Article Text

Abstract
Background To date, none of randomised trials aim to compare the efficacy of programmed death 1 (PD-1) inhibitor plus chemotherapy and bevacizumab plus chemotherapy as first-line treatment for non-squamous non-small-cell lung cancer (NSCLC). This analysis pooled prospective data to compare the survival benefits of the two regimens for advanced NSCLC without targetable genetic mutations.
Methods Data were pooled from three randomised phase III clinical trials: NCT03607539, NCT03134872 and NCT02954172. 466 patients received PD-1 inhibitor (200 mg) plus pemetrexed (500 mg/m²) and platinum (cisplatin 75 mg/m2 or carboplatin area under the curve (AUC) 5 mg/mL/min), while 432 patients received bevacizumab (15 mg/kg) plus paclitaxel (175 mg/m2) and carboplatin (AUC 6 mg/mL/min). Propensity score matching in a 1:1 ratio was performed to balance baseline characteristics of the two arms. The endpoints of this analysis were progression-free survival (PFS), overall survival (OS) and objective response rate (ORR).
Results In total, 375 patients in each arm were matched. With a median follow-up of 23 months (IQR 21–26), results showed that median PFS was significantly prolonged in the PD-1 inhibitor arm than in the bevacizumab arm (10.1 vs 7.4 months; HR 0.62, 95% CI 0.52 to 0.73, p<0.001). Improved OS was also demonstrated in the PD-1 inhibitor arm (27.9 vs 20.2 months; HR 0.75 95% CI 0.61 to 0.91, p=0.004). ORR in the PD-1 inhibitor arm was 56.8%, while that in the bevacizumab arm was 45.1%. However, exploratory subgroup analysis indicated that median PFS and median OS of the two arms were comparable in patients with negative programmed death ligand 1 expression or in patients aged ≥65 years old.
Conclusions PD-1 inhibitor plus chemotherapy was associated with significant survival benefits compared with bevacizumab plus chemotherapy in patients with advanced non-squamous NSCLC, which provides evidence support to guide clinical practice. Nonetheless, the comparative survival outcomes in several subgroups indicated that bevacizumab plus chemotherapy still mattered.
- lung cancer
- non-small cell lung cancer
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The current guidelines prioritising programmed death 1 (PD-1)/programmed death ligand 1 inhibitor plus chemotherapy over bevacizumab plus chemotherapy are mainly based on indirect extrapolation of the results of several previous clinical trials; there is a paucity of literature directly comparing the regimens.
WHAT THIS STUDY ADDS
This pooled analysis is, to our knowledge, the first study of prospectively obtained data to compare the survival outcomes of PD-1 inhibitor plus chemotherapy and bevacizumab plus chemotherapy for first-line treatment of advanced non-squamous non-small-cell lung cancer (NSCLC) without epidermal growth factor receptor (EGFR) or Anaplastic Lymphoma kinase (ALK) alteration, which could provide evidence reference to guide treatment option in clinical practice.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results provided evidence support for the preference of PD-1 inhibitor plus chemotherapy in first-line treatment for non-squamous NSCLC, while the comparative survival outcomes in several subgroups indicated that bevacizumab plus chemotherapy still mattered.
Introduction
Bevacizumab plus chemotherapy and programmed death 1 (PD-1)/programmed death ligand 1 (PD-L1) inhibitor plus chemotherapy have been approved successively for the first-line treatment of non-squamous non-small-cell lung cancer (NSCLC) without sensitising EGFR or ALK alteration. Both regimens have demonstrated substantially improved progression-free survival (PFS) and overall survival (OS) compared with chemotherapy alone.1–5 Nonetheless, a comparison of survival benefits between the two regimens has not been clearly explored. The rationale that current guidelines preferentially recommend PD-1/PD-L1 inhibitor plus chemotherapy for first-line treatment of advanced non-squamous NSCLC is mainly based on an extrapolation of the results of previous clinical trials, which lacks sufficient power to guide clinical practice to some extent.1 3–6
The IMpower150 trial conducted a prospective, head-to-head comparison of PD-L1 inhibitor atezolizumab plus chemotherapy and bevacizumab plus chemotherapy for the treatment of patients with advanced non-squamous NSCLC.7 Unexpectedly, no statistically significant difference in PFS and OS was observed in light of the published results. In addition, Asian populations tend to respond better to bevacizumab plus chemotherapy than non-Asian populations. The survival benefits of bevacizumab plus chemotherapy in the BEYOND trial and east Asian subgroup analysis in the AVAiL and SAiL trials were superior to those in the global ECOG 4599 trial with a predominantly white population included, and even comparable to survival benefits of pembrolizumab plus chemotherapy in the KEYNOTE 189 trial.1–3 8 9 Collectively, exploration is warranted to confirm whether current guidelines are appropriate in prioritising recommendations of PD-1/PD-L1 inhibitor plus chemotherapy in the first-line treatment for non-squamous NSCLC, especially in Asian populations. Moreover, the further exploration in some key subgroups is of great significance to achieve optimal treatment.
