Article Text

Abstract
Introduction Treatment pathways of patients with chronic obstructive pulmonary disease (COPD) receiving single-device dual therapies in England remain unclear. This study describes the characteristics of patients with COPD before initiating treatment with a single-device inhaled corticosteroid/long-acting β2-agonist (ICS/LABA) in primary care in England.
Methods This is a retrospective, descriptive study of linked primary and secondary healthcare data (Clinical Practice Research Datalink Aurum, Hospital Episode Statistics). Patients with COPD were indexed on first prescription of fixed-dose, single-device ICS/LABA (June 2015–December 2018). Demographics, clinical characteristics, prescribed treatments, healthcare resource use (HCRU) and direct healthcare costs were assessed over 12 months pre-index. Incident users (indexed on first ever prescription) could be non-triple users (no concomitant long-acting muscarinic antagonist at index); a subset were initial maintenance therapy (IMT) users (no history of pre-index maintenance therapy).
Results Overall, 13 451 incident users (non-triple users: 7448, 55.4%; IMT users: 5162, 38.4%) were indexed on beclomethasone dipropionate/formoterol (6122, 45.5%), budesonide/formoterol (2703, 20.1%) or Other ICS/LABA combinations (4626, 34.4%). Overall, 20.8% of incident users had comorbid asthma and 42.6% had ≥1 moderate-to-severe acute exacerbation of COPD pre-index. Baseline characteristics were similar across indexed therapies. At 3 months pre-index, 45.3% and 35.4% of non-triple and IMT users were receiving maintenance treatment. HCRU and direct healthcare costs were similar across indexed treatments. Prescribing patterns varied regionally.
Conclusion Patient characteristics, prior treatments, prior COPD-related HCRU and direct healthcare costs were similar across single-device ICS/LABAs in primary care in England. A high proportion of patients were not receiving any respiratory medication pre-index, indicating that prescribing in primary care in England is more closely aligned with national guidelines than global treatment strategies. Comorbid asthma may have influenced prescribing decisions. Less than half of users had preindex exacerbations, suggesting that ICS/LABA is not being prescribed principally based on exacerbation history.
- COPD pharmacology
- COPD epidemiology
- inhaler devices
Data availability statement
Data may be obtained from a third party and are not publicly available. The data analysed in this publication are derived from the Clinical Practice Research Datalink (www.cprd.com) and Hospital Episode Statistics database (https://digital.nhs.uk/ data-and-information/data-tools-and-services/data-services /hospital-episode-statistics). The authors had access to the study data for the purposes of this work only. Data were accessed through an existing GSK licence to address prespecified research questions only. Therefore, the data cannot be broadly disclosed or made publicly available at this time. Access to each database can be requested via the respective websites.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
This study aimed to clarify the extent of variability in baseline characteristics, treatment pathways and healthcare resource use (HCRU) in patients with chronic obstructive pulmonary disease (COPD) receiving inhaled corticosteroid/long-acting β2-agonist (ICS/LABA) therapy in primary care settings in England.
WHAT THIS STUDY ADDS
Patient characteristics, HCRU and direct healthcare costs were similar between patients with COPD receiving different single-device ICS/LABA therapies in England.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A high proportion of patients were not receiving any respiratory medication prior to initiating ICS/LABA, possibly reflecting patients with comorbid asthmatic features or indicating that prior to initiating dual therapy patients may not be receiving optimal pharmacological treatment.
These findings can help inform the design of future studies comparing the effectiveness of different single-device dual-inhaler therapies.
Introduction
Chronic obstructive pulmonary disease (COPD) is currently the third global leading cause of mortality, responsible for approximately 6% of the total deaths globally.1 In the UK, COPD is the second most common lung disease after asthma, affecting around 2% of the total population.2 COPD is associated with a substantial clinical and economic burden worldwide, with exacerbations contributing significantly to disease burden.3 4
Long-acting bronchodilators (including long-acting muscarinic antagonists (LAMA)) and long-acting β2-agonists (LABA)) either as monotherapy or in combination, are the mainstay of maintenance treatment for patients with COPD.3 Inhaled corticosteroids (ICS) are also indicated for some patients as maintenance therapy in combination with long-acting bronchodilators.3 5 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy report recommends a stepwise approach to treatment, with ICS/LABA dual therapy as a maintenance therapy option for patients at increased risk of exacerbations.3 The UK National Institute for Health and Care Excellence (NICE) guidelines also recommend ICS/LABA therapy for patients with COPD and features such as a history of asthma, an elevated blood eosinophil count or substantial variation in spirometry assessments over time.5–7 ICS/LABA therapy has been shown to improve lung function and health status and to reduce rates of moderate or severe exacerbations compared with either ICS or LABA alone.8–10
In the UK, five fixed-dose single-inhaler ICS/LABA therapies are licensed for treatment of COPD or asthma in adults: beclomethasone dipropionate/formoterol fumarate (BDP/FOR), budesonide/formoterol(BUD/FOR), fluticasone propionate/salmeterol (FP/SAL), fluticasone propionate/formoterol (FP/FOR) and fluticasone furoate/vilanterol (FF/VI).6 7 Of these, four combinations (BDP/FOR, BUD/FOR, FP/SAL and FF/VI) are licensed for treatment of COPD, although FF/VI is only indicated for patients with an exacerbation history and is not indicated as a general maintenance therapy for all patients with COPD.6 11
In England, it is unclear how different single-device ICS/LABA therapies are used in routine clinical practice. As such, there is a need to describe the treatment pathways and characteristics of patients receiving different treatments prior to ICS/LABA initiation to inform the design of future studies comparing the effectiveness of different single-device dual-inhaler therapies. The aim of this study was to provide a clear picture of the characteristics of a cohort of patients in England with COPD before initiation of dual therapy. This in turn can inform the design of future studies comparing the effectiveness of different single-device dual-inhaler therapies, as the characteristics of any baseline population will already have been clearly established by this study. The focus of the study was therefore to describe the characteristics of patients with COPD prior to initiation of treatment with a single-device ICS/LABA dual therapy, including baseline demographic and clinical characteristics, prior treatments prescribed, prior healthcare resource use (HCRU) and direct healthcare costs, in a general practice (GP) cohort in England.
