Article Text

Abstract
Introduction Therapeutic advances have markedly increased life expectancy for those with cystic fibrosis (CF), resulting in a median predicted survival over 50 years. Consequently, people with CF (pwCF) are living through their reproductive years and the rate of pregnancy is rapidly rising. Despite the increased relevance of this topic, multicentre studies investigating the association between maternal health and choices made during pregnancy on maternal and fetal outcomes do not exist. Furthermore, there are very limited data on the outcomes following CF transmembrane conductance regulator (CFTR) modulator use during pregnancy and lactation.
Methods and analysis Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) is a prospective, multicentre observational clinical trial which will enrol approximately 285 pregnant pwCF including those who are modulator ineligible and those who choose to continue or discontinue CFTR modulator therapy during pregnancy and lactation. The primary aim of this 35-month study is to assess whether lung function changes during pregnancy differ based on the continued use of modulators or other factors such as pre-existing comorbid conditions. Secondary objectives include evaluation of pregnancy related and obstetrical complications and changes in mental health.
Ethics and dissemination The design of this study required special consideration of study burden on pregnant and lactating people with chronic illness in the setting of a substantial number of unanswered questions under these conditions. MAYFLOWERS is the first prospective clinical trial examining pregnancy in CF; the outcomes will guide providers on pregnancy management in pwCF and others with chronic respiratory disease.
- Cystic Fibrosis
- Bronchiectasis
- Rare lung diseases
Data availability statement
No data are available. NA.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
While a number of single-centre, and some multicentre cohort studies were previously conducted to evaluate the health of pregnant people with cystic fibrosis (pwCF), the data were collected retrospectively and in a therapeutic era prior to the widespread use of cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapy.
What this study adds
The Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) is the first prospective study of pregnancy in CF. It will also provide the first prospectively collected data on infants born to mothers with CF, and include outcome data for mothers and infants for 2 years following pregnancy.
How this study might affect research, practice and/or policy
The outcomes of the MAYFLOWERS study will guide providers on pregnancy management including glucose control and use or discontinuation of CFTR modulators in pwCF. Many of the outcomes will be relevant for other pregnant people with chronic respiratory disease.
Introduction
Advances in medical treatment have markedly increased life expectancy for those with cystic fibrosis (CF), resulting in a median survival over 50 years of age.1 This therapeutic success is anticipated to continue to increase survival. Consequently, people with CF (pwCF) are living through their reproductive years and the rate of pregnancy in pwCF is rising (figure 1). Therefore, issues related to the effects of pregnancy on pwCF and their infants require greater attention.
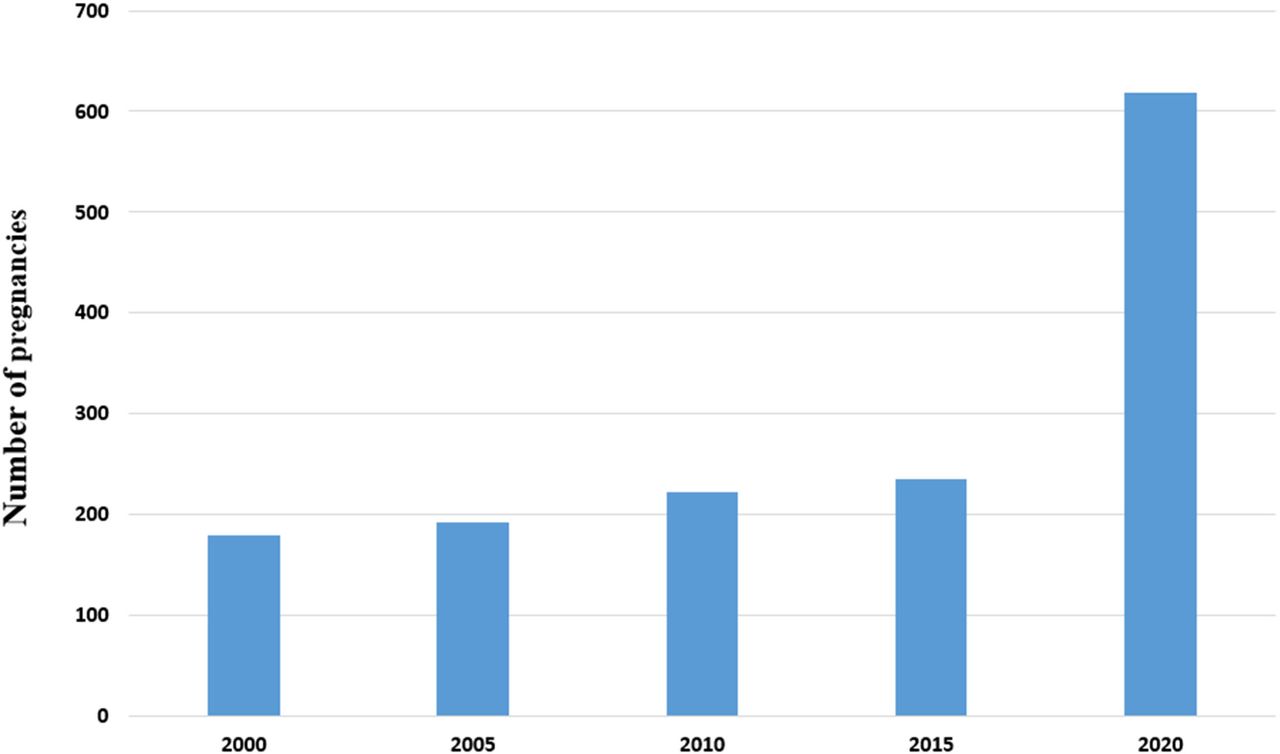
Pregnancies in people with cystic fibrosis (CF) have dramatically increased over the last 20 years. Based on historical increases in morbidity and mortality during pregnancy, particularly for people with severely impaired lung function, pregnancy was discouraged. With improvements in therapy and long-term prognosis, pregnancy rates reported in the US CF Foundation Patient Registry for people with CF aged 14–45 increased substantially, particularly in 2020 following the approval of elexacaftor–tezacaftor–ivacaftor in 2019.1
While a number of single-centre, and some multicentre cohort studies were conducted to evaluate the health of pregnant pwCF, the data were collected retrospectively and often contradictory.2–8 Furthermore, no large cohort studies have been conducted in the modern era of CF care.9 10 Investigators used large national and state databases to demonstrate that pregnant pwCF experience increased morbidity and mortality compared with people without CF: they are more likely to undergo Caesarean section (C-section), have preterm/low-birth weight infants and deliver infants with congenital anomalies.11–13 In addition, pwCF with pregestational diabetes, a common complication, also have higher rates of C-section.6 Previous reports further suggest that the first year post delivery is a time of extreme shift in hormones and stress, and can be associated with loss in body mass index (BMI) and per cent predicted forced expiratory volume in 1 s (ppFEV1) below prepregnancy baseline.5–7 Using data from the UK CF Registry in a cohort of pwCF pregnant between 2016 and 2018, we recently confirmed a decline in ppFEV1 and BMI, and an increase in pulmonary exacerbations in the year following pregnancy.14 Importantly, neither our study nor other cohort studies have reported infant outcome data beyond birth.9 10 Many pwCF, therefore, are concerned about the consequences of pregnancy on their health and that of their infants.15 16 Despite the increased relevance of this topic, to date there have been no multicentre prospective trials in CF aimed at helping identify the potential associations of prepregnancy health and choices made during pregnancy with maternal and fetal outcomes.