Herein, the present study seeks to compare the survival benefits of PD-1 inhibitor plus chemotherapy versus bevacizumab plus chemotherapy in the first-line treatment of Chinese patients with non-squamous NSCLC without EGFR or ALK alteration by a pooled analysis of three prospective trials.10–12
Methods
Study design and patients
Data were pooled from three randomised phase III trials done at a number of medical centres in China.10–12 Briefly, the CameL study was an open-label, multicentre (52 sites), phase III trial with medication of carboplatin and pemetrexed with or without PD-1 inhibitor camrelizumab.11 The ORIENT 11 study was a double-blind, multicentre (47 sites), phase III trial with medication of pemetrexed and platinum with or without PD-1 inhibitor sintilimab.10 Moreover, the remaining bevacizumab study was a double-blind, multicentre (42 sites), positive drug-controlled, phase III trial exploring the clinical equivalence of bevacizumab biosimilar IBI305 to the reference bevacizumab.12 Patients with advanced metastatic non-squamous NSCLC were eligible if they were aged 18–75 years and had a baseline Eastern Cooperative Oncology Group Performance Status of 0 or 1. Patients with sensitising EGFR mutations, ALK translocations or unknown status were excluded. Nearly all patients enrolled from the CameL and ORIENT 11 studies had the PD-L1 expression assessed. Other detailed design and eligibility criteria have been previously reported elsewhere.10–12
Treatment interventions
In the PD-1 inhibitor arm, 200 mg camrelizumab or sintilimab was administered intravenously on day 1 of every 3-week (Q3W) treatment cycle. In the CameL study, camrelizumab was combined with carboplatin (area under the curve (AUC), 5 mg/mL/min, day 1 Q3W) and pemetrexed (500 mg/m², day 1 Q3W) for four to six cycles, while in the ORIENT 11 study, sintilimab was in combination with pemetrexed (500 mg/m2, day 1 Q3W) and either cisplatin (75 mg/m2, day 1 Q3W) or carboplatin (AUC 5 mg/mL/min, day 1 Q3W) for four cycles. Each regimen was then followed by corresponding PD-1 inhibitor camrelizumab or sintilimab plus pemetrexed as maintenance therapy Q3W until disease progression, intolerable toxicity, death, withdrawal of consent, investigator decision, loss of follow-up or study completion for up to 24 months. Notably, patients with radiographic progression but were in clinically stable condition could continue the treatment based on the investigator’s discretion until progression was corroborated at a subsequent assessment 4 weeks later.
In the bevacizumab arm, patients administered bevacizumab biosimilars IBI305 (15 mg/kg Q3W) or reference bevacizumab (15 mg/kg Q3W), in combination with carboplatin (AUC 6 mg/mL/min, Q3W) and paclitaxel (175 mg/m2, Q3W) no more than six cycles. Patients then administered corresponding IBI305 or reference bevacizumab as maintenance therapy until disease progression, intolerable toxicity, death, withdrawal of consent, investigator decision, loss of follow-up or study completion.
Outcomes
In this pooled analysis, the prespecified endpoints included PFS, OS and objective response rate (ORR). PFS was defined as the time from randomisation to disease progression or death from any cause; OS was defined as the time from randomisation to death from any cause; ORR was defined as the proportion of patients with a confirmed complete or partial response. Independent radiographic review committee has conducted efficacy assessment based on Response Evaluation Criteria in Solid Tumours V.1.1 in all of the three studies. The efficacy assessment intervals and follow-up plans were basically similar among the three studies. Tumour imaging assessments were done every 6 weeks for the first 48 weeks and every 12 weeks thereafter in the ORIENT 11 study and bevacizumab study, while tumour imaging was conducted every 6 weeks for the first 54 weeks and every 12 weeks thereafter in the CameL study.
