Article Text

Abstract
Background There is a paucity of data on the burden of the full spectrum of community-acquired pneumonia (CAP) and acute otitis media (AOM) from outpatient and inpatient settings across the age spectrum.
Methods We conducted a population-based retrospective study in Ontario and British Columbia (BC), Canada, to estimate the incidence rate of CAP and AOM in children and adults over a 14-year period using health administrative databases. CAP and AOM cases were identified from outpatient physician consultation and hospitalisation data in both provinces, and from emergency department visit data in Ontario.
Results During 2005–2018, Ontario had 3 607 124 CAP, 172 290 bacterial CAP, 7814 pneumococcal pneumonia, and 8 026 971 AOM cases. The incidence rate of CAP declined from 3077/100 000 in 2005 to 2604/100 000 in 2010 before increasing to 2843/100 000 in 2018; bacterial CAP incidence rate also declined from 178/100 000 in 2005 to 112/100 000 in 2010 before increasing to 149/100 000 in 2018. The incidence rate of AOM decreased from 4192/100 000 in 2005 to 3178/100 000 in 2018. BC had 970 455 CAP, 317 913 bacterial CAP, 35 287 pneumococcal pneumonia and 2 022 871 AOM cases. The incidence rate of CAP in BC decreased from 2214/100 000 in 2005 to 1964/100 000 in 2010 before increasing to 2176/100 000 in 2018; bacterial CAP incidence rate increased from 442/100 000 in 2005 to 981/100 000 in 2018. The incidence rate of AOM decreased from 3684/100 000 in 2005 to 2398/100 000 in 2018. The incidence rate of bacterial CAP increased with age in older adults (≥65 years) with the highest burden in the oldest cohort aged ≥85 years both before and after 13-valent pneumococcal conjugate vaccine (PCV13) programme in both provinces. Hospitalised pneumococcal pneumonia decreased slightly but non-hospitalised pneumococcal pneumonia increased in BC during PCV13 period. No consistent direct benefit of PCV13 on CAP was observed in the paediatric population.
Conclusions There is a substantial burden of CAP and AOM in Ontario and BC. Indirect benefits from childhood PCV vaccination and polysaccharide vaccination of older adults have not substantially decreased the burden of pneumococcal pneumonia in older adults.
- pneumonia
- respiratory infection
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organisations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors on request, understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a high burden of hospitalised all-cause pneumonia and pneumococcal pneumonia in Canada, with high burden in young children and older adults; the comprehensive burden of pneumonia (all cause and pneumococcal) with and without hospitalisation is not known.
Acute otitis media (AOM) in young Canadian children results in high utilisation of physician consultation. Recent burden of AOM across all ages remains unknown.
WHAT THIS STUDY ADDS
This study estimated comprehensive burden of community-acquired pneumonia (CAP), bacterial CAP, pneumococcal pneumonia (hospitalised and non-hospitalised) and AOM across all ages in two large Canadian provinces, and found continued high burden even approximately 8 years after introduction of publicly funded paediatric 13-valent pneumococcal conjugate vaccine (PCV13) immunisation programme.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICES OR POLICY
The study strengthens evidence that pneumococcal disease continues to be a concern in a Canadian setting. It provides rates that capture burden beyond hospitalized cases and can thus serve as a baseline to assess the impact of switching to higher valent PCV (e.g., PCV15 or PCV20 being considered in Canada) on CAP and AOM. This is a valuable approach as our finding of continued high burden of CAP during the PCV13 period together with the evidence of observed increase in serotype 3 and non-vaccine serotype hospitalized CAP, and increased burden of non-PCV13 unique PPV23 and non-vaccine serotype invasive pneumococcal disease from previous studies in Canada will provide the contextual information to consider a switch to higher valent PCV vaccines in reducing the disease burden, particularly in the older population.
Introduction
Pneumonia causes substantial morbidity, mortality and healthcare service utilisation.1 In Canada, pneumonia was the sixth leading cause of hospitalisation across all ages2 and accounted for nearly 140 000 emergency department (ED) visits in 2019–2020.3 Studies estimating the burden of community-acquired pneumonia (CAP) have primarily focused on hospitalised cases4 5; however, it is likely that the majority of CAP cases in Canada are treated in ambulatory settings and do not require hospitalisation. In some European settings, <10% of adult diagnosed CAP cases resulted in hospitalisation.6 7 Acute otitis media (AOM) is a common childhood infection but affects all age groups, and can lead to different complications and sequelae, including, rarely, death.8 AOM results in high utilisation of physician consultation and antibiotic prescriptions, especially for children.9–11
Streptococcus pneumoniae is the most common bacterial cause of CAP and AOM,12 13 although other bacterial and viral pathogens have been implicated as the aetiological agents of CAP and AOM.12 14–16 Definitive microbiological confirmation of pneumococcal pneumonia among CAP cases is difficult because of the very low (approximately 10%) yield of pneumococcus from blood culture of clinical episodes of pneumonia.17 Additionally, pneumococcus carriage in the nasopharynx makes it difficult to attribute pneumococcus as the underlying aetiology of a pneumonia episode when isolated from non-sterile upper respiratory sites.18 In adults the proportion of CAP attributable to pneumococcus varies depending on the diagnostic test used, with 8% by blood culture, 20% by sputum culture and 24% by urinary antigen.19 However, pneumococcal CAP is often empirically treated precluding diagnostic testing, particularly in primary care settings. AOM is almost always treated presumptively based on clinical features and otoscopic findings without collecting middle ear fluid for microbiological testing.
