Article Text

Abstract
Background Past exposure to secondhand tobacco smoke (SHS) is associated with exercise limitation. Pulmonary factors including air trapping contribute to this limitation but the contribution of cardiovascular factors is unclear.
Objective To determine the contribution of cardiovascular mechanisms to SHS-associated exercise limitation.
Methods We examined the cardiovascular responses to maximum-effort exercise in 245 never-smokers with remote, prolonged occupational exposure to SHS and no known history of cardiovascular disease. We estimated the contribution of oxygen-pulse (proxy for cardiac stroke volume) and changes in systolic blood pressures (SBP), diastolic blood pressures and heart rate (HR) towards exercise capacity, and examined whether the association of SHS with exercise capacity was mediated through these variables.
Results At peak exercise (highest workload completed (WattsPeak)=156±46 watts (135±33 %predicted)), oxygen consumption and oxygen-pulse (O2-PulsePeak) were 1557±476 mL/min (100±24 %predicted) and 11.0±3.0 mL/beat (116±25 %predicted), respectively, with 29% and 3% participants not achieving their predicted normal range. Oxygen saturation at peak exercise was 98%±1% and remained >93% in all participants. Sixty-six per cent showed hypertensive response to exercise. In models adjusted for covariates, WattsPeak was associated directly with O2-PulsePeak, HRPeak and SBPPeak and inversely with SHS, air trapping (residual volume/total lung capacity) and rise of SBP over workload (all p<0.01). Moreover, SHS exposure association with WattsPeak was substantially (41%) mediated through its effect on O2-PulsePeak (p=0.038). Although not statistically significant, a considerable proportion (36%) of air trapping effect on WattsPeak seemed to be mediated through O2-PulsePeak (p=0.078). The likelihood of having baseline respiratory symptoms (modified Medical Research Council score ≥1) was associated with steeper rise in SBP over workload (p<0.01).
Conclusion In a never-smoker population with remote exposure to SHS, abnormal escalation of blood pressure and an SHS-associated reduction in cardiac output contributed to lower exercise capacity.
- lung physiology
- tobacco and the lung
- exercise
- COPD ÀÜ mechanisms
Data availability statement
The data sets generated and analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prolonged past exposure to secondhand tobacco smoke is associated with exercise limitation. Pulmonary factors including air trapping contribute to this limitation but the contribution of cardiovascular factors is unclear, as is the interaction between pulmonary and cardiovascular systems in this setting.
WHAT THIS STUDY ADDS
Healthy never-smokers with history of remote exposure to secondhand tobacco smoke have an abnormal cardiovascular response to exercise, which is characterised by a stroke volume and thus an exercise capacity that are reduced proportional to their years of exposure to secondhand tobacco smoke.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The abnormal cardiovascular response to exercise in this population reveals the presence of an occult or subclinical pathology that impairs the cardiopulmonary functional reserve and reduces the efficiency of body’s oxygen delivery machinery, which could be disadvantageous during the times of increased cardiopulmonary output demands as in physiological distress or disease.
Introduction
Secondhand tobacco smoke (SHS) remains a major public health problem.1 2 Although SHS exposure among non-smokers in the USA has declined from 88% in 1988 to 25% in 2014, the rate of decline has plateaued with one in four non-smokers, including 14 million children, continuing to be exposed to SHS annually between 2011 and 2014.3 The consequences of such substantial continued exposure may now be more manifest as the generations that endured the highest levels of SHS exposure grow older. In particular, advancing age could aggravate or unmask SHS-related health problems that may have been previously too subtle to be recognised.
Although immediate health effects of exposure to SHS have been studied,4–9 its long-term consequences, particularly the effect of remote exposures, have been more difficult to examine in part because of challenges with exposure assessment. Never-smoking flight crews who worked on commercial aircrafts before the enactment of the smoking ban were exposed to heavy SHS in aircraft cabin for many years, in a range similar to the nicotine exposure burden experienced by ‘light’ smokers.10 11 The regularity of this intense exposure in the cabin work environment lends itself to relatively accurate SHS exposure quantification through employment history.12 This makes the exposed flight crews a unique population in which the long-term health effects of previous exposure to SHS can be examined as a form of ‘natural’ experiment that is also generalisable to other SHS-exposed populations.
