Article Text

Abstract
Objective To estimate the incidence of ischaemic heart disease, atrial fibrillation and heart failure in community patients with or without chronic obstructive pulmonary disease (COPD).
Methods For this population-based study, we used primary care data of the Julius General Practitioners’ Network. Eligible participants were aged 40–80 years old and contributed data between January 2014 and February 2019. Participants were divided into groups according to COPD status and were followed up for new ischaemic heart disease, atrial fibrillation and/or heart failure. Age-specific and sex-specific incidence and incidence rate ratios were calculated for patients with and without COPD.
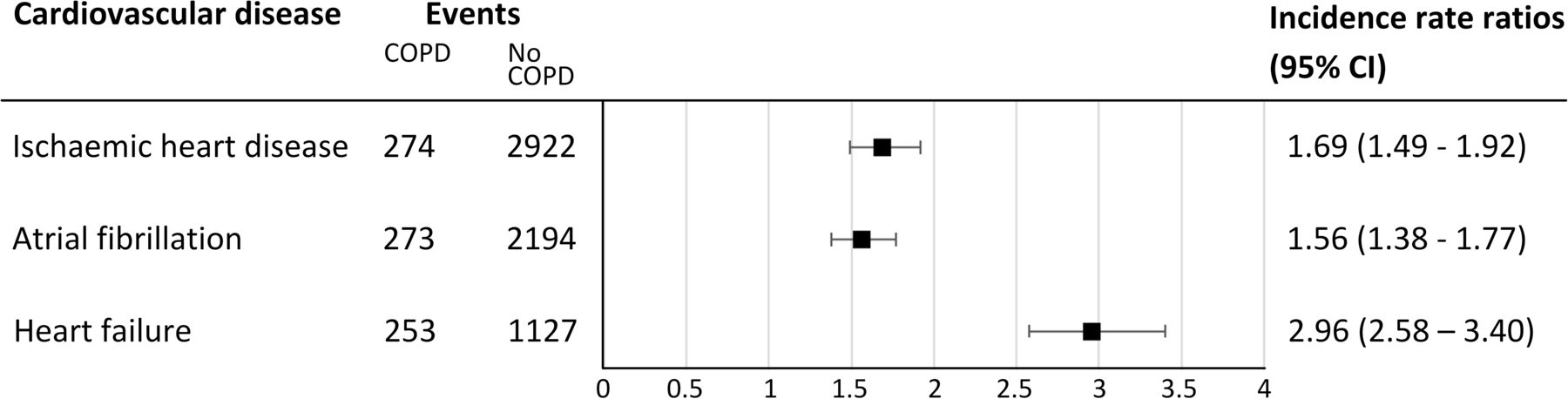
Results Mean follow-up was 3.9 years, 6223 patients were included in the COPD group, and 137 028 individuals in the background group without COPD. Incidence rates of all three heart diseases increased with age and were higher in males, independent of presence of COPD. Incidence rate ratios for patients with COPD, adjusted for age and sex, were 1.69 (95% CI 1.49 to 1.92) for ischaemic heart disease, 1.56 (95% CI 1.38 to 1.77) for atrial fibrillation and 2.96 (95% CI 2.58 to 3.40) for heart failure.
Conclusion The incidence of all major cardiovascular diseases is higher in patients with COPD, with the highest incidence rate ratio observed for heart failure.
- COPD epidemiology
- Clinical Epidemiology
Data availability statement
Data may be obtained from a third party and are not publicly available. Our data will be returned to the JGPN after publication, in line with JGPN terms and conditions and privacy regulations. The JGPN committee will evaluate requests for data sharing and will make data available under strict conditions.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Chronic obstructive pulmonary disease (COPD) is an important risk factors for the development of cardiovascular diseases (CVDs), notably ischaemic heart disease, atrial fibrillation and heart failure.
There is a paucity of longitudinal studies estimating the incidence of new-onset CVDs in this population. New estimates of CVD incidence are needed to inform on the burden of disease and the opportunities for prevention.
WHAT THIS STUDY ADDS
The incidence of all major CVDs is higher in patients with COPD, but the highest incidence rate ratio was observed for heart failure.
Analysis by age and sex provides insight in the patient groups that are most at risk. In young females, for example, COPD seems to negate some of the premenopausal protection for all three CVDs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study may urge physicians to proactively screen for CVDs in patients with COPD.