The exploratory subgroup analysis was performed based on prespecified covariates including age (<65 or ≥65 years old), gender (male or female), disease stage (Ⅲ or Ⅳ), smoking history (<20 or ≥20 pack years), ECOG PS (0 or 1) and PD-L1 Tumour Proportion Score (TPS) (<1% or ≥1%). In the PD-1 inhibitor arm, the vast majority of patients underwent PD-L1 TPS evaluation by the PD-L1 immunohistochemistry 22C3 pharmDx test. Notably, none of the patients in the bevacizumab arm was tested for PD-L1 expression. Previous studies have shown that the therapeutic efficacy of bevacizumab was not affected by the expression status of PD-L1.13 Therefore, in the exploratory subgroup analysis with different PD-L1 TPS, the overall population in bevacizumab arm was compared with patients with different PD-L1 TPS in PD-1 inhibitor arm to identify the optimal regimen.
Statistical analysis
Data were pooled from the full analysis set populations in the three randomised trials and entered into two arms with PD-1 inhibitor plus chemotherapy versus bevacizumab plus chemotherapy. Owing to the pooling of three separate trial populations, Q statistics and I² values were used to assess the possible heterogeneity among the three trials. Propensity score matching was performed to adjust unbalanced covariates between the two regimens. The propensity score for each enrolled patient was calculated by a multivariable logistic regression model based on the covariates including age, gender, ECOG PS, clinical disease stage, histopathological features and smoking history. The matched subjects (1:1) were then generated by the nearest neighbour matching without replacement. A calliper of 0.2 was set to be the maximum tolerated deviation of the paired propensity score. Moreover, the absolute standardised difference no more than 0.1 between the two matched groups was deemed as a good match.
χ2 and t-tests were used to compare the categorical and continuous variables of baseline characteristics between the two groups, respectively. The Kaplan-Meier curves and log-rank test were adopted to estimate and compare PFS and OS between the two arms. Moreover, the exploratory subgroup analyses were performed by unstratified Cox proportional hazards models with estimated HRs and associated 95% CIs.
Statistical power calculations were presented in the original publications for each trial.10–12 A two-side p value less than 0.05 was deemed as statistically significant. All statistical analyses were done using SPSS V.23.
Patient and public involvement statement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
Study population
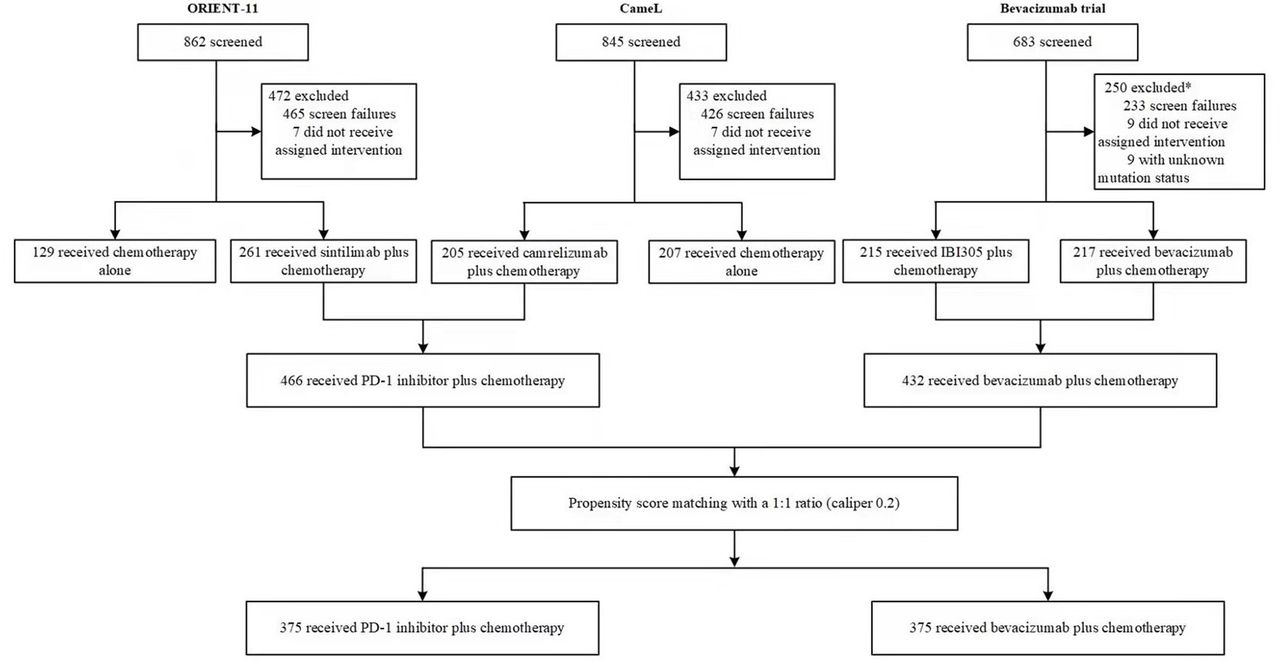
Among the three enrolled studies, patients were recruited from 28 November 2016 to 30 July 2019 (bevacizumab study, from 28 November 2016 to 23 May 2018; CameL study, from 12 May 2017 to 6 June 2018; ORIENT 11 study, from 23 August 2018 to 30 July 2019). Totally, 205 patients in the CameL study and 261 patients in the ORIENT 11 study were pooled into the PD-1 inhibitor arm (n=466). Given the clinical equivalences of bevacizumab biosimilar IBI305 to bevacizumab in efficacy, patients administering either IBI305 or bevacizumab in the enrolled study were all pooled into the bevacizumab arm for further analysis (n=432). Selection of patients from the three studies was shown in figure 1. After propensity score matching, eventually, survival outcomes were compared in 375 patients in the PD-1 inhibitor arm and the matched 375 patients in the bevacizumab arm. Baseline characteristics were generally well balanced between the two matched arms (table 1).

