Article Text

Abstract
Introduction The role of haemoglobin (Hb) value and red blood cell (RBC) transfusions in prolonged weaning from mechanical ventilation (MV) is still controversial. Pathophysiological considerations recommend a not too restrictive transfusion strategy, whereas adverse effects of transfusions are reported. We aimed to investigate the association between Hb value, RBC transfusion and clinical outcome of patients undergoing prolonged weaning from MV.
Methods We performed a retrospective, single-centred, observational study including patients being transferred to a specialised weaning unit. Data on demographic characteristics, comorbidities, current and past medical history and the current course of treatment were collected. Weaning failure and mortality were chosen as primary and secondary endpoint, respectively. Differences between transfused and non-transfused patients were analysed. To evaluate the impact of different risk factors including Hb value and RBC transfusion on clinical outcome, a multivariate logistic regression analysis was used.
Results 184 patients from a specialised weaning unit were analysed, of whom 36 (19.6%) failed to be weaned successfully. In-hospital mortality was 18.5%. 90 patients (48.9%) required RBC transfusion during the weaning process, showing a significantly lower Hb value (g/L) (86.3±5.3) than the non-transfusion group (95.8±10.5). In the multivariate regression analysis (OR 3.24; p=0.045), RBC transfusion was associated with weaning failure. However, the transfusion group had characteristics indicating that these patients were still in a more critical state of disease.
Conclusions In our analysis, the need for RBC transfusion was independently associated with weaning failure. However, it is unclear whether the transfusion itself should be considered an independent risk factor or an additional symptom of a persistent critical patient condition.
- respiratory muscles
- systemic disease and lungs
- assisted ventilation
- clinical epidemiology
Data availability statement
Data are available on reasonable request. The patient datasets, which were generated and analysed in this study, are not publicly available due to medical confidentiality. They are available from the corresponding author in deidentified form on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Anaemia is a common condition in intensive care unit patients undergoing prolonged weaning from mechanical ventilation. However, the impact of haemoglobin value and related to that of red blood cell (RBC) transfusions in prolonged weaning is still controversial. While pathophysiological considerations suggested a not too restrictive transfusion strategy in weaning patients, adverse effects of transfusions became more and more apparent.
WHAT THIS STUDY ADDS
In our analysis, the need for RBC transfusion was associated with weaning failure. However, as the transfused group also showed indicators of a higher severity of disease, it was ultimately unclear whether the transfusion is an independent risk factor itself or more an additional symptom for the persistence of a critical patient condition.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
A need for RBC transfusions may be a surrogate for the presence of a persistent critical condition that delays or prevents patient recovery and progress in weaning. Targeted prospective studies could first create evidence for the actual existence of this condition and, in a subsequent step, search for therapeutic strategies to overcome it.
Introduction
In a majority of patients, mechanical ventilation (MV) can be discontinued without any relevant problems. Contrarily, approximately 15% of patients show a so called prolonged weaning from MV1 due to several reasons. This particular patient group requires complex, multimodal, multiprofessional and protracted concepts and should be treated in specialised weaning centres.2 One aspect potentially impairing the weaning process is anaemia, which is a common phenomenon in nearly all patients after prolonged treatment on an intensive care unit (ICU).3 Anaemia of critical illness has a multifactorial pathogenesis, including haemodilution, (partly iatrogenic) blood loss, reduced red cell survival and production, abnormal iron metabolism, nutritional deficiencies and an inappropriate erythropoietin production.4
The role of the haemoglobin (Hb) value and the impact of red blood cell (RBC) transfusions in prolonged weaning has been controversial for years. To the best of our knowledge, no randomised clinical trials with a relevant number of patients have addressed this issue so far. From a pathophysiological point of view, there are good reasons to argue for higher Hb values or a more liberal transfusion strategy. The rationale of an RBC transfusion with the intended increase of Hb concentration is the increase of the arterial oxygen content (CaO2) in order to improve the global and cellular oxygen delivery (DO2) and to consecutively increase the cellular oxygen consumption (VO2).5 Since DO2 is the product of CaO2 and cardiac output, an increase of CaO2 would unburden the cardiac system. However, the critical threshold for DO2, below which tissue hypoxia develops, varies individually and is difficult to determine precisely, even more in patients under prolonged weaning. In these patients, there is usually no tissue hypoxia during MV phases securing a sufficient gas exchange, while this can change considerably under spontaneous breathing. Anaemia can lead to increased cardiac output with consecutive additional load on the respiratory system. This is especially disadvantageous in prolonged weaning since these patients frequently show an insufficiency of respiratory musculature as well as of cardiac function. Compensation of anaemia can lead to a decrease in total oxygen consumption, since oxygen demand of both organs is increased in anaemia.6 Contrarily, there is growing evidence that an uncritical, liberal strategy in RBC transfusions has several disadvantages including nosocomial infections,7–11 but also immunological reactions12 up to a lung injury.13–15 Moreover, there is still controversy about Hb thresholds for transfusion to compensate anaemia-conditioned burden of ventilatory and/or cardiac load.6 16–18
The objective of our study was to describe the clinical practice regarding RBC transfusions in a specialised weaning unit. We aimed to examine possible effects that could derive from Hb value or RBC transfusions onto the outcome represented by weaning success and hospital mortality in patients undergoing prolonged weaning from MV.
