Article Text

Abstract
Introduction Respiratory infections are ubiquitous. The COVID-19 pandemic has refocused our attention on how morbid and potentially fatal they can be, and how host factors have an impact on the clinical course and outcomes. Due to a range of vulnerabilities, patients with sarcoidosis may be at higher risk of poor outcomes from respiratory infections. The objective of the SARCoidosis Outcomes in all respiratory Viral Infectious Diseases (SARCOVID) Study is to determine the short-term and long-term impacts of respiratory viral illnesses (COVID-19 and non-COVID-19) in sarcoidosis.
Methods and analysis Up to 20 clinical sites across the USA are participating in the recruitment of 2000 patients for this observational, prospective study. To ensure that the study cohort is representative of the general population with sarcoidosis, participating sites include those dedicated to reaching under-represented minorities or patients from non-urban areas. Baseline data on demographic features, comorbidities, sarcoidosis characteristics and pre-enrolment lung function will be captured at study entry. During this 3-year study, all acute respiratory infectious events (from SARS-CoV-2 and any other respiratory pathogen) will be assessed and recorded at quarterly intervals. The level of required medical care and survival outcomes determine infection severity, and the impact of infection on quality of life measures will be recorded. Post-infection lung function and imaging results will measure the long-term impact on the trajectory of sarcoidosis. Patients will be analysed according to the clinical phenotypes of cardiac and fibrotic pulmonary sarcoidosis. Control groups include non-infected patients with sarcoidosis and patients with non-sarcoidosis interstitial lung disease.
Ethics and dissemination Each site received local institutional review board approval prior to enrolling patients, with the consent process determined by local institution standards. Data will be published in a timely manner (goal <12 months) at the conclusion of the 3-year follow-up period and will be made available upon request.
- Sarcoidosis
- Viral infection
- COVID-19
- Interstitial Fibrosis
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The risk of respiratory infections may be heightened for patients with sarcoidosis as they have high comorbidity burdens, are often on immune-suppressing therapies, and may have reduced pulmonary or cardiac function due to sarcoidosis.
WHAT THIS STUDY ADDS
The SARCoidosis Outcomes in all respiratory Viral Infectious Diseases (SARCOVID) Study is uniquely positioned to answer questions about respiratory infection outcomes, the risk associated with sarcoidosis treatment(s), and the toll of infections on quality of life and long-term functionality in sarcoidosis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Drawn from a large registry prospectively enrolling patients across a diversity of sites, the SARCOVID Study cohort is reflective of the diversity of demographic and clinical features of patients with sarcoidosis.
Introduction
Sarcoidosis is an inflammatory disease of unknown aetiology which triggers a range of proinflammatory and regulatory immune responses. The accumulation of macrophages which aggregate into granulomas at sites of disease is central to the pathophysiology.1 T helper 1 lymphocytes are amplified and are thought to augment macrophage recruitment and function. Key chemokines and cytokines which mediate these cellular events include IFNg (interferon gamma), tumour necrosis factor-α, interleukin 2, CXCL9 (chemokine ligand 9) and CXCL10 (chemokine ligand 10).2–4 Immunosuppressive therapies, when titrated to patient response, often induce clinical remission.5 6 However, disease recurrence is common following discontinuation of treatment,7 8 and many patients with disabling, progressive or potentially dangerous disease require long-term immunosuppression.
Sarcoidosis can affect the lungs, heart, central nervous system, eyes, skin and other organs.2 While multisystem disease is common, the lungs are the most frequently affected organ and nearly all patients have some degree of pulmonary involvement.3 Sarcoidosis-interstitial lung disease (sarcoid-ILD) encompasses inflammation, fibrosis or a mixture of these processes in the lung interstitium. The development of fibrotic sarcoid-ILD is a risk for lung function decline, respiratory failure and death,9 and thus is a key determinant of prognosis in sarcoidosis. While sarcoid-ILD accounts for an estimated 20% of ILD burden,10 11 it is under-represented in ILD research.
The demographic features of patients with sarcoidosis differ from those of other ILDs.12 Most patients with sarcoidosis are diagnosed as a young or middle-aged adult, and in the USA the incidence of sarcoidosis is up to three times higher for black patients compared with white patients.13 14 In addition, women are more likely than men to develop the disease, and black women have the highest rate of sarcoidosis among sociodemographic groups.14
Regardless of organ phenotype and demographic features, quality of life impairment is common in sarcoidosis.15 16 In a large survey, quality of life was the most important disease metric identified by patients.17 In addition to psychosocial strain, sarcoidosis is associated with work absenteeism, which is a risk for financial strain.18 19 For these and other reasons, including reduced lung reserve and the use of immunosuppression, patients with sarcoidosis may be more vulnerable than healthy people to the multifaceted impacts of respiratory infections (figure 1).