The population of pwCF experiencing pregnancy is growing at least in part due to the availability of better chronic medications, including the oral systemic medications that affect the basic CF defect, CF transmembrane conductance regulator (CFTR) modulators such as ivacaftor, lumacaftor/ivacaftor, tezacaftor/ivacaftor and elexacaftor/tezacaftor/ivacaftor (ETI). However, pregnant people were excluded from phase III trials of these medications.17–22 In the USA, preclinical, clinical and postmarketing experiences drive pregnancy classifications for drugs; ivacaftor, lumacaftor/ivacaftor and tezacaftor/ivacaftor have category B ratings.23–25 Using the post-2015 Federal Drug Administration (FDA) system of categorising risk of drug use in pregnancy, although animal reproductive studies of the individual components of ETI did not show teratogenic effects, there is inadequate information in humans.26 27 There have been case reports and case series describing successful pregnancies in people using CFTR modulator therapy but there are no prospective studies of the effects of CFTR modulators on pregnancy.28–33 Because there are clear reports of destabilisation occurring in pregnant pwCF on withdrawal from modulators,28 29 clinicians and pwCF are in urgent need of more data on the maternal–fetal impact of CFTR modulator use or discontinuation during pregnancy and/or lactation.
The Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) study is the first prospective, multicentre study in CF to assess the impact of pregnancy and that of CF medications on the health of pwCF. The primary aim is to assess whether lung function changes during pregnancy differ based on the use of modulators or other factors such as pre-existing comorbid conditions.
Methods and analysis
Study sites and coordination
The MAYFLOWERS trial is sponsored by the CF Foundation (CFF) and is currently enrolling across 40 participating centres in the CF Therapeutics Development Network (TDN). The CF TDN is comprised of 91 research centres in the USA dedicated to the safe and efficient conduct of clinical research in CF with the coordinating centre in Seattle, Washington.34
Study-design overview
MAYFLOWERS is a prospective, multicentre, observational clinical trial that follows pregnant pwCF and their infants who are and who are not exposed to CFTR modulators. PwCF≥16 years of age with confirmed diagnosis of CF (including pregnant pwCF who have undergone lung transplantation are included; complete inclusion and exclusion criteria are described in box 1). Participants will be followed over the course of pregnancy and for 2 years post delivery (figure 2A). With participant consent, the infants of participants will also be enrolled at birth and followed for 2 years.
Inclusion and exclusion criteria
Main study
Consent
Written informed consent (and assent when applicable) obtained from participant or participant’s legal guardian.
Enrolled in the Cystic Fibrosis Foundation Patient Registry.
Willing and able to adhere to the study visit schedule and other protocol requirements, as judged by the investigator.
Demographics
Must be ≥16 years of age at enrolment visit.
Health history
Documentation of CF diagnosis.
Currently pregnant (ie, either positive in-home pregnancy test with an absence of negative confirmatory pregnancy test or positive in-clinic pregnancy test).
Planning to continue with pregnancy.
Additional eligibility criteria for PK substudy
Written informed consent for PK substudy.
Must be at age of majority* at enrolment visit.
Must be currently prescribed ETI.
Able and willing to perform the testing and procedures required for this study, as judged by the investigator.
Additional eligibility criteria for CGM substudy
Written informed consent/assent for CGM substudy.
Must be ≤12 weeks pregnant at the enrolment visit.
Willing to self-insert the Dexcom G6 or G6 Pro CGM sensor at up to five different times and wear the sensor for up to 10 days each time.
Willing to remove CGM sensor and return by mail within 1 week of CGM completion (if the device is not used for clinical care) OR willing to share CGM data with researchers through Dexcom Clarity via uploading data using Dexcom Clarity app on a smartphone (if the device is already being used for clinical care).
Willing to withhold doses of acetaminophen greater than 1 g every 6 hours (4 g/day) while wearing the Dexcom G6.
Able and willing to perform the testing and procedures required for this substudy, as judged by the investigator.