Methods
The weaning unit
The interdisciplinary weaning unit (referred to as WEA in the further course) of the University Hospital RWTH Aachen, Germany consists of 18 beds and is equipped to provide full organ support (ie, invasive and non-invasive ventilation (NIV), intermittent dialysis, vasopressor therapy). It is run by a team of certified physicians, certified nurses, physiotherapists, respiratory therapists, as well as one speech therapist and one psychologist. Patients are referred from surgical and medical in-house ICUs, but also from external hospitals. Admission criteria include the absence of acute illness and multi organ failure, absence of high-dosage or multiple vasopressor therapy and absence of continuous renal replacement therapy (RRT). The surgical treatment, especially multistage procedures that require repeated performance of general anaesthesia, should be preferably completed prior to admission. An already performed tracheostomy not shorter than 24 hours and a documented spontaneous breathing trial (SBT) (including reasons for withdrawal) as well as consideration of assessing readiness to wean,1 respectively, on the ICUs were further admission criteria for the weaning unit. The weaning is carried out systematically according to the German S2k-guideline ‘Prolonged Weaning’.2
Weaning subcategories according to the German S2k-guideline for prolonged weaning2 are defined as follows:
3a: Successful weaning after at least three failed SBT or MV longer than 7 days after the first failed SBT without the use of NIV.
3b: Successful weaning after at least three failed SBT or MV longer than 7 days after the first failed SBT in combination with NIV; if necessary, continued into out-of-hospital (home) MV.
3c: Weaning failure: indication for permanent, invasive home ventilation or death during the process of prolonged weaning.
RBC transfusion guidelines
Indication for RBC transfusion was made according to the German guideline for prolonged Weaning.2 According to this guideline, transfusions can be considered below a Hb value of 100 g/L considering patient’s risk factors, like certain comorbidities or physiological transfusion triggers, for example, tachycardia. The target Hb value should be between 70 and 90 g/L. If clinical symptoms indicate inadequate compensation for low Hb levels or significantly increased work of breathing (in severe lung disease) hampering successful weaning, the Hb value should be raised, at least over a value of 80 g/L.2 These recommendations are congruent with international guidelines as well.19 On WEA, the decision for RBC transfusion is made by the physician in charge at his clinical discretion. There are no additional local policies beyond the respective Guideline. Naturally, factors such as the patient’s cardiac situation or the clinical impression of an increased work of breathing were included into the clinical reasoning for or against an RBC transfusion.
