Article Text

Abstract
Introduction Primary ciliary dyskinesia (PCD) is a rare, progressive, inherited ciliopathic disorder, which is incurable and frequently complicated by the development of bronchiectasis. There are few randomised controlled trials (RCTs) involving children and adults with PCD and thus evidence of efficacy for interventions are usually extrapolated from people with cystic fibrosis. Our planned RCT seeks to address some of these unmet needs by employing a currently prescribed (but unapproved for long-term use in PCD) macrolide antibiotic (azithromycin) and a novel mucolytic agent (erdosteine). The primary aim of our RCT is to determine whether regular oral azithromycin and erdosteine over a 12-month period reduces acute respiratory exacerbations among children and adults with PCD. Our primary hypothesis is that: people with PCD who regularly use oral azithromycin and/or erdosteine will have fewer exacerbations than those receiving the corresponding placebo medications. Our secondary aims are to determine the effect of the trial medications on PCD-specific quality-of-life (QoL) and other clinical outcomes (lung function, time-to-next exacerbation, hospitalisations) and nasopharyngeal bacterial carriage and antimicrobial resistance.
Methods and analysis We are currently undertaking a multicentre, double-blind, double-dummy RCT to evaluate whether 12 months of azithromycin and/or erdosteine is beneficial for children and adults with PCD. We plan to recruit 104 children and adults with PCD to a parallel, 2×2 partial factorial superiority RCT at five sites across Australia. Our primary endpoint is the rate of exacerbations over 12 months. Our main secondary outcomes are QoL, lung function and nasopharyngeal carriage by respiratory bacterial pathogens and their associated azithromycin resistance.
Ethics and dissemination Our RCT is conducted in accordance with Good Clinical Practice and the Australian legislation and National Health and Medical Research Council guidelines for ethical conduct of Research, including that for First Nations Australians.
Trial registration number ACTRN12619000564156.
- bronchiectasis
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The best approach to minimising respiratory compromise in people with primary ciliary dyskinesia (PCD) is uncertain, although one randomised controlled trial (RCT) showed that 6 months of azithromycin reduces acute respiratory exacerbations. However, azithromycin is often used empirically for much longer periods and further trials are needed to assess potential interventions.
WHAT THIS STUDY ADDS
Our RCT will evaluate whether a currently prescribed (but unapproved for long-term use in PCD) macrolide antibiotic (azithromycin) and a novel mucolytic agent (erdosteine) improve clinical outcomes and/or sustain lung function.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
If our hypotheses are correct, our RCT may influence national and international clinical practice involving the regular and/or prolonged use of azithromycin and/or erdosteine. Additionally, our planned cost-effectiveness analysis that will be informed by this RCT will be the first study of its kind to contribute to evidence on the economic management of people with PCD.
Introduction
Primary ciliary dyskinesia (PCD) is a rare, incurable, genetic disorder of ciliary structure and function.1 It is progressive in nature and characterised by ineffective mucus clearance from the airways resulting in recurrent or chronic respiratory infections. The lower airway infections and accompanying inflammation can result in bronchiectasis,2 leading eventually to respiratory failure and premature mortality.1 Recurrent upper airway infections causing persistent sino-ear-nasal disorders and hearing impairment are the most common early clinical manifestations of PCD.1 Despite the serious nature of PCD, there are large unmet needs in both its diagnosis and management.3 4
In addition to optimising general respiratory health (eg, vaccinations, enhancing nutrition, avoiding inhaled toxicants),2 current therapy for people with PCD seeks to improve mucociliary clearance and reduce infection and tissue injury from airway inflammation.1 5 However, current interventions used in PCD are without a strong evidence base and are generally extrapolated from studies and clinical experience gained from treating people with cystic fibrosis (CF) and other causes of bronchiectasis.1 2 5 These treatments in PCD include antibiotics for managing and preventing acute exacerbations,6 7 hypertonic saline (a mucolytic agent) in selected patients8 9and airway clearance therapies to ameliorate the deleterious effects of ciliary dysfunction on the lung.1
Reducing acute respiratory exacerbations in PCD is important as these episodes impair quality-of-life (QoL) and can lead to chronic infection, bronchiectasis and a decline in lung function.10 11 Recently, several RCTs have demonstrated that oral macrolides (mainly azithromycin) can significantly reduce exacerbations in people with bronchiectasis.12 13 A meta-analysis of nine randomised controlled trials (RCTs) involving 572 patients with non-CF bronchiectasis found that adults (risk ratio (RR)=1.66, 95% CI 1.37 to 2.02) and children (RR=5.03, 95% CI 2.02 to 12.50) receiving placebo were at significantly greater risk of exacerbations than those taking long-term (>3 months) macrolides.12 Nevertheless, data specific to people with PCD14 are needed, especially as azithromycin use by clinicians is highly variable.15 Moreover, not all people with PCD have bronchiectasis, and none of the RCTs of azithromycin in bronchiectasis have informed cost-effectiveness analyses.
