Regression numbers varied with each outcome (n=3062–3196)†‡. post-BD, post-bronchodilator; TAHS, Tasmanian Longitudinal Health Study; TLco, transfer factor for carbon monoxide of the lung.
Data collection methods
Details of lung function testing have been described22 and summarised in online supplemental methods E1a. Lung function testing was standardised across testing sites in accordance with the 2005 American Thoracic Society/ European Respiratory Society (ATS/ERS) standards.24 25 For this analysis, lung function data at age 7 and 53 years were converted to z-scores (ie, SD or SD units) using established standard reference values.26 27 Airflow obstruction was defined by forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <lower limit of normal (LLN), and spirometric restriction by post-BD FVC <LLN and FEV1/FVC ≥LLN.
Supplemental material
Definition
Exposure
Childhood bronchitis (or ‘wet’ cough as current clinical definitions) was defined by an affirmative response by parents/guardian to the 1968 survey question by age 7: ‘Has he/she at any time in his/her life suffered from attacks of bronchitis or attacks of cough with sputum (phlegm) in the chest (‘loose’ or ‘rattly’ cough)?’. Based on the number of episodes and duration of attacks, those with childhood bronchitis was divided into three severity groups based on predetermined categories at the time of the 1968 survey: the non-recurrent subgroup had between one and five episodes only of any duration; the recurrent group had ≥6 episodes lasting <1 month on average; and the recurrent-protracted subgroup had either ‘continuous’ symptoms or ≥6 episodes each lasting an average of a month or more.
Outcomes
Adult lung conditions, current CB, which was a subset of those reporting ever-CB, was defined by the presence of a ‘usual’ cough with sputum (phlegm) for at least 3 months for the last two consecutive years at age 53. Asthma—current at age 53 was defined by a past doctor diagnosis of asthma associated with asthma-like symptoms, asthma medication use and/or related healthcare utilisation within 12 months prior to testing.
Online supplemental methods E1b provides further details for the exposure, other outcomes, confounders and effect modifier/s.
Statistical methods
Analyses were carried out using Stata (V.16, Stata). Our exposure, CB, included four categories as defined above, that is, no CB, non-recurrent bronchitis, recurrent non-protracted bronchitis, and recurrent-protracted bronchitis. Univariable trends of continuous/categorical respiratory outcomes were examined across these ordered categories (non-parametric trend tests (nptrend)28/univariable logistic regression, respectively). This latter trend estimate approach assumes the relationship between the exposure expressed as an ordered variable attached to numerical values is linearly related to the outcome.
Using complete cases, multivariable linear and logistic regression were used to examine associations between CB and with continuous and categorical respiratory outcomes respectively. For the lung function outcomes, the regression coefficients represented the associations between exposure categories and lung function values expressed as z-scores (SD units) which accounted for age, sex and height (online supplemental methods E2a).26 27
We chose ‘no childhood bronchitis’ as the reference exposure category so differences between categories of childhood bronchitis severity were only relative to the reference group and not compared directly. To interpret differences between childhood bronchitis categories, the absolute numbers of participants estimated to have the lung condition at age 53 were calculated using the ‘margins’ command following the syntax for the separate multivariable regression analyses.
Informed by conceptualising the models using a directed acyclic graph,29 30 regression models were adjusted for paternal occupation, parental bronchitis, rurality of primary school, number of siblings and parental smoking when participants were aged 7, plus male/female for the non-lung function analyses (online supplemental methods E1b and E2b).
Childhood asthma, pneumonia-pleurisy and pre-BD FEV1 at 7 years (ie, non-discriminatory for obstructive and restrictive lung function deficits) partly mediated relationships of corresponding adult outcomes as per causal mediation analyses (online supplemental methods E2c, table E1), thus were not included as model covariates. Mediation by FEV1/FVC was possible but was not additionally performed. As childhood asthma/wheezing, ever-smoking and participant sex could plausibly strengthen the exposure/outcome relationships, corresponding interaction terms were used for the following reasons: to exclude the possibility that adult asthma was only related to participants who also wheezed in childhood; to assess whether the association with adult CB was related to adult cigarette smoking; and, because of known sex differences in lung function and asthma development. Sensitivity analyses that excluded participants who self-recalled asthma-ever and doctor-diagnosed pneumonia-ever before age 7 were performed (referred to as ‘recalled’ asthma and pneumonia, respectively).