Does NOT currently require treatment and is not expected to require treatment with hydroxyurea while wearing the Dexcom G6.
Does NOT have a history of lung transplantation.
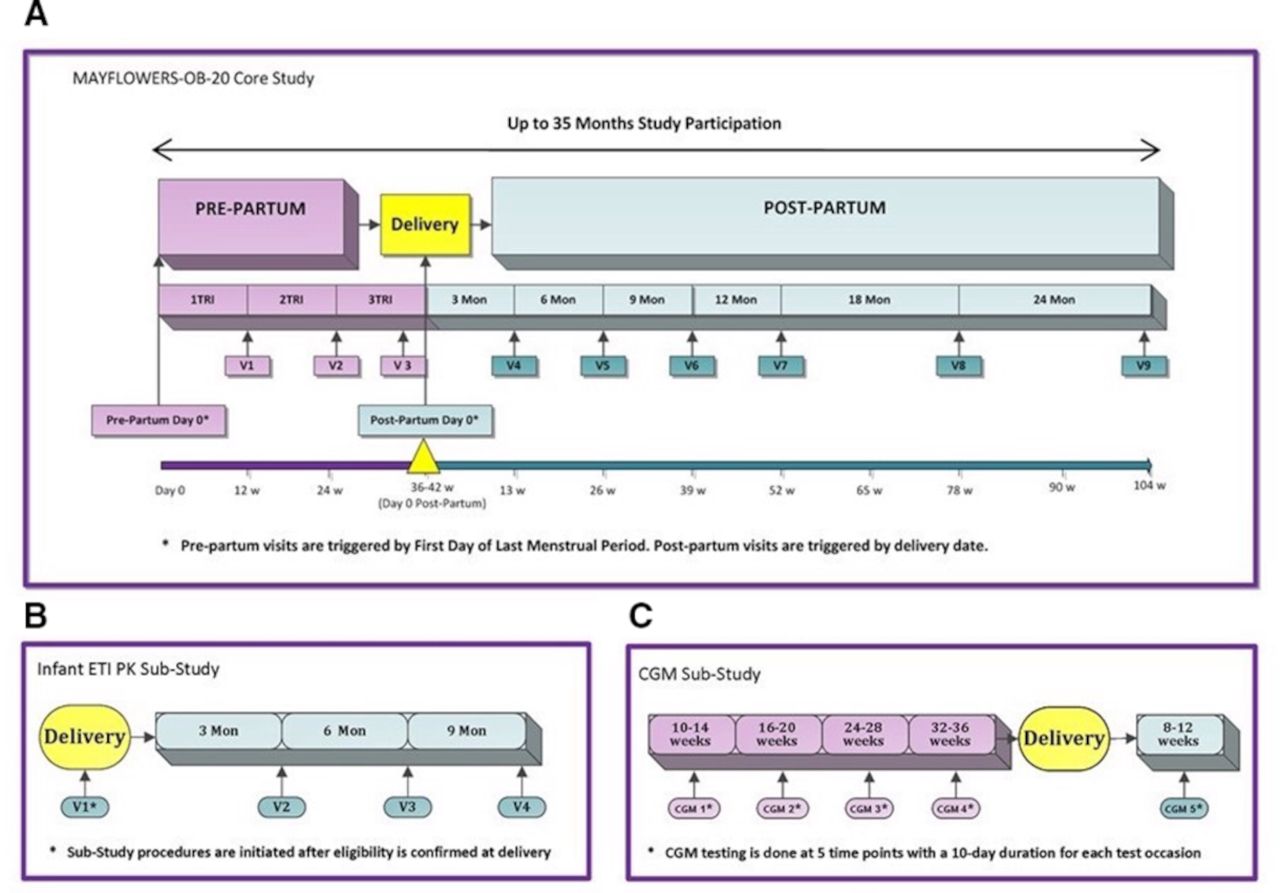
Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) study design: (A) planned study visits for core study, (B) planned study visits for the 20 mother–infant dyads that consent for the elexacaftor–tezacaftor–ivacaftor (ETI) pharmacokinetic (PK) substudy, (C) planned study visits for the 105 participants who consent to participation in the continuous glucose monitoring (CGM). v: visit; Tri, trimester; w: week.
Approximately 285 participants will be enrolled in the trial. People will be enrolled in the first trimester of pregnancy if possible and assessed every 3 months during pregnancy and during the first year after delivery, then every 6 months for an additional year. The duration of participation for each participant is expected to be approximately 35 months (figure 2A).
At the enrolment visit, spirometry and weight measurements will be obtained in clinic followed by a remote visit (coached telehealth visit or a phone call) during which baseline home spirometry and weight measurements will be repeated. Over the course of the study, CF clinical data, patient-reported outcomes, questionnaires including mental health questionnaires, obstetrical outcomes, infant growth and development outcomes, and comorbidities will be collected. All concomitant medication and concurrent therapies will be documented throughout the study with changes in CFTR modulator usage through pregnancy and lactation specifically captured. Blood collection for banking will be offered to all participants.
In addition, a select number of sites will enrol eligible participants in two substudies (figure 2B,C). One of these substudies is focused on understanding glucose metabolism during pregnancy using continuous glucose monitoring (CGM) and the other is aimed at understanding the pharmacokinetics (PK) of ETI in pregnancy, at birth and during lactation in mother and infant.
Patient and public involvement statement
The study was designed with feedback and review by pwCF. PwCF were formally surveyed regarding the relative importance of proposed study endpoints through CFF Community Voice,35 and a mother with CF (acknowledgements) participated in initial protocol design and subsequent protocol review. In order to minimise subject stress and inconvenience, the study allows remote data collection in lieu of in-person visits as needed. Further, the trial is structured around routine obstetrical and CF clinical care visits including the option of telehealth or phone visits if in-person CF clinical visits are not convenient or feasible. The trial is being conducted according to International Conference of Harmonisation E6: Good Clinical Practice Consolidated Guidance to protect subject safety and data integrity.