In previous studies of never-smoking flight crews with a history of remote but prolonged exposure to SHS in aircraft cabins, we examined the pulmonary health effects of long-term exposure to SHS. These studies showed an association of adverse pulmonary outcome measures with the number of years during which flight crews were exposed to SHS in aircraft cabins.12–14 While this never-smoking SHS-exposed cohort had no evidence of spirometric chronic obstructive pulmonary disease (COPD) (a preserved ratio of forced expiratory volume in 1 s to forced vital capacity), they had abnormal lung function measures that were suggestive of presence of an occult early/mild obstructive lung disease.14 In the current study, we wished to examine the cardiovascular health effects of remote but prolonged exposure to SHS in this never-smoking cohort with evidence of early obstructive lung disease. We hypothesised that in addition to impacting pulmonary mechanisms (eg, air trapping), prolonged exposure to SHS contributes to exercise limitation through its adverse cardiovascular health effects. To evaluate this hypothesis, we analysed the cohort’s cardiovascular response to maximum effort cardiopulmonary exercise testing.
Methods
Study overview
This was a prespecified analysis of data collected as part of the Secondhand Smoke Respiratory Health Study, an observational cohort study of non-smoking participants with a range of occupational SHS exposure, as previously described.12–14 Briefly, between July 2007 and July 2015, we recruited US airline flight crewmembers with a history of occupational exposure to SHS, along with non-smoker controls without such occupational exposure, who were participating in a larger study of cardiopulmonary health effects of prolonged remote exposure to SHS.14 The participants were characterised by respiratory symptom questionnaires, full pulmonary function testing and a maximum effort cardiopulmonary exercise testing (CPET). We used the data from this cohort to perform a prespecified analysis to determine the associations among exercise capacity (highest workload completed (WattsPeak in Watts), volume of oxygen uptake