Methods
Study design
This study was a retrospective, longitudinal cohort study using linked primary care electronic medical record data and secondary care administrative data from the Clinical Practice Research Datalink (CPRD-Aurum) and Hospital Episode Statistics (HES) databases,respectively. CPRD-Aurum contains longitudinal,representative anonymised electronic health records of primary care interactions in England. It provides data ondemographics, diagnosis, symptoms, prescriptions, referrals, immunisations, lifestyle factors, tests and results and represents approximately 13% of the living population as of September 2018.12 The HES data sets that were linked to CPRD-Aurum in this study were admitted patient care (including data on basic patient demographics, date and method of hospital admission and discharge, diagnoses, specialists seen and procedures undertaken), outpatient (including outpatient appointment dates, specialty,clinical diagnosis and procedures), and accident andemergency (A&E; including diagnoses, investigations and attendance outcomes).
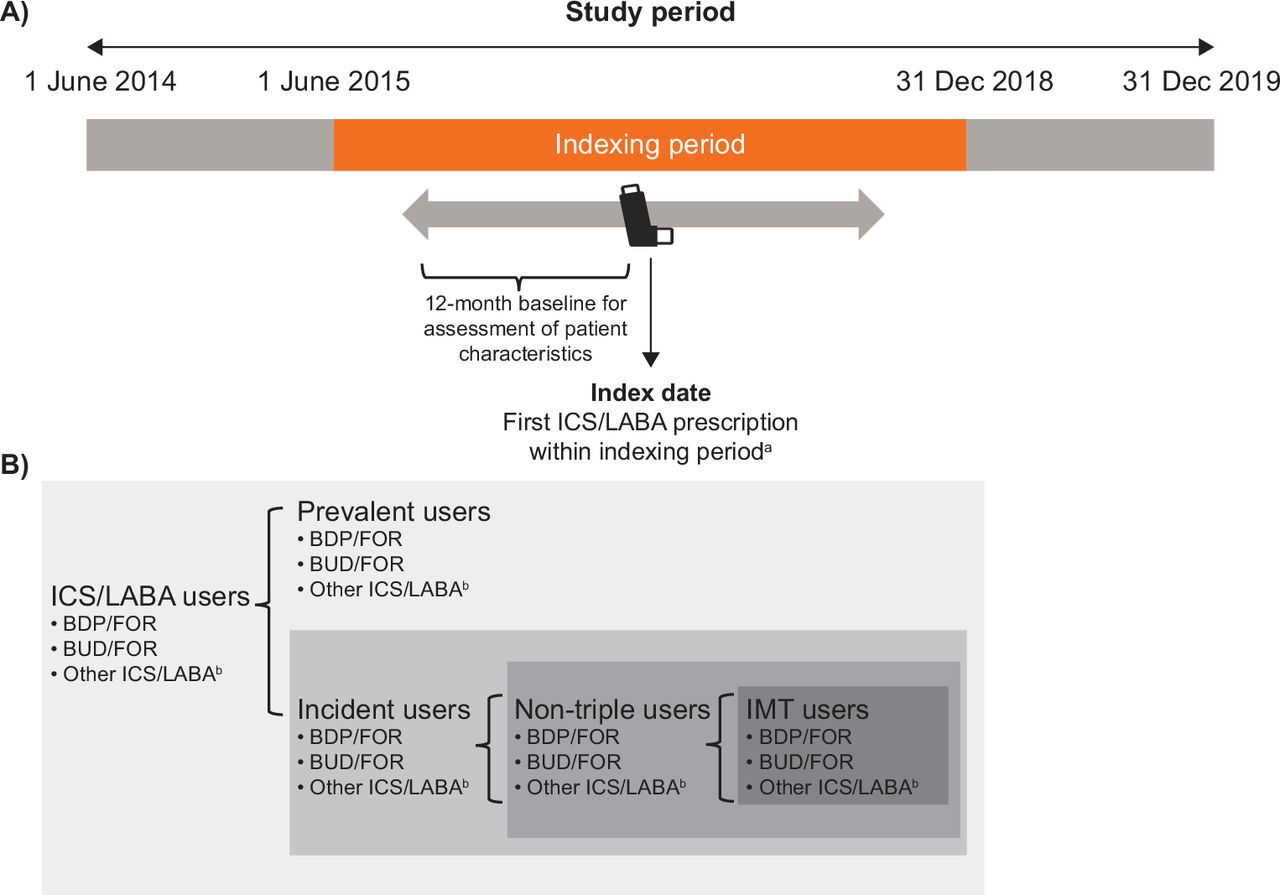
The indexing period spanned from 1 June 2015 to 31 December 2018 (figure 1A). The index date was defined as the earliest prescription of a single-device ICS/LABA therapy within the indexing period. The baseline period comprised the 12 months prior to index.