Patient enrolment flowchart. PD-1, programmed death 1.
Baseline characteristics before and after propensity score matching
Efficacy
In the entire population before matching, median follow-up was 23.4 months (IQR 21.6–25.3) in the PD-1 inhibitor arm and 22.2 months (IQR 19.8–27.6) in the bevacizumab arm with an overall median follow-up of 23.0 months (IQR 20.9–25.9). The median PFS was substantially prolonged in the PD-1 inhibitor arm (10.1 months, 95% CI 8.9 to 11.2) versus the bevacizumab arm (7.4 months, 95% CI 6.8 to 8.0) with an HR of 0.64 (95% CI 0.54 to 0.75, p<0.001). Improved OS in the PD-1 inhibitor arm was also observed (median OS 27.9 months (95% CI 25.0 to 30.7) vs 20.6 months (95% CI 17.7 to 23.5); HR 0.80, 95% CI 0.67 to 0.97; p=0.021). The ORR was significantly higher in the PD-1 inhibitor arm than in the bevacizumab arm (56.9% vs 45.1%, p<0.001).
Comparison between the two matched groups confirmed basically consistent results. Median follow-up was 23.4 months (IQR 21.6–25.3) in the PD-1 inhibitor arm and 22.5 months (IQR 20.2–27.6) in the bevacizumab arm with an overall median follow-up 23.0 months (IQR 21.0–26.0). The median PFS was 10.1 months (IQR 8.8–11.3) in the PD-1 inhibitor arm vs 7.4 months (IQR 6.8–8.0) in the bevacizumab arm (HR 0.62, 95% CI 0.52 to 0.73; p<0.001; figure 2A). Median OS was significantly extended in the PD-1 inhibitor arm as well (27.9 months (not reached) vs 20.2 months (IQR 17.5–22.9); HR 0.75, 95% CI 0.61 to 0.91; p=0.004; figure 2B). In the PD-1 inhibitor arm, 56.8% of patients achieved objective response as did 45.1% in the bevacizumab arm (p=0.001).

Kaplan-Meier analysis for progression-free survival (A) and overall survival (B) in the matched population. NR, not reached; PD-1, programmed death 1.
Exploratory subgroup analysis was conducted in the matched arms (figure 3A,B). Collectively, most baseline characteristic subgroups were observed to have improved PFS and OS in the PD-1 inhibitor arm compared with those in the bevacizumab arm. Nonetheless, there were several subgroups in which PD-1 inhibitor plus chemotherapy did not significantly prolong PFS and OS than bevacizumab plus chemotherapy. In the subgroup analysis of patients aged ≥65 years old, median PFS was 7.0 months (IQR 5.1–8.9) in the PD-1 inhibitor arm and 8.5 months (IQR 7.0–10.0) in the bevacizumab arm (HR 1.07, 95% CI 0.77 to 1.49; p=0.670; figure 4). Corresponding median OS was 15.6 months (IQR 12.0–19.1) vs 17.7 months (IQR 14.0–21.4), respectively. Of 103 patients, 47 (45.6%) achieved an objective response in the PD-1 inhibitor arm, as did 47 of 97 patients (48.5%) in the bevacizumab arm (p=0.689).

Exploratory subgroup analysis in progression-free survival (A) and overall survival (B) in the matched population. ECOG-PS, Eastern Cooperative Oncology Group Performance Status; NR, not reached; PD-1, programmed death 1; TPS, Tumour Proportion Score.

Kaplan-Meier analysis for progression-free survival (A) and overall survival (B) in the subgroup of patients aged ≥65 years old. PD-1, programmed death 1.