at peak exercise (VO2Peak in L/min) and cumulative work achieved (WorkTotal in Watts-Minutes)), cardiovascular responses to maximum effort CPET (oxygen-pulse (O2-Pulse; a proxy for cardiac stroke volume), systolic and diastolic blood pressures (SBP and DBP) and heart rate (HR)), years of airline employment during which the participants worked in smoky cabin (cabin SHS exposure) and their interactions with each other as well as with air trapping (ratios of residual volume, or functional residual capacity, to total lung capacity; RV/TLC or FRC/TLC), which we had previously shown to be associated with exercise capacity (WattsPeak and VO2Peak).
Study population
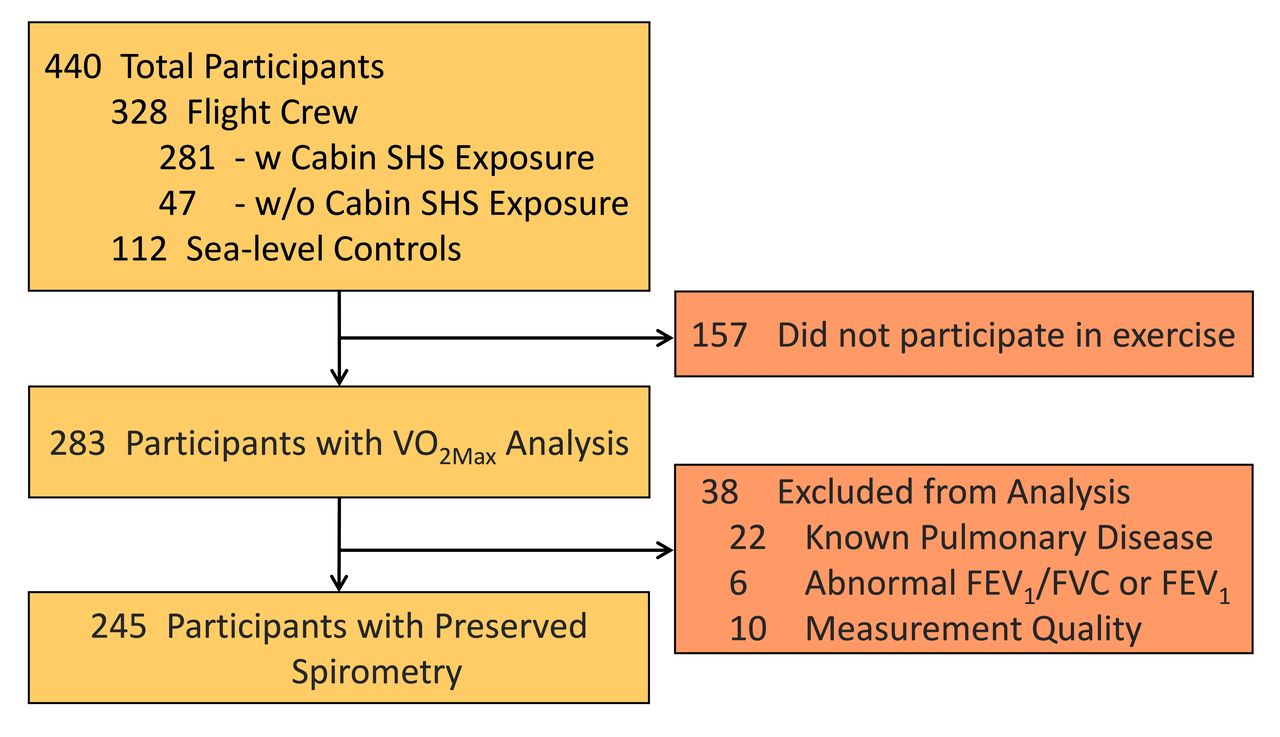
The Secondhand Smoke Respiratory Health Study recruited the USA airline flight crewmembers as part of an investigation of the potential adverse health effects of the cabin environment on those employed before and after introduction of the ban on smoking in US commercial aircraft. Crewmembers were eligible to participate in the study if they had worked ≥5 years in aircraft. A referent group of ‘sea-level’ participants who lived in the San Francisco Bay area and had never been employed as airline crewmembers was also recruited. All participants were non-smokers defined by never-smoking or, in ever smokers, a cumulative history of smoking <20 pack-years and no smoking for ≥20 years prior to enrolment. Participants with known history of pulmonary disease (such as asthma or COPD) or cardiovascular disease (such as coronary artery disease or heart failure) were excluded. Participants with known history of hypertension were included if their blood pressure was medically controlled as defined by SBP ≤145 and DBP ≤90 mm Hg at the time of visit. Overall, out of the 283 participants who underwent CPET, 245 individuals were included in this analysis after such exclusions (figure 1).14
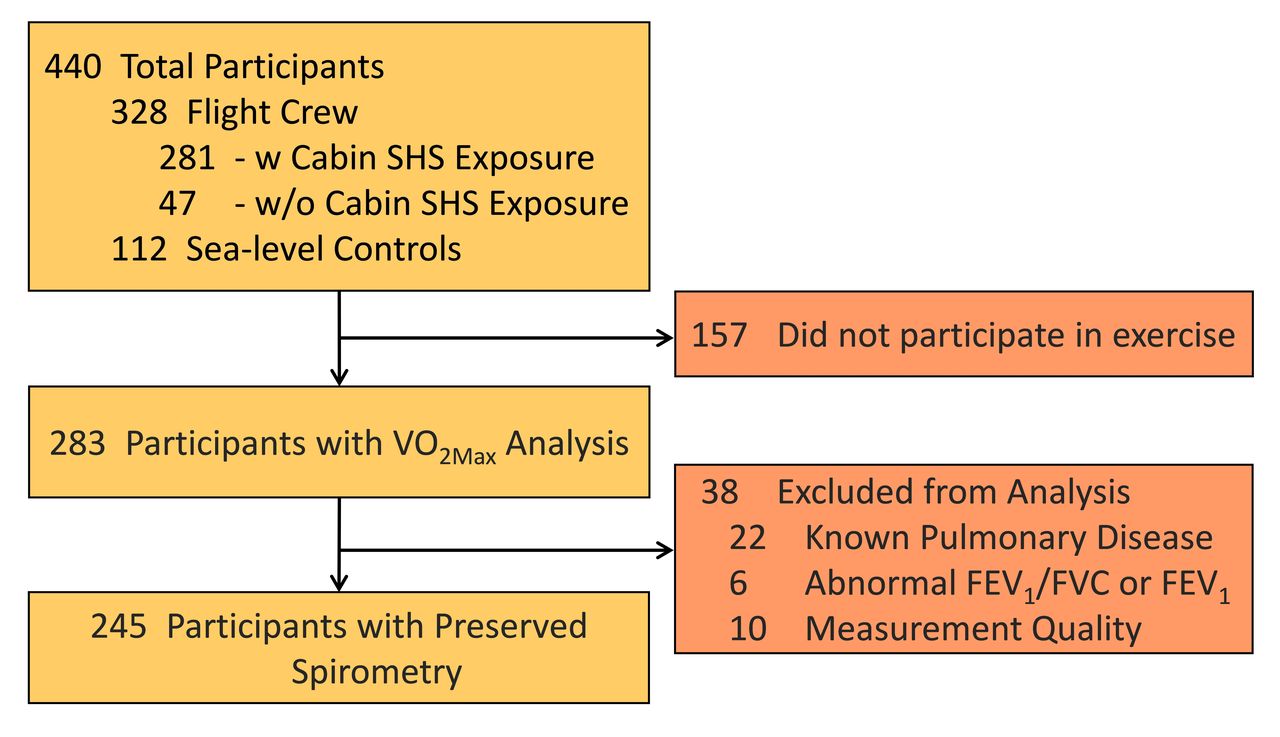
Participants flow through the study. BMI, body mass index; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; PFT, pulmonary function test; SHS, secondhand tobacco smoke; VO2Max, volume of maximum oxygen uptake.