The sole RCT that examined oral azithromycin (250 or 500 mg three times per week) enrolled 90 people with PCD,14 having planned to recruit 125 people.16 The participants’ mean age was 18.9 (SD=8.9) years in the azithromycin group and 19.7 (SD=10.8) years in the placebo group.14 We believe that although this RCT14 is important and showed that azithromycin more than halved the exacerbation rate in the active treatment group (RR=0.45, 95% CI 0.26 to 0.78), it has limited clinically applicability. There were just 26 (29%) participants aged ≤12 years and the trial drugs were only administered over a 6-month period. These limitations are relevant, as managing children with bronchiectasis differs in several aspects to adults,2 17 while longer-term RCTs (>12 months) in CF18 and bronchiectasis7 found the maximum effect of azithromycin extended beyond the 6-month period.7 Moreover, in clinical practice, azithromycin is usually prescribed for much longer durations, often years.15 Thus, further RCTs using azithromycin in people with PCD are required to inform clinical practice and health policies.
Our RCT plan includes assessing the risk/benefit of long-term antibiotics by measuring antimicrobial resistance (AMR) as clinical benefits arising from azithromycin must be balanced against possible adverse effects. Although nasopharyngeal cultures do not reliably predict lower airway bacteria,19 they provide good data on post-treatment AMR in colonising respiratory bacterial pathogens.6 7 We have identified previously that poor adherence (<70%) and living in remote communities are risk factors for AMR development in Australian First Nations children.20 However, these data need repeating in a different cohort, setting (urban centres) and clinical profile (PCD with or without bronchiectasis). Furthermore, azithromycin AMR in First Nations children should be contextualised, since in remote Australian communities, azithromycin is second only to amoxicillin as the most prescribed antibiotic and is used widely to treat skin, respiratory and genitourinary infections.21 Because of its long half-life, we will assess AMR in respiratory bacterial pathogens 3 months after ceasing azithromycin.
Chronic bronchitis, mucus hypersecretion and disruption of the mucociliary apparatus are all integral to the vicious cycle (vortex) hypothesis of bronchiectasis2 and also occur in people with PCD5 and chronic obstructive pulmonary disease (COPD).22 Despite the importance of these airway clearance mechanisms, there is only one small published RCT on mucolytics in people with PCD, which failed to identify a clinical benefit for hypertonic saline in 22 adult participants.23
Erdosteine is a novel thiol, synthesised to overcome problems (eg, non-efficacy and toxicity related to increased free thiols in the circulation) observed with other thiols (eg, N-acetylcysteine).22 Erdosteine has four main properties that could moderate the effects of ciliary dysfunction in the lungs (and thus potentially reduce exacerbations) in PCD. These are: (a) a mucolytic, modulating mucus production and increasing mucociliary transport; (b) an antioxidant, with (c) airway anti-inflammatory and (d) bacterial antiadhesion properties.22 24 As these actions target the underlying lung pathogenetic mechanisms in PCD,5 25 it is plausible that regular erdosteine could improve clinical outcomes.
Despite its potential benefit, there are no studies on erdosteine in PCD and only a single open-label RCT of erdosteine for 15-days in 30 elderly bronchiectasis patients that showed small but significant improvements in lung function and sputum volumes.26 Like macrolides, such medications are usually given for prolonged periods and a 15-day study is too short to assess its benefit. Erdosteine is licenced currently in 40 countries, including the UK (orphan drug in the USA,27 but not in Australia.27 RCTs in approximately 500 children aged >1 year with acute respiratory infections showed erdosteine for up to 2 weeks was well tolerated and significantly accelerated cough resolution in two studies28 29 but not in the third.30 Erdosteine has been used for longer-term studies in adults with chronic bronchitis/COPD, and a meta-analysis of individual patient data (n=1046) found it was associated with significant improvements in respiratory symptoms, including cough frequency and intensity, as well as sputum viscosity, when compared with either placebo or other mucolytics.31
Diagnosing PCD is not straightforward. It relies on gene analysis and interpreting cilia biopsy specimens.32–34 However, academic society guidelines provide differing recommendations for confirming a PCD diagnosis, and no single test or combination of tests conclusively excludes PCD in someone exhibiting a strong clinical phenotype.32 33 Importantly, in a recent comparative study, the different algorithms used to diagnose PCD resulted in a discordant diagnosis in 8/54 (15%) patients.35 Furthermore, acquired cilia ultrastructural defects or dyskinesia secondary to respiratory infections4 may be difficult to differentiate from PCD, particularly outside specialised testing centres.32 Consequently, cilia biopsies should only be undertaken at least 4–6 weeks after a viral infection or 2 weeks after full recovery from an illness.1 Unfortunately, this is virtually impossible in settings where recurrent ear and sino-nasal-pulmonary disease are highly prevalent as in Australian First Nations children living in remote communities where at any one time about 20% have chronic suppurative otitis media, up to 80% will be hospitalised during infancy, and as many as 1 in 68 will have a diagnosis of bronchiectasis.7 21 36 To help address these difficulties, a validated, simple diagnostic prediction tool (PICADAR) has been developed (box 1).37 Since current diagnostic methods are substantially limited,32–34 especially for First Nations children who have a high prevalence of bronchiectasis,7 our RCT includes children diagnosed by current traditional methods as well as those with a PICADAR score ≥5 and low nasal nitric oxide (nNO) or clinically suspected of having PCD.