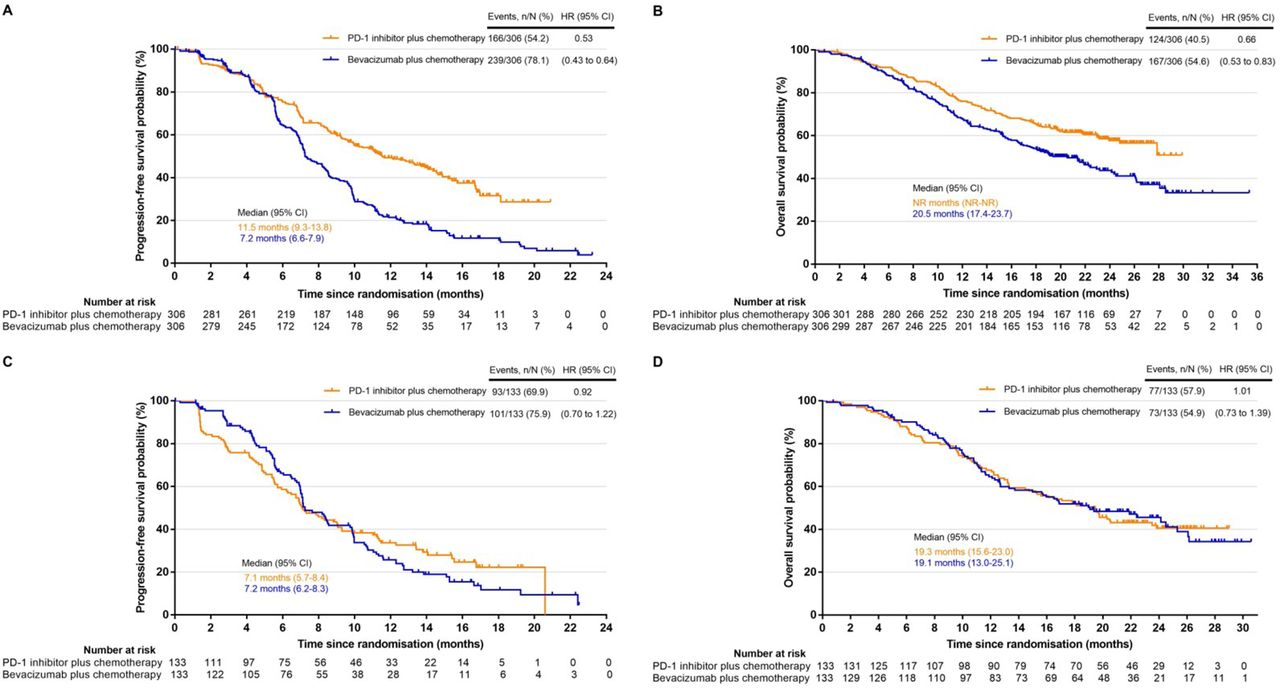
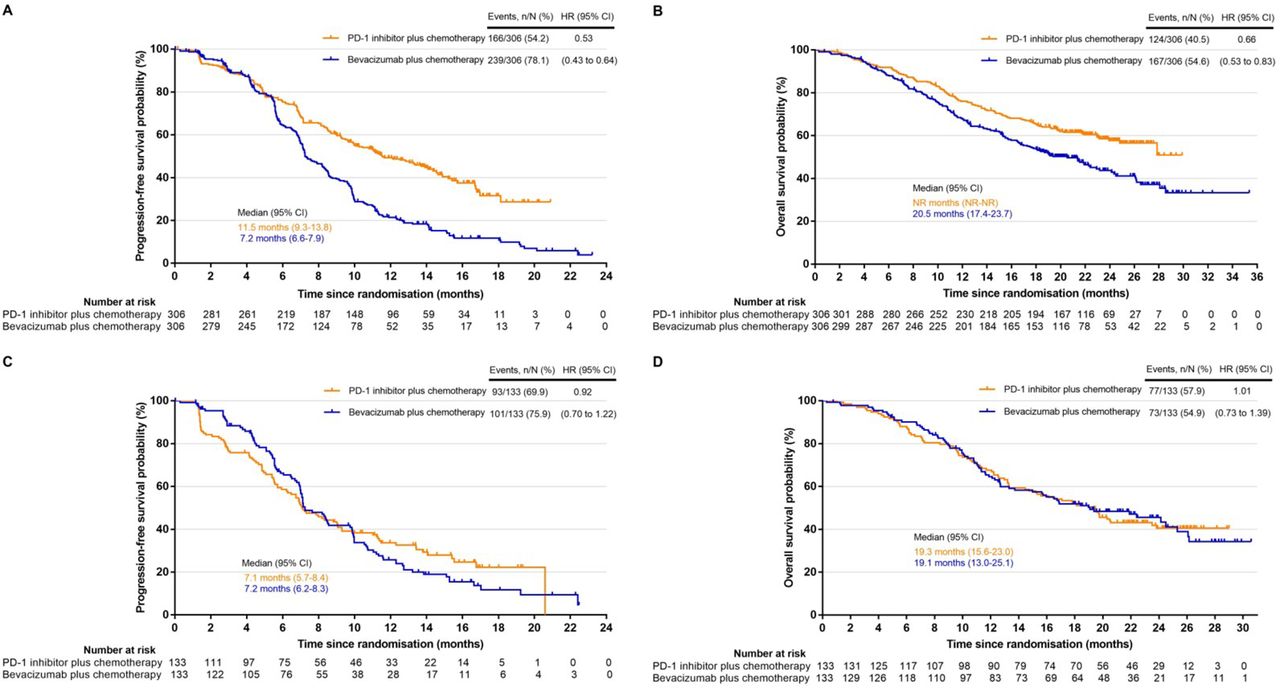
Survival outcomes were also analysed in the subgroup of patients with different PD-L1 expression. In patients with positive PD-L1 expression (TPS ≥1%), 306 patients in the PD-1 inhibitor arm were matched to 306 patients in the bevacizumab arm using propensity scores. Matched covariates were well balanced with standardised differences between the two arms generally less than 0.1 (online supplemental table S1). Median PFS was 11.5 months (IQR 9.3–13.8) in the PD-1 inhibitor arm and 7.2 months (IQR 6.6–7.9) in the bevacizumab arm (HR 0.53, 95% CI 0.43 to 0.64; p<0.001; figure 5A). Improved OS in the PD-1 inhibitor arm was also demonstrated (median OS, not reached (NR) (NR–NR) vs 20.5 (17.4–23.7); HR 0.66, 95% CI 0.53 to 0.83; p<0.001; figure 5B). Of 306 patients, 193 (63.1%) achieved objective response in PD-1 inhibitor arm while 137 of 306 patients (44.8%) in bevacizumab arm (p<0.001).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier analysis for PFS (A) and OS (B) in the subgroup of patients with PD-L1 ≥1% and PFS (C) and OS (D) in the subgroup of patients with PD-L1 <1%. PD-1, programmed death 1; NR, not reached; OS, overall survival; PD-L1, programmed death ligand 1; PFS, progression-free survival.
In patients with negative PD-L1 expression (TPS <1%), survival outcomes were compared in 133 patients in the PD-1 inhibitor arm and the matched 133 patients in the bevacizumab arm. Online supplemental table S2 showed the balanced baseline characteristics with standardised differences between the two arms generally less than 0.1. No significant improvement in PFS, OS and ORR was observed with PD-1 inhibitor treatment versus bevacizumab treatment. Median PFS was 7.1 months (IQR 5.7–8.4) in the PD-1 inhibitor arm and 7.2 months (IQR 6.2–8.3) in the bevacizumab arm (HR 0.92, 95% CI 0.70 to 1.22; p=0.579; figure 5C). The corresponding median OS was 19.3 months (IQR 15.6–23.0) vs 19.1 months (IQR 13.0–25.1), respectively (HR 1.01, 95% CI 0.73 to 1.39; p=0.956; figure 5D). The ORR was 42.9% in both the two arms.