Institutional Review Board approval
The University of California San Francsico (UCSF) Institutional Review Board (IRB) and the San Francisco Veterans Affairs (VA) Medical Center Committee on Research and Development approved the study protocols. Written IRB-approved informed consent and Health Insurance Portability and Accountability Act were obtained from all study participants. All participants received monetary compensation for their participation in the study.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research. However, the participants did act as a referral source and referred other interested potential people to participate in our study, and in that sense participated in dissemination of the study.
SHS exposure characterisation
SHS exposure was characterised by a questionnaire developed by the UCSF Flight Attendant Medical Research Institute (FAMRI) Center of Excellence,15 and modified to acquire information on airline-related occupational history (UCSF FAMRI SHS Questionnaire), as detailed in the online supplemental appendix and described previously.12 13
Supplemental material
Pulmonary function and cardiopulmonary exercise testing
Details of pulmonary function and maximum effort cardiopulmonary function testings are available in the online supplemental appendix and have been previously.12 14
Respiratory symptom scoring
Respiratory symptoms were assessed using modified Medical Research Council (mMRC) Dyspnoea Scale16 and another self-reported questionnaire (UCSF FAMRI SHS Questionnaire) that elicited symptoms of dyspnoea, cough and participants’ perception of a decreased level of exertion compared with peers over the year preceding enrolment.15 A dichotomous indicator of respiratory symptoms was defined by mMRC ≥1 or report of at least one respiratory symptom on the UCSF FAMRI SHS Questionnaire. A dichotomous cause of exercise cessation (dyspnoea vs fatigue or effort; DyspnoeaPeak) was determined based on the highest score reported by the participants at the end of the maximum effort exercise testing using the modified Borg Rating of Perceived Exertion (Borg), with the Category-Ratio Scale anchored at number 10 (CR10).17
Data analysis
Per cent predicted as well as lower and upper limits of normal (LLN and ULN) values for measures of spirometry and lung volumes at rest and cardiopulmonary responses to exercise were calculated using Global Lung Function Initiative, Quanjer et al, and Wasserman et al predicted formulas, respectively.18–20 American Thoracic Society guidelines were also used for assessment of normal ranges of cardiopulmonary exercise indices.21
Distributions of participants’ characteristics, pulmonary function, cardiopulmonary exercise and SHS exposure quantification variables were examined. Changes in HR, SBP, DBP and O2-Pulse with respect to the workload were approximated by estimating the slopes from linear regression modelling of those measures (HR, SBP, DBP and O2-Pulse) over workload at each stage. Peak cardiopulmonary exercise variables were estimated using the last 30 s average values obtained during the highest stage of the exercise test as described above. Cumulative work achieved throughout the exercise (WorkTotal), or the area under the curve of workload in Watts versus time in minutes, was computed as the sum of the product of watts completed and time spent at each stage in the unit of Watts-Minute. A comparison of the distributions was performed using an unpaired t-test for each continuous variable or a χ2 test for each binary or categorical variable.
Associations between exercise capacity (WattsPeak, WorkTotal or VO2Peak, as dependent variables) and each of the cardiovascular outputs (including SBP, DBP and O2-Pulse, as independent variables) were examined in multivariable linear regression models with adjustment for covariates (age, sex, height and body mass index (BMI) unless noted otherwise). Because O2-Pulse (proxy for stroke volume) estimates were calculated using VO2 and HR, the associations and mediation analyses of O2-Pulse was only examined with WattsPeak and WorkTotal measures of exercise capacity and not with VO2Peak to prevent bias from ‘mathematical coupling’.22
Similarly, associations between presence of respiratory symptoms (mMRC or UCSF FAMRI SHS Questionnaire, as dependent variables) and each of the cardiovascular outputs (as independent variables) were examined in multivariable logistic regression models with adjustment for covariates. The respective baseline variable was also adjusted whenever a slope variable was used in a model. Additionally, associations between each of the cardiovascular outputs (SBP, DBP and O2-Pulse) and baseline air trapping (FRC/TLC or RV/TLC) as a pulmonary factor affecting exercise capacity and cardiovascular outputs,23–26 and SHS exposure were examined using linear regression models.
To investigate potential confounding effects of respiratory symptoms on the association of exercise capacity with cardiovascular outputs, we also performed multivariable regression modelling of exercise capacity (work) versus relevant cardiovascular outputs along with respiratory symptoms to determine the adjusted contributions of these variables to exercise capacity.