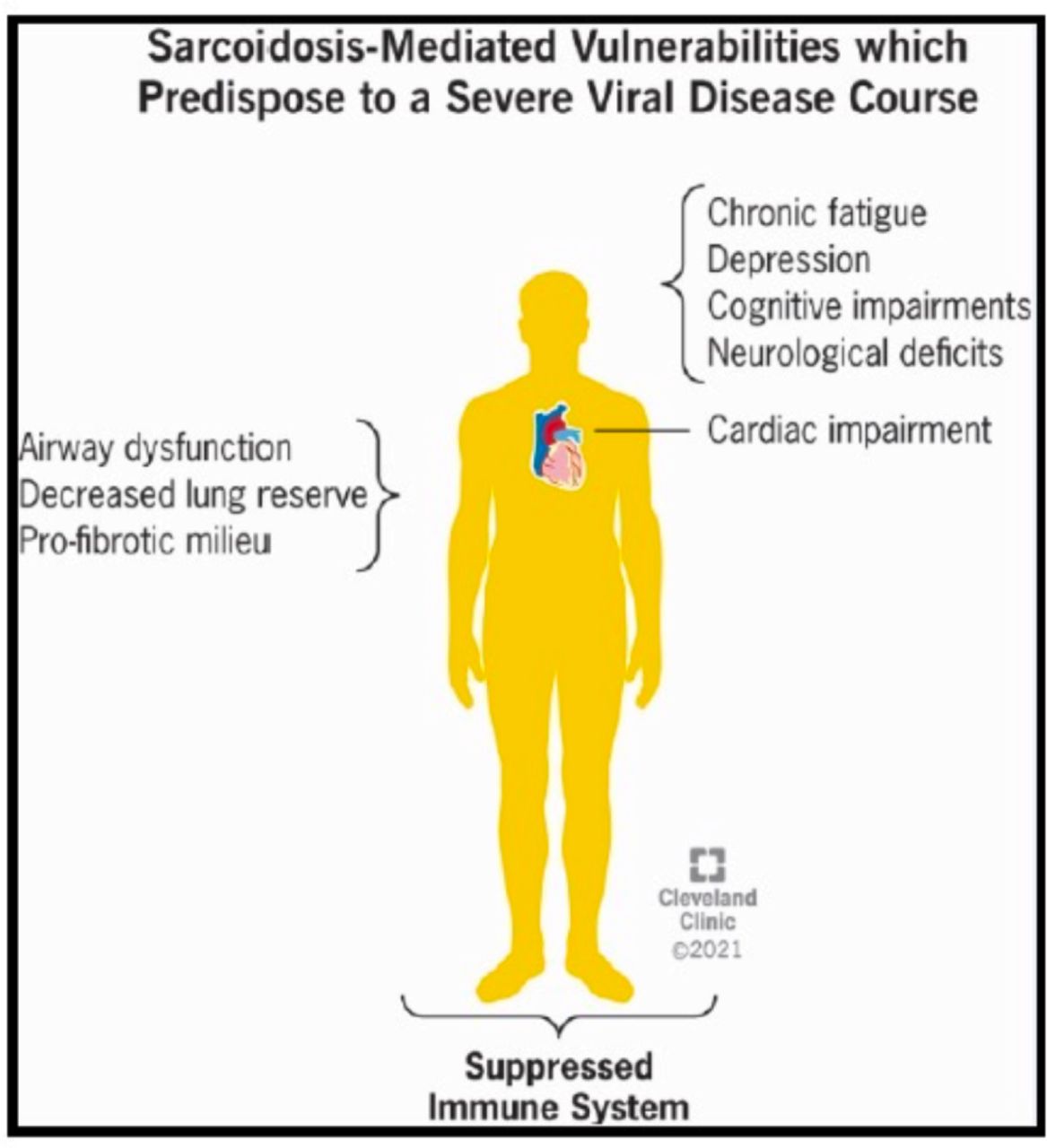
Sarcoidosis-related vulnerabilities which predispose to a more severe respiratory infectious disease course. Due to a variety of potential sarcoidosis-related impairments, infections with upper respiratory tract pathogens may cause higher burden or lead to a more severe course in patients with sarcoidosis.