(A) Study design and (B) study cohort and subgroups. The IMT user and non-triple user cohorts were not mutually exclusive. aThe first single-inhaler ICS/LABA prescription within the indexing period was defined as the ‘index date’; bincluded fluticasone propionate/salmeterol, fluticasone propionate/formoterol fumarate and fluticasone furoate/vilanterol. BDP, beclomethasone dipropionate; BUD, budesonide; FOR, formoterol; ICS, inhaled corticosteroids; IMT, initial maintenance therapy; LABA, long-acting β2-agonist.
Study population
Eligible patients had ≥1 COPD diagnosis in the primary care setting at ≥35 years of age, had ≥1 prescription for a single-device ICS/LABA within the indexing period, a forced expiratory volume in 1 s to forced vital capacity (FEV1:FVC) ratio <0.7 at any time prior to and including the index date, ≥12 months of pre-index continuousregistration with a GP, had data eligible for linkage to HES and had no diagnosis of medical conditions incompatible with a COPD diagnosis at any time (including conditions related to lung or bronchial developmental anomalies, degenerative processes, pulmonary resection or other respiratory disorders that could interfere with COPD diagnosis).
ICS/LABA users were classified into two mutually exclusive cohorts, prevalent users and incident users. Prevalent users had ≥1 prescription of a single-device or an open combination ICS/LABA prior to the index date; incident users were those with no priorsingle-device or open combination ICS/LABA on the index date. Within the incident user cohort, non-triple users were those with no concomitant LAMA use on the index date; initial maintenance therapy (IMT) users were a subset of non-triple users who had no history ofmaintenance therapy. All cohorts were further stratified by indexed therapy (BDP/FOR, BUD/FOR or OtherICS/LABA combinations (included FP/SAL, FP/FOR and FF/VI); figure 1B).
Outcomes
Study outcomes assessed during the baseline period included the demographic and clinical characteristics of prevalent and incident users, COPD-related treatment use, all-cause and COPD-related HCRU, and all-cause and COPD-related direct healthcare costs in incident users at various time points.
Age was assessed as of the index date, sex and region were included as the last recorded at the time of data cut-off. Acute exacerbations of COPD (AECOPD; moderate-to-severe, moderate and severe), GOLD 2019 classification and blood eosinophil count were assessed in the 12 months prior to and including the index date. FEV1/FVC ratio, FEV1 % predicted, Medical Research Council (MRC) Dyspnoea Scale score and current asthma diagnosis were assessed in the 24 months prior to and including the index date (historical asthma was defined as an asthma diagnosis >24 months prior to the index date; the CPRD-Aurum database has a long median duration of follow-up, as such the number of patients with <24 months of prior data is expected to be low). Both current and historical were defined according to an algorithm using a set of validated specificdiagnosis codes, a commonly used method for classification in COPD studies.13 14 Body mass index, smoking status and comorbidities (reported based on the presence of diagnosis codes) were assessed at any time prior to and including the index date (not restrained by the study period). Where more than one value was available in the patient’s record, the most recent measurement prior to or on the index date was reported.
Moderate AECOPD was defined as any of the following (derived from primary care records): a prescription for antibiotics and oral corticosteroids for 5–14 days each, respiratory symptoms and a prescription of antibiotics or oral corticosteroids on the same day, a lowerrespiratory tract infection medical code or an AECOPD-specific medical code, as described previously.15 Severeexacerbations were those requiring hospital admission (derived from HES).
To evaluate treatment pathways in the baseline period, COPD-related inhaled therapy use was assessed inincident users only at 3, 6, 9 and 12 months pre-index (inclusive) and was categorised by mutually exclusive classes. Prescribing patterns in incident users were also investigated by AECOPD occurrence in the 12-month baseline period.