Safety
In the entire population, the incidence of treatment-related adverse events (AEs) of grade 3 or higher was 65.5% in the PD-1 inhibitor arm and 88.9% in the bevacizumab arm. Eight (1.7%) of 466 patients with PD-1 inhibitor treatment developed grade 5 treatment-related AE, while none of the patients with bevacizumab treatment developed grade 5 treatment-related AE. The most common grade 3 or higher treatment-related AEs were decreased neutrophil count, decreased white blood cell count and decreased platelet count in both arms. Grade 3 or higher immune-related AEs occurred in 58 of 466 patients (12.4%) in the PD-1 inhibitor arm, while grade 3 or higher bevacizumab-related AEs were reported in 74 of 432 patients (17.1%) in the bevacizumab arm. Other details were reported in the original publications for each trial.10–12
Discussion
To our knowledge, this pooled analysis is the first study of prospectively obtained data to compare the survival outcomes of PD-1 inhibitor plus chemotherapy and bevacizumab plus chemotherapy for first-line treatment of advanced non-squamous NSCLC without EGFR or ALK alteration. The results demonstrated that PD-1 inhibitor plus chemotherapy was associated with substantially prolonged PFS and OS compared with bevacizumab plus chemotherapy, which provided evidence support for the preference of PD-1 inhibitor plus chemotherapy in the first-line treatment of advanced non-squamous NSCLC. Notably, no significant improvement in both PFS and OS was observed in the PD-1 inhibitor arm versus the bevacizumab arm in the subgroup of patients with negative PD-L1 expression and subgroup of patients aged ≥65 years old, which warrants further exploration to identify the optimal regimen.