Pneumococcal vaccines can prevent pneumococcal CAP and AOM in children and adults, and reduce some of the CAP and AOM burden.9 20 Canada introduced publicly funded 7-valent pneumococcal conjugate vaccine (PCV7, 3+1 dose schedule, 2002–2006), 10-valent PCV10 (3+1 dose schedule, 2009) and 13-valent PCV13 (2+1 dose schedule, 2010–2011) vaccines in infant immunisation programmes, and publicly funded 23-valent pneumococcal polysaccharide vaccine (PPV23, 1996) for adults aged 65 years and older and high-risk individuals following recommendations from the National Advisory Committee on Immunisation (NACI).21 22 Ontario introduced publicly funded PCV7 in the childhood immunisation programme in January 2005, switched to PCV10 in October 2009 for a brief period before being replaced by PCV13 (2+1 dose schedule at 2, 4 and 12 months) in November 2010 with a catch-up PCV13 dose for children aged 12–36 months who completed the PCV7 schedule. British Columbia (BC) introduced PCV7 in September 2003 followed by PCV13 (2+1 schedule similar to Ontario) in June 2010. The coverage of up-to-date PCV13 was 80% among 4-year-old s in 2013,23 and between 74% and 80% among 7-year-olds from 2014 to 2018 in Ontario24; between 82% and 86% of 2-year-olds in BC were up to date with PCV13 from 2011 to 2018.25 However, measuring the impact of vaccination on these outcomes requires better understanding of the comprehensive burden of CAP and AOM across the lifespan in Canada.
We conducted a population-based retrospective study in Ontario and BC among a population of 20 million, representing 53% of the Canadian population,26 to estimate the incidence rate of CAP and AOM in children and adults over a 16-year period. We also focused on understanding pneumococcal-associated CAP and AOM and how their burden has changed since the maturation of the pneumococcal vaccine programmes.
Methods
Data sources
We used population-based health administrative databases to identify and establish cohorts of CAP and AOM cases from 2005 to 2018 in Ontario and BC. CAP and AOM cases were identified from the Discharge Abstract Database (DAD) for hospitalised cases and physician billing claims databases (Ontario Health Insurance Plan (OHIP) and BC Medical Services Plan (MSP)) for outpatient cases in primary care settings in both provinces,27 28 and from the National Ambulatory Care Reporting System (NACRS) for cases requiring ED visits in Ontario. ED visit data from BC was not available. We obtained information on age and sex from the Registered Persons Database in Ontario and the MSP Registration and Premium Billing patient registry in BC.29 Data from Ontario and BC were analysed separately using similar methods. The Ontario datasets were linked using unique identifiers and analysed at ICES. BC datasets were similarly linked using unique identifiers and analysed at Population Data BC.
Outcomes/definitions
CAP included cases with a diagnosis of pneumococcal pneumonia, bronchopneumonia and unspecified lobar pneumonia, other pneumonia, viral pneumonia, empyema or abscess of lung with pneumonia. As bronchopneumonia and lobar pneumonia commonly occur with bacterial infection and are treated presumptively without laboratory confirmation in the primary care settings, CAP cases with a diagnosis of ‘pneumococcal pneumonia’ or ‘bronchopneumonia and lobar pneumonia, unspecified’ were considered as ‘bacterial CAP’; CAP cases with a diagnosis of ‘pneumococcal pneumonia’ were analysed separately. AOM included cases with a diagnosis of acute suppurative otitis media (ASOM), acute serous otitis media and other acute nonsuppurative otitis media. ASOM was analysed separately as a more specific case definition for AOM resulting from bacterial infection. Cases with an assigned primary or secondary diagnosis were identified using diagnostic codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA)30 in DAD and NACRS, OHIP fee codes in OHIP for physician consultation in primary care settings in Ontario or the ICD, 9th Revision, Clinical Modification (ICD-9)31 codes in MSP for physician consultation in primary care settings in BC (online supplemental table 1). However, OHIP fee codes for CAP except 486 (other pneumonia) are generally not available to the physicians using most of the billing software in Ontario, precluding use of specific codes for pneumococcal pneumonia, bronchopneumonia and lobar pneumonia. CAP cases without codes indicating invasive pneumococcal disease (IPD), and AOM cases without codes indicating IPD and CAP were included.
Supplemental material
We identified and removed duplicate records within each database using unique identifiers and the following dates: admission date in DAD, registration date in NACRS, and service date in OHIP and MSP. The following dates were used as index dates for the outcomes to link databases and identify recurrent cases across databases together with the unique identifiers: discharge date (DAD) to account for the length of hospital stay, registration date (NACRS) and service date (OHIP and MSP). CAP/AOM episodes across databases within 90 days of the earliest index date were considered the same episode, and the earliest index date was retained; CAP/AOM episodes >90 days after the earliest index date were considered recurrent episodes and included. We classified pneumococcal pneumonia cases into mutually exclusive ‘hospitalised’ and ‘non-hospitalised’ cases. Cases identified from the ED visits or outpatient physician consultations in primary care settings that did not result in hospitalisation were considered as non-hospitalised cases.