PICADAR score37 is used to predict the likelihood of Primary Ciliary Dyskinesia in patients with chronic respiratory symptoms from early childhood. The features in the score are:
Born full term.
Chest symptoms present in the neonatal period (eg, tachypnoea, pneumonia, cough).
Admission to a neonatal unit.
Presence of a situs abnormality (heterotaxy).
Presence of congenital heart disease.
Presence of persistent perennial rhinitis.
Chronic ear or hearing symptoms.
Our RCT’s primary question is: among children and adults with PCD, can exacerbations be reduced during 12 months of treatment with: (a) oral azithromycin (given three times a week) compared with placebo (equivalent volume) or (b) oral erdosteine (given two times a day) compared with placebo (equivalent volume or capsule)?
Our primary hypothesis is that people with PCD who are prescribed either oral azithromycin or erdosteine for 12 months will have fewer exacerbations than those taking the corresponding placebo.
Our secondary aims are to evaluate the impact of the active treatments on:
PCD-specific QoL and other clinical outcomes (lung function, time-to-next exacerbation, hospitalisations).
Nasopharyngeal carriage of respiratory bacterial pathogens and their AMR to azithromycin.
Additionally, we will collect healthcare-related resource use for use in subsequent economic evaluation of these active treatments.
Our secondary hypotheses are that (a) azithromycin and/or erdosteine improve QoL and (b) azithromycin reduces bacterial carriage of respiratory pathogens, but with increased AMR to the antibiotic. Our additional hypothesis is that these active treatments will be associated with less exacerbation-related less resource use.
Methods and analysis
Design
We are undertaking a parallel, 2×2 partial factorial design, double-blind, double-dummy, superiority multicentre RCT (with concealed allocation) to determine the efficacy of 12 months of azithromycin and/or erdosteine at reducing acute respiratory exacerbations. We randomised the first participant on 21 July 2020 and we anticipate continuing recruitment until December 2022.
Study population
Inclusion criteria
(a) Children or adults aged 2–65 years, (b) known PCD (defined by gene analysis or by transmission electron microscopy and/or high-speed video microscopic analysis of cilia motility) or probable PCD defined as: (i) chronic wet/productive cough and a PICADAR score ≥5 with nNO <77 nL/min (or equivalent thresholds) on two separate occasions in children aged >5 years) or (ii) clinician assessment based on medical history, (c) ≥2 exacerbations or one hospitalisation for an acute respiratory exacerbation in the last 18 months AND (d) plan to remain at one of the study sites for at least 15 months.
Exclusion criteria
(i) CF, (ii) prior (last 6 months) or current infection with non-tuberculous mycobacteria, (iii) contraindication for macrolide or erdosteine (eg, liver dysfunction, hypersensitivity), (iv) pregnant, pregnancy planned (in next 12 months) or nursing mothers, (v) abnormal ECG (QTc >460 ms) or history of cardiac arrhythmia, (vi) previously randomised, (vii) hospitalised in the last 4 weeks for respiratory illness, OR (viii) active participation in another intervention trial.
Study sites
Our current study sites are: Queensland Children’s Hospital (Brisbane), Royal Children’s Hospital (Melbourne), Concord Repatriation Hospital (Sydney), Perth Children’s Hospital (Perth) and the Royal Darwin Hospital (Darwin).
Recruitment
Potential participants are identified from clinic lists and hospital databases and are approached by a research team member uninvolved in their clinical care. Also, our RCT has been uploaded onto the PCD Foundation and Lung Foundation Australia websites. Interested patients contacting one of the local sites are offered enrolment into the study if they fulfil the eligibility criteria.
A research team member then discusses the study with the parent/guardian/participant in detail using the consent documents, information booklet and interpreters (where appropriate). After all aspects of study are explained and agreed on, written informed or electronic consent (e-consent) are obtained from the parent/guardian/participant and/or assent/consent (age-dependent). Our processes are consistent with the principles of good clinical practice (GCP), the Declaration of Helsinki and the Australian National Health and Medical Research Council (NHMRC) requirements and cultural aspects of consent for First Nations Australians.