A cut-off of p<0.10 for interactions was used to assess for effect modification as this was a low powered statistical test. A z-score of >0.5 SD27 and absolute increase in FEV1 of 200 mL and 12% post-BD were considered clinically significant.31
Patient and public involvement
Patients, TAHS participants or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Childhood sociodemographic and clinical characteristics
Among 3202 participants who had complete questionnaire data when aged 53, 47.5% had one or more episodes of childhood bronchitis (table 1). The prevalence of non-recurrent and recurrent but non-protracted bronchitis was 28.1% (95% CI 26.6% to 29.7%) and 18.1% (95% CI 16.7% to 19.4%), respectively. The prevalence of 1.31% (95% CI 0.94% to 1.77%) for recurrent-protracted bronchitis was similar to that of the 2379 participants with complete lung function data (1.18% (95% CI 0.78% to 1.70%), online supplemental table E2) and the original 1968 cohort (1.21% (95% CI 0.98% to 1.47%), where n=101 of n=8583 = 1.18%).
Sociodemographic and clinical characteristics at age 7 of the middle-aged TAHS participants who formed the study sample for the current analysis
Minor differences in baseline characteristics at age 7 for those who did not participate in the subsequent follow-up and/or who had missing data at age 53 were seen, namely males of lower socioeconomic status were less likely to have data available (online supplemental results E1, table E2a). The differences between exposure groups and subsequent participation were also only modest, especially for the recurrent-protracted subgroup for which the percentages participating and not participating varied between 1.2% and 1.3%. There was little difference in the prevalence of doctor-diagnosed asthma as a proxy outcome at mean age 43 years, and the reduced participation by those with self-reported CB was not significant (online supplemental table E2b).
At age 7, participants with recurrent childhood bronchitis, with or without protracted episodes, were more likely to be male (table 1). Children with a history of bronchitis trended to have fewer siblings and fewer mothers of the recurrent-protracted group smoked regularly. Positive trends were seen across the childhood bronchitis severity subgroups with regard to an increasing prevalence of parental bronchitis and/or symptoms, coexistent asthma/wheezing (ever and recurrent) and doctor-diagnosed pneumonia and/or pleurisy (p-trend <0.001, table 1).
Middle-age sociodemographic and clinical characteristics
Similar positive trends across the childhood bronchitis severity subgroups were observed between and the actual and estimated prevalence of asthma-ever, current asthma and pneumonia-ever by middle-age (p-trend <0.001, tables 2 and 3, respectively). While the proportions of usual cough, usual phlegm at age 53 were higher in the recurrent-protracted group, trends did not attain statistical significance. Nevertheless, the prevalence for current CB was 2.4-fold higher in this severe compared with the no childhood bronchitis subgroup (12.0% compared with 5.0%, respectively, p-trend=0.07).
Sociodemographic and clinical characteristics at age 53 of TAHS participants
Estimated prevalence of lung conditions by childhood bronchitis severity, adjusted for confounding variables
The prevalence of current smoking in individuals at age 53 was similar across childhood subgroups (~17%), although a disproportionately high percentage of participants in the recurrent-protracted group had ever-smoked (83% compared with ≤60%, table 2). Clear positive trends across childhood bronchitis severity-subgroups were also seen for transfer factor of the lung for carbon monoxide (TLco) and its coefficient (Kco) with a modest inverse trend for alveolar volume. There were similar trends for lower pre- and post-bronchodilator FEV1 and FEV1/FVC at age 53(p-trend between 0.005 and 0.042, table 2). These trends were somewhat stronger when participants underwent spirometry when aged 7 (pre-BD FEV1 p-trend=0.004; FEV1/FVC p-trend <0.001).
Main associations
Using multivariable regression, compared with no childhood bronchitis, all three childhood bronchitis (non-recurrent, recurrent non-protracted and recurrent-protracted) subgroups were associated with both doctor-diagnosed current and ever-asthma in middle-age. These associations increased in strength in a dose response manner as severity increased (table 4). Compared with no bronchitis, increasing childhood bronchitis severity was associated with recalled doctor-diagnosed pneumonia after 7 years (p=0.032, p<0.001, p=0.05, respectively).
Multivariable main associations between increasing childhood bronchitis severity by age 7 and various lung conditions at age 53 years
For spirometry outcomes at age 53, compared with no childhood bronchitis, associations were observed for the recurrent (non-protracted) childhood bronchitis subgroup with regards to a significant association with pre-BD airflow obstruction and lower post-BD FEV1/FVC taken as a continuous variable and paradoxically, a borderline association with spirometric restriction (table 5). Recurrent-protracted childhood bronchitis was associated with significantly higher levels of TLco and Kco but not alveolar volume in middle-age.