COPD-related and all-cause HCRU (medication use, GP consultations, outpatient visits, inpatient stays (hospitalisations) and A&E visits) and direct healthcare costs were assessed in incident users in the 12-month baseline period (0–3, >3–6, >6–12 and 0–12 months). Thecumulative length of stay (days) across all hospitalisations per patient with ≥1 hospitalisation was also reported.
HCRU and direct healthcare costs were classified as COPD-related if a COPD-related event (prescription medication, diagnosis or service provider) was recorded on the same day. Costs were derived from data reported by the Personal Social Service Resource Unit (PSSRU),16 the National Health Service (NHS) Drug Tariff compiled and provided by NHS Prescription Services17 and NHS England.18 For all sources of unit cost data, the most recent version available at the time of analysis was used (PSSRU 2019; Drug Tariff 2019; National Tariff 2019/2020).16–18
Statistical analysis
All patients who met the inclusion criteria were included in the study and no formal sample size calculations were performed. Outcomes were analysed descriptively. Medication use was reported as the number and percentage of prescriptions for each class of COPD medication; all other resources were reported as counts. All-cause and COPD-related direct healthcare costs were reported as total values and by HCRU type. Resource users were defined as those who had at least one unit of use for the respective healthcare service.
Patient and public involvement
Patients and the public were not involved in the design, or conduct, or reporting or dissemination plans of the research.
Results
Demographic and clinical characteristics
In total, 78 245 patients were prescribed single-device ICS/LABA during indexing and met the eligibility criteria. Of these, 64 794 (82.8%) were prevalent users and 13 451 (17.2%) were incident users. Among incident users, 7448 (55.4%) were non-triple users (BDP/FOR: n=3601; BUD/FOR: n=1432; Other ICS/LABAcombinations: n=2415) and 5162 (38.4%) patients were IMT users (BDP/FOR: n=2427; BUD/FOR: n=1056; Other ICS/LABA combinations: n=1679) (table 1 and online supplemental figure S1).
Supplemental material
Demographic and clinical characteristics of incident users
Baseline demographic and clinical characteristics were generally similar across prevalent and incident users, with the exception of the proportion of patients with current or historical asthma diagnosis (current: 37.3% prevalent vs 20.8% incident; historical: 62.1% prevalent vs 26.4% incident) (table 1 and online supplemental table S1). Baseline characteristics were similar across indexed therapies.
The majority of incident users were in the western regions. Numerically greater proportions of patients indexed on BDP/FOR were seen in the North West, Yorkshire and The Humber, East and West Midlands, East of England, and South Central regions relative to the overall proportion of users in those regions, while greater proportions of patients indexed on BUD/FOR were seen in the North East, and greater proportions of patients indexed on Other ICS/LABA combinations were found in London, South West and South East Coast (table 1 and online supplemental figure S2). Just under half of patients were in the two most deprived quintiles based on the 2015 Index of Multiple Deprivation (IMD) score (table 1 and online supplemental figure S2). Among incident users with available MRC dyspnoea scores (non-triple: 73.9%; IMT: 60.6%), the majority had scores of 1–3 (non-triple users: 67.6%; IMT users: 56.3%) andapproximately 31% of patients had GOLD grade ≥ 3 (severe to very severe airflow limitation). Eosinophil counts were equivalent among both non-triple and IMT users; 32.6% of patients had <150 cells/µL and 67.4% had ≥150 cells/µL. However, 44.9% and 44.2%, respectively, did not have eosinophil data available. Depression andrheumatoid/osteoarthritis were the most commoncomorbidities among non-triple and IMT user cohorts and these comorbidities were similar across indexed therapies.
In the incident user cohort, slightly more patients receiving Other ICS/LABA combinations experienced ≥1 moderate-to-severe AECOPD (45.2%) or had GOLD 2019 category C–D (47.7%) than those receivingBDP/FOR (41.5% and 43.1%) or BUD/FOR (40.1% and 42.5%). In both cohorts, slightly more patients receiving BDP/FOR had a current asthma diagnosis (IMT users: 31.6%; non-triple users: 27.8%) than those indexed on BUD/FOR (IMT users: 23.1%; non-triple users: 22.1%) or Other ICS/LABA combinations (IMT users: 25.3%; non-triple users: 23.4%).