Statistical analyses
The study period was divided into two intervals in each province according to the PCV13 immunisation programme implementation (1 November 2010 in Ontario and 1 June 2010 in BC): (1) pre-PCV13 period and (2) PCV13 period. Age was categorised into age groups (0–4 years, 5–17 years, 18–39 years, 40–64 years, 65–74 years, 75–84 years and ≥85 years). We estimated incidence rates for CAP, bacterial pneumonia, pneumococcal pneumonia, AOM and ASOM. We used Poisson regression models to estimate crude as well as age-adjusted and sex-adjusted annual incidence rates (95% CIs) and used annual population estimates from Statistics Canada as the offset parameter.32 We also estimated age-group-specific cumulative incidence rates according to the PCV vaccine programme periods in the provinces. All analyses were conducted using SAS V.9.4 (SAS Institute) software.
Results
Table 1 shows the number of cases identified in the two provinces. Ontario had 3 607 124 CAP cases during 2005–2018 with less than 2% identified from hospitalisation discharge data. Among the CAP cases, 172 290 (5%) were bacterial CAP, identified from hospitalisation discharge data (40%) and outpatient visits to emergency room or physician consultation; of the 7814 pneumococcal pneumonia, majority (93%) were hospitalised (online supplemental table 2, online supplemental table 3). Ontario had 8 026 971 AOM cases, of which 3 319 670 (41%) were ASOM (online supplemental table 3) suggesting a likely bacterial aetiology.
Age and sex distribution of the community-acquired pneumonia and acute otitis media cases in Ontario and British Columbia, 2005–2018
BC had 970 455 CAP cases during the study period, of which 317 913 (33%) were bacterial CAP; 35 287 were pneumococcal pneumonia (online supplemental table 2, online supplemental table 3). Emergency room data were not available, but regardless 91% of bacterial pneumonia were identified from outpatient physician consultation (online supplemental table 2), and 89% of pneumococcal pneumonia were non-hospitalised cases (online supplemental table 3). During 2005–2018, BC had 2 022 871 AOM cases. Of the AOM cases, 1 442 411 (71%) were ASOM (online supplemental table 3).
Community-acquired pneumonia
Annual incidence trends