Study design and patient selection
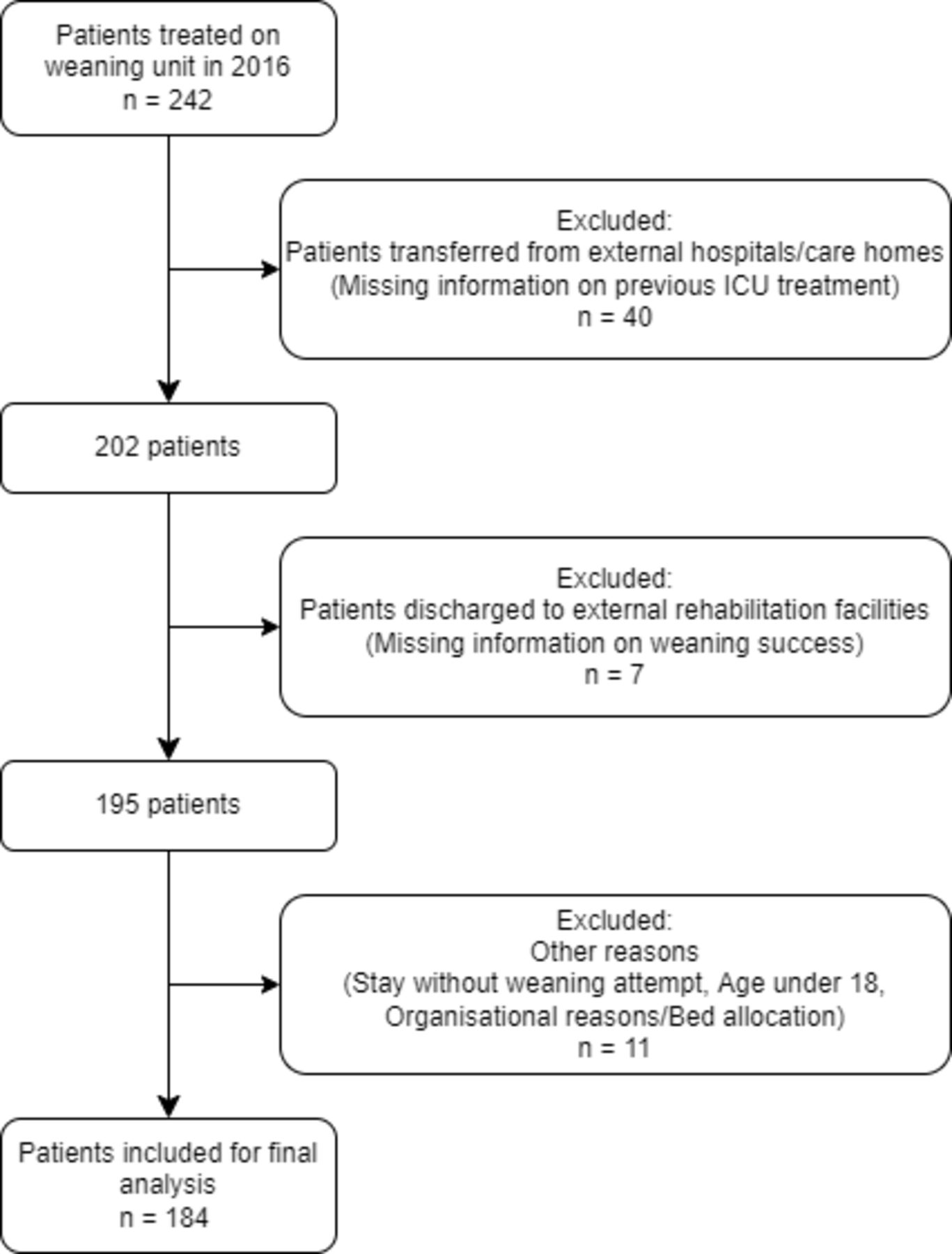
This study was a retrospective, single-centred, observational study. We used the Strengthening the Reporting of Observational Studies in Epidemiology case–control checklist when writing our report.20 We included all patients with prolonged weaning group 3 being transferred to the WEA in the year 2016 from another ICU of our university hospital. Patients transferred from an external hospital with incomplete data or information about the preceding treatment and those admitted from an external care facility for a therapy check-up or a further weaning attempt were excluded. Patients discharged to a specialised rehabilitation centre with the aim to continue the weaning process there were excluded as well. A flow chart of exclusion process is indicated in figure 1. If a patient had more than one distinct stay on WEA, the final stay allowing a clear classification of weaning outcome was chosen.

Flow chart of the exclusion process indicating the reasons to exclude patients and the respective numbers of excluded patients. ICU, intensive care unit.
Patient and public involvement
Due to the retrospective characteristics of this study, no patients were involved in setting the research question, the outcome measures, or the design or carrying out of the study. The result of the study will be disseminated publicly via conference presentations and publication in an open-access journal.