Introduction
Cardiovascular diseases (CVDs) rank among the most common comorbidities in patients with chronic obstructive pulmonary disease (COPD) and are associated with reduced longevity.1 According to a 2015 meta-analysis, patients with COPD have a twofold increased odds of having any CVD, compared with patients without COPD.2 Notably arrhythmias, ischaemic heart disease, heart failure and coronary, cerebrovascular and peripheral disease are common. In fact, patients with COPD are, on average, just as likely to die from a CVD as they are from a pulmonary cause.3
Accumulating evidence confirms that COPD and CVD are linked through more than a shared set of risk factors, although smoking remains an important cause for both. COPD can be described as the pulmonary component of ‘inflammageing’; a range of proinflammatory processes that lead to systemic endothelial inflammation and facilitate atherosclerosis and other CVDs.4 5
Despite a growing understanding of the importance of COPD as a risk factor for CVD, there is a relative paucity of longitudinal studies estimating the incidence of new-onset CVDs in this population.
Methods
Data source
For this population-based study, we used primary care data of the Julius General Practitioners’ Network. The JGPN is a registration network of nearly 70 general practices in the Netherlands, including over 370 000 enlisted individuals. General practitioners register diagnoses according to international classification of primary care (ICPC) coding, and drug prescriptions are entered in international anatomical therapeutic coding. The same cohort was used in a previous study estimating the incidence of CVDs in patients with and without diabetes, with methods similar to those described below.6 More detailed information on the JGPN is published elsewhere.7
Study cohort
Eligible participants were aged 40–80 years old and contributed data between January 2014 and February 2019. Participants entered the cohort at baseline or when they first enlisted at a participating practice. They were followed until they left the cohort due to death, movement out of the region, development of the outcome or until the end of the study.
COPD status was based on ICPC-coding (R95: Emphysema/COPD). In patients labelled with an ICPC-code for COPD who (1)did not receive a prescription for any type of inhalation medication used in patients with COPD during the last 12 months, and (2) did not participate in a primary care disease management programme for COPD, and (3) in whom spirometry data or COPD morbidity scores were never registered, the diagnosis COPD was considered too uncertain. These participants were excluded from the analyses. (see flow chart 1). Because the induction time for CVDs as a result of COPD is unclear, patients who developed COPD during follow-up contributed time at risk in the background group without COPD and were removed from the cohort at the time of first COPD diagnosis.
Study outcomes
Individuals with a newly developed target disease (ischaemic heart disease, atrial fibrillation and/or heart failure) were identified by ICPC-code (see table 1). Patients with a target disease at baseline, or who developed a target disease during follow-up, were censored for that particular disease from that moment onwards, but could still contribute person time for the other target diseases (see flow chart 1).
ICPC-codes used to identify outcomes
Data analysis
Baseline characteristics are presented as means (for normally distributed continuous data) or frequencies (for categorical data). Incidence of ischaemic heart disease, atrial fibrillation and heart failure was calculated as number of cases per 1000 person-years according to COPD status. Groups based on age (≤64, 65–74 and ≥75) were formed to estimate incidence by age. Additionally, age-adjusted and sex-adjusted Incidence rate ratios were calculated with Poisson regression analysis with person-time in years added as offset.
After exclusion of patients with any CVD at baseline, disease-free survival was calculated using Cox proportional hazard regression. Cumulative incidence curves were plotted for individuals with and without COPD at baseline, adjusting for sex and age. Ischaemic heart disease, atrial fibrillation and heart failure were applied as composite outcome. The competing risk of death was taken into account, using the SAS PROC PHREG procedure to fit the semiparametric proportional hazards model for the subdistribution of a competing risk analysis proposed by Fine and Gray. Because the hazard of CVD is expected to change more as a function of age than as a function of time on study, age was used as the timescale instead of follow-up duration. Individuals were entered into the analysis at their baseline age and exited at their censoring or event age. All analyses were conducted using IBM SPSS Statistics V.25 and SAS Studio V.3.8.
Results
Mean follow-up was 3.9 years, and 143 646 participants were included in the cohort. COPD diagnosis was considered too uncertain in 395 individuals with an ICPC code for COPD, but who did not receive a prescription for any inhalation medication during the year before or after diagnosis, and in whom COPD morbidity scores or spirometry reports were never registered. These individuals were removed from the cohort, which left 137 028 (95.6%) individuals without COPD and 6223 (4.4%) with COPD for analysis. Figure 1 shows the person-time and numbers of cases per subcohort 1. The baseline characteristics of the COPD group and the background group are presented in table 2.