Objectives and endpoints
We hypothesise that pregnancy and lactation in pwCF cause short-term adverse health consequences that are compounded by complications of CF and may improve or stabilise with maternal use of CFTR modulators during pregnancy and lactation. Our primary hypothesis is that ppFEV1 subsequent to pregnancy (3 months) will decrease relative to ppFEV1 prior to pregnancy (1 year) and this decrease will be more pronounced among women who discontinue use of modulators. We will additionally account for other factors that may influence changes in ppFEV1, including duration of prepregnancy modulator use, baseline ppFEV1, genotype, history of exacerbations and pre-existing comorbid conditions (box 2).
MAYFLOWERS study endpoints
Primary endpoint
Change in ppFEV1 after delivery relative to measures assessed prior to pregnancy.
Secondary endpoints
Change in ppFEV1 per cent predicted from prepregnancy until 1 and 2 years after delivery.
Change in maternal weight and maternal BMI from prepregnancy until last measured prior to delivery (maximum weight gain).
Proportion of participants who have an insufficient weight gain during pregnancy as currently defined by the Institute of Medicine.62
Proportion of participants who have insufficient recovery of weight loss associated with lactation.
Incidence of CF exacerbations over the course of pregnancy, as number of exacerbations requiring intravenous antibiotics over person-years pregnant.
Incidence of gestational diabetes.
Incidence of gestational hypertension/pre-eclampsia.
Proportion of participants having interventional deliveries, that is, C-sections.
Change in CFQ-R (total and domains), PHQ-8 and GAD-7 scores.
Exploratory endpoints
Change in concentration of CFTR modulators in maternal plasma during pregnancy and post pregnancy.
Proportions of participants with diagnosis of CFRD, abnormal glucose tolerance and normal glucose tolerance based on historical OGTT.
Proportion of participants who develop gestational diabetes during pregnancy overall and based on historical OGTT.
Maternal and obstetrical outcomes among those with a diagnosis of CFRD or abnormal glucose tolerance from historical OGTT, or gestational diabetes during the study.
Infant outcomes at birth (gestational age, birth weight, congenital anomalies) among those with a diagnosis of CFRD or abnormal glucose tolerance from historical OGTT, or gestational diabetes during the study.
Management of gestational diabetes, that is, proportions of participants with gestational diabetes on dietary measures alone, oral medications, or insulin, as well as maternal and obstetrical outcomes by treatment type.
Infant PK substudy endpoints
Concentration of ETI in cord blood.
Concentration of ETI at delivery, 3, 6 and 9 months post partum in maternal blood.
Concentration of ETI at delivery, 3, 6, and 9 months post partum in infant blood.
Concentration of ETI at 3, 6, and 9 months post partum in breast milk.
CGM substudy endpoints
CGM measures of interest at each time point (10–14 weeks, 16–20 weeks, 24–28 weeks, 32–36 weeks, and 8–12 weeks’ post partum):
Time in the following ranges: <54 mg/dL, <63 mg/dL, 63–140 mg/dL, >140 mg/dL and >180 mg/dL.
Number of severe hypoglycaemic episodes <54 mg/dL.
Average glucose, SD and coefficient of variation.
Mean amplitude of glycaemic excursions (MAGE), calculated as the mean of the differences between consecutive glucose peaks and nadirs of major glucose fluctuations.63 64
The secondary objectives of this study (box 2) are to assess (1) whether any changes that occur in ppFEV1 over the course of pregnancy are recovered at one and 2 years post pregnancy (figure 2A); (2) whether there is any association of duration of modulator therapies prior to and during pregnancy with other maternal health and obstetrical outcomes including pregnancy-related complications; (3) whether there is any association between CF symptom scores and measures of mental health as measured by the Cystic Fibrosis Questionnaire-Revised, Patient Health Questionnaire Depression Scale and Generalised Anxiety Disorder Scale; (4) whether maternal health and obstetrical outcomes are additionally associated with baseline ppFEV1 or with prepregnancy BMI; and (5) whether prenatal care is associated with changes in ppFEV1. Finally, exploratory objectives will aid in describing the PK of CFTR modulators during and post pregnancy in mothers and infants with CF as well as characterise blood glucose excursions in pwCF during and post pregnancy (figure 2B, C).
Statistical plan
Demographic and baseline variables will be described for participants including CFTR modulator use (figure 3), genotype, race/ethnicity, age at pregnancy, height, weight, spirometry and other comorbidities (including lung transplantation). Additionally, neonatal data will be summarised for infants.