The current guidelines prioritising PD-1/PD-L1 inhibitor plus chemotherapy over bevacizumab plus chemotherapy are mainly based on indirect extrapolation of the results of several previous clinical trials.1 3–6 To date, there is a scarcity of large, randomised, head-to-head clinical trials directly comparing PD-1 inhibitor plus chemotherapy versus bevacizumab plus chemotherapy. Of particular concern, bevacizumab plus chemotherapy has shown relatively more potent antitumor efficacy in Asian populations than non-Asian populations. Clinicians have been puzzled as to which of the two regimens is superior for the Asian population. Our study pooled prospectively obtained data from three randomised phase III clinical trials of Chinese population with non-squamous NSCLC without EGFR or ALK alteration and further made head-to-head comparison of PD-1 inhibitor plus chemotherapy and bevacizumab plus chemotherapy in efficacy and safety. The results substantiated significantly improved survival benefits of PD-1 inhibitor plus chemotherapy, which could provide evidence support for guidance and clinical practice to some extent.
The phase III IMpower150 trial explored the comparative efficacy of PD-L1 inhibitor atezolizumab plus chemotherapy versus bevacizumab plus chemotherapy for the first-line treatment of metastatic non-squamous NSCLC.7 Contrary to what was anticipated, there was no significant difference in PFS and OS between the two regimens in the intention-to-treat population. Result discrepancies between the IMpower150 trial and our analysis were possibly attributed to the differences in patient baseline characteristics and more remarkably, the type of immune checkpoint inhibitors (PD-L1 inhibitor vs PD-1 inhibitor). Specifically, a meta-analysis including 19 clinical trials of PD-1 and PD-L1 inhibitors for diverse cancer types demonstrated favourable survival outcomes with PD-1 inhibitors compared with PD-L1 inhibitors.14 The results of a pooled analysis of four randomised clinical trials including KEYNOTE-021 Cohort G, KEYNOTE-189, IMpower130 and IMpower150 also showed a substantially longer PFS and OS with PD-1 inhibitor pembrolizumab plus chemotherapy than with PD-L1 inhibitor atezolizumab plus chemotherapy.15 Nonetheless, further randomised trials are needed to corroborate the differences.
Survival benefits favoured PD-1 inhibitor plus chemotherapy against bevacizumab plus chemotherapy in the entire population and the majority of subgroups. However, there were several subgroups in which no significant difference in survival outcomes was found between the two regimens. Of particular concern, in the subgroup of patients aged ≥65 years old, bevacizumab plus chemotherapy induced longer PFS and OS than PD-1 inhibitor plus chemotherapy, though without statistical significance. Further analysis of our study observed that survival benefits with PD-1 inhibitor plus chemotherapy in elderly patients (≥65 years old) were limited in comparison with young patients. The efficacy of immunotherapy in elderly patients remains controversial and has been not completely explored. Several studies failed to demonstrate a significant survival benefit in elderly patients, while some studies showed a comparable efficacy and toxicity profile of immunotherapy between young patients and elderly patients.16–19 Immunosenescence during ageing may be associated with impaired immune response against tumour cells, which could affect the efficacy of immunotherapy in elderly patients to varying degrees.20 21 Elderly patients account for a considerable proportion of patients with lung cancer,22 and it is of great significance to identify the optimal regimen in this population. The subgroup analysis of elderly patients in this study was limited by small sample sizes and therefore should be interpreted with caution. Besides, for elderly patients especially with high PD-L1 expression, whether immunotherapy alone could achieve superior survival benefits remains unclear. Further randomised trials with large volumes are needed to guide clinical practice.