Treatment pathways
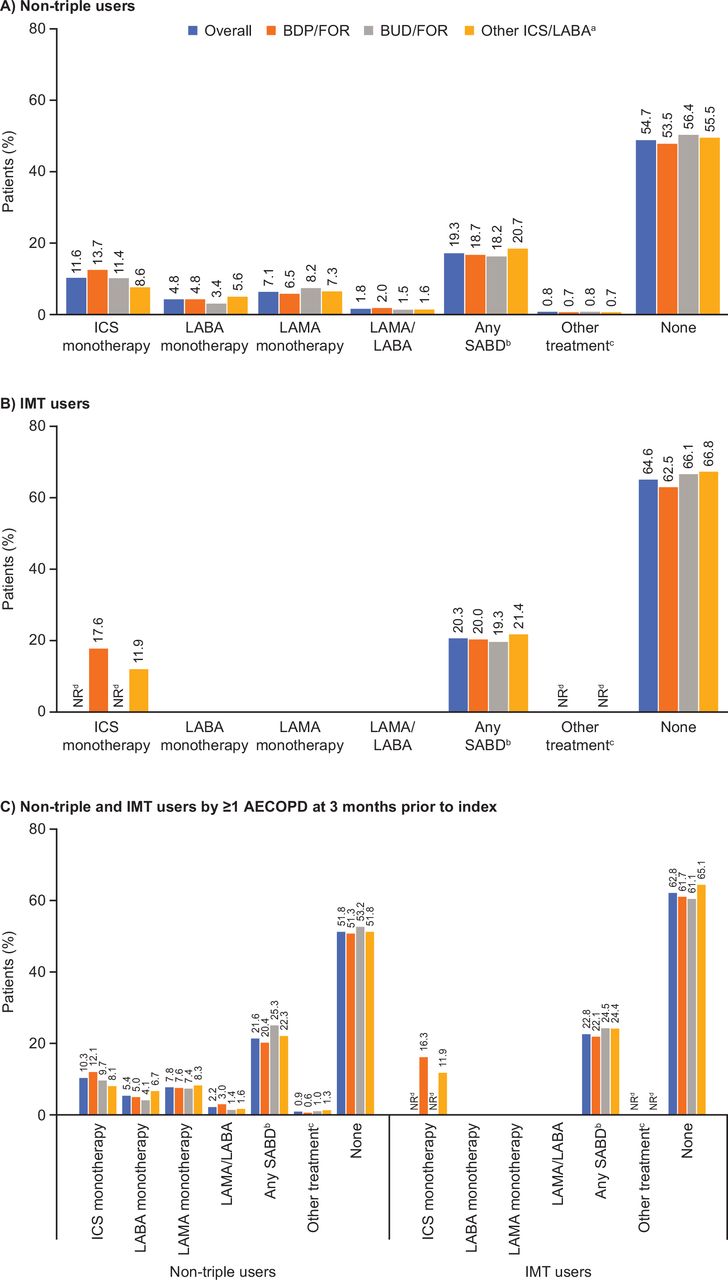
Overall, 55.5% of incident patients were not receiving an inhaled COPD therapy at 12 months prior to index, decreasing to 43.1% at 3 months. Short-acting bronchodilators and ICS monotherapy were the most frequently prescribed treatments among patients receiving inhaled therapy (figure 2A,B). Treatment pathways were similar across indexed therapies, with patients indexed on BDP/FOR comprising the greatest proportion of those prescribed ICS monotherapy at 3 months pre-index. Treatment patterns were generally similar at all other time points between non-triple and IMT users and across indexed therapies (online supplemental figure S3).
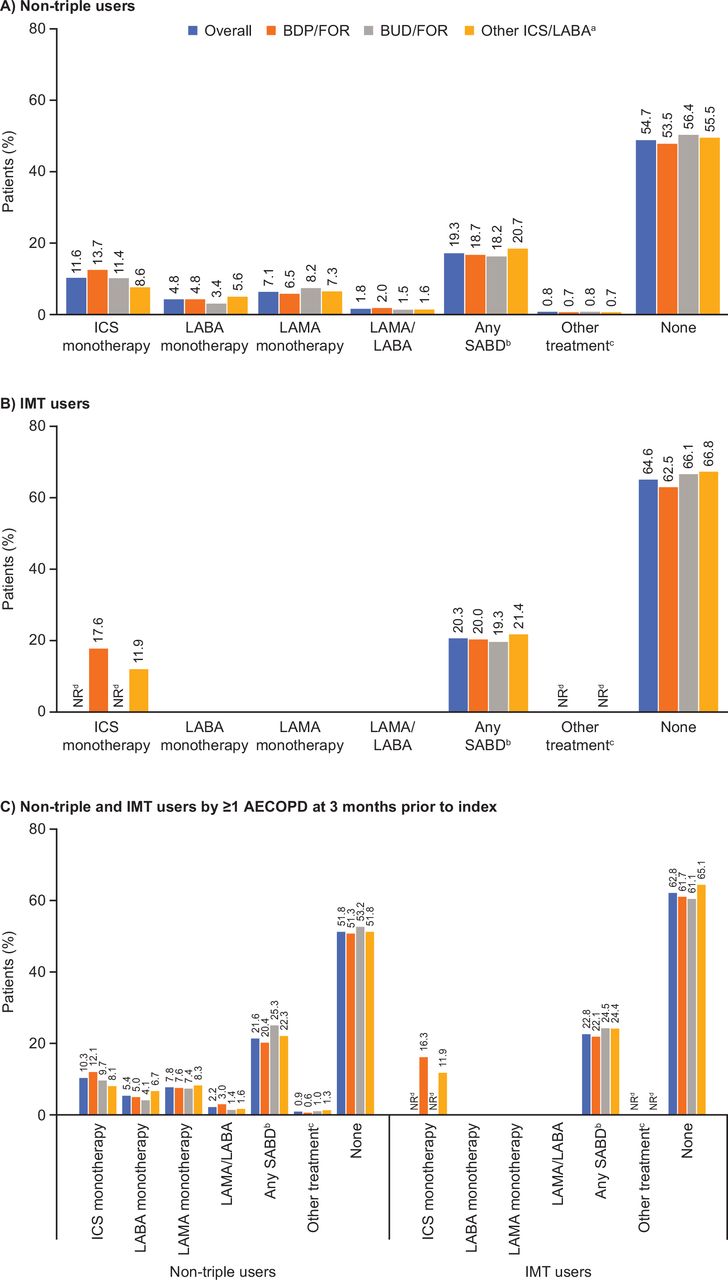
Treatment classes prescribed for (A) non-triple users or (B) IMT users at 3 months prior to index and (C) non-triple and IMT users at 3 months prior to index and by AECOPD status. aIncluded fluticasone propionate/salmeterol, fluticasone propionate/formoterol fumarate and fluticasone furoate/vilanterol; bincluded treatment with SABA, SAMA or SABA/SAMA fixed and open combinations; cincluded phosphodiesterase-4 inhibitors, methylxanthines and treatment combinations not reflected elsewhere; dresults based on small numbers of patients (n<5) were suppressed, as well as related values to protect primary suppression. AECOPD, acute exacerbation of chronic obstructive pulmonary disease; BDP, beclomethasone dipropionate; BUD, budesonide; FOR, formoterol; ICS, inhaled corticosteroids; IMT, initial maintenance therapy; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; NR, not reported; SABA, short-acting β2-agonist; SABD, short-acting bronchodilator; SAMA, short-acting muscarinic antagonist.
Of the incident patients who experienced ≥1 AECOPD during the 12-month baseline period, the majority were not receiving an inhaled COPD therapy at 3 months prior to index (figure 2C). In general, treatment patterns were similar across patients with and without an AECOPD in the year prior to index.
HCRU and direct healthcare costs
Over the 12 months pre-index, the mean totalCOPD-related direct healthcare costs for incident users were higher for non-triple users than IMT users (figure 3A). Minimal differences in direct COPD-related healthcare costs were observed between indexed therapies (figure 3 and online supplemental table S2). Inpatient stays were consistently the greatest contributor to meanCOPD-related direct healthcare costs among resource users across all indexed therapies and time periods (figure 3B and online supplemental table S2). Over the 12 months prior to index, the mean direct healthcare cost ofCOPD-related inpatient stays for the incident user cohort was £3533 (non-triple users: £3469; IMT users: £3104). Similar results were generally observed for all-cause direct healthcare costs (online supplemental table S3).