SARS-CoV-2 has altered our understanding of the potential significance of common respiratory infections. Early in the pandemic, it became evident that patients with underlying cardiac20 or lung disease21 22 were at increased risk of severe COVID-19. Patients with ILD, for example, had higher hospital admission and mortality rates compared with patients without ILD, with ILD severity serving as an additional modifying risk factor for COVID-19 outcomes.23 24 Outcomes for patients with sarcoid-ILD are less clear, however, as few patients with sarcoidosis have been included in studies on ILD and COVID-19.23
In a retrospective review, the risk of hospitalisation or death from COVID-19 was not increased for patients with sarcoidosis compared with controls matched for age and comorbidities.25 While several other sarcoidosis-specific reports have been published, the findings are not widely applicable due to limitations such as small or non-diverse cohorts with non-severe disease,26–29 or selection bias in the other direction of limiting enrolment to hospitalised patients.28 Data from self-reported questionnaires given to patients with sarcoidosis offer some insight into the course of infection among patients fit enough to complete a survey,30 but the lack of a control group and an inability to verify data make extrapolation of outcomes to the general population with sarcoidosis difficult. A comprehensive assessment of outcomes is needed to measure impacts beyond the binary outcome of severe versus non-severe disease, and to evaluate the associated risk of sarcoidosis phenotype on outcomes. In addition to fibrotic sarcoid-ILD, the impact of underlying cardiac sarcoidosis on COVID-19 has not been measured, in spite of the identification of cardiac disease as a risk factor for poor outcomes in viral respiratory infections.31
While COVID-19 is a uniquely disruptive pandemic, a range of other respiratory pathogens continue to circulate. Nearly all of these pathogens can cause a severe illness, and even mild infection courses can trigger exacerbation of chronic lung diseases such as asthma, chronic obstructive pulmonary disease and cystic fibrosis.32 33 In addition to measuring outcomes of COVID-19, a key objective of the SARCoidosis Outcomes in all respiratory Viral Infectious Diseases (SARCOVID) Study is to assess the burden and impact of a broad range of respiratory infections in sarcoidosis, with the goal that elucidation of the short-term and long-term impacts of infection will be meaningful for patients and will inform clinical management.34–36