Multivariable main associations between increasing childhood bronchitis severity by age 7 and lung function at age 53 years
Effect modification
Among those without childhood asthma/wheezing, the odds for current asthma at age 53 were higher for participants with recurrent-protracted childhood bronchitis (OR 4.29 (95% CI 1.45 to 12.6), p=0.008), p-interaction=0.063, online supplemental table E3) although case numbers in the recurrent-protracted subgroup were relatively few (5-10 cases).
To contrast the above-mentioned finding, interactions were consistently seen between childhood bronchitis and childhood asthma/wheezing with regards to lung function measures used as continuous variables in middle-age, namely pre-BD FEV1, change in FEV1 post-BD, pre-BD FEV1/FVC, and post-BD FEV1/FVC (p-interaction <0.1, online supplemental results E2, table E4). When the analysis was stratified by presence of childhood asthma/wheezing, compared with no childhood bronchitis, only participants with 1–5 episodes of any duration (ie, non-recurrent group) had non-obstructive lung function changes: reduced post-BD FVC (z-score –0.42 SD (95% CI –0.72 to –0.12), p=0.006), increased pre-BD FEV1/FVC (+0.43 (95% CI +0.11 to +0.74), p=0.008) and post-BD FEV1/FVC (+0.33 (95% CI +0.01 to +0.66), p=0.043) despite an increased pre-BD FEV1. There was also an associated threefold decrease in the odds for pre-BD airflow obstruction (OR 0.34 (95% CI +0.14 to +0.87), p=0.024), but there were too few cases to assess spirometric restriction as the outcome.
Despite few case numbers for the recurrent-protracted childhood bronchitis subgroup, associations with pneumonia-ever by age 53 were still seen for females (online supplemental results E3, table E5) and with current CB for middle-aged non-smokers (online supplemental results E4, table E6).
Discussion
Using data from our whole-of-community cohort of European descent born in 1961, parent-reported childhood ‘bronchitis’ (and/or coughing phlegm, or ‘loose or rattly’ cough) was associated with consequential lung outcomes in middle-age, with significant trends for doctor-diagnosed asthma and pneumonia across the spectrum of cough-severity. Associations with doctor-diagnosed asthma and pneumonia were especially evident for the most severe subgroup termed ‘recurrent-protracted childhood bronchitis’. The findings of a low prevalence of CB and substantially higher lung gas transfer in mid-adult life for this subgroup have not previously been described. Similarly, the main association with a mixed obstructive/restrictive lung function pattern of modest magnitude for the subgroup with non-recurrent bronchitis episodes was also unexpected and probably not clinically important. Overall, we provide evidence to support childhood bronchitis as a contributor to clinical lung disease in mid-adult life, especially when chronic, recurrent and protracted.
Unexpectedly, a history of recurrent-protracted bronchitis in childhood was not strongly associated with CB is middle-age. Therefore, we postulate that only a relatively small subgroup at most may have had persistent productive cough episodes spanning childhood to mid-adult life, with adult CB mainly influenced by two age-related factors. Analogous to asthma remission that is common in later childhood and adolescence, most children seem to ‘grow out of’ bronchitis during their late childhood or early adolescent years9 32 that could be in part explained by immune system maturation.33 34 Equally, CB most commonly develops during the productive working years of an adult resulting from environmental exposures e.g. cigarette smoking and/or air pollutants in the workplace,35 36 which is in keeping with CB-onset in adulthood.
Interestingly, among those most affected by childhood bronchitis, we found associations with current asthma in middle-age which were evident even for participants without a history of childhood asthma/wheezing at age 7. This suggests that a predisposition to multiple and protracted episodes of childhood bronchitis could lead to damaged airways, and that a degree of airway narrowing from remodelling could impair normal airway development to manifest as symptomatic asthma in later life.37 As we were unable to tease out the precise overlaps between PBB, virus-associated wheeze and classic allergic asthma with regard to childhood wheezing, this prompted us to perform the analysis within strata of childhood asthma/wheezing. In this interaction analysis, we were still able to detect a significant association between the severe recurrent-protracted bronchitis subgroup and adult asthma for those who did not have parent-reported asthma and/or wheezing in childhood, suggesting the observed association could be independent of childhood asthma.