In Ontario, the crude incidence rate of CAP declined from 2041.1/100 000 in 2005 to 1780.1/100 000 in 2010 before increasing to 2020.5/100 000 in 2018; bacterial CAP crude incidence rate also declined from 118.2/100 000 in 2005 to 77.9/100 000 in 2010 before increasing to 111.0/100 000 in 2018 (figure 1A, (online supplemental table 4). In BC, the crude incidence rate of CAP decreased from 1507.8/100 000 in 2005 to 1376.0/100 000 in 2010 before increasing to 1595.8/100 000 in 2018; bacterial CAP crude incidence rate increased from 307.2/100 000 in 2005 to 749.3/100 000 in 2018 (figure 1B, online supplemental table 4). After age and sex adjustment, the incidence rates increased in both provinces. The adjusted incidence rates of hospitalised pneumococcal pneumonia declined in both provinces; from 5.7/100 000 in 2005 to 4.5/100 000 in 2018 in Ontario, and from 8.0/100 000 in 2005 to 6.3/100 000 in 2018 in BC (online supplemental table 4, online supplemental figure 1).

Annual incidence of community-acquired pneumonia (CAP) and acute otitis media (AOM): (A) CAP in Ontario (B) CAP in British Columbia (C) AOM in Ontario (D) AOM in British Columbia, 2005–2018. PCV, pneumococcal conjugate vaccine.
Age-group-specific cumulative incidence before and after PCV13 programme
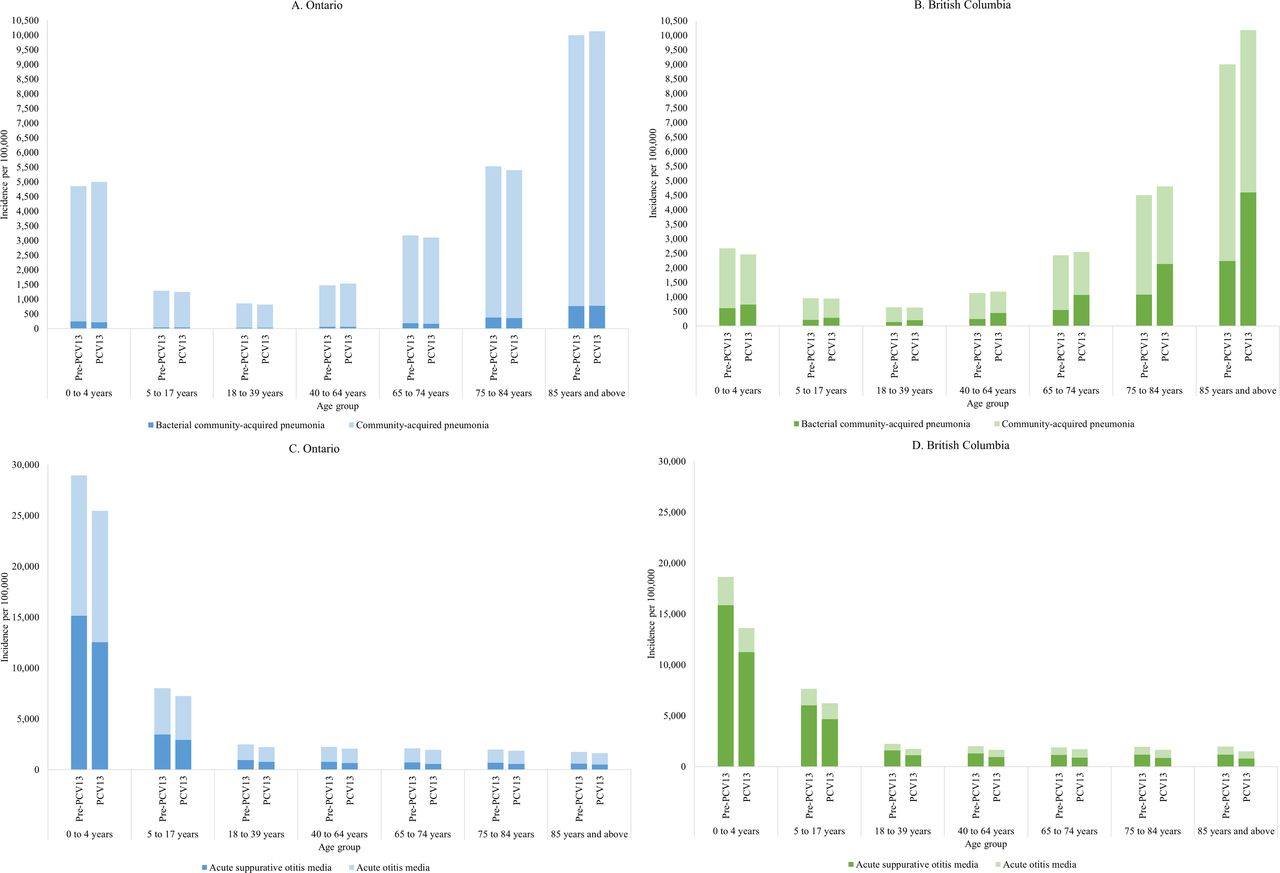
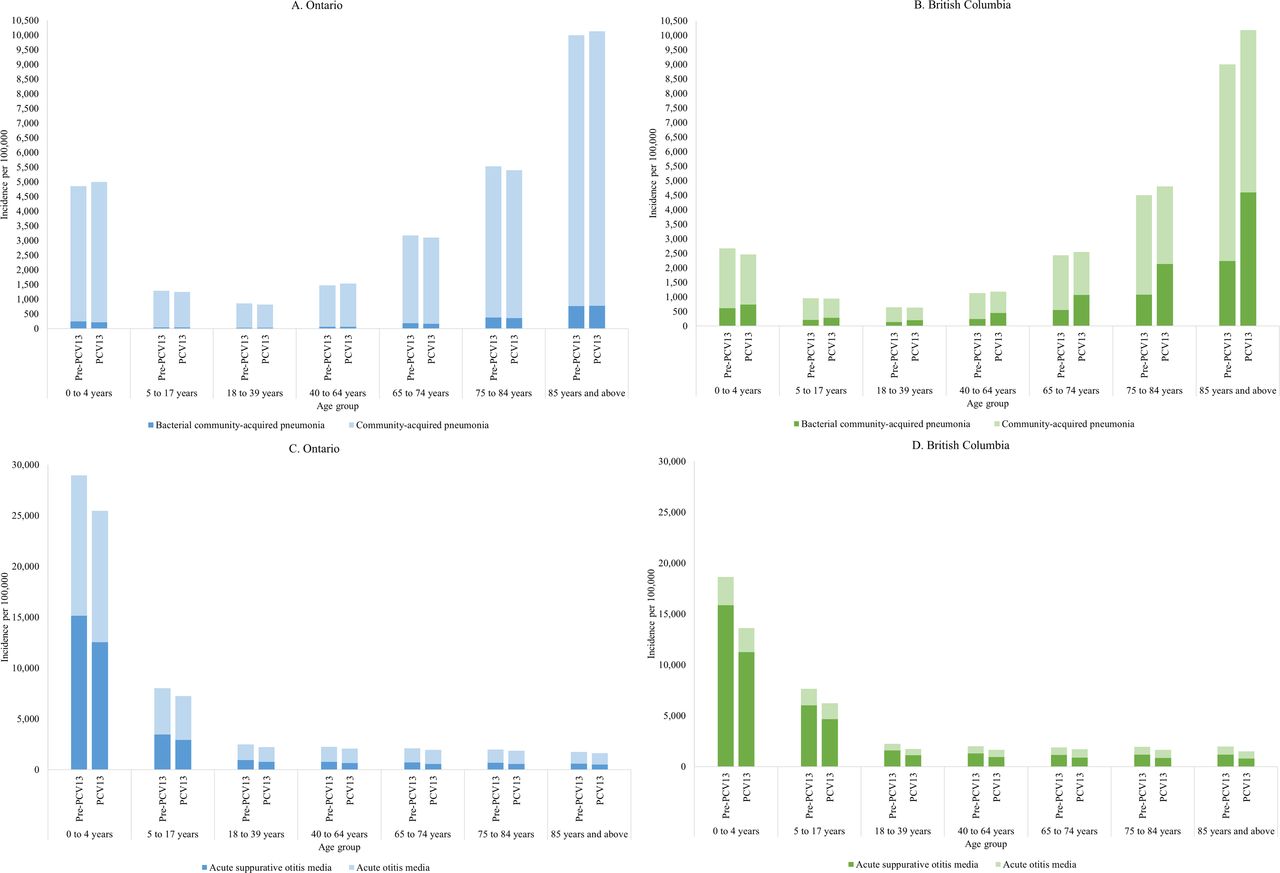
A high incidence rate of CAP was observed in the youngest cohort of children (0–4 years) and older adults aged ≥85 years in both provinces (table 2). In children aged 0–4 years, the incidence rate of bacterial CAP was lower during the PCV13 period compared with the pre-PCV13 period in Ontario but was higher during the PCV13 period compared with the pre-PCV13 period in BC (online supplemental table 5, online supplemental table 6, figure 2A and B). The incidence rate of bacterial CAP increased with age in older adults (≥65 years) with the highest burden in the oldest cohort aged ≥85 years both before and after PCV13 programme in both provinces. Bacterial CAP burden in adults aged ≥85 years was almost half the CAP burden during PCV13 period in BC (online supplemental table 6, figure 2B). Ontario had higher incidence rates of hospitalised pneumococcal pneumonia compared with non-hospitalised pneumococcal pneumonia across all age groups during both pre-PCV13 and PCV13 periods; in contrast, BC had higher incidence rates of non-hospitalised pneumococcal pneumonia (online supplemental table 5, online supplemental table 6, online supplemental figure 2). The incidence rate of hospitalised pneumococcal pneumonia increased with age in adults in both provinces. The burden of hospitalised pneumococcal pneumonia appears to have declined slightly although with overlapping confidence intervals after PCV13 in Ontario; the burden of hospitalised pneumococcal pneumonia declined in adults during PCV13 period but non-hospitalised pneumonia increased across all age groups during PCV13 period in BC.