Rationale
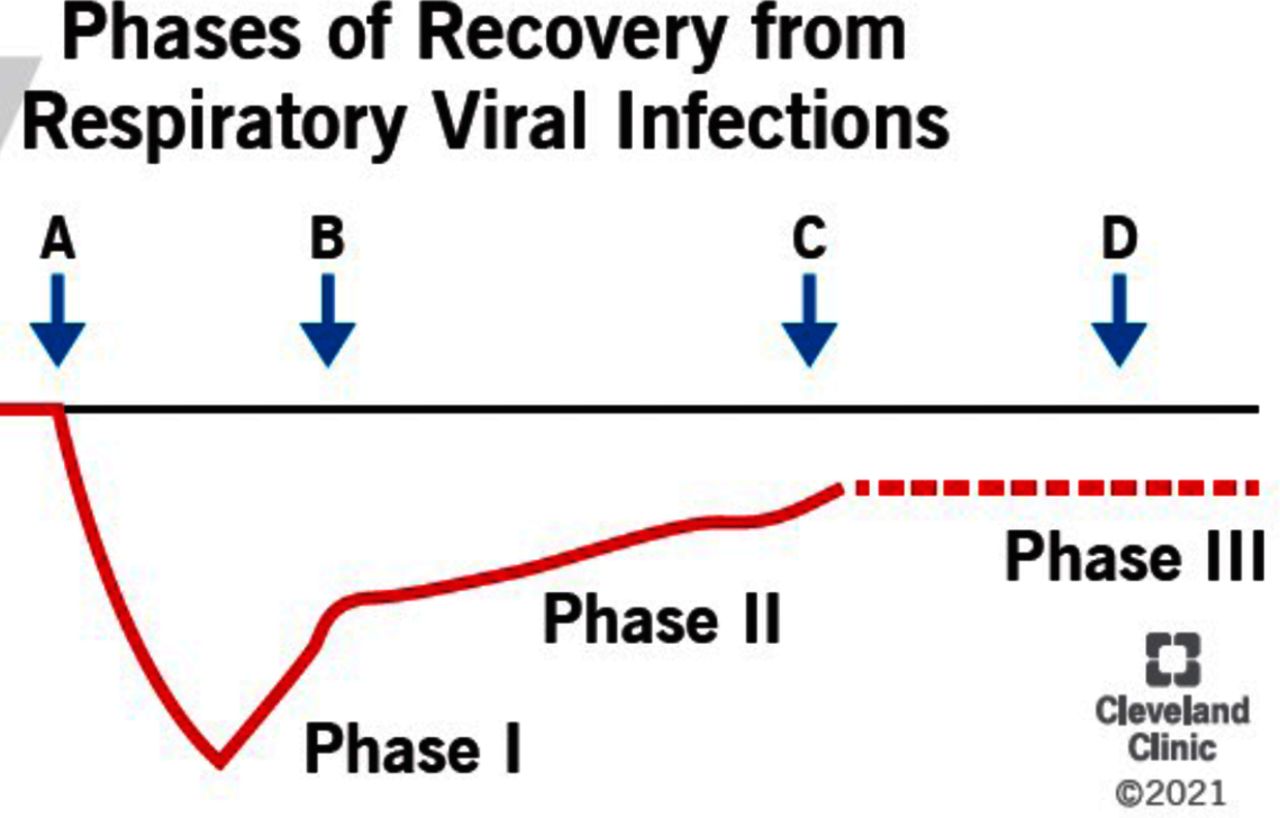
Whether certain clinical features of sarcoidosis increase the risk of severe respiratory viral illnesses remains unclear. In addition, it is unknown if or to what extent respiratory infections compound underlying functional and psychosocial burdens in sarcoidosis. Early in the pandemic, short-term outcomes of infection were the only feasible outcome to measure. However, a narrow focus on short-term outcomes fails to capture the potential morbidity associated with longer-term effects of infection and the complex nature of recovery (figure 2).37 The SARCOVID Study captures infectious event data over 3 years, corresponding to several respiratory viral seasons, and is the only study of its kind to assess both short-term and long-term outcomes in a diverse cohort of patients. In addition to functional assessments, the long-term effects of respiratory infections on the natural history of sarcoidosis are also measured. We hypothesise that, in sarcoidosis, patients with lung fibrosis or cardiac involvement are at increased risk of severe infection courses compared with patients with less dangerous phenotypes of sarcoidosis37 and that—across all phenotypes—respiratory infections will be associated with prolonged functionality declines.
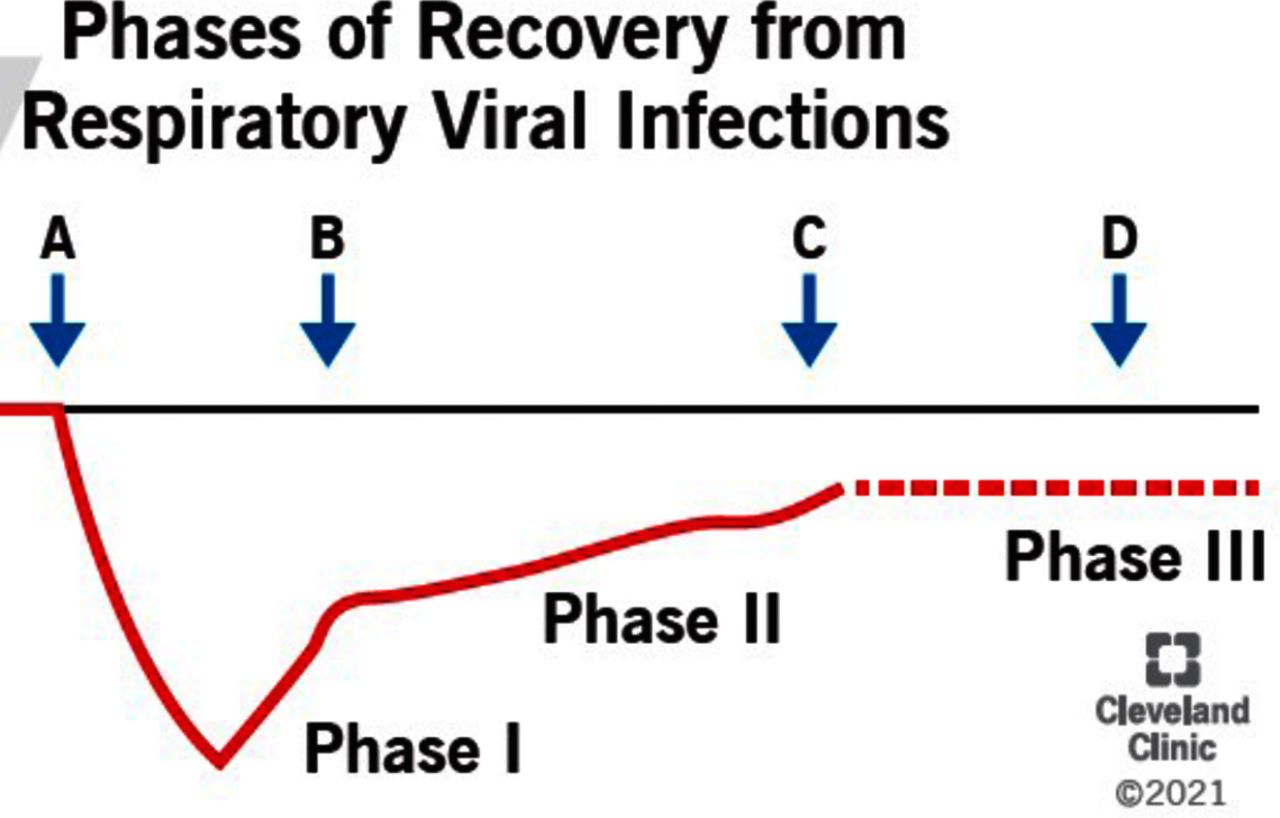
Phases of recovery from respiratory infections. Phases of recovery from respiratory infections include recovery from the acute illness (phase I) associated with microbial clearance and resolution of infectious symptoms; early ongoing recovery (phase II) which may occur over a longer period of time than acute recovery, and includes ongoing restoration of strength, stamina, and functionality; and, in some cases, permanent damage (eg, lung scarring) results from the infectious event and recovery is incomplete, resulting in a new baseline (phase III) with diminished functionality or well-being compared with pre-infection state. While