{kind=link}
{kind=link}
{kind=link}
Total COPD-related direct healthcare costs per (A) resource user overall and (B) per resource user and by HCRU over 12 months prior to index. aIncluded fluticasone propionate/salmeterol, fluticasone propionate/formoterol fumarate and fluticasone furoate/vilanterol. A&E, accident and emergency; BDP, beclomethasone dipropionate; BUD, budesonide; COPD, chronic obstructive pulmonary disease; FOR, formoterol; GP, general practice; HCRU, healthcare resource utilisation; ICS, inhaled corticosteroids; IMT, initial maintenance therapy; LABA, long-acting β2-agonist.
During the baseline period, COPD-related HCRU was similar across indexed therapies (table 2). All-cause HCRU was also similar across treatment cohorts (table 2 and online supplemental table S2). In the 12 months prior to index, non-triple users had a COPD-related cumulative mean (standard deviation) length of stay per patient of 7.0 days (16.0); the corresponding value for IMT users was 6.2 days (13.3). Patients indexed on Other ICS/LABA combinations had slightly longer COPD-related inpatient stays than those indexed on BDP/FOR (non-triple users: 7.0 days (16.1); IMT users: 6.0 days (11.6)) orBUD/FOR (non-triple users: 6.0 days (15.6); IMT users: 5.2 days (16.5)) in the same time period. Similar results were generally observed across indexed therapies and forall-cause inpatient stays.
COPD-related HCRU for incident users over 12 months and at 0–3 months prior to index in incident users
Discussion
This study retrospectively assessed the characteristics of patients with COPD receiving ICS/LABA therapy in a primary care setting in England. Overall, in the 12 months prior to index, demographics and clinicalcharacteristics in this patient population were generally similar across indexed therapies. Compared with those receiving BDP/FOR or BUD/FOR, incident users indexed on Other ICS/LABA combinations appeared to have more severe disease based on their history of moderate/severe AECOPD and GOLD 2019 categorisation. Patients who had received ICS/LABA therapy prior to index (prevalent users) also showed evidence of more severe disease and had a higher prevalence of comorbidities (including asthma) than those who had not received ICS/LABA therapy prior to index (incident users).