Data collection
Patient data were retrieved from an electronic patient record system (medico//s, Siemens, Germany) and from an online patient data documentary system (IntelliSpace Critical Care and Anesthesia, ICCA Rev. F.01.01.001, Philips Electronics, Netherlands). The information on RBC transfusions was taken from the documentation system of the hospital’s Department of Transfusion Medicine (Lauris, Nexus Swisslab, Berlin, Germany). Acquired data consisted of demographic data, comorbidities, length of stay, duration of MV, number of RBC transfusions, Hb values on admission and as mean value throughout the stay, information regarding medication and RRT. The Simplified Acute Physiology Score II (SAPS II) and the Therapeutic Intervention Scoring System (TISS) were acquired on admission. Although all patients had a continuous hospital stay, the stay in the ICU, which preceded the WEA treatment, was partly collected and analysed separately. Anaemia was defined according to the WHO definition21 using a cut-off value of Hb <130 g/L in males and <120 g/L in females, respectively.
Statistical analysis
Statistical analysis was carried out using SAS V.9.4. Continuous variables were expressed as mean value and SD. For comparison between subcohorts of transfused and non-transfused patients, the difference in means±CI for continuous variables and the OR ±CI for categorical variables (where applicable) was used. Weaning failure, that is, a weaning classification of 3b and 3c, was defined as the primary endpoint. As a secondary endpoint, hospital mortality was chosen. To evaluate the influence of RBC transfusions or the number of RBC transfusions respectively in combination with other risk factors on the outcome we performed a multivariate logistic regression analysis. 16 risk factors for weaning failure and hospital mortality were identified through an extensive literature research. Beside the German S2k-Guideline for Prolonged Weaning,2 systematic reviews and articles22–27 were analysed. In consideration of their perceived importance for the outcome, their interest in relation to the research question and the availability of data, the predictive risk factors were selected by group consent of two physicians who are experienced in the treatment of patients undergoing prolonged weaning. The examined factors included age, gender, the sum of SAPS II and TISS on admission at ICU and at WEA, Hb concentration on admission at ICU and at WEA, mean Hb concentration during WEA stay, duration of MV, RBC transfusions at ICU and at WEA, usage of vasopressors and RRT during WEA stay and presence of comorbidities (coronary heart disease, cardiovascular risk factors and chronic obstructive pulmonary disease (COPD)) and the patient’s treating department (surgical or medical). In a first step, all parameters without relevant influence on the probability for a weaning failure were removed using a backward elimination approach with a significance level of α=0.2. Selected variables were inserted into the final model. The null hypothesis that the OR is OR=1 for all influence variables was tested with a Wald test at the 0.05 significance level. The linearity in the logit was tested graphically by plotting the observed values of continuous variables against the predicted logits of outcome parameters. The possible presence of multicollinearity was discussed using a correlation matrix making sure that each pair of variables had a Pearson correlation coefficient below 0.8 and a variance inflation factor below 2.5 to exclude excessive multicollinearity.28
Results
Clinical characteristics
During the observed period, 242 patients were admitted to the WEA, of whom 58 patients met exclusion criteria. The analysed dataset consisted of 184 patients. Thirty-six patients could not be weaned successfully, of whom 34 patients died in hospital (see figure 2) resulting in a hospital mortality rate of 18.5%. The mean length of stay on WEA was 24.0 (median 20) days with a mean MV duration of 336.7 hours (median 253). Patients who required no transfusions could be discharged from the WEA relevantly earlier compared with the transfusion group (mean: 16.5 vs 31.8; median: 15 vs 25.5) and required dramatically less time of MV until they could be liberated from it (184.30 vs 495.90; median: 156.5 vs 363) (see figure 3). The full clinical characteristics are given in table 1.
Clinical characteristics of the total population and subdivided according to received red blood cell transfusion on WEA

Percentage of weaning failure and hospital mortality grouped by the requirement for RBC transfusions. RBC, red blood cell.

Survival plots indicating (A) the length of stay on WEA and the probability of discharge and (B) the duration of MV and the probability of liberation from MV. Blue line: non-transfusion group, red line: transfusion group. MV, mechanical ventilation; WEA, weaning unit.
Hb and RBC transfusions
Already at admission to the ICU, 72.28% of the analysed population fulfilled the criteria of anaemia. During the period of ICU treatment, the mean Hb value dropped about 22.9±23.3 g/dL. At the end of the WEA stay, there was only one non-anaemic patient left.