{kind=link}
{kind=link}
Age group-specific incidence of community-acquired pneumonia (CAP) and acute otitis media (AOM) before and after implementation of 13-valent pneumococcal conjugate vaccine (PCV13) programme: (A) CAP in Ontario (B) CAP in British Columbia (C) AOM in Ontario (D) AOM in British Columbia, 2005–2018.
Cumulative incidence of community-acquired pneumonia and acute otitis media before and after implementation of 13-valent pneumococcal conjugate vaccine (PCV13) programme stratified by age group in Ontario and British Columbia, 2005–2018
Acute otitis media
Annual incidence trends
The crude incidence rate of AOM, including ASOM decreased during the study period in both provinces (figure 1C, online supplemental table 4). In Ontario, the incidence rate decreased from 5308.8/100 000 in 2005 to 3794.8/100 000 in 2018 for AOM, and from 2364.7/100 000 in 2005 to 1494.0/100 000 in 2018 for ASOM. BC had a similar decrease in incidence from 4118.3/100 000 in 2005 to 2530.3/100 000 in 2018 for AOM, and from 3141.9/100 000 in 2005 to 1574.9/100 000 in 2018 for ASOM (figure 1D, online supplemental table 4). After age and sex adjustment, the incidence decreased in both provinces.
Age-group-specific cumulative incidence before and after PCV13 programme implementation
The highest incidence rate of AOM was among the youngest cohort (0–4 years) in both provinces (table 2, figure 2C and D). In both provinces, the incidence rate decreased markedly with age and slightly reduced with the introduction of PCV13. The burden of ASOM, suggestive of bacterial aetiology, comprised half to three-quarters of the AOM burden.
Discussion
We estimated the comprehensive burden of CAP and AOM across all age groups by combining cases from both inpatient and outpatient care settings using ICD-9, ICD-10-CA and physician billing coding in health administrative data. Our findings suggest that the burden of CAP in older adults and AOM in young children remains substantially high in two of the most populous provinces in Canada. There remains a sizeable burden of CAP and AOM attributable to bacterial pathogens, including pneumococcus in the context of PCV programmes during the study period even with underestimation of outpatient burden in Ontario. No consistent direct and indirect benefits of PCV13 programme was observed in both provinces.