The baseline descriptive statistics of the study population (aged 40–80 at start) enrolled in the Julius General Practitioners’ Network between 2014 and 2019
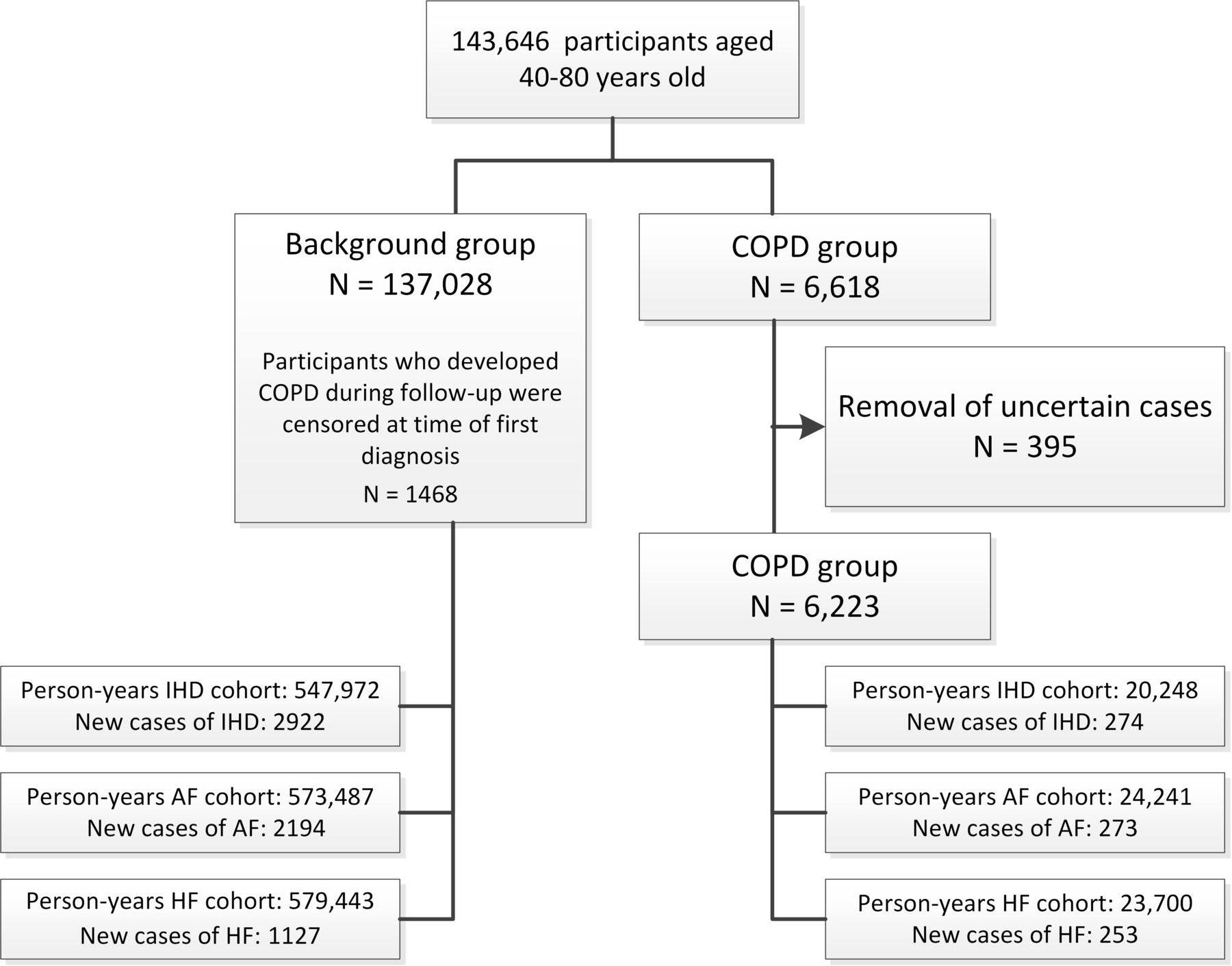
Composition of the cohort and subcohorts. AF, atrial fibrillation; COPD, chronic obstructive pulmonary disease; HF, heart failure; IHD, ischaemic heart disease.
Characteristics of the study population
Participants with COPD were usually older (64.1 years vs 55.3 years) and had more cardiovascular risk factors and comorbidities at baseline compared with participants without COPD. At baseline, patients with COPD more often had ischaemic heart disease (20.2% vs 5.6%), atrial fibrillation (6.7% vs 2.2%) and heart failure (7.7% vs 1.1%).