While during acute critical care on ICU 139 patients, that is, 75.5% of the total population required RBC transfusion, this proportion decreased to 90 patients (48.9%) during treatment on WEA. Patients transfused on WEA, received 4.38 RBC units in the mean during WEA stay. These patients had a significantly lower mean Hb value (86.3±5.3 g/L) compared with those without need for RBC transfusion (95.8±10.5 g/L).
Organ dysfunction
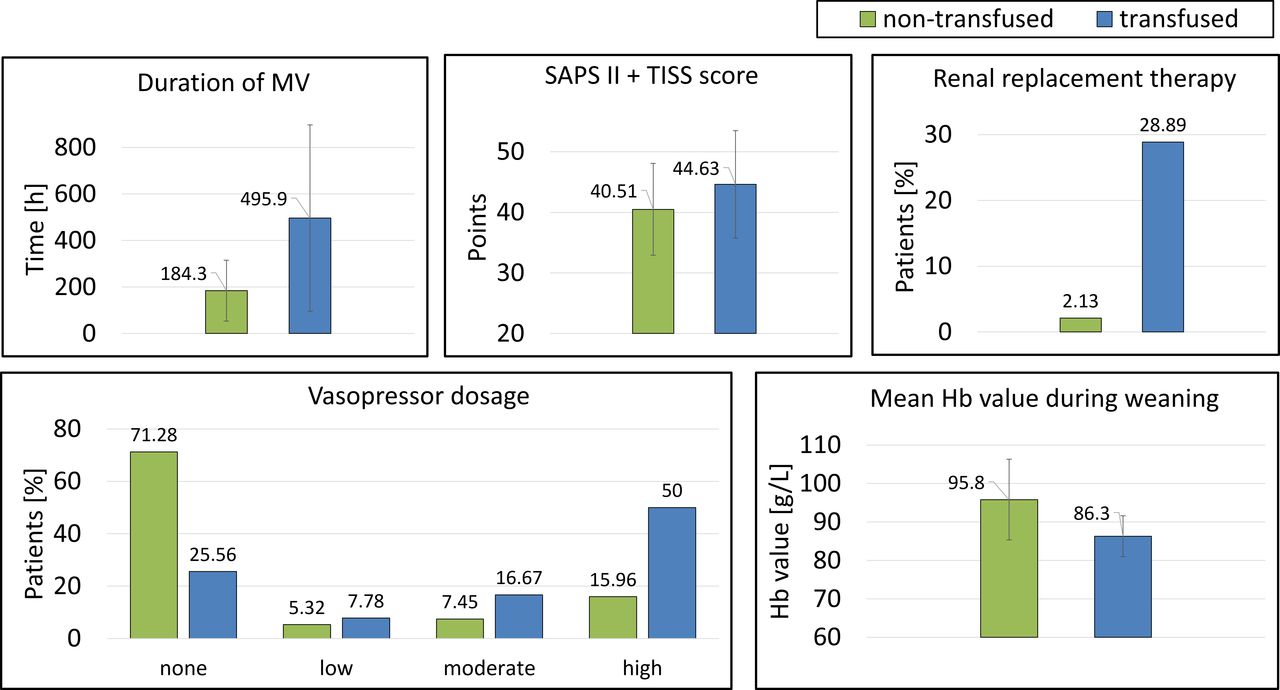
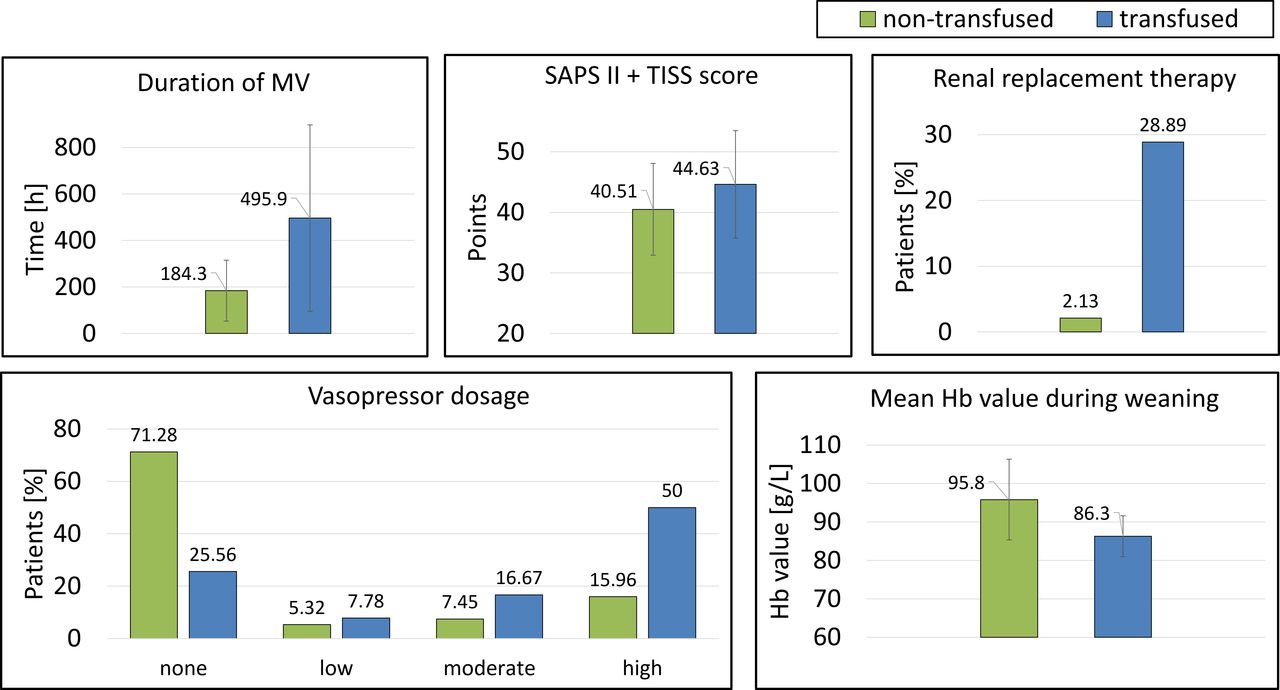
The patients requiring RBC transfusion showed findings indicating a severer condition in many organ systems. In addition to a longer duration of MV and a lower mean Hb value, which were already described above, the proportion of patients requiring RRT during weaning was also most pronounced in the transfusion group (2.1% vs 28.9%). A vast majority of non-transfused patients did not require vasopressors (71.3%) during their stay on WEA while a similar proportion in the transfusion group showed a need for vasopressors (74.4%), with 50% of transfused patients even requiring high doses. Moreover, the sum of the SAPS II and the TISS score at admission on WEA representing the general severity of disease was 4.12 (CI 1.73; 6.52) points higher in transfused patients (see figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration of the different degrees of disease severity grouped by the requirement for RBC transfusions based on different organ systems. Duration of MV on WEA, SAPS II+TISS on WEA admission and