To assess whether associations between exercise capacity and SHS exposure or air trapping (FRC/TLC or RV/TLC) were potentially mediated through cardiovascular outputs, we performed mediation analyses with exercise capacity (dependent variable), SHS exposure or air trapping (independent variable) and cardiovascular outputs (mediator variables), with inclusion of covariates using the ‘mediation’ package in R.27 Absolute proportion of mediated effects with corresponding p values were reported.
For each analysis, the total number of participants who had complete set of data for that analysis was reported along with the results from the regression modelling or mediation analysis. Statistical significance was defined as a P-value <0.05.
Results
Participant characteristics and response to exercise
The characteristics of the 245 individuals included in this analysis are shown in table 1. All participants reported ceasing exercise due to dyspnoea or leg fatigue. When pressed to identify a single cause for ceasing exercise, 117 (48%) identified dyspnoea as opposed to fatigue or effort as the main cause (DyspnoeaPeak) (table 2).
Participant characteristics
Cardiopulmonary testing measurements
The average volume of oxygen consumption at peak exercise (VO2Peak) was 1557±476 mL/min (100±24 %predicted) with 71 (29%) having a VO2Peak <84 %predicted, a presumed threshold for abnormal results. This VO2Peak was achieved at a peak workload of 156±46 watts (135±33 %predicted). The ratio of oxy-haemoglobin to total haemoglobin (oxygen saturation or SpO2Peak) at peak exercise was 98%±1% with nearly all participants but one having a SpO2Peak of >93%. The pulmonary response to exercise was remarkable for a peak-exercise minute ventilation (VEPeak) of 57.0±17.0 L/min (50±12 %predicted) with only 12 (5%) exceeding the 70% threshold for inappropriate ventilatory response to maximum effort exercise. The peak-exercise respiratory rate (RRPeak) remained below the 60 breaths/min threshold in all but one participant (table 2). All participants reached their anaerobic threshold (VO2AT) as determined by V slope method. Furthermore, ventilatory efficiency (VE/VCO2) at peak exercise was 30.7±3.8 (108±12 %predicted) with lowest VE/VCO2 at 29.4±3.4 (103±11 %predicted) (table 2).
None of the participants reported any chest pain, chest tightness, lightheadedness or dizziness during the CPET. None had any clinically significant ECG changes or arrhythmia besides occasional premature ventricular contractions that did not increase in frequency with exercise testing. Nevertheless, 66% of the participants (149 out of 226) showed a hypertensive response to exercise by at least one established criterion. The heart rate at peak exercise was 142±18 beat/min (85±10 %predicted). Oxygen-pulse at peak exercise (O2-PulsePeak) was 11.0±3.0 mL/beat (116±25 %predicted), with 8 (3.3%) participants not achieving their 80% predicted values (a presumed threshold for abnormal results). Further details of the exercise test are discussed in the online supplemental appendix.
Association of exercise capacity with cardiovascular response measures, air trapping and SHS exposure
In multivariable models that included each (single) cardiopulmonary exercise testing (CPET) output separately as a predictor along with age, sex, height and BMI as covariates, workload (as measured by WattPeak or VO2Peak) and cumulative work (as measured by Watt-Minute) were positively associated with the peak of heart rate and systolic blood pressure during exercise (HRPeak and SBPPeak). However, workload and cumulative work were negatively associated with the rate of increase in SBP, DBP and HR (HRSlope, SBPSlope and DBPSlope) (all p<0.05), with faster rise of these indices being associated with lower workload or cumulative work the participants could achieve (table 3). Similarly, workload (WattPeak) and cumulative work (Watt-Minute) were associated positively with O2-PulsePeak but negatively with O2-PulseSlope. Moreover, WattPeak, VO2Peak and Watt-Minute were positively associated with respiratory rate, tidal volume and minute ventilation at peak exercise (RRPeak, VTPeak and VEPeak) and negatively with a lung function measure of air trapping (RV/TLC) (all p<0.05) (table 3).
Associations of exercise capacity with each of the cardiopulmonary exercise outputs or SHS exposure
Workload (WattPeak and VO2Peak) was also negatively associated with years of exposure to cabin SHS (both p<0.05), but was not significantly associated with non-cabin SHS exposure including childhood and adulthood home exposures (table 3).