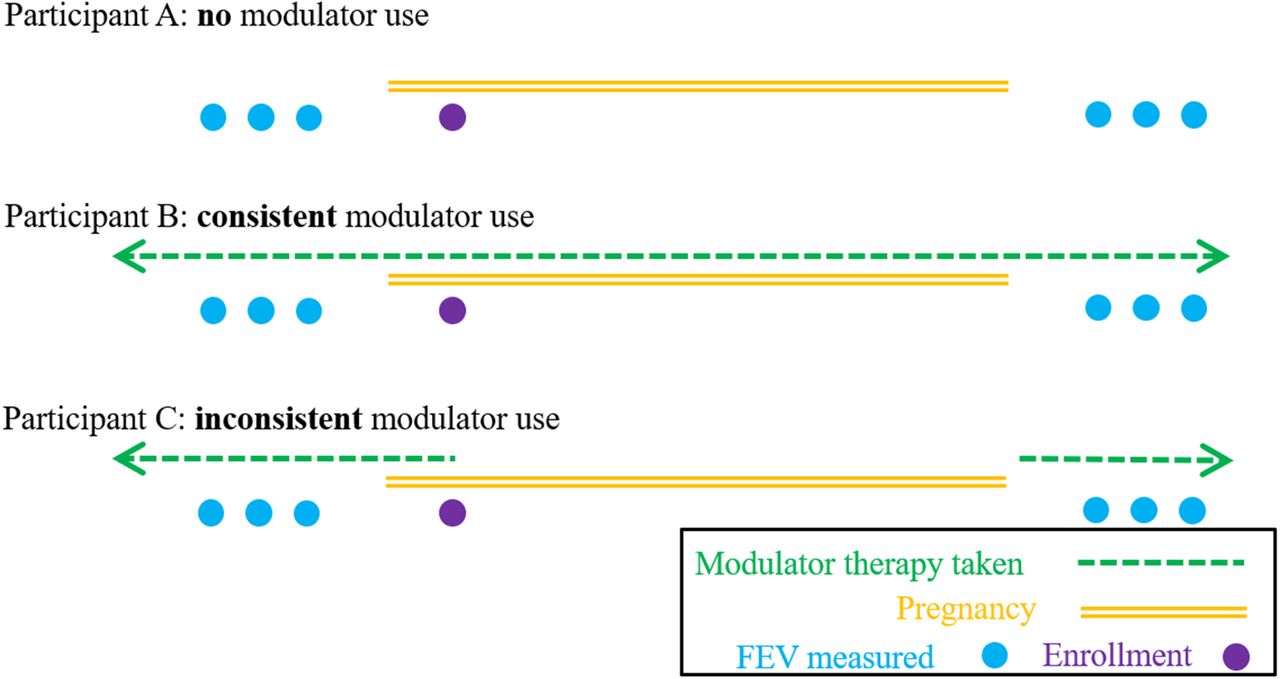
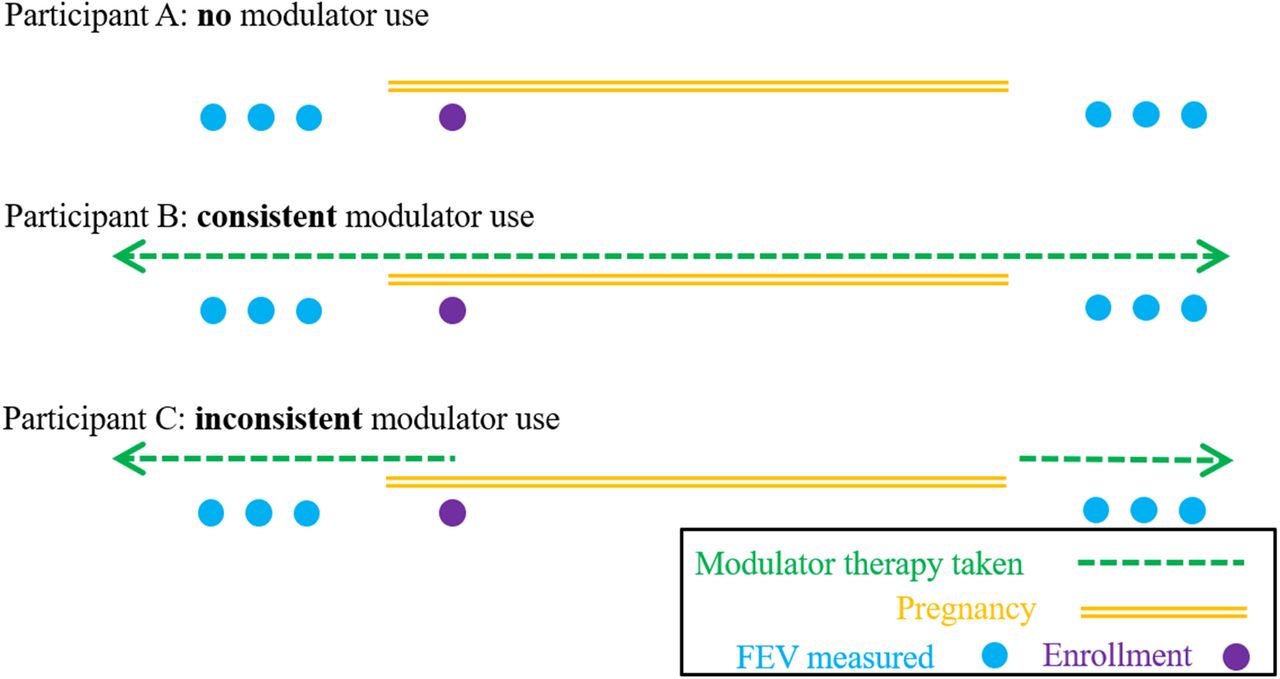
Study Groups. The study will enrol participants regardless of their use of cystic fibrosis transmembrane conductance regulator (CFTR) modulators. Based on a survey of potentially participating sites, approximately 25% of women are likely to discontinue CFTR modulators during pregnancy due to the unknown/understudied risks of CFTR modulators to the fetus. Statistical analysis will take into account those who have never been on CFTR modulator (eg, participant A), those who choose to stay on CFTR modulators throughout their pregnancy (eg, participant B), and participants who are using CFTR modulators during conception, but elect to discontinue CFTR modulators when pregnancy is diagnosed (eg, participant C). Other patterns of inconsistent use may be seen. FEV, forced expiratory volume.