mean Hb value are given as mean±SD, renal replacement therapy and vasopressor usage are given as N (%). Hb, haemoglobin; MV, mechanical ventilation; RBC, red blood cell; SAPS II, Simplified Acute Physiology Score II; TISS, Therapeutic Intervention Scoring System; WEA, weaning unit.
Multivariate regression analysis
Dependent factor: weaning failure
To analyse the influence of certain risk factors on weaning failure as the primary endpoint, 16 potential risk factors (see Methods) were integrated into a multivariate logistic regression model. The null hypothesis that all ORs are OR=1 for all influence variables was rejected (Wald test=27.01, p<0.0001). After removal of the irrelevant parameters using a backward elimination approach, four parameters remained: (1) need for vasopressors on WEA, (2) duration of MV, (3) transfusion of RBC on WEA and (4) Hb concentration on admission WEA. The ORs and 95% CI are given in table 2.
Multivariate regression analysis, dependent variable: weaning failure
When the categorical variables for RBC transfusion (yes/no) were substituted by the absolute number of RBC units as input variables before the backward elimination, this caused some changes in the resulting model: the number of RBC units persisted in the final model due to the α=0.2 of the selection process but did not reach the stricter p value of <0.05 missing the significance level (OR 0.902; 95% CI 0.789 to 1.031, p=0.1292). Further, the variable ‘Hb value at admission on WEA’ was substituted by the variable ‘RRT on WEA’.