Association of respiratory symptoms with cardiopulmonary response measures
The association of respiratory symptoms with exercise measures were examined by determining the likelihood of having respiratory symptoms at baseline (mMRC ≥1 or any respiratory symptoms by FAMRI SHS questionnaire) or reporting dyspnoea at peak exercise as the main cause of exercise cessation (reporting higher dyspnoea score on Borg Dyspnoea Scale (DyspnoeaPeak)). As shown in table 4, baseline respiratory symptoms (as measured by mMRC Dyspnoea Scale) were negatively associated with workload (WattPeak or VO2Peak) and cumulative work (Watt-Minute) achieved. Respiratory symptoms at baseline (as measured by FAMRI questionnaire) and at peak exercise (as measured by modified Borg Dyspnoea Scale) were not significantly associated with exercise capacity.
Associations of respiratory symptoms with each of the cardiopulmonary exercise outputs and SHS exposure
Overall, only a few CPET outputs were associated with respiratory symptoms. Among cardiovascular outputs, the likelihood of having an mMRC ≥1 was associated with faster rise in SBP (SBPSlope) and with lower HR at peak exercise (HRPeak). On the other hand, the likelihood of stopping exercise due to dyspnoea as measured by modified Borg Dyspnoea Scale was associated with a higher DBP at peak exercise (DBPPeak). Among pulmonary outputs, the likelihood of having an mMRC ≥1 was associated with lower RR and VE at peak exercise (RRPeak and VEPeak), and lower anaerobic threshold (VO2AT). Furthermore, baseline respiratory symptoms were significantly associated with FRC/TLC with more air trapping being associated with higher likelihood of having respiratory symptoms at baseline (RV/TLC association was marginally significant; p≤0.079).
Association of cardiovascular response measures with SHS exposure
Among the cardiovascular predictors of exercise capacity, O2-PulsePeak was negatively associated with years of exposure to cabin SHS, showing a parameter estimate of −0.032±0.015 (p=0.040), which indicates a decrease in O2-PulsePeak of 0.32 mL/beat for every 10 years increase in exposure to cabin SHS (online supplemental table S1). Consistently, the rate of increase in heart rate (HRSlope) was directly associated with years of exposure to cabin SHS (online supplemental table S1). Furthermore, mediation analysis showed that a substantial fraction of cabin SHS exposure association with exercise capacity (WattPeak) was mediated through the SHS relationship with O2-Pulse (41%; p=0.038) (table 5). Although not significant, cabin SHS association with cumulative work (Watt-Minute) also seemed to be mediated through O2-Pulse (74%; p=0.112). The associations of SBPSlope and DBPSlope with SHS were not statistically significant (online supplemental table S1).
Effect of SHS exposure on exercise capacity through mediators
Relationship among exercise capacity, respiratory symptoms and cardiovascular outputs
To determine whether respiratory symptoms affected the association of exercise capacity with cardiovascular outputs, we included mMRC as an additional predictor in the regression modelling of work versus cardiovascular outputs. In those analyses, SBPSlope, DBPSlope and HRSlope retained their associations and statistical significance, as did having an mMRC of ≥1 (online supplemental table S3).
Moreover, to determine the relationship between O2-Pulse and blood pressure, we examined the contribution of SBP and DBP to O2-Pulse, and found that O2-Pulse at peak exercise was negatively associated with SBPSlope and DBPSlope after adjustment for covariates (online supplemental table S4).
Cardiovascular response measures and baseline air trapping
Given the physical location of lung, heart and great vessels within the thoracic cavity, we examined the potential interaction of baseline air trapping and cardiovascular outputs of exercise. To do this, we examined whether the cardiovascular predictors of exercise capacity including O2-Pulse (proxy of stroke volume) and blood pressure (SBP and DBP) mediate the association of air trapping (FRC/TLC and RV/TLC) with exercise capacity.
These mediation analyses showed that a substantial fraction of RV/TLC association with exercise capacity (cumulative work (Watt-Minute)) was mediated through RV/TLC effect on O2-Pulse at peak exercise (39%; p=0.036) (table 6). Although not significant, RV/TLC association with workload (WattPeak) also seemed to be mediated through O2-Pulse (36%; p=0.078). Consistent with this finding, the heart rate at peak exercise (HRPeak) also mediated the association of RV/TLC with exercise capacity (mediated 21% and 28% of the total effect of RV/TLC on WattsPeak and WorkTotal, respectively; all p<0.05). The mediation analyses of FRC/TLC were not statistically significant (online supplemental table S2).