Assessment of whether there are modifiable or non-modifiable factors associated with maternal health over the course of pregnancy will be performed. The primary outcome is change in ppFEV1 from 1 year prepregnancy until post pregnancy (post pregnancy ppFEV1 measurements will take place >2 weeks after resumption of modulator use, if applicable, at 3 months). For the primary analyses, changes in ppFEV1 from prepregnancy until post pregnancy will be summarised and tested via paired t-test and longitudinal mixed-effect model, adjusted for cumulative CFTR modulator usage and potential confounding variables. A sensitivity analysis will be conducted that excludes participants who have undergone lung transplantation. Potential confounding measures may include age, baseline ppFEV1, baseline BMI, sputum microbiology and the presence of common CF comorbidities. Changes in ppFEV1 relative to CFTR modulator usage will be assessed initially using ‘any discontinuation’ versus ‘continuous use’ and secondarily, based on cumulative months off modulators (figure 3). Finally, if relevant, should the timing of modulator interruption vary over trimesters, an additional adjustment for cumulative time off modulators in each of the trimesters will be performed.
Sensitivity analyses will assess the tradeoff between measures taken proximal to post delivery with the stability afforded by having multiple ppFEV1 measurements. The influence of missingness (eg, whether our findings change when persons with <3 prepregnancy or postpregnancy measures are excluded from analyses) will be explored in conjunction with the assumption of missing at random (eg, whether any potential measures of maternal health are associated with the availability of ppFEV1 measures). Short-term as well as long-term changes in ppFEV1 will be assessed out to 2 years post delivery (figure 2A).
Second, comparisons will occur between any associations of baseline ppFEV1 and CFTR modulator use during pregnancy with other maternal outcomes (symptoms, weight and BMI changes over pregnancy) as well as with any observed pregnancy complications and delivery complications. In exploratory analyses, other potential associations between baseline measures and secondary outcomes will be assessed. Because all associations will be observational, linear and logistic regressions will be used to adjust for potential confounding measures.
Sample size
Our primary hypothesis is that ppFEV1 following pregnancy (3 months) will decrease relative to ppFEV1 prior to pregnancy (1 year), and this decrease will be more pronounced among women who discontinue use of modulators. Based on informal survey of potential mothers and providers, decreases in ppFEV1 up to 5% were deemed a potentially acceptable trade-off for maternity. From previously published studies, change in ppFEV1 over the course of a pregnancy has an SD of 7%–12%.4 5 With 244 persons, we have at least 80% power to identify an overall average change prepregnancy versus post pregnancy in ppFEV1 of at least 1.3% to 2.2%, assuming an SD in change of 7% to 12%, respectively (table 1). The study size 244 provides adequate power to detect a 5% difference in change in ppFEV1 by potential risk factors, whether the difference is between a 0% ppFEV1 decline in one group versus 5% in another, or equivalently between a 3% increase versus a 2% decline (table 1). Anticipating 10% of the total study population will be modulator-ineligible and 5% loss to follow-up, 285 participants will be enrolled. While CFTR modulator use is the key predictor of interest, the study is powered to detect differences in change in ppFEV1 by other baseline characteristics specified in the primary aim (ppFEV1<70, presence of CF-related diabetes (CFRD), historical annual pulmonary exacerbation rate), which is present in >25% of participants (table 1).
Sample size needed to achieve 80% power, in order to detect a difference in ppFEV1 decline during pregnancy comparing groups determined by practices, conditions or treatments
Trial status
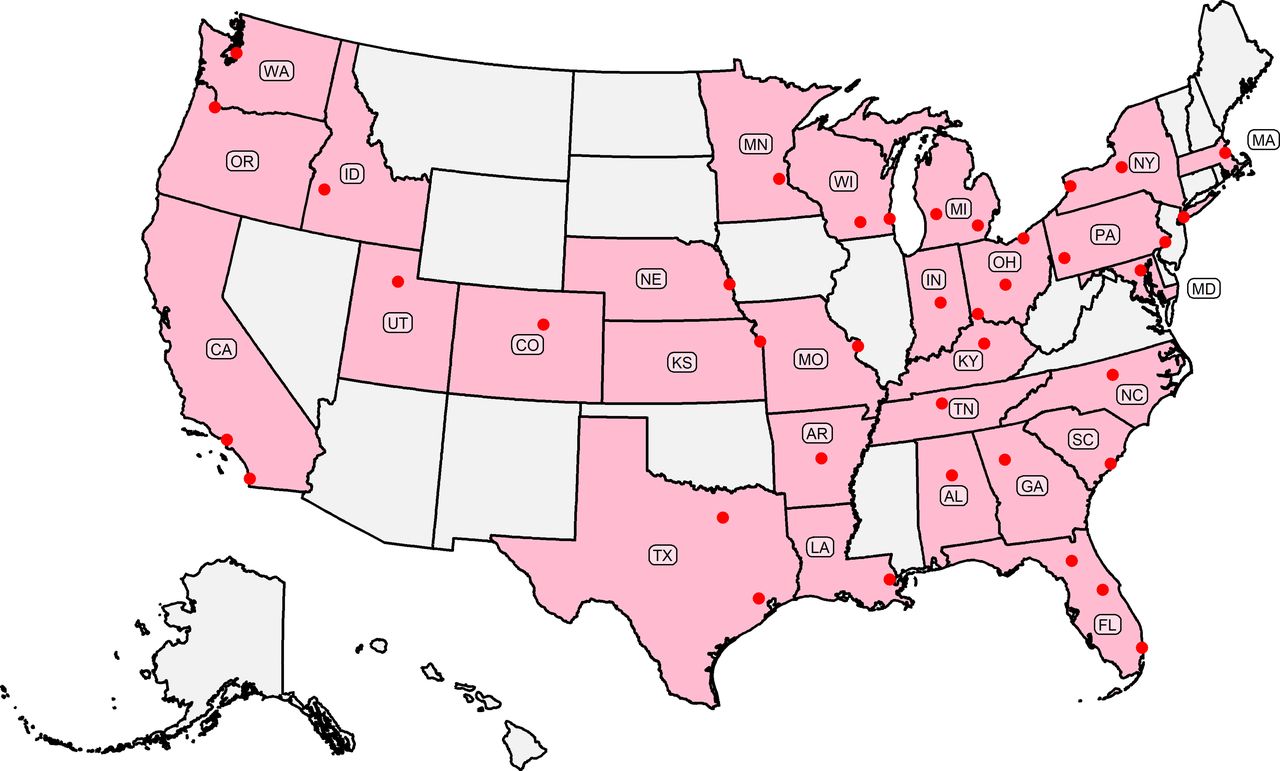
The trial protocol was IRB approved on 10 June 2021. The first patient was enrolled on 30 September 2021. As of May 2022, approximately 20% of participants have been enrolled from sites across the USA (figure 4). Our goal date for the last visit for the last participant is 30 December 2025.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trial enrolment sites. The Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS) study is sponsored by the Cystic Fibrosis Foundation and is currently enrolling across 40 participating centres in the CF Therapeutics Development Network.