The GOLD strategy report and the UK NICEguidelines suggest that ICS/LABA may be prescribed as IMT for patients with COPD and a history of asthma.3 5 Our finding that over 60% of prevalent users in England had a history of asthma suggests that these patients may frequently be prescribed ICS/LABA. Moreover,approximately 20% of incident users had a current asthma diagnosis, further suggesting that ICS/LABA may have been prescribed for that reason and as per UK NICE guidelines.
The GOLD strategy report recommendsconsideration of ICS/LABA as IMT for patients with a history of asthma or patients with a significant exacerbation history and a blood eosinophil count >300 cells/µL and a stepwise escalation from a LAMA or a LABA toICS/LABA (guided by blood eosinophil count) for patients who continue to experience exacerbations.3 In this study, fewer than 20% of incident users were receiving an LAMA prior to an ICS/LABA and over one-third were IMT users receiving no maintenance therapy for COPD before initiating treatment with an ICS/LABA. Less than half of incident users had an exacerbation during the baseline period, suggesting that ICS/LABA is not being prescribed based on exacerbation history, even though in COPD the primary role of ICS is to reduce the risk of exacerbations.3 19 Furthermore, approximately 50% of patients were not taking any treatment in the 3 months prior to initiating treatment with an ICS/LABA, which also provides evidence that prescribing patterns are not in accordance with the stepwise approach recommended by GOLD. These results suggest that this patientpopulation may not be optimally treated in England, although historical or current asthma may have influenced the prescribing decision. However, we cannot say with certainty that the GOLD strategy reportrecommendations were not being followed. For example, the mean blood eosinophil count <300 cells/µL does not take into account the distribution of eosinophil levels across the population, nor the potential reduction in levels in patients who may have been taking oral corticosteroids when blood tests were taken. This was accounted for within the methodology by only considering bloodeosinophil measurements not within 14 days of an AECOPD or prescription of oral corticosteroids. Conversely, the treatment patterns observed may be consistent with NICE guidelines, which recommend initiatingtreatment with ICS/LABA dual therapy in patients withasthmatic features.5 This is in line with several studies that have shown disparities between international treatment recommendations and national prescribing practices in the UK and in other countries.20–24
Disparities between a particular set ofrecommendations and prescribing practices in primary care may be related to variation in familiarity and implementation across different international, national and localguidelines.23 25 In support of this, we observed geographical variation in prescribing patterns, with most prevalent and incident users located in western regions, likely due to differing practices across local clinical commissioning groups and the greater representation of patients in these regions in the CPRD-Aurum database. In England, it has been identified that referrals, diagnosis andtreatments differ significantly across practices; aspects include quality of spirometry undertaken and interpretation of results, support for self-care and treatment optimisation.26 Furthermore, clinical commissioning groups may lead to different regional pricing and prescription switching, further influencing prescribing patterns in primary care. These patterns represent substantial variation in care given to patients with COPD within England; almost half of non-triple and IMT patients were in the two IMD quintiles indicative of greater deprivation. A recent post-hoc analysis of the Salford Lung Studies in COPD has also shown that 52% of participants included were in the most deprived quintile.27 While the level of deprivation did not influence treatment outcomes in the Salford Lung Studies, it was found to be associated with greater HCRU and costs.27 The geographical variation in prescribing patterns and its effects should be taken into closeconsideration in future observational studies as a potential confounding factor. This variation in care, along with the specifics of patients’ primary and secondary care, could affect outcomes and subsequently the generalisability of any findings from specific regions of England.Furthermore, this variation highlights how diagnostic andtreatment decisions by primary care physicians also drive prescribing patterns in conjunction with patients’characteristics. Further studies exploring the drivers behind inconsistent implementation and variation in treatment of patients diagnosed with COPD by GPs in primary care will be of interest, as the discrepancies in diagnosis and management suggest that prescribing patterns may be affected.26
Prior COPD-related and all-cause HCRU were similar between non-triple and IMT users and across indexed therapies, even though non-triple users experienced numerically more moderate-to-severe and moderate AECOPDs in the year prior to index and had clinical characteristics potentially indicative of more advanced disease than IMT users. The lack of numerical differences in total healthcare costs may be due to similar inpatient stay costs, which seemed to be the greatest contributor to COPD-related and all-cause healthcare costs among patients who used healthcare services. Inpatient stays seemed to be the main driver of costs even though only approximately one-third of patients had experienced an inpatient visit over the 12-month period prior to index; this is in line with several studies that have shownhospitalisations are the main drivers of direct healthcare costs in patients with COPD.4 28 29 Costs for GP visits werenumerically lower than for inpatient stays, even though nearly all patients (>99%) had GP consultations. In contrast, a previous UK retrospective study showed that GPinteractions contributed more to costs than moderate-to-severe exacerbations and non-COPD hospitalisations.30 This disparity may have arisen because a smaller proportion of patients with severe (FEV1 ≥30%–<50% predicted) or very severe COPD (FEV1 <30% predicted) were included in that study (27%) compared with the present study (approximately 32%–36%), as these patients would be expected to experience more frequent and severeexacerbations than populations with milder disease.