In contrast, we also found lung function deficits, for example, decrease in the odds for airflow obstruction for the subgroup with non-recurrent bronchitis episodes and coexistent childhood asthma/wheezing, but there was limited power to detect coexistent spirometric restriction. While we cannot draw firm conclusions, these findings are consistent with the Tucson Children’s Respiratory Study (TCRS). The TCRS accurately defined ‘other lower respiratory illnesses (LRIs) by age 3’ after excluding radiologically confirmed pneumonia and found a main association with active wheeze but not physician-diagnosed asthma by age 30 (n=738), however, did not stratify analyses by childhood asthma/wheeze status.38 These authors also found consistent reductions in FEV1 and FVC of around 120 mL prebronchodilator and postbronchodilator in those with LRIs in early life, which could predispose individuals to COPD with a normal age-related decline if peak lung function was not attained from impaired lung function growth due to adverse exposures in utero and early childhood.13–18 39 The latter lung function finding is also consistent with our previous study that investigated the long-term outcomes of doctor-diagnosed childhood pneumonia and/or pleurisy and showed a restrictive lung function pattern on measures of static lung volumes in middle-age.22
The observed ‘physiologically relevant’ elevations in lung transfer factor levels27 in the absence of increased alveolar volume for the severe recurrent-protracted subgroup could plausibly relate to the high observed prevalence of coexistent asthma/wheezing in childhood40 and adulthood.41 42 However, this finding also raises the possibility of a vascular mechanism like that seen in bronchiectasis in which broncho-pulmonary anastomoses derived from an expansion of a collateral and high-pressure bronchial artery network diverts pulmonary artery blood flow away from diseased parts to better supply the normal lung,43 although the increase in bronchitic symptoms was only modest. Interestingly, lung transfer factor (TLco) can be high for adult patients at their first clinical presentation with bronchiectasis, which could be a feature prior to an accelerated decline which typically accompanies disease progression.44
Our detailed questioning of parents of the 7 year-old children from a whole-of-community population allowed us to identify a severe subgroup that probably resembles PBB as closely as was possible without having data on antibiotic therapy and its response, given PBB was not defined until 2016.7 Notably, 8%–10% of children with PBB are complicated by bronchiectasis within the next 5 years,9 10 which raises the possibility that some positive auscultatory signs heard by a medical practitioner who diagnosed pneumonia during an acute respiratory illness could rather have actually been bronchiectasis in our most severe subgroup and high resolution CT scans would have ideally been performed to investigate this hypothesis.45 Nonetheless, the awareness of PBB as a treatable and preventable cause of bronchiectasis is crucial especially for some socially disadvantaged communities, for example, Indigenous Australian populations.
The main strength of our TAHS cohort is the prospective, longitudinal data collection over five decades used to evaluate relationships between childhood respiratory health and long-term respiratory outcomes. The comprehensive questioning allowed us to create severity categories for childhood cough phenotypes that identified some severity–outcome relationships which strengthens the argument for a causal association. Although the severe subgroup with recurrent-protracted childhood bronchitis was small in this general population sample, there was sufficient statistical power to detect significant associations with long-term outcomes enhanced by a large reference group without bronchitis in childhood.
Regarding limitations, our study relied on parental report of their children’s health at age 7 and self-report of doctor-diagnosed conditions at mean age 53. We acknowledge the potential for misclassification of childhood bronchitis (and asthma/wheezing), which could have been overestimated or underreported by parents according to its severity, but this misreporting of information across multiple exposure groups would bias estimates towards the null as such misclassification is more likely to be non-differential. There was also potential for differential misclassification of the self-reported adult lung conditions by exposure status. However, with the 46-year lag between exposure and outcome measurements and the likelihood of multiple intervening life events, such differential reporting by participants seemed unlikely. While a typical pattern of attrition was observed for males of lower socioeconomic class, the possibility of collider bias (from inappropriately controlling for a collider variable that is influenced independently by both the exposure and outcome) is not likely because the prevalence of proxy outcomes 10 years earlier were largely unaffected and the loss to follow-up was similar between the exposure groups. Although several hypotheses were tested, these were predetermined by their biological plausibility based on previous literature9 10 19 22 and so we interpreted the general pattern of results rather than focusing on individual p values or using a Bonferroni correction. Finally, the Australian participants included in this study were almost exclusively of European ethnicity and in this era (born 1961) were not routinely immunised against common childhood pathogens, for example, measles, pneumococcus and Haemophilus influenzae type B. This may limit the generalisability of our findings to later birth cohorts and other ethnic groups in the vaccination era.
Conclusion
In summary, our findings suggest associations between childhood ‘bronchitis’ and doctor-diagnosed pneumonia and asthma in adulthood, especially evident for the recurrent-protracted subgroup, with trends across the spectrum of cough severity. The elevation of lung gas transfer in middle-age for this recurrent-protracted group is interesting and may be explained by asthma, chronic vascular changes and/or mild bronchiectasis; where possible, replication in other similar cohorts and further research to establish its clinical significance is warranted. Collectively, these findings provide novel insights into the potential natural history of severe bronchitis in children. Importantly, they support initiatives to enhance awareness among primary care physicians to promote the timely diagnosis and management of protracted episodes of cough in children with close monitoring for subsequent development of asthma and other complications such as bronchiectasis.