Exploratory substudies
Pharmacokinetics
Emerging evidence suggests that PK/pharmacodynamics (PD) inter-relationships are variable and that this information is completely unknown in pregnant women, who are generally excluded from interventional trials.17–22 Physiologic changes in pregnancy may induce profound alterations to the PK properties of many medications, including effects on distribution, absorption, metabolism and excretion of drugs. Thus, the PD properties of some therapeutics may be altered during pregnancy.36 37 This impact is likely particularly true for drug combination therapy, such as ETI, which is susceptible to differences in blood and cellular metabolism and drug–drug interactions. If the timing of recent drug administration is known, blood sampling can be used to assess population PK over the course of pregnancy and compare it to published PK in non-pregnant individuals.
A key unknown factor with the use of ETI is the amount that may be transmitted from mother to infant in utero and after delivery through breast feeding. Animal reproductive models showed that elexacaftor crosses into the placenta and into breast milk.27 In one woman with CF and her infant, both lumacaftor and ivacaftor crossed the placenta, with lumacaftor concentrations greater in cord blood than in maternal plasma concentrations; both drugs were present in breast milk and infant plasma.38 Similarly, investigators recently reported that in three women who used ETI during pregnancy and lactation, all three components of ETI were present in cord and infant blood as well as breast milk.33 Interestingly, despite continuous dosing of ETI in the women, the perinatal concentrations were lower than those post pregnancy. Also, tezacaftor concentrations were higher in breast milk and in breastfeeding infants than those of elexacaftor and ivacaftor. To further understand the PK of ETI in pregnant women and their exposed infants, data collection and analysis in a larger group of mother–infant pairs are needed.
Finally, there is little information to guide recommendations for monitoring infants exposed to modulators during lactation. Animal data showed that ivacaftor administration to juvenile rats led to cataracts (leading to a recommendation for ophthalmologic exams in those under the age of 18 years receiving ivacaftor).23 Additionally, although fluctuations of liver function tests (LFTs) in young children are understudied, there are reports of elevated LFTs in young children treated with ivacaftor.39 Although the limited data from case series provide some reassurance,28 29 33 it is unclear if all infants exposed in utero or during lactation require ophthalmologic examination and routine LFT monitoring.
The MAYFLOWERS study will provide an opportunity to assess the changes in CFTR modulator PK during pregnancy and modulator concentrations in both mothers and infants peripartum over time. We will enrol 20 mother and infant pairs in the infant ETI PK substudy to determine the amount of each component of ETI present in cord blood, breast milk and infant plasma (figure 2B). This assessment may allow us to better characterise the potential risk of adverse effects for the infant.
Continuous glucose monitoring
Gestational diabetes is the most common medical disorder in pregnancy. It is associated with increased short and long-term health risks for both the mother (gestational hypertension and diabetes, and subsequently, hypertension and type II diabetes) and the infant (congenital anomalies, especially cardiac and neurologic, large for gestational age infants who may experience birth injury and hypoglycaemia, and subsequent risk for childhood obesity and its metabolic consequences).40 41 A substantial amount of data demonstrates a direct correlation between glycaemic control in pregnancy and poor infant outcomes42–46 and that improved glucose control decreases incidence of adverse outcomes.43 45 47–50
More than 30% of adults with CF were reported to have CFRD in the 2020 US Cystic Fibrosis Foundation Patient Registry (CFFPR).1 Reynaud et al reported that compared with pregnant women without CFRD, pregnant pwCF with CFRD had a trend towards need for assisted conception (p=0.06) and a higher need for delivery by C-section (p=0.005).6 Furthermore, Jelin et al reported that compared with women without CF, pwCF were more likely to have pregestational diabetes, require C-section and give birth to premature infants and infants with congenital anomalies.11
For both CFRD and gestational diabetes, the standard of care diagnostic test is an Oral Glucose Tolerance Test (OGTT).51–53 Nonetheless, clinicians and investigators are increasingly interested in exploring the use of CGM, which provides comprehensive glycaemic data using minimally invasive subcutaneous sensors. CGM has been validated in children and adolescents with CF.54 Two small studies showed that early glucose abnormalities are detectable by CGM in pwCF and are associated with historical decline and contemporaneously worse health outcomes.55 56 Finally, in a pilot study of adults with CF, Taylor-Cousar et al demonstrated that CGM identified a greater degree of impaired glucose metabolism than the gold standard 2-hour OGTT.57 Although there are no published studies investigating CGM in pregnant pwCF, a recent prospective multicentre study in pregnant women with type I diabetes showed that use of CGM significantly improved maternal glycaemic control, was associated with fewer adverse neonatal outcomes and minimised diabetes care burden on the expectant mothers.58
In the main study, we hypothesise that the level of abnormal glucose metabolism by prepregnancy OGTT will be associated with the adverse maternal and fetal outcomes known to occur in participants with (1) diabetes or (2) gestational diabetes. In the CGM substudy, we will enrol 105 participants in the first trimester of pregnancy to assess (1) any potential longitudinal changes in glycaemic control, (2) whether there is an association between OGTT and CGM results and (3) whether glucose and glycaemic variability on CGM provide additional information beyond what can be obtained from OGTT (figure 2C).