Incidence of ischaemic heart disease
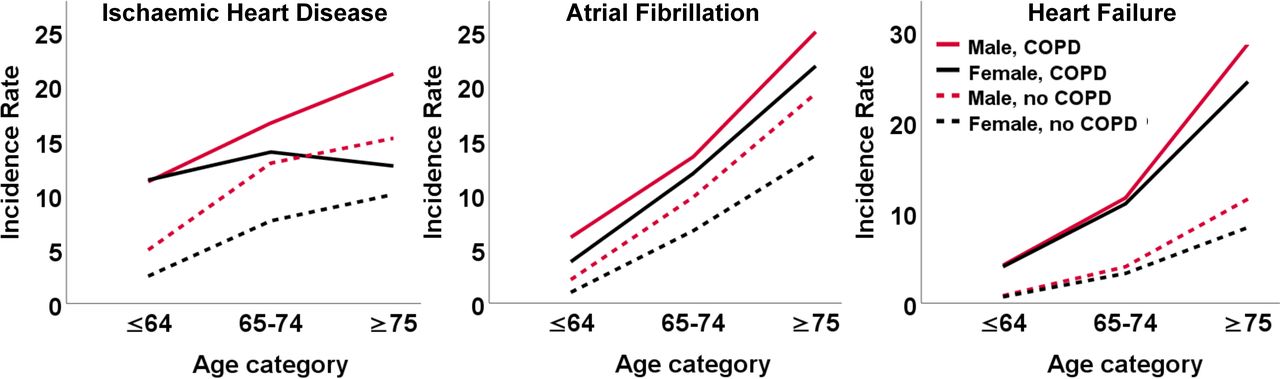
In general, patients with COPD had a higher risk of ischaemic heart disease compared with patients without COPD. The higher risk in patients with COPD was most pronounced in the younger age group (table 3 and figure 2). In individuals without COPD, the incidence of ischaemic heart disease was significantly higher in males than in females at any given age. In patients with COPD, there was no significant difference between the sexes. The incidence rate ratio for ischaemic heart disease in participants with COPD versus participants without COPD was particularly high in younger females(≤64 years old).
IR of ischaemic heart disease per 1000 person-years, for patients with and without COPD, per age category
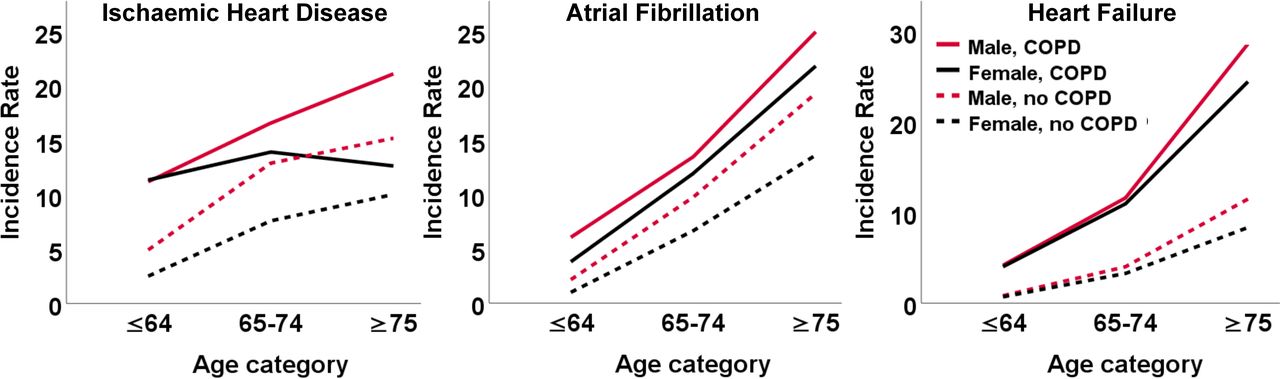
Incidence of cardiovascular diseases per 1000 person-years, for patients with and without COPD, per age category. COPD, chronic obstructive pulmonary disease.
Incidence of atrial fibrillation
In the total population, incidence of atrial fibrillation was higher in patients with COPD compared with those without COPD in all age categories, although the incident rate ratios converged somewhat in the elderly. In participants without COPD, incidence of atrial fibrillation was higher in males than in females at any given age. Although a similar trend was present in participants with COPD, the CIs overlapped, indicating that these differences were not statistically significant (table 4).
IR of atrial fibrillation per 1000 person-years, for patients with and without COPD, per age category
Incidence of heart failure
Across all age categories, the incidence of heart failure was significantly higher in individuals with COPD, for both males and females (table 5). Incidence of heart failure generally increased with age and reached its peak in the oldest age category. Incidence rates were fairly similar for males and females.
IR of heart failure per 1000 person-years, for patients with and without COPD, per age category
The overall incidence rate ratio for COPD versus no COPD was highest for heart failure (2.96), followed by ischaemic heart disease (1.69) and atrial fibrillation (1.56) (figure 3).

Age-adjusted and sex-adjusted incidence rate ratios of ischaemic heart disease, atrial fibrillation and heart failure for patients with and without