only a small minority of patients will experience permanent damage, phase II of recovery is potentially common yet understudied. The recent recognition of ‘long COVID’ has focused attention on the burden of post-viral fatigue, among other lingering symptoms which afflict a substantial subset of patients with COVID-19.48–50 Arrows indicate acute infection onset (arrow A); recovery from acute infection (arrow B); recovery from phase II chronic symptoms (arrow C); residual damage (arrow D).
Study objectives
The primary aim of this study is to determine the association of clinical features and respiratory infection outcomes in sarcoidosis. To assess whether patients with fibrotic pulmonary or cardiac sarcoidosis have higher risk of severe infection, we will use multivariate analyses to measure the association of these phenotypes with binary measures of infection severity in SARS-CoV-2 and other respiratory infections (diagnosed by viral gene or antigen testing or clinical features), with severe infection defined by the need for new or augmented supplemental oxygen support, hospitalisation or death. For all patients with sarcoidosis, we will measure symptom duration, and compare pre-infection and post-infection psychosocial function including quality of life measures through the validated King’s Sarcoidosis Questionnaire.16 38 Our secondary aim is to measure the impact of respiratory infections on the trajectory of sarcoidosis through serial pulmonary function and imaging measures, and via a quarterly assessment of infection-mediated changes in sarcoidosis treatment.
Methods and analysis
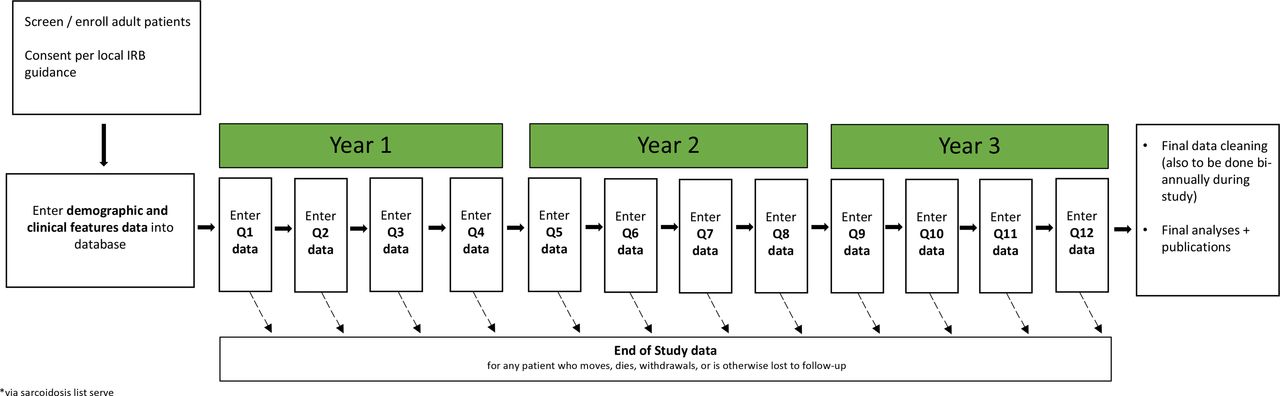
The SARCOVID Study is an observational, prospective study (figure 3). Patients with sarcoidosis meeting inclusion criteria will be enrolled at a diversity of study sites across the USA (tables 1 and 2). Select sites will also enrol patients with non-sarcoidosis ILD. Infection outcomes will be measured against the phenotypes of pulmonary fibrosis and cardiac involvement, and against other clinical features including treatment status. Non-infected patients with sarcoidosis—matched to age, race and sex—will serve as the primary comparison group. Patients with non-sarcoidosis ILD will also serve as a comparator group.