Applying the overall age-adjusted and sex-adjusted incidence rates in 2018, an estimated 70 397 bacterial pneumonia, 974 hospitalised and 4049 non-hospitalised pneumococcal pneumonia, and 222 572 ASOM cases occurred in Ontario and BC. As expected, the majority of the CAP cases in both provinces were identified from outpatient settings. Only a handful of studies have reported the incidence of CAP in outpatient settings. An annual incidence of 293–306 per 100 000 population was reported for all-cause CAP during 2005–2009 in individuals aged ≥15 years in a study conducted in Italian general practices.6 Another study reported an annual incidence of 470 per 100 000 population for all-cause outpatient CAP in French adults aged >18 years in 2011–2012.7 Our estimated annual rates of hospitalised and outpatient CAP for all age groups for the corresponding years are much higher than these reported rates. A previous systematic review estimated that approximately 27% of hospitalised adult CAP were attributable to pneumococcus.19 Pneumococcus was identified in approximately 25% of AOM cases in Japanese children.33 We observed a decline in the annual incidence rates of CAP, bacterial CAP and hospitalised pneumococcal pneumonia during pre-PCV13 years in both provinces, which likely resulted from the earlier use PCV7 or PCV10. Contrary to our expectation that PCV13 would have impacted the incidence rates of CAP and bacterial CAP, we observed relatively stable rates in Ontario and increasing rates of bacterial CAP in BC during our study PCV13 period. Hospitalised pneumococcal pneumonia seemed to decline slightly, particularly in older adults aged ≥65 years in both provinces, while non-hospitalised pneumococcal pneumonia increased specifically in BC. A substantial reduction in the incidence of hospitalised pneumococcal pneumonia, pneumonia of unspecified causative organism, and empyema was observed after PCV13 implementation among children aged <2 years in the UK; hospitalised pneumococcal pneumonia was also reduced in individuals aged 2–44 years, but increased in individuals aged ≥45 years.34 A reduction in hospitalised non-invasive pneumococcal CAP was observed only in infants during the post-PCV13 period compared with the pre-PCV13 period (6.2/100 000 vs 8.1/100 000) in Israel.35 The incidence of hospitalised all-cause pneumonia declined in Canadian children aged 0–17 years and older adults aged ≥65 years during early PCV13 years (2010–214)36; the incidence of pneumococcal pneumonia among hospitalised Canadian adults was also reported to have declined during early PCV13 years before increasing again in 2015.5
Our study identified several differences with respect to age-specific trends for CAP. We observed a very small decline in the cumulative incidence of bacterial CAP and hospitalised pneumococcal pneumonia from pre-PCV13 to PCV13 period in children aged <18 years in Ontario; furthermore, the incidence rate of bacterial CAP in BC increased substantially during PCV13 period compared with pre-PCV13 period, and the incidence rate of non-hospitalised pneumococcal pneumonia increased in children aged 0–4 years during PCV13 period. In contrast, the incidence of inpatient and outpatient non-invasive pneumococcal pneumonia using administrative database in US children aged <18 years decreased considerably during our study period from 2006 to 2009 (late PCV7) to 2014–2018 (late PCV13): from 102.0 to 32.2 per 100 000 patient-years in children <2 years, from 83.9 to 30.8 per patient-years in children aged 2–4 years, and from 34.1 to 12.5 per 100 000 patient years in children aged 5–17 years.37 In our study, the burden of bacterial CAP and pneumococcal pneumonia continued to increase with age in older adults aged ≥65 years even after introduction of PCV13 in children and publicly funded PPV23 in older adults. This phenomenon has also been observed in US-based studies evaluating hospitalised CAP in adults.38 We would expect influenza vaccination to reduce some of the burden of primary CAP caused by influenza virus and prevent secondary pneumonia caused by pneumococcus and other bacteria during vaccine-matched influenza seasons, particularly in older adults.39 For example, during 2016–2017 influenza season, 24% of children, 37% of adults aged 18–64 years with chronic medical conditions, and 69% of older adults aged ≥65 years were reported to have received influenza vaccine in Canada.40 The expected benefits of influenza vaccination on CAP and pneumococcal pneumonia may have been offset by suboptimal influenza vaccine coverage and the observed decline in vaccine effectiveness with influenza vaccination programme maturation.41 Nevertheless, the absence of aetiology data limits us from fully understanding the observed time trends of CAP, including bacterial CAP and pneumococcal pneumonia burden in our study.
We could not directly measure the impact of vaccination on AOM cases; however, we observed a decline in the incidence of AOM and ASOM from the pre-PCV13 period to the PCV13 period across all age groups in both provinces. This could have resulted from a reduction in the prevalence of pneumococcus as the causative organism of AOM in children with the introduction of PCV13 as reported previously,42 and reflects the direct benefit of PCV13 vaccine in children along with indirect and/or direct benefit in adults. However, a small reduction in AOM could also have resulted from influenza vaccination in children.43 The incidence of AOM in US children also declined from 1998 to 2018 using claims data from commercial plans (1111–727/1000 person-years in children aged <2 years, 517–400/1000 person-years in children aged 2–4 years, and 112–87/1000 person-years in children aged 5–17 years) and Medicaid (895–656/1000 person-years in children aged <2 years, 385–329/1000 person-years in children aged 2–4 years, and 98–87/1000 person-years in children aged 5–17 years).44 A lack of contemporaneous data on the burden of AOM in adults precluded comparison of our rates.