Study protocol
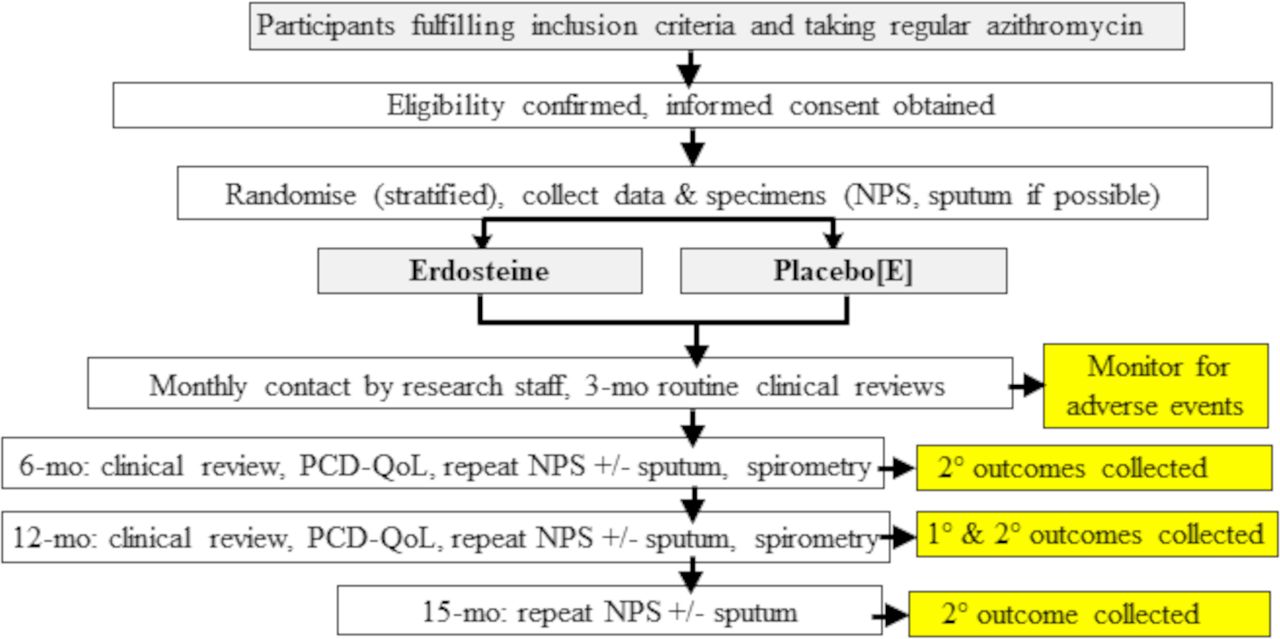
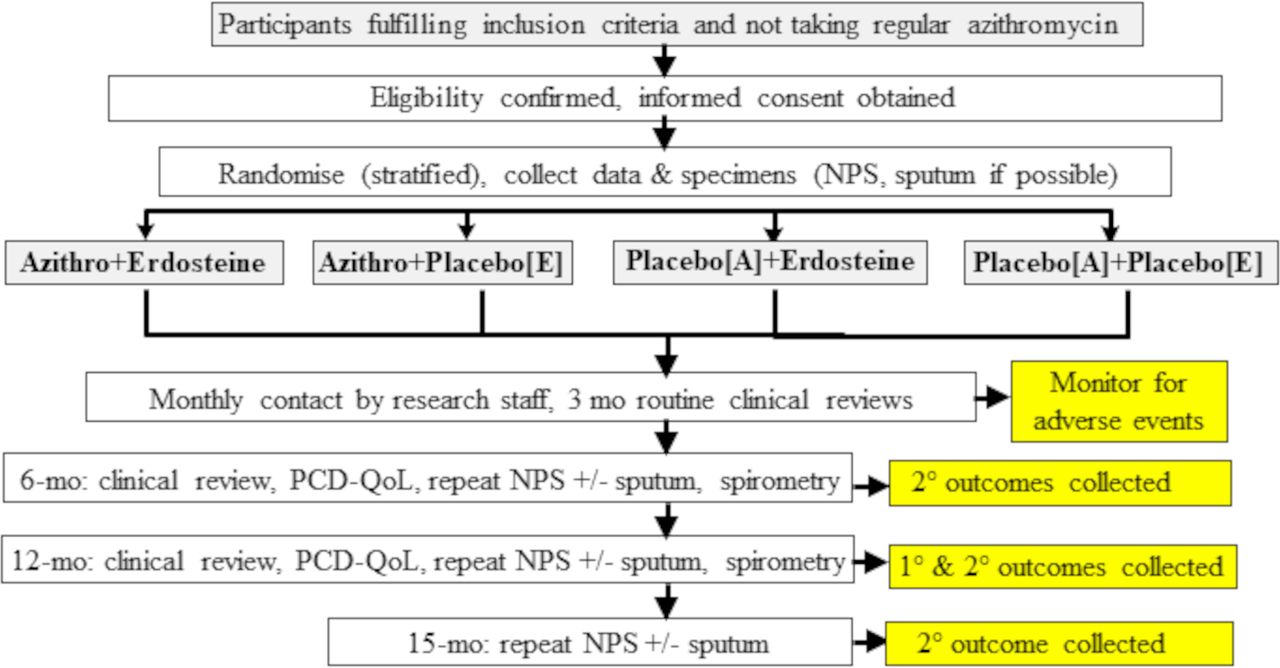
Participants are included in either the erdosteine intervention only (figure 1) or the azithromycin and erdosteine interventions (figure 2). The former is applied if the participant is receiving regular azithromycin and is judged by their primary respiratory physician to be at risk of becoming too unstable should azithromycin be discontinued. These participants are randomised to one of two arms: (a) erdosteine or (b) placebo-erdosteine (placebo[E]). Enrolled participants who are not taking regular azithromycin are randomised to one of the four arms: (c) azithromycin with erdosteine,

Participants taking regular azithromycin are randomised to only erdosteine/placebo arms. E, erdosteine; Mo, months; NPS, nasopharyngeal swabs; PCD-QoL, primary ciliary dyskinesia-quality of life.

{kind=link}
{kind=link}
Participants not taking regular azithromycin are randomised to both azithromycin/placebo and erdosteine/placebo arms. A, azithromycin; Azithro, azithromycin; E, erdosteine; Mo, months; NPS, nasopharyngeal swab; PCD-QoL, primary ciliary dyskinesia-quality of life.
(d) azithromycin with placebo[E], (e) placebo-azithromycin (placebo[A]) with erdosteine or,
(f) placebo[A] with placebo[E], summarised in the figures. All participants are managed according to local clinical protocols for their other PCD-related care.
Trial medications
Oral azithromycin suspension (200 mg/5 mL), at a dose of 10 mg/kg/dose (maximum 500 mg/dose), or placebo in equivalent volume is administered three times per week for 12 months. Azithromycin is repackaged in the same bottles as the placebo by PCI Pharma Services in Victoria where the placebo is manufactured. The reconstituted placebo matches the active preparation in smell, colour, taste, texture and consistency as well as packaging and labelling.
Erdosteine is available as powder for suspension (175 mg/5 mL) or capsules (300 mg) given two times a day for 12 months. Doses are weight-based, that is, <15 kg: 2.5 mL/dose; 15–19 kg: 5 mL/dose; 20–30 kg: 7.5 mL/dose or one capsule; >30kg: 10 mL/dose or one capsule. Equivalent placebo capsules or oral suspension also match the active preparation.
Randomisation, allocation concealment and blinding
Allocation is undertaken externally by the NHMRC Clinical Trial Centre (CTC), supervised by a statistician. We are using the minimisation method to ensure balance between treatment groups for (a) site (Brisbane, Melbourne, Sydney, Perth, Darwin), (b) age group (≤16, >16 years) and (c) PCD confirmation (definite/probable). A random component is being used. The CTC directly informs the local site’s pharmacist (or representative) who then dispenses the trial medications to the participant. Trial medications are dispensed every 3 months and adherence is monitored by return of bottles and collection of study medications.
People who are blinded to treatment allocation are those: receiving the treatment/s, administering the treatment/s, assessing the outcomes and analysing the results/data.
Data collection, monitoring and follow-up details
All collected data are recorded by GCP-trained researchers using standardised data sheets or on-line surveys (similar to our previous RCTs.6 7 38
At enrolment, demographic/clinical data, spirometry and specimens (nasopharyngeal swabs±sputum only) are collected. Demographics include age, gender, family and household size, smoking, family and immunisation history, medications and comorbidities are obtained from the carers/participant and/or reviewing the medical notes. Participants are contacted every month via electronic communication (email or text) or by telephone to monitor progress and adverse events (eg, vomiting, diarrhoea, rash) and economic data (eg, medical visits, treatments, other interventions, school/work absenteeism). They are also seen in the clinic 3-monthly (if they reside locally at one of the study sites) and specimens are collected at 6-month, 12-month and 15-month postrandomisation. Hospital records are also reviewed for hospitalisations. Additionally, at enrolment, a pregnancy test is undertaken if a female participant is aged ≥14 years and in adults, an ECG is performed.
Exit criteria include: consent withdrawn, severe study-related adverse events, intolerance to study medications or any other clinical indication as determined by study site doctors, treating clinicians or the independent data monitoring committee (iDMC).
Outcomes and endpoints
Our primary outcome is acute respiratory exacerbations whereby an episode is defined by an acute respiratory event that: (a) is treated with antibiotics AND (b) has an increase in sputum volume and/or purulence or >3 days of change in cough (at least 20% increase in cough score or change in quality (dry to wet/productive)) or physician confirmed acute change in respiratory rate, effort or chest signs.6 39 These are collected by participant reports and medical records. Our primary endpoint is the respiratory exacerbation rate by 12-month postrandomisation.
Other outcomes (see online supplemental file for further information) are:
Supplemental material
PCD-QoL scores at 12 months.
Time-to-next exacerbation. Defined from time of commencing trial medications to next respiratory exacerbation (defined above), measured in days.
Time-to-next respiratory-related hospitalisation.
Spirometry values (forced expiratory volume in 1 s (FEV1 %predicted) and forced vital capacity (FVC) %predicted, and FEV1/FVC ratio).
Adverse events, including gastrointestinal symptoms (eg, nausea, vomiting, abdominal pain, diarrhoea), headaches, rashes, use of additional non-macrolide antibiotics for non-pulmonary infections during the intervention, that is, for 12-month postrandomisation.
Presence of macrolide-resistant respiratory bacterial pathogens in the upper airways.
Healthcare resource use.
We also plan sensitivity analyses for exacerbation episodes meeting a different definition to our own based on the recommendations of a PCD consortium40 (box 2).
The definition of an acute respiratory exacerbation as recommended by the PCD consortium.40 A respiratory exacerbation is one that has ≥3 of the following criteria:
Increased cough.
Change in sputum volume and/or colour.
Increased shortness of breath perceived by parent/patient.
Decision to start or change antibiotic treatment because of perceived pulmonary symptoms.
Malaise, tiredness, fatigue or lethargy.
New or increased haemoptysis.
Temperature >380°C.
Data monitoring, management and analyses
All adverse events, including serious adverse events, are monitored by an iDMC, which was established and met prior to commencing the study. A First Nations Reference Group based at the Menzies School of Health Research (Darwin) oversees the cultural aspects of the study. Data coding and entry is coordinated in Brisbane and conducted in accordance with GCP.
The analyses will be directed by biostatisticians. Results will be reported and presented in accordance with CONSORT guidelines. We will use the ‘intention-to-treat’ approach for the main analyses. We also plan a ‘per-protocol’ analysis. Missing data will not be imputed. A detailed statistical analysis plan will be developed and approved by the iDMC before undertaking the final analysis. Any exploratory, posthoc or unplanned analysis will be identified clearly.
For the primary aims
Efficacy of the interventions will be determined by comparing outcomes of the active drugs versus their respective placebos. We will undertake two separate analyses testing efficacy of the drugs.
To assess azithromycin efficacy, we will compare the exacerbation rate in the azithromycin group (those receiving azithromycin+erdosteine or azithromycin+placebo[E]) with its control group (receiving erdosteine+placebo[A] or placebo[A]+placebo[E]).
To assess erdosteine efficacy, the exacerbation rate in those randomised to receive erdosteine (erdosteine±azithromycin or erdosteine±placebo[A]) will be compared with controls (receiving placebo[E]±azithromycin or placebo[E]±placebo[A]). We will use a negative binomial regression model (as recommended,41 including treatment group, and number of months in the study included as an offset) to determine between-group differences (with 95% CI), as done previously.7
For the secondary aims
The change (12 months minus baseline) in (a) respective domain scores of the QoL and (b) spirometry values (FEV1 %predicted, FVC %predicted and FEV1/FVC) between treatment arms will be analysed using analysis of covariance and presented as the mean difference (95% CI). A Kaplan-Meier curve will be constructed for each group (intervention vs respective controls) for time-to-the next exacerbation and respiratory-related hospitalisation and a log-rank test will be performed and a HR reported (using Cox regression model).6 7 We will follow recommendations for factorial trials and assume no interaction as the active drugs act through separate pathways.42
We will compare between-group nasopharyngeal respiratory bacterial pathogen colonisation and the AMR of these pathogens to azithromycin, as done previously using χ² tests expressed as the ORs (95% CI)6 7 at 12-month and 15-month postrandomisation.
For the additional aim
Healthcare resource use will be collected and summarised for each trial arm for inclusion in subsequent cost-effectiveness analyses making comparisons consistent with comparisons made in the primary analyses.
Sample size
Based on the primary outcome (exacerbation rate), we want to detect a significant difference between those allocated to (a) azithromycin vs controls and (b) erdosteine versus controls. We used a negative binomial model and assumed the dispersion parameter of 0.46,41 similar to that in our previous NHMRC-funded RCT.7 Using 90% power (alpha=0.05), we require final outcome data from 92 persons. To account for 10% attrition, we will enrol 104 people. Our calculations are based on the following: our previous RCT (n=89 participants)7 found a 50% relative reduction in exacerbations (95% CI 0.35 to 0.71) in the azithromycin group compared with placebo. For participants in the erdosteine group, a paediatric study (total n=158 in study) reported an absolute reduction in cough by 47%,29 while adults with COPD (total n=155) had 58% fewer days in hospital,43 compared with placebo. Our pilot work found exacerbation rates of 2.4/year. Assuming 50% reduction in exacerbations per intervention (vs associated placebo), we used the numbers in table 1 to calculate the sample size. At the time the study was being planned, we expected few participants to be taking azithromycin. However, when recruiting for the RCT, we realised many patients were taking azithromycin (see study limitations).
Numbers used to calculate our sample size
Trial oversight
The study is being monitored by an iDMC. The iDMC met before the study began and meets every 4–6 months. The trial is overseen by the chief investigators of the grant (listed below) and sponsored by the Menzies School of Health Research (Darwin, Australia).
Patient and public involvement
The grant submission was informed by both patient and public consultation. The formal research team and the original successful Australian Medical Research Future Funds (MRFF) grant applicants include a representative of the Lung Foundation of Australia and the president of PCD Australia and founding Member of both PCD Australia and the PCD Family Support Group (https://pcdaustralia.org.au/).
Discussion
With very few RCTs targeting people with PCD,1 5 14 23 current pulmonary management is largely extrapolated from CF-based studies and guidelines skewed towards patients with other causes of bronchiectasis.44 Given the very different pathobiological mechanisms between these conditions, there is a risk that some therapies that are beneficial to people with CF might have little benefit, or worse be detrimental to people with PCD, as demonstrated by dornase-alfa in those with idiopathic bronchiectasis.2 45 Our RCT tests two therapeutics based on a sound scientific rationale and addresses some of these unmet needs by employing a currently prescribed (but unapproved for long-term use in PCD) macrolide antibiotic (azithromycin) and a novel mucolytic agent (erdosteine).24
Choice of study outcomes
Respiratory exacerbations and QoL as outcomes were chosen when developing the study plan as they were considered the most important from the consumer perspective.46 Also, exacerbations have major negative health impacts on people with underlying lung diseases, including bronchiectasis,46 and are associated with increased psychological stress, impaired QoL, lung function decline and substantial healthcare costs.47 48 Thus, we chose exacerbation rate as our primary outcome.
We used the standard definition to identify acute exacerbations for determining our primary outcome,6 39 rather than the recent definition suggested by the PCD consortium.40 This was because: (a) the PCD consortium definition lacked a time duration for symptoms, which compromises its robustness as symptoms lasting a few hours could be classified as an exacerbation, and to date it has not been used in any published trials, and (b) in contrast, the standard definition has been validated49 and is in-line with current European Respiratory Society guidelines for bronchiectasis.13
QoL is important from the patients’ perspective.3 PCD-specific QoL tools developed for children50 and adults51 include non-pulmonary morbidities, for example, ear and sinus disease. Azithromycin and erdosteine may also impact favourably on these organs, but with no feasible and validated outcome measures for evaluating these non-pulmonary morbidities, we chose QoL as a composite patient-related outcome. Our other secondary outcomes (hospitalisation, lung function) are also important from both consumer and clinical perspectives.46 However, our trial may not be powered for these outcomes.
Potential study limitations
While our study has many novel and robust aspects, there are also limitations. First, ideally, all children would be randomised to one of the four arms. However, with the increasing recognition of the potential beneficial role of azithromycin, many people with PCD are now given long-term azithromycin routinely and the participants (and/or their physicians) are unwilling to cease their regular use of azithromycin. Thus, our RCT will be underpowered for assessing azithromycin efficacy.
Second, we included children with probable PCD (ie, without requiring a genetic or molecular diagnosis), but we believe that this is important in the context of the: (a) increasing appreciation of the difficulty in diagnosing PCD,34 (b) lack of a universal gold standard, (c) high prevalence of secondary cilia abnormalities in First Nations children, (d) new genetic abnormalities increasingly found in people without the typical PCD phenotype (ie, absence of daily cough, sino-pulmonary disease in early life),52 (e) confirmation of PCD using current diagnostic methods is limited to very high-resource settings and (f) although yet to be confirmed, people who are not of European or North American origin are likely to be more commonly affected by PCD.53 Importantly, we believe including this group will make our results more generalisable globally while not depriving those without a confirmed PCD diagnosis of a potential benefit. Our proposed intervention is not targeted at the underlying gene-defect, but as both azithromycin and erdosteine have broad effects they are likely beneficial when excessive lower airway secretions exist.
Third, in light of the adverse impact of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic (See the next section), our RCT is probably underpowered for assessing the efficacy of erdosteine for the primary outcome too.
Impact of the SARS-CoV-2 pandemic on the study
The current pandemic has substantially affected many aspects of our RCT. First, recruitment was severely affected by strict state and regional lockdowns and travel restrictions preventing face-to-face visits required by our study. Second, the incidence of exacerbations is substantially lower than that predicted, a phenomenon found worldwide coincident with the public health measures enacted to reduce transmission of SARS-CoV-2.54 Third, the reluctance of parents/patients to attend clinics during the pandemic prevented effective recruitment in some centres. Fourth, there are also financial consequences as no additional funds were made available by the funding body and research team members continued to be paid throughout this pandemic. Overall, we anticipate that our study’s findings will be substantially affected by the SARS-CoV-2 pandemic. Nevertheless, to minimise the impact of the pandemic, we instigated several mitigations strategies as outlined in the online supplemental file.
Summary
In this protocol paper, we described our double-blind, double-dummy, partial factorial, superiority RCT examining the clinical benefits of 12-month treatment with azithromycin and/or erdosteine for children and adults with PCD. Our consumer-informed RCT addresses the paucity of RCTs in the field. The multicentre nature of our study increases the generalisability of the future findings of our RCT.
We also plan additional side studies that have not been included in this protocol paper. These include a trial-based economic evaluation and undertaking whole exome sequencing (WES) to (a) evaluate the impact on the diagnostic odyssey, (b) compare with previous clinical test results as a proof-of-concept to determine the sensitivity and specificity of WES and (c) reinterrogate cases which are negative for mutations in known genes to see if we can identify new ones.
Ethics and dissemination
The Human Research Ethics Committees (HREC) of all the recruiting institutions and academic institutions approved the study: Children’s Health Queensland HREC/19/QCHQ/53457 (for Brisbane, Perth, Sydney and Melbourne sites), Queensland University of Technology HREC 1900001112; and Northern Territory Department of Health and Menzies School of Health Research HREC 2019–3464 for the Darwin site. All have approved the research protocol V.5.
We will publish the results in a major medical journal and share the outcomes with the academic and medical community, funding and relevant patient organisations, including the Darwin First Nations Reference Group.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Professors Dell, Leigh, Lucas and Quittner for allowing us to use their PCD-QoL tools in our RCT. We are grateful to members of the First Nations Reference Group of the Child Health Division at Menzies School of Health Research, Darwin (Bilawara Lee, Mark Mayo, Tracey Brand, Christine Campbell, Dennis Bonney, Lorna Murakami-Gold, Pirrawayinyi Puruntatameri, Veronica McClintic, Lesley Versteegh) for supporting this study and for overseeing the cultural aspects. We are also grateful to Professor Craig Mellis (Chair), Professor Tom Snelling, Professor Katherine Lee, Professor Hiran Selvadurai, Professor Paul Robinson and A/Professor Lucy Burr for voluntarily providing their time and expertise as members of the iDMC. We also thank the research staff (Dan Arnold, Jack Roberts, Samantha Grogan, Eleanor Ferguson, Julie Smith, Katharine Gantert, Stephanie Riley, Carli McClure) for facilitating the study. Likewise, we thank the many clinical staff of the participating hospitals for their kind assistance in our study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PJR and KG are joint senior authors.
Contributors ABC conceived and designed the study, drafted the manuscript and was primarily responsible for obtaining the grant. KG had a major input in editing the grant submission and manuscript. PR suggested the inclusion of erdosteine as an intervention. ABC, KG, PR, ELD, LCM, PJL, MDC, AS and GBM are chief investigators in the MRFF grant and contributed to study design and manuscript. AML also contributed to writing the grant and the study design. SMcP and YZ are leading the health economy aspects, HCS-V leading the respiratory pathogens component, ALC is currently coordinating all aspects of the project and STY and HOF are coordinating the biological specimens. JMM, DW and PM are medical practitioners in the RCT. LV, ES-S, HD and CK are community representatives and associate investigators of the grant (representing First Nations, Lung Foundation and PCD, respectively). HD and LV are First Nations advisors. MM coordinates all the ethics and governance aspects. SF is the trial coordinator in Brisbane. All authors read and approved the final manuscript.
Funding The study is funded by a 5-year Australian MRFF project grant (number 1169868) and supported by AusBREATHE (NHMRC Centre for Research Excellence in Bronchiectasis for Children grant number 1170958; www.crelungs.org.au). ABC is supported by a NHMRC senior practitioner fellowship (grant 1154302) and the Queensland Children’s Foundation (QCF). AMM-L is supported by a NHMRC investigator grant (ID 1158111). JMM is supported by QCF and Lung Foundation of Australia fellowships. WES and analysis is performed at the Translational Research Institute (TRI), Woolloongabba, Qld 4102, Australia. The TRI is supported by a grant from the Australian Government.
Disclaimer The views expressed in this publication are those of the authors and do not reflect the views of the MRFF/NHMRC.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.