Dependent factor: hospital mortality
For the secondary endpoint, namely hospital mortality, another multivariate regression model was developed. When hospital mortality was used as dependent variable, the composition of risk factors changed. Despite its relevant impact on weaning failure, neither RBC transfusions on ICU nor on WEA seemed to have a relevant impact on mortality in our cohort and thus were removed early during the elimination process. The respective variables, the ORs and 95% CIs are given in table 3.
Multivariate regression analysis, dependent variable: hospital mortality
Discussion
Meaning of our findings
In our observational study, we found that nearly 50% of the included patients undergoing prolonged weaning from MV on a specialised weaning unit required one or more RBC transfusion during the weaning procedure. Patients who failed to be weaned successfully received significantly more RBC transfusions. In a multivariate analysis, RBC transfusions were significantly associated with weaning failure, but not mortality. The mean Hb value did not have a significant influence on the outcome. Given these results, it is rather confusing that in multivariate analysis, a higher Hb value at admission on WEA appeared to be associated with weaning failure. It should be noted, however, that this parameter only meets the much less stringent alpha of 0.2 used in feature selection and not the classical threshold for statistical significance of 0.05. The CI therefore clearly extends into the range that would allow a contrary conclusion, leaving the relevance of this result unclear.
A remarkable result of our study was that patients in the transfusion group showed characteristics that can be interpreted as a higher disease severity in several different aspects, indicated by higher scores of SAPS II and TISS, but also a higher requirement for vasopressors and RRT beyond the patients requiring RBC transfusion. According to this severe disease state, transfused patients showed a consistently lower mean Hb value than the non-transfused group. Obviously, the patients who did not require RBC transfusions were able to build up a higher Hb level without external support than the transfused group who received additional erythrocytes from external. Summarising our results, the question arises whether the debate of the optimal Hb level in patients undergoing prolonged weaning is not an illegitimate truncation. Research that focusses on an optimal Hb value for the weaning process may tend to ignore the additional problems which prevent a patient’s recovery and aim to treat rather a symptom than the underlying problem. Possibly, the need for transfusions rather forms a surrogate parameter for a persistency of a critical disease status, which encompasses not only an impaired haematopoiesis but also, for example, a failure of vasomotors or an insufficient kidney function. Thus, our results need to be interpreted with caution. In addition, the length of stay of transfused patients on the weaning ward was significantly longer than in the group without transfusion. This exposure interval could introduce bias, since the repeated diagnostic blood samples could cause anaemia and finally lead to RBC transfusion.29 The long duration of treatment could also, if perceived by the treating physicians as a failure of the previous therapy, lead them to consider further therapeutic options. Thus, the conscious or unconscious opinion that RBC transfusions might be beneficial for the patient may also play a role, an attitude whose incorrectness still persists among physicians despite growing evidence to the contrary.30 31
Comparison with other studies
Until today, the impact of transfusions on the outcome of patients in prolonged weaning is unknown. Patients with COPD typically show an increased work of breathing, which exceeds the respiratory muscle capacity and thus hampers an easy MV liberation. In this patient group, it was shown that RBC transfusion could reduce work of breathing and mean minute ventilation, while this effect in patients without pulmonary disease was lacking.32 According to that, Schönhofer et al reported a cases series of five anaemic COPD patients who were weaned successfully after increasing their Hb value.33 In a retrospective study including 138 difficult-to-wean patients, Lai et al found that patients with an Hb value above 80 g/L were significantly more likely to be successfully weaned compared with those with an Hb value below that threshold. In the same study, RBC transfusions were associated with weaning failure if they were given to patients with an Hb value above 100 g/L. Below that value they showed no effect.27 In 2019, Ghiani et al published an observational study on the influence of RBC transfusions in 378 prolonged weaning patients.11 Their results were similar with our findings within the usual range of variation. Deviating from our results, they did not find an association between RBC transfusion and weaning failure, but a trend to increased mortality in the transfusion group which was vice versa in our population. In agreement to our findings, they showed a higher disease severity within the transfusion group, as well. Several authors reported that a liberal transfusion strategy was not shown to be beneficial in MV patients,34 35 although the MV durations in these studies were regularly shorter and thus not comparable to patients in prolonged weaning. At first sight, our results seem to support this negative view on RBC transfusions. But as already pointed out, it is at least questionable whether the undesired outcome of the transfused patients in the observed population has a direct causal relationship with the received RBC transfusion. An important factor for anaemia in critically ill patients is a persisting systemic inflammation,36 which was already shown to impair erythropoiesis.37 38 Such an inflammatory process contributes to chronic critical illness which is common among long-term MV patients and has a considerably poor outcome.39 40 This link could offer an explanation for the apparent coincidence of lower Hb value, repeated need for RBC transfusions and poor outcome.