Ethics and dissemination
Despite the decline in pregnancies in the general US population, pregnancies in pwCF nearly doubled from 310 in 2019 to 619 in 2020.13 Data from the CFFPR from 1985 to 1997 showed that pwCF who became pregnant had similar long-term outcomes compared with people who never became pregnant; however, those who became pregnant were healthier at baseline than pwCF who did not become pregnant.4 14 Currently, more people with moderate to severe disease are becoming pregnant; use of modulator therapy has enabled even people with very severe lung dysfunction to conceive and maintain pregnancies.29 59 Nonetheless, little information is available regarding the long-term impacts of pregnancy in those with a wide range of baseline disease on lung function, exacerbations, nutrition, glucose control and mental health, and even less data have been described for infant outcomes. While the CFFPR is a key source of epidemiologic information regarding CF, neither key maternal factors such as data regarding circumstances surrounding pregnancy, detailed medication use and glucose control, nor important infant outcomes such as gestational age, birth injury, congenital malformations and early child development are available in the CFFPR.1 MAYFLOWERS will provide the comprehensive and timely data that pwCF and their care providers need to optimally prepare and manage CF in pregnancy and lactation.
The MAYFLOWERS trial will enable us to describe detailed health outcomes following pregnancy in pwCF and their infants. Because all trial participants will be pregnant pwCF, we will not be able to compare outcomes related to pregnancy nor to contrast infant outcomes between pwCF and without CF. However, we plan to leverage the data generated from this study for future comparative analyses through the US CFFPR to address separate but important questions about how lung function in pregnancy compares to that in the absence of pregnancy. With ~244 potential live births, our focus will be to estimate rates of infant outcomes and not to formally test for differences in outcomes by baseline exposures or identify potential risk factors. To achieve adequate power to identify risk factors associated with infant outcomes, the study would require (1) 1900 births to detect a 5% absolute difference in proportion of infants born at <37 weeks’ gestational age, (2) 1270 births to detect differences in birth weight of 100 g and (3) over 10 000 births to detect 1% absolute differences in frequencies of birth defects (usually present in fewer than 3% of births). MAYFLOWERS will be the first to report frequencies of infant outcomes, which can serve to motivate future studies of neonatal health among mothers-to-be with CF. Furthermore, the MAYFLOWERS PK substudy will aid paediatricians in their recommendations regarding safety monitoring and breast feeding when caring for healthy infants exposed to modulators.
Although MAYFLOWERS is enroling only pwCF, many of the results will likely be applicable to other people with chronic respiratory disease, particularly those with concomitant diabetes. In a review of a nation-wide database that included 1.3 million childbirths over 25 years, Jøvling et al reported an increasing prevalence of maternal chronic disease during pregnancy.60 Of the 23 chronic disease categories they examined, chronic lung disease was the most common. Given the potential adverse impact of chronic lung disease and diabetes on both maternal and infant health, the prospectively collected data in MAYFLOWERS on medication use, glucose control, changes in lung function post pregnancy and during lactation, and correlation of outcomes with baseline disease as well as impact on infant outcomes may inform management for other pregnant people with chronic lung disease and/or pregestational and gestational diabetes.
This pivotal study will provide an early examination of potential risk factors for successful or poor maternal outcomes in pregnant pwCF in the modern era, with a particular focus on the role of CFTR modulators for which approximately 90% of pwCF are now eligible.21 22 61 The data derived from this first of its kind study in CF will provide crucial information to guide pregnancy and lactation management by CF care providers and pwCF, as well as others with chronic respiratory disease.
Data availability statement
No data are available. NA.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Advarra IRB, SSU00159104. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We sincerely express our appreciation to the members of CFF Community Voice whose contributions aided in primary outcome choice. We would also like to thank Megan Lapore, Dr. Katie Rustici, and Dr. Edith Chang for protocol review, and the CFF TDN coordinating center staff for their operational assistance.
References
Footnotes
Contributors All authors drafted the manuscript or revised it critically for important intellectual content. All authors contributed to the design of the MAYFLOWERS study. All authors approved the final version of the manuscript. The content of this manuscript is the responsibility of the authors alone and does not necessarily reflect the views or policies of the study sponsor.
Funding Supported by the Cystic Fibrosis Foundation (CFF) (funding for the MAYFLOWERS study).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests JLT-C: received grants from Vertex Pharmaceuticals Incorporated and Eloxx; has received fees from Vertex Pharmaceuticals Incorporated related to consultation on clinical research design, participation on advisory boards, and speaking engagements; and has served on advisory boards and/or provided consultation for Novartis, Genentech, Gilead, Protalix, Santhera, 4DMT, AbbVie and Proteostasis. NMH has received grant funding from the CFF and NIH and has participated on an advisory board for Vertex. CRE has received grant funding from the CFF and NIH. MSP has received research grants from the CFF, NIH, and Vertex Pharmaceuticals; in-kind support from Dexcom Inc; and speaking fees from Vertex Pharmaceuticals. RJ has received grants from the CFF, Vertex, Boehringer_Ingelheim, Genentech, and Armata and received fees for consulting or serving on advisory boards from Gilead, Vertex and Boehringer Ingelheim.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.