Substantial benefits of the childhood PCV have been observed in the USA in preventing healthcare visits for otitis media and hospitalisations for pneumonia in children.45 But more recently, partial replacement with non-vaccine serotype IPD across all age groups and an increase in non-PCV13 IPD hospitalisation in children aged <5 years have been reported in some high-income countries, including Canada.46–48 This could also apply to non-IPDs, such as CAP; the lack of considerable benefit of pneumococcal vaccines observed in our study may have resulted from pneumococcal serotype replacement with non-vaccine serotypes. Indeed, non-vaccine serotype CAPs have been reported in Canadian hospitalised adult patients with pneumococcal pneumonia, and these cases would not be prevented by PCV13 or PPV23; CAP cases caused by 22F and 33F serotypes were also reported.5 An increase in the incidence of hospitalised pneumococcal CAP, primarily due to non-vaccine serotypes and serotype 3 has also been reported in individuals aged ≥16 years in the UK.49 Similar increase in the incidence of hospitalised pneumococcal CAP with serotype 3 was observed in Canadians aged ≥16 years, which partly offset the indirect benefit of PCV13 conferred against 7F and 19A in adults.5 50 Pathogen-specific (eg, capsular polysaccharide and invasiveness) and host-related (eg, immunotolerance) factors together with a lower PCV13 vaccine effectiveness against serotype 3 with the current vaccine schedules and doses in children may explain the persistence of serotype 3 in adults.51 Nevertheless, limited evidence suggests 52.5% vaccine effectiveness of PCV13 against serotype 3 hospitalised CAP in older adults aged ≥65 years.52
Another reason for the increase we observed in CAP rates may be related to pneumococcal vaccine coverage and the differences in the vaccine schedule between Canada and the USA. Pneumococcal vaccination coverage remains suboptimal in both children and adults in Canada. Approximately 80% of Canadian children were reported to have received PCV by 2 years of age during 2013–2017,53 which is below the national coverage goal of 95%.54 Canada changed the PCV schedule to 2+1 back in 2010 while the USA had maintained the original 3+1 schedule. Studies have shown a considerable number of children in Canada are only partially vaccinated with the PCV vaccines and/or delayed their vaccination.55–57 It is possible that incomplete receipt of PCV vaccine is impacting the indirect benefits seen in adults in Canada compared with the USA. Additionally, PPV23 vaccination coverage in older adults also remained at 36%–58% during 2006–2019 in Canada, which is much lower than the national target coverage of 80%, and uptake of pneumococcal vaccine in younger adults (18–64 years) with chronic medical condition was estimated at 12%–25%.40 58 PPV23 has lower effectiveness against CAP hospitalisation (10%) and pneumococcal CAP hospitalisation (32%–51%) in older adults59 and minimum effect on all-cause pneumonia and pneumococcal pneumonia in adults.60 The US Advisory committee on Immunisation Practices (ACIP) recommended routine use of PCV13 in series with PPV23 for all adults aged ≥65 years in 2014 considering an estimated 20%–25% of IPD and 10% of CAP cases in US adults aged ≥65 years were caused by PCV13 serotypes that could be prevented in view of demonstrated efficacy of PCV13 against PCV13-type IPD and pneumonia in this population.61 This recommendation was made to achieve additional reductions in disease burden in adults aged ≥65 through the ongoing indirect effects of paediatric PCV13 programme and the direct effects of PCV13 in adults aged ≥65. However, the direct and indirect effects resulted in minimum changes in population-level incidence of pneumococcal disease in adults following implementation of this recommendation.62 Consequently, in 2018, the ACIP changed the recommendation to a routine single dose of PPV23 for all adults aged ≥65 years, and recommended shared clinical decision-making for use of PCV13 in adults aged ≥65 years without any immunocompromised condition, cerebrospinal fluid leak, or cochlear implant and who have not received PCV13 previously while recognising that some adults aged ≥65 years are at increased risk of exposure to PCV13 and would benefit from PCV13. In Canada, the NACI recommended the use of PCV13 in immunocompetent adults aged ≥65 years not previously immunised against pneumococcal disease who desire additional protection against PCV13 serotypes in addition to the routinely recommended PPV23 for all adults aged ≥65 years.63 NACI does not recommend inclusion of PCV13 in publicly funded immunisation programme for adults aged ≥65 years.64 Considering the low level of protection conferred by PPV23 vaccines and the observed persistent high burden of CAP and pneumococcal pneumonia in older adults during PCV13 period in our study, it may be worthwhile to consider the higher valent PCV vaccines for older adults and evaluating the effectiveness of PCV in this population. Newer generation, higher valent PCV vaccines, such as PCV15 or PCV20 that would provide extended protection against non-PCV13 or non-PPV23 serotypes causing CAP could maximise the potential direct and indirect benefits from polysaccharide vaccines and reduce CAP and pneumococcal pneumonia burden.
One key strength of our study is that we used data from multiple points of contact with the healthcare system (eg, hospitalisation, ambulatory and emergency care, and primary care) that enabled us to better approximate the overall healthcare burden of CAP and AOM by not focusing on serious episodes requiring hospitalisation. Our estimated CAP and AOM burden that could be potentially attributable to bacteria, including pneumococcus demonstrates the burden that could be preventable by the PCV programmes.