{kind=link}
{kind=link}
{kind=link}
Study design and timeline. Following the initial entry of demographic and detailed clinical details, infectious event data are collected and entered quarterly over 3 years. IRB, institutional review board.
Collaborating sites by geographical location in the USA
Inclusion and exclusion criteria along with case versus control groups
Recurrent assessments for infection events or changes in sarcoidosis status will be collected quarterly over 3 years. Each site has obtained institutional review board approval locally, with most sites initiating data collection near the time of the COVID-19 pandemic outbreak (winter 2020). Adult patients with an established diagnosis of sarcoidosis or another ILD and receiving clinical care at a recruiting site will be screened for study participation. At sites requiring informed consent, any patient meeting inclusion criteria and who provides consent will be enrolled.
To achieve the aims of the study, the recruitment goal of 2000 patients with sarcoidosis was established. This goal was based on an assumed rate of hospitalisation at 15% for patients with sarcoidosis who develop a viral infection.39 The recruitment goal of 2000 patients provides 80% power to detect a 20% absolute change in one of our primary outcomes, hospitalisation, with a two-sided α level of 0.05.
Patient and public involvement
Patients were not explicitly involved in the study design planning, which was done in an urgent fashion at the onset of the pandemic. However, our study design was heavily informed by patient survey data,17 which indicate that functionality and quality of life are critically important aspects of sarcoidosis management. Our data will be published in a timely manner at the conclusion of the 3-year follow-up period and will be made available upon request.
Clinical measures and outcomes
Data will be extracted from the electronic clinical records generated from routine clinical care. Data will be uploaded into local Research Electronic Data Capture (REDCap) databases,40 universal database template was provided to all participating centres, with the option for individual sites to add additional data fields to support local study interests. The database template consists of a defined set of fields for demographic and clinical features, including treatment status, as well as recurrent quarterly acute infection assessment forms (box 1).
Clinical research forms
Demographics and disease features
Race, ethnicity, sex, age at enrolment, tobacco use, body mass index.
Comorbidities: diabetes, hypertension, coronary artery disease, pulmonary hypertension, other cardiovascular disease, stroke, COPD, renal disease (dialysis dependent or independent), autoimmune disease, cancer (past or present), organ transplant, HIV, CVID, chronic lung infection, unknown or none.
If cancer history: cancer type, when diagnosed and current status.
Sarcoidosis
Biopsy/diagnosis date.
Organs affected: thoracic lymph nodes, extrathoracic lymph nodes, heart, eyes, skin, liver, spleen or bone marrow involvement, CNS, MSK/joints, other or unknown; Lofgren’s syndrome (Y/N).
If pulmonary involvement: fibrosis (Y/N based on CT findings of honeycombing, architectural distortion, fibrous bands, traction bronchiectasis, and/or asymmetric volume loss); assessment of disease activity in the past year (active disease defined by progression, active symptoms or treatment requiring).
Non-sarcoidosis ILD
Diagnosis date and how diagnosed.
ILD subtype: IPF, CTD-ILD, hypersensitivity pneumonitis, idiopathic NSIP, COP, chronic beryllium disease, asbestosis, other pneumoconiosis, RB-ILD/DIP, unclassifiable ILD, pulmonary alveolar proteinosis, Langerhans cell histiocytosis, other diffuse cystic lung disease, other ILD, unknown ILD.
IPAF: Y/N.
For all subjects
Objective measures at enrolment: lung function (FVC, absolute and % predicted), and resting and exertional oxygen saturation.
Sarcoidosis treatment(s) at enrolment: none, prednisone average daily dose 10 mg or lower, prednisone average daily dose >10 mg, methotrexate, TNF-α inhibitor, leflunomide, mycophenolate mofetil or azathioprine, hydroxychloroquine, JAK inhibitor, IL-6 inhibitor, acthar gel, rituximab, antifibrotic agent (nintedanib or pirfenidone).
Acute infection assessments (recurrent/quarterly)
Type of infection: SARS-CoV-2 (with questions about how diagnosed), influenza, respiratory syncytial virus, parainfluenza virus, human metapneumovirus, human rhinovirus, adenovirus, other.
Associated symptoms: temperature >100.0°F/37.8°C, new or worsening hypoxaemia, new or worsening shortness of breath, new or worsening cough, new or increase sputum production, new (non-fleeting) chest pain or pressure, haemoptysis, headache, GI symptoms, muscle aches or weakness, other symptoms not listed, asymptomatic or unknown.