Effect of air trapping on exercise capacity through mediators
Discussion
In this observational study of a never-smoking cohort with a history of remote but prolonged exposure to SHS, we found the cohort to have an abnormal cardiovascular response to exercise that was proportional to their SHS exposure. Exercise capacity, as measured by highest workload completed (WattsPeak) or volume of oxygen uptake at peak exercise (VO2Peak), was associated with years of exposure to SHS. Remarkably, over 40% of the association of exercise capacity (WattsPeak) with SHS was dependent on O2-PulsePeak, which suggests that the effect of SHS exposure on exercise capacity is importantly mediated through SHS effect on stroke volume and cardiac output. Our finding that past exposure to SHS is a predictor of exercise capacity in an O2-pulse-dependent (a proxy of stroke volume and cardiac output) manner is novel and suggests that SHS exposure has a lasting effect on cardiac function that is observable years after the exposure has ceased. We also found suggestive evidence, which scarcely fell short of statistical significance (p=0.078), that pulmonary air trapping (especially elevated RV/TLC) contributes to lower exercise capacity through its effect on O2-PulsePeak. The latter finding tends to implicate an interacting lung and heart pathophysiology wherein pulmonary hyperinflation limits cardiac output to further impairs exercise capacity (figure 2). Furthermore, we found over 60% of the participants to have a hypertensive response to exercise, suggesting that abnormal escalation of blood pressure contributed to lower exercise capacity in this SHS-exposed cohort in whom only a small minority (4.3%) had known history of hypertension, which was well-controlled in all cases.

{kind=link}
{kind=link}
Proposed model for interaction of SHS with cardiovascular and pulmonary contributors to exercise capacity. Illustration of mediation effects between SHS exposure and exercise capacity. HR, heart rate; HRE, hypertensive response to exercise; IC, inspiratory capacity; SHS, secondhand tobacco smoke; SV, cardiac stroke volume; VC, vital capacity; VE, minute ventilation; VT, volume of tidal breathing.
In previous studies of this cohort of never-smokers with a history of prolonged remote exposure to SHS, we showed the cohort to have an abnormal lung function at rest and abnormal pulmonary response to exercise including (1) reduced diffusing capacity at rest,12 (2) reduced pulmonary capillary recruitment (as measured by impaired rise in diffusing capacity) during exercise,13 (3) decreased small airways airflow indices on spirometry (maximal flow in mid-expiratory and end-expiratory airflows (FEF25–75% and FEF75%)),12 (4) plethysmographic and radiographic evidence of pulmonary air trapping at rest14 and (5) progressive (dynamic) pulmonary hyperinflation during exercise.14 Overall, these abnormalities are suggestive of presence of an unrecognised early or mild obstructive lung disease that, while not meeting the spirometric definition of COPD, is consistent with an early/mild disease that could be categorised as ‘pre-COPD’ and could contribute to lower pulmonary reserve and potential adverse health outcomes.28 29 In the current study, we found evidence that prolonged exposure to SHS, even when remote, is associated with cardiovascular abnormalities suggestive of occult cardiovascular dysfunction with potential additional contribution from pulmonary hyperinflation. These abnormalities reveal subtle but lower cardiopulmonary functional reserve, manifested here as lower exercise capacity, and implicate a reduced efficiency of the body’s oxygen delivery machinery, which could be disadvantageous during the times of increased cardiopulmonary output demands as in physiological distress or disease.
Although it remains unclear how exposure to SHS causes an impairment in cardiac function, an interaction between pulmonary and cardiovascular systems, which occupy the same body cavity (thorax), has been proposed to play a role. Air trapping as measured by lung volumes (FRC/TLC and RV/TLC) is the earliest manifestation of COPD,28 29 and is associated with reduced exercise capacity due to ventilatory limitation caused by progressive air trapping and pulmonary hyperinflation.14 Changes in lung volumes due to pulmonary hyperinflation could cause increased intra-thoracic pressures, particularly during exertion, and thus adversely affect the cardiovascular function.23 25 To investigate this possible mechanism, we examined whether air trapping did contribute to exercise capacity through an interaction with cardiac output by performing a mediation analysis among pulmonary air trapping (FRC/TLC and RV/TLC), cardiac stroke volume (O2-pulse), and exercise capacity (WattsPeak) (figure 2). Although the analysis did not reach statistical significance (p=0.078 for RV/TLC) and thus could not provide any further corroborating evidence for our hypothesis, the analysis did suggest that a substantial proportion (36%) of air trapping effect on exercise capacity may be mediated through stroke volume.