Notably, no significant improvement in OS and PFS was demonstrated in the PD-1 inhibitor arm versus the bevacizumab arm in the subgroup of patients with negative PD-L1 expression. Consistent results were previously reported in the IMpower150 trial.7 13 23 Survival outcomes were comparable with atezolizumab plus chemotherapy and bevacizumab plus chemotherapy in the negative PD-L1 expression subgroup (median OS 14.8 vs 14.1 months; HR 0.96, 95% CI 0.76 to 1.22). Of particular concern, the addition of atezolizumab to bevacizumab plus chemotherapy failed to attain significantly prolonged survival outcomes as well (median PFS 7.1 months vs 6.9 months, HR 0.77, 95% CI 0.61 to 0.99; median OS 16.9 months vs 14.1 months, HR 0.90, 95% CI 0.71 to 1.14).13 23 Additionally, a randomised phase III trial of nivolumab in combination with carboplatin, paclitaxel, and bevacizumab as first-line treatment for patients with advanced non-squamous NSCLC published the results of interim analysis.24 Promisingly, the results showed that nivolumab in combination with chemotherapy and bevacizumab was associated with substantially prolonged PFS compared with bevacizumab plus chemotherapy in patients with PD-L1 TPS of <1% (median PFS 13.6 months vs 8.4 months, HR 0.55, 95% CI 0.38 to 0.78). The OS analysis was immature with a slight trend favouring nivolumab combination. Longer follow-up is warranted to evaluate the OS benefits. Collectively, the optimal treatment regimen for patients with PD-L1 TPS of <1% remains unclear. Of note, moreover, bevacizumab plus chemotherapy remains an important regimen option in the first-line treatment for this subgroup.
This study has several limitations. First, the pooled data were retrospectively retrieved from three prospective trials. To minimise baseline characteristic differences between the two arms, propensity score matching was performed. Nonetheless, the analysis of this study was exploratory and lacked sufficient power to definitely confirm differences in survival outcomes between treatment regimens. Prospective, randomised, head-to-head clinical trials are warranted to make direct comparison of PD-1 inhibitor plus chemotherapy and bevacizumab plus chemotherapy to determine the optimal treatment regimen in the entire population and in some key subgroups. However, pretty large samples and long follow-up time make it a little difficult to initiate such clinical trials. In addition, more and more attention is paid to development of new anti-tumour drugs and regimens. Therefore, this pooled study, as the only study to date exploring comparative efficacy of PD-1 inhibitor plus chemotherapy and bevacizumab plus chemotherapy, could provide evidence reference for current guidelines and clinical practice to some extent. Second, although with updated data of survival outcomes, the follow-up in this analysis was still relatively short and few death events occurred during this period. Besides, the detail of second and later line treatments of some patients were incomplete. Therefore, the available data limit further exploration in the effect of cross-over treatment in the bevacizumab arm on OS results. Nevertheless, a significant difference in OS between the two arms in the entire population was demonstrated. Lastly, the analysis was limited to the Chinese population. Considering the potential impact of ethnic differences on survival outcomes, we found that further exploration in other population is needed.
In summary, our pooled analysis demonstrated that PD-1 inhibitor plus chemotherapy induced substantially increased survival benefits compared with bevacizumab plus chemotherapy for the first-line treatment of non-squamous NSCLC without sensitising EGFR or ALK alteration. The result supports a preferential consideration of PD-1 inhibitor plus chemotherapy for the first-line treatment of non-squamous NSCLC in clinical practice. Despite this, the optimal regimen for some key subgroups including those with negative PD-L1 expression and age of ≥65 years old needs to be further explored. The comparative survival outcomes suggested that bevacizumab plus chemotherapy still mattered in these subgroups at present. Large, head-to-head, randomised clinical trials are warranted to validate the exploratory outcomes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This pooled analysis involves human participants, and the study protocols of the three trials were approved by the independent ethics committees or institutional review boards of Shandong Cancer Hospital and Institute (reference ID SDTHEC202003011). All enrolled patients provided written informed consent before any study-related intervention. All of the three enrolled trials were registered with ClinicalTrials.gov and conducted according to the Declaration of Helsinki as well as Guidelines for Good Clinical Practice.
Acknowledgments
We thank all the enrolled patients and their families for supporting our work and are grateful to all the participating medical centres.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
XM and YC are joint first authors.
XM and YC contributed equally.
Contributors XM and YC performed the statistical analysis and drafted the manuscript, which was critically reviewed and revised by JY, CZ and LZ. LX, XL, KZ and LJ collected, analysed and interpreted the data. JY, CZ and LZ accepted full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors approved the manuscript for submission.
Funding JY received grants from the Academic Promotion Program of Shandong First Medical University (2019ZL002), Research Unit of Radiation Oncology, Chinese Academy of Medical Sciences (2019RU071), the National Natural Science Foundation of China (81627901, 81972863 and 82030082) and the Natural Science Foundation of Shandong (ZR201911040452). XM received grants from the National Natural Science Foundation of China (81972796) and the Natural Science Foundation of Shandong (ZR2019MH010 and ZR2020MH289).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.