Medical course: managed at home without a visit to a health facility, outpatient clinic or ER visit, hospital admission (regular floor), ICU admission but no mechanical ventilation, ICU admission with mechanical ventilation, referred to hospice, died due to infection or unknown.
Duration of illness: <14 days, 2–4 weeks, >1 month, unknown duration or not applicable: patient asymptomatic.
Treatments rendered: antiviral medications (Y/N) and/or antibiotics (Y/N).
Reported impact of infection on quality of life: missed work, quit working or lost job, missed a family event or holiday travel, less active lifestyle persisting >1 month after infection, other, none or unknown.
Measured impact of infection on quality of life: pre-infection and post-infection KSQ results (select sites).
Infection-related changes to medications: no known changes, stopped medication, reduced dosage or increased dosage.
Objective measures: updated PFT results (if testing done), and capture of CT chest done around time of infection (Y/N).
Chronic infections assessments (recurrent/yearly)
Type of infection: aspergillosis, histoplasmosis, Nocardia infection, MAI/MAC infection, chronic/recurrent colonisation with Pseudomonas or Burkholderia or Staphylococcus sp, other.
Signs and symptoms: chronic shortness of breath, chronic cough, chronic sputum production, recurrent chest tightness or wheezing, haemoptysis, recurrent fevers (temperature ≥100.4°F or 38.0°C), weight loss, fatigue, none of these symptoms, unknown.
Chronicity of infection.
Infection treatments (free text).
Miscellaneous comments box.
End of study
Date and reason for withdrawal: patient moved, died, was lost to follow-up, asked to be removed or other.
If died: was cause related to sarcoidosis or non-sarcoidosis ILD: Y/N.
Demographic details captured at enrolment include age, race, ethnicity and sex. A comprehensive smoking history assessment includes past or present tobacco use, vaping, marijuana use and other inhalations. A large range of comorbidities, with a focus on conditions which alter immune responses or modify infection risk, are captured. Sarcoidosis features include method of diagnosis, disease chronicity, organ involvement, CT chest imaging findings in patients with lung fibrosis, pre-infection treatment status, recent (within 12 months of enrolment) pre-infection, pulmonary function testing (PFT) and oxygen saturation results for testing done within a year prior to enrolment. Predefined phenotypes of interest include fibrotic pulmonary sarcoidosis and cardiac sarcoidosis. Systemic therapies for sarcoidosis are recorded at the time of enrolment and are updated in the recurrent quarterly assessments for infectious events (see below).41–43
Acute viral infection assessments are updated quarterly for 12 sequential quarters. Acute infection surveys query for all potential viral respiratory tract infections occurring within a defined quarter (box 1). For the purposes of this study, a respiratory infection event is any episode of acute (upper or lower) respiratory symptoms reported by the patient and labelled by the clinician as consistent with acute infection, or any incidentally detected infection in patients without respiratory symptoms but undergoing screening testing for respiratory viruses. For each infection, the method of diagnosis (including nasal/pharyngeal swab for viral gene or antigen testing, if available, to determine the specific pathogen), infection-related signs and symptoms, and severity of illness including highest level of medical care required are recorded. To measure the full impact of respiratory infections, we include symptom duration, missed work, impact on other social activities and potential adjustments to sarcoidosis treatment in our outcomes assessment. A subset of centres will collect pre-infection and post-infection health-related quality of life data through use of the validated King’s Sarcoidosis Questionnaire.16 38 Each quarterly update will include entries for new sarcoidosis organ involvement and any recently performed PFT data, as well as any change in sarcoidosis treatments.
An assessment for chronic infections also allows the capture of non-acute infections, such as aspergillosis or non-tuberculosis mycobacterial infections, and is an additional instrument included in our database. An end of study instrument is included for patients who die, are lost to follow-up, drop out or are otherwise unable to continue to be longitudinally followed.
Data management
Given the recurrent need for quarterly data collection, sites will maintain study identification keys, which will not be shared with the global database. Biannually, data from local REDCap databases will be uploaded to the global database administered by the University of Pennsylvania. Data use agreements with the University of Pennsylvania are in place for actively enrolling centres. Data evaluation will be performed regularly by lead study personnel experienced in database management, with additional oversight to be provided by the Biostatistics and Data Science Core at the University of Pennsylvania.
Study analysis
Our enrolment goal of 2000 was derived to ensure sufficient power to measure outcomes against discrete clinical features or phenotypes of sarcoidosis. Disease characteristics will be summarised using descriptive statistics (median values with SDs for continuous variables, and numbers with percentages for categorical variables). Continuous variables will be compared with the Student’s t-test, and categorical variables with the Pearson’s Χ2 test to determine if there is a significant difference in the sex, race and smoking backgrounds between groups of patients with mild versus severe infection outcomes in sarcoidosis. Logistic and Cox regression analyses will be conducted to identify potential predictors of outcomes.