Strengths and limitations
In our study, we focused on patients in prolonged weaning admitted to a specialised weaning unit. These patients suffer from the most severe form of respiratory insufficiency and show several characteristics that may separate them from other ICU patients.41 The evidence in this field is insufficient and the role of Hb value and RBC transfusion is in our opinion scientifically and clinically relevant. By limiting the inclusion to patients from a specialised unit, it was possible to generate a profound population which was large especially compared with previous observational studies.32 33 This allowed us more complex statistical analyses like multivariate regression analyses. Nevertheless, it must be noted that the number of events per included variable are below the widely recommended lower limit of 5. Although there are authors who point out that the current evidence supporting EPV rules for binary logistic regression is weak and other factors like the total sample size also have an influence,42 we must acknowledge that our analysis may be underpowered to some extent.
Regarding the RBC transfusions, it should be noted that there were no strict rules or threshold values that would have led directly to a transfusion. The German guideline only provided basic orientation, which gave the attending physician a relatively large degree of freedom in making the indication. Information about the reasons for a physician’s decision to transfuse a certain patient in a certain situation, were lacking. Thus, it cannot be ruled out that the—possibly unconscious—perception of the patient’s poor condition may have influenced the decision for a transfusion. Due to the retrospective character of our study, several parameters, which would have been interesting, for example, for the correlation between RBC transfusions and infectious complications, were not available and prohibited an examination of this aspect. Missing data also led to exclusion of 58 patients due to transferral from or to external hospitals. Although the proportion of transfused patients in this excluded group was nearly identical to that of included patients, the weaning success rate was lower among the excluded patients (62% excluding vs 80% including) from whom a final weaning outcome was known. However, the introduction of bias through this event is as well possible. Finally, it cannot be ruled out that there is an influence of unmeasured or residual confounding from important factors that were not measured or included, especially given the complexity of the population. This is also due to the fact that risk factors included to the regression analysis were ultimately chosen via a consensus process between two physicians.
In the end, it must be considered that the explanatory power of a retrospective monocentric study is low. These studies are regularly prone to relevant bias and can only offer associations. In addition, if these associations are real and not caused by potential biases, they are not necessarily due to causal effects. Nevertheless, they can form the base to generate new hypotheses for prospective observational, or even randomised controlled trials.
Further research
The results of our retrospective analysis raise a number of questions which should be addressed in future prospective, ideally randomised controlled studies. The need for RBC transfusions seemed to be associated with a persisting critical state of disease, which negatively influences several organ functions contributing to a low Hb value, as well. Further research should focus on a more detailed characterisation of this critical condition that can be inferred from our results and its underlying processes and, in the case that its existence can be demonstrated, seek appropriate therapeutic approaches. Ultimately, our study cannot answer the question of whether patients in prolonged weaning benefit from actively increasing their Hb levels, since the transfusions observed in our study were not even sufficient to raise the Hb value of the transfusion group to the level of the non-transfused patients. This point still requires further examination, as well.
Data availability statement
Data are available on reasonable request. The patient datasets, which were generated and analysed in this study, are not publicly available due to medical confidentiality. They are available from the corresponding author in deidentified form on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the local ethical review board (EK 122/13) Ethics Committee, Faculty of Medicine, RWTH Aachen, Aachen, Germany). Due to the retrospective character of the study, the need for an informed consent was waived.
Acknowledgments
We would like to thank Marc Kaiser for his contribution in the conception of the study and his preparation of data extraction.
References
Footnotes
Contributors SJF und JB designed the study, SJF acquired and analysed the data and drafted the manuscript. All authors contributed to the interpretation of the data and revised the manuscript critically. All authors read and approved the final version of the manuscript. SJF acts as guarantor for this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.