Data availability statement
Data are available on reasonable request. TAHS is a cohort study with data that has been prospectively collected since 1968 and will be an ongoing resource for future epidemiological analyses. Data collection protocols have been detailed in the TAHS cohort profile paper published in 2016 (Matheson et al. 2016 doi: 10.1093/ije/dyw028). The raw data have not been made widely available, but expressions of interest can be discussed with the corresponding author, JLP and/or principal investigator, SCD, on an individual basis.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Human Ethics Review Committees at all participating institutions, principally the Universities of Melbourne (040375) and Tasmania (H0012710). Written informed consent was obtained from all participants.
Acknowledgments
We acknowledge the TAHS study participants and previous investigators, Drs Heather Gibson, Bryan Gandevia, Harold Silverstone and Norelle Lickiss. We thank Professors Mark Jenkins (Centre for Epidemiology & Biostatistics, VIC), Alan James (Sir Charles Gardner Hospital, WA), Peter Frith (Flinders University, SA), Graham Giles (Cancer Council Victoria), A/Prof David Johns (UTAS) and Richard Wood-Baker (Royal Hobart Hospital, TAS), and Drs Melanie Matheson (University of Melbourne, VIC), Iain Feather (Gold Coast Hospital, QLD), James Markos (Launceston General Hospital, TAS) and Geza Benke (Monash University, VIC), who are investigators of TAHS but not coauthors of this manuscript, for their assistance with obtaining funds and data collection. We also acknowledge all the study site coordinators and respiratory scientists who collected data in the lung function laboratories of Tasmania, Victoria, Queensland and New South Wales; the research interviewers and data entry operators; and the organisational roles of Ms Cathryn Wharton and Dr Desiree Mészáros. Furthermore, we thank the late Dr Stephen Morrison (University of Queensland) for his assistance with obtaining funds/ data collection. Finally, we thank the Archives Office of Tasmania for providing data from the 1968 and 1974 TAHS questionnaires and copies of the school medical records.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ABC and SCD are joint senior authors.
Contributors The authors alone are responsible for the content and writing of the article. SCD, EHW, MJA, JLH, PST, GH, BE, LG and JLP were involved in acquiring funding and/or establishing study directions and protocols. The data was acquired by SCD, EHW, MJA, PST and BRT. JLP led the analysis and interpretation of data with support especially from SCD, DW and ABC, as well as MAR, AJL, CJL, DSB and GB. JLP wrote the initial draft of the manuscript, which was critically revised for important content by all authors, especially DW, ABC and EHW. All authors approved the submission of the manuscript. JLP is acting guarantor who accepts full responsibility for the work and/or conduct of the study, had access to the data, and controlled the decision to publish.
Funding The TAHS was supported by the National Health and Medical Research Council (NHMRC) of Australia, research grants 299901 and 1021275; the University of Melbourne; Clifford Craig Foundation; the Victorian, Queensland and Tasmanian Asthma Foundations; Royal Hobart Hospital; Helen MacPherson Smith Trust; and GlaxoSmithKline. JP, AL, ABC and SCD are funded through the NHMRC of Australia. DW is funded by a fellowship from the NHMRC CRE in bronchiectasis (AusBREATHE). ABC is also supported by the Queensland Children’s Foundation.
Competing interests JP, AL, CL, DB, EHW, MJA and SCD have received an investigator-initiated grant from GlaxoSmithKline for unrelated research, and SCD holds a similar grant from AstraZeneca. MJA also holds investigator-initiated grants from Pfizer, Boehringer-Ingelheim and Sanofi for unrelated research; has undertaken an unrelated consultancy and received assistance with conference attendance from Sanofi; and received a speaker’s fee from GlaxoSmithKline. ABC is on independent data safety and monitoring boards for a SARs-COV2 vaccine (Moderna), an unlicensed RSV vaccine (GSK) and monoclonal antibody (AstraZeneca), where the monies are received by her institution. BRT serves on the medical advisory boards of Chiesi Australia and 4D Medical and has received an unrelated consultancy from GlaxoSmithKline and speaker fees from Mundipharma. AL has received investigational product (EpiCeram TM) free of charge from Primus Pharmaceuticals for use in unrelated research. DW has received consultancy fee from MSD for participation on an expert input forum, outside the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.