Other factors that may have contributed to lower O2-pulse in this setting include impaired left ventricular (LV) filling from myocardial stiffness, and decreased LV systolic emptying in the setting of increased vascular resistance.30 SHS could through pro-inflammatory effects predispose to endothelial dysfunction.31 At the level of the coronary microvasculature, endothelial dysfunction can promote cardiomyocyte stiffening and myocardial fibrosis,32 whereas peripherally, it can interfere with normal exercise-related relaxation of the muscular arterioles, increasing afterload.30
As relates to vascular dysfunction, it is notable that 62% of our participants experienced a hypertensive response to exercise, a proportion that exceeds the 30%–40% reported in other settings.33–35 Such hypertensive response has been linked to both LV systolic and diastolic dysfunction,36 37 as well as to increased risk of cardiovascular events.38–40 Although we did not detect a relationship between hypertensive response to exercise and SHS, this does not exclude a role for abnormal arterial impedance with exercise as a potential mechanism underlying the SHS-associated diminution in stroke volume.30 Indeed, further research will be necessary to delineate the relative contributions of cardiopulmonary interaction, myocardial disease and vascular dysfunction to exercise intolerance in the context of exposure to direct or indirect smoke.
Our study has limitations that should be kept in view. First, there may be concerns about the generalisability of the findings because the cohort studied are mostly women, which reflects the demographics of those who worked in airlines as flight crew in the latter half of the last century when smoking in aircraft cabin was permitted. The choice to study flight crews permitted overcoming the challenge of long-term SHS exposure assessment by allowing estimation of a more objective and reproducible exposure index based on employment history and the smoking ban timeline on domestic and international flights of different airlines.12 Women have been reported to be more susceptible to adverse health effects of tobacco smoke,41 such that the findings are not necessarily generalisable to men. Second, the cardiovascular findings reported in this study are mainly derived from CPET with no imaging (such as echocardiography and MRI) or invasive haemodynamic monitoring to provide additional robust evidence to corroborate our findings. Such studies are needed and are in progress (ClinicalTrials.gov Identifier: NCT04715568). Nevertheless, studies describing cardiovascular health effects of direct smoking using echocardiography and MRI have been previously reported, which corroborate our findings.42 43 Our report, however, is the first to describe the chronic and long-term cardiovascular health effects due to past prolonged exposure to SHS. Third, while we found association of exercise capacity (WattsPeak) with years of SHS exposure, the association of respiratory symptoms with SHS was less striking and less consistent across the different questionnaire platforms. However, it is not uncommon to see differences in scores across different respiratory questionnaires,44 and similarly, baseline respiratory symptoms (mMRC Dyspnoea Scale and UCSF FAMRI SHS questionnaire) may measure different things and thus produce different scores compared with those done at peak exercise (modified Borg Dyspnoea Scale). For example, participants who had impairments at baseline and thus were more symptomatic are likely to not perform as well during the exercise and thus may report lesser symptoms in a sub-maximal effort exercise test.
In conclusion, healthy never-smokers with history of remote but prolonged exposure to SHS have an abnormal cardiovascular response to exercise, which is characterised by a stroke volume (oxygen-pulse) and thus an exercise capacity that are reduced proportional to their years of exposure to SHS. The mechanisms by which past exposure to SHS may limit stroke volume and thus exercise capacity are not entirely clear. But impaired LV filling and emptying may be involved, with contributions from pulmonary hyperinflation (beyond ventilatory limitation) and vascular dysfunction, both peripherally and centrally. Overall, the abnormal cardiovascular response to exercise in this population reveals the presence of subclinical pathology that impairs the cardiopulmonary functional reserve and reduces the efficiency of body’s oxygen delivery machinery, which could be disadvantageous during the times of increased cardiopulmonary output demands as in physiological distress or disease.
Data availability statement
The data sets generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by UCSF IRB# 12-10510. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Wendy Ching, BS; Charlotte Hunt, BS; and Melissa Nishihama, BS, for their assistance with performing the cardiopulmonary exercise testing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceived and designed the current manuscript study: MA. Developed study protocols: WMG, MA. Collected samples and data: SZ, MD, WMG, MA. Analysed and interpreted data: SZ, MD, JRK, MA. Prepared and edited the manuscript: SZ, MD, WMG, JRK, MA. Obtained funding: SZ, MA. Guarantor: MA. All authors read and agreed to the published version of the manuscript.
Funding This work was supported by: the Flight Attendant Medical Research Institute (FAMRI) (012500WG and CIA190001 to MA), California Tobacco-Related Disease Research Program (TRDRP) (T29IR0715 to MA), The Department of Veterans Affairs (CXV-00125 to MA) and National Library of Medicine Training Grant (NIH: T15LM007442 to SZ).
Competing interests MA reports grants from the Departments of Defense (W81XWH-20-1-0158) and Veterans Affairs (CXV-00125), the Flight Attendant Medical Research Institute (012500WG and CIA190001) and the California Tobacco-Related Disease Research Program (T29IR0715) during the conduct of the study. He has received research support from Guardant Health and Genentech.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.