Study potential
This study has several unique features which position it to answer important unknowns in sarcoidosis. First, the design of this study aims to improve health equity through proportional representation. The SARCOVID Study is projected to become one of the largest prospective clinical studies of sarcoidosis derived from clinician-verified disease characteristics. Recruiting from a broad swathe of geographical sites and catchment areas, we are enrolling a diverse cohort of patients, with strong representation from the south and from urban hospital centres; the latter are, in many cases, safety net hospitals, which have historically been under-represented in sarcoidosis research. Broad study site inclusion positions us to enrol a large number of black patients, which are not only at higher risk of having sarcoidosis, but also of having a more severe disease course.13 44–47
This is a time of heightened awareness of the importance of respiratory infections in health. Unique among other pandemic-inspired cohort studies, we measure the risk factors and outcomes associated with all respiratory infection events in sarcoidosis. Our results will be relevant to the clinical management of sarcoidosis long after the COVID-19 pandemic has run its course or settled into an endemic disease process.
Finally, while hospitalisation and death are critical outcomes in respiratory infections, other outcomes—while less dramatic—may contribute to the cumulative burden of infections in sarcoidosis. To capture their full morbidity, we measure a range of psychosocial, functional and well-being outcomes. Quality of life impairment is a major morbidity factor in sarcoidosis; superimposed damage from respiratory infections may compound this morbidity, and impact not only the well-being but also the livelihoods, financial security and vitality of patients.
Conclusion
The SARCOVID Study will provide unique insight into the full impact of respiratory infections in sarcoidosis, including impacts on quality of life and on the underlying disease course of sarcoidosis. While prior work has established an association of underlying lung impairment with poor outcomes from respiratory infections including COVID-19, the SARCOVID Study uniquely explores the broader dynamics of sarcoidosis clinical heterogeneity, including pulmonary and cardiac involvement, on outcomes from all respiratory infections. Data from this large, diverse study cohort will improve the understanding of the complex relationship between epidemiological factors, distinct clinical phenotypes of sarcoidosis and outcomes of respiratory illnesses. Identifying potentially modifiable risk factors is directly relevant to clinical management, and the results of this study hold the potential to improve the lives and outcomes of a vulnerable patient population while addressing health disparities for a historically understudied disease. This collaborative study also answers the call to match sarcoidosis research efforts to clinical centres which care for a high burden of sarcoidosis and serve a diverse range of patients, and to leverage large data from multisite research to better elucidate the full burden of sarcoidosis.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but institution-specific IRB approval exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful for all the work of local site investigators and study personnel (listed below) for the tremendous amount of work to initiate this study at their local centres, and for their ongoing efforts with data collection. The SARCOVID Study Group: Albany Medical Center: Om Dawani, Marc A Judson. Boston University/Boston Medical Center: Praveen Govender. Cleveland Clinic Foundation: Manuel L Ribeiro Neto, Daniel A Culver, Josh Schweta. East Carolina University: Ogugua Ndili Obi. Medical College of Wisconsin: Gabriel D Ryan (prior: Vijay Ramalingam). National Jewish Hospital: Lisa A Maier, Briana Barkes. New York University: Kerry M Hena. University of California San Diego: Bernie Y Sunwoo, Jisha K Joshua. University of Chicago: Mary E Strek, Rachel Strykowski, Spring Maleckar, Karina Mak. University of Florida (Gainsville): Divya C Patel, Diana Gomez Manjarres. University of Florida (Jacksonville): Mehdi Mirsaeidi. University of Illinois Chicago: Nadera Sweiss, Samreen Ahmed. University of Iowa: Alicia K Gerke. University of Miami: Ivan Escalona. University of Pennsylvania: Cheilonda Johnson, Karen Patterson. University of South Florida: Debabrata Bandyopadhyay. University of Texas: Rohini Samudralwar, Pascal L King. University of Utah: Stacey L Clardy, Mary Beth Scholand, Lawanda Esquibe, Jonathan P Boltax. Virginia Commonwealth University: Huzaefah J Syed. Yale University: Mridu Gulati. Study Monitoring Board and Scientific & Publication Committee: Karen Patterson, Divya Patel, Lisa Maier, Rohit Gupta, Ogugua Obi, Manny Ribeiro.
References
Footnotes
Contributors All authors have made substantial contributions to the work reported in this manuscript, including study design, writing and editing. All authors have approved of the final, submitted version of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.