Our study had a number of limitations. One major limitation of our study is the inability to establish aetiology-specific pneumonia in primary care settings. This precluded identification and quantification of pneumococcal pneumonia cases among all-cause CAP that were treated in outpatient settings alone and consequently led to considerable underestimation of the burden of bacterial CAP and pneumococcal pneumonia. In the absence of routine microbiological testing to identify aetiological agents with subjectivity in clinical diagnosis and use of diagnostic codes in primary care settings, there remains uncertainty and some degree of imprecision in estimating the burden of CAP and AOM attributable to bacterial pathogen, including pneumococcus using diagnostic codes. There are limited data on the validity of pneumonia and AOM diagnostic codes used in primary care settings. However, previous studies in Canada have reported that in paediatric and adult populations, administrative billing codes for pneumonia and otitis media used in our study were reasonably accurate compared with medical records.65–67 Other studies have also validated codes in hospitalised, and ED visit paediatric pneumonia cases.68 69 Diagnostic codes similar to ours have been used to estimate the incidence of all-cause CAP hospitalisation in Canada previously.4 36 The incidence of paediatric AOM has also been estimated using administrative billing codes in the USA.44 As such, it is unlikely that our burden estimates are substantially overestimated because of false positive cases. Diagnostic and laboratory practices to identify a patient with CAP or AOM may vary among physicians in Ontario and BC. Our study used administrative databases and relied on the use of diagnostic codes. As a result, there is the potential for misdiagnosis, miscoding or misclassification of CAP and AOM, resulting in underestimation or overestimation of the burden.70 71 The differences in incidence between Ontario and BC (higher incidence of CAP and AOM in Ontario, while higher incidence of bacterial CAP, non-hospitalised pneumococcal pneumonia and ASOM in BC) most likely resulted from differences in case ascertainment/diagnosis and/or coding practices, although there may also have been local variability in viral and bacterial pathogen occurrence, including pneumococcal serotype replacement, and/or variable distribution of risk factors, particularly in adults. However, we would expect within province comparisons and trends over time to be less affected by these factors. Most of the bacterial CAP and pneumococcal pneumonia cases in BC were identified from the primary care settings and BC had much higher burden of bacterial CAP and non-hospitalised pneumococcal pneumonia than Ontario. A lack of general availability of billing codes for aetiology-specific pneumonia in primary care settings in Ontario likely resulted in the observed considerable underestimation of bacterial CAP and non-hospitalised pneumococcal pneumonia in Ontario. Furthermore, bacterial CAP and non-hospitalised pneumococcal pneumonia burden in BC also has the potential for overestimation in absence of microbiological confirmation in primary care settings. Although we included CAP and/or AOM cases from the primary care settings in both provinces, we also included cases treated at the ED from Ontario; the lack of ED visit data from BC may have led to an underestimation of CAP burden in BC.
Conclusion
The findings from our study provide a better understanding of the overall burden of CAP and AOM across 14 years in two large Canadian provinces. Our study suggests ongoing substantial burden of CAP and pneumococcal disease in Canada, despite publicly funded pneumococcal vaccination programmes in place for more than a decade, reinforcing the need to investigate the reasons. Future studies estimating the population-level impact of PCV13 programme on CAP and AOM compared with pre-PCV13 period would help quantify the direct and indirect (herd) effects and provide evidence to suggest if conjugate vaccines with additional prevalent pneumococcal serotypes (eg, PCV15 or PCV20) should be considered to augment reduction in disease burden. Another issue to consider is whether older adults would benefit from directly receiving PCV in the context of lower PPV23 vaccine effectiveness against CAP.
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organisations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors on request, understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Ethics statements
Patient consent for publication
Ethics approval
We obtained ethics approval from the Ethics Review Boards of the Ontario Agency for Health Protection and Promotion, the University of British Columbia and BC Ministry of Health.
Acknowledgments
Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed in the material are those of the author(s), and not necessarily those of CIHI. We thank Population Data BC and British Columbia Center for Disease control for acquisitive and provision of administrative data. We would like to thank Frank Rudicz for reviewing the manuscript. We also thank Zishu Chen for literature review on the validity of diagnostic codes used for CAP and AOM. The authors are grateful to the residents of Ontario and British Columbia without whom this research would be impossible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FM and NSC conceived of the study, and FM and SAF oversaw the study. FM, NSC, SAF, JCK, SN and JW designed the study. SN and JW prepared the data and performed statistical analyses. SN drafted the manuscript. All authors interpreted the results, critically reviewed and edited the manuscript, and approved the final version of the manuscript. SAF is the guarantor of the study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported by the Canadian Immunisation Research Network (CIRN) (Grant no. CIRN PC11). This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH). SN was supported by a University of Toronto Connaught Global Challenge Award to NC 2019-2020. JCK is supported by Clinician-Scientist Award from the University of Toronto Department of Family and Community Medicine. MS is supported via salary awards from the BC Children’s Hospital Foundation, the Canadian Child Health Clinician Scientist Program and the Michael Smith Foundation for Health Research. CQ was supported by the Fonds de recherche du Québec—Santé (chercheur boursier de mérite) and is the Canada Research Chair—tier 1 in Infection Prevention. This research was supported, in part, by a Canada Research Chair in Economics of Infectious Diseases held by Beate Sander (CRC-950-232429).
Competing interests MS has been an investigator on projects funded by GlaxoSmithKline, Merck, Moderna, Pfizer, Sanofi-Pasteur, Seqirus, Symvivo and VBI Vaccines. All funds have been paid to his institute, and he has not received any personal payments. SKM is co-PI on a project funded by Pfizer that is unrelated to this manuscript, has served on ad hoc advisory boards for Pfizer and Sanofi-Pasteur, and has received speaker fees from GlaxoSmithKline. AM is an investigator on projects funded by Merck, Pfizer, Sanofi-Pasteur and Seqirus with payments to her institution, and has served on advisory boards for GlaxoSmithKline, Merck, Pfizer, Sanofi-Pasteur and Seqirus. The Centre for Vaccine Preventable Diseases is operated by the Dalla Lana School of Public Health, which receives funding from government, philanthropic, not for profit and private sector organization, including vaccine manufacturers. This includes a donation from Merck to the institution that supports the salary of SF. SF does not receive funding directly from Merck or any personal payment or direct funds from vaccine manufacturers to support her research. Other authors declare no conflicts of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.