This study has several strengths, including thereal-world insight into prescribing patterns in England and the large cohort which is representative of the UK population. Patients with COPD are largely managed in the primary care setting in the UK and thusCPRD-Aurum adequately captures the majority of a patient’s COPD healthcare journey, even though it does not cover privately insured patients. This study is not without its limitations. First, only medications prescribed in the primary care setting were recorded, so patients may have initiated ICS/LABA therapy earlier than the index date if they received an earlier prescription through secondary care. Second, in this study, over 20% of patients had a current asthma diagnosis. In England, it has been shown that clinicians have difficulties diagnosing up to 19.8% of patients based on clinical presentation and spirometry results, which can lead to inappropriatediagnoses and treatment initiation.31 The approach used in this study does not allow for potential misdiagnosis of asthma as COPD and vice versa to be identified; as such, the potential inclusion of patients with asthma–COPD overlap syndrome cannot be ruled out. Similarly, COPD and COPD-related chronic airflow limitations were not differentiated; however, patients were required to have received a diagnosis of COPD, be at least 35 years of age and have an FEV1/FVC ratio of <0.7, in line with adefinition of COPD which was validated against patient notes.32 Third, approximately 25% of patients were missing MRC score and 25% of patients were missing GOLD status data; however, these were not necessary for inclusion in the study and as such did not impact therepresentativeness of the study sample. In addition, approximately 50% of patients were missing eosinophil count data, which precluded further analysis on whether this treatable trait is taken into account in ICS prescribing in a real-world setting in England. Patients with asthma and COPD may also require a different treatment from those with COPD only and could arguably be classified as having asthma–COPD overlap syndrome rather than asthma and COPD. However, suggested treatment generally involves both ICS and LABA therapy33 and they were considered appropriate to include in this cohort. Additionally, a small percentage of patients in the cohort are neither current nor historical smokers. However, the proportions of smokers in this study are in line with what would be expected in a population of patients with COPD in the UK.34 Finally, direct costs may have been underestimated as some tariffs are negotiated locally and not nationally.
Conclusions
This real-world study showed that patients with COPD initiating single-device ICS/LABA therapy in England had similar clinical characteristics, HCRU and direct healthcare costs across indexed therapies. Real-world prescribing in England appears to be more closely aligned with national guidelines than GOLD treatment strategy, although asthma may have influenced prescribingdecisions. Less than half of incident users had anexacerbation during the baseline period, suggesting thatICS/LABA is not being prescribed principally based onexacerbation history, even though the primary role of ICS treatment in patients with COPD is to reduce the risk of exacerbations. These findings can help inform the design of future studies comparing the effectiveness of different single-device dual-inhaler therapies.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data analysed in this publication are derived from the Clinical Practice Research Datalink (www.cprd.com) and Hospital Episode Statistics database (https://digital.nhs.uk/ data-and-information/data-tools-and-services/data-services /hospital-episode-statistics). The authors had access to the study data for the purposes of this work only. Data were accessed through an existing GSK licence to address prespecified research questions only. Therefore, the data cannot be broadly disclosed or made publicly available at this time. Access to each database can be requested via the respective websites.
Ethics statements
Patient consent for publication
Ethics approval
Approval of this study was provided by the GSK Protocol Review Committee and by the Independent Scientific Advisory Committee (ISAC), which reviewed the protocol and approved access to Clinical Practice Research Datalink data (ISAC study no: 20_000145). No personal subject contact or primary collection of individual human data occurred, and anonymised patient-level data were used in this analysis; patient consent was therefore not required.
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing and referencing) was provided by Maria Guillermina Casabona, PhD, of Fishawack Indicia, UK, part of Fishawack Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Two abstracts based on this study were previously presented as poster presentations at the ERS 2021 Congress and at the Virtual ISPOR Europe 2021 Congress.
Contributors All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, contributed to the writing and reviewing of the manuscript, and have given final approval of the version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. AC (guarantor), VB, GR, RWo, TT, RWi and ASI were involved in the conception and design of the study, acquisition of data, and data analysis and interpretation. CC and MD were involved in the conception and design of the study and in data analysis and interpretation.
Funding This study was funded by GSK (GSK study 214731). GSK-affiliated authors had a role in study design, data analysis, data interpretation and writing of the report and GSK funded the article processing charges and open access fee. Editorial support was also funded by GSK.
Competing interests AC, GR, CC, MD and ASI are employees of GSK and hold stock and shares at GSK. ASI is also a part-time member of the McMaster University faculty. VB, TT, RWo and RWi are employees of Adelphi Real World (or were at the time of the study), which received funding from GSK to conduct the study. Adelphi Real World is a business that provides consulting and other research services to pharmaceutical, device, government and non-government organisations. Adelphi Real World employees work with a variety of companies and organisations and are expressly prohibited from receiving any payment or honoraria directly from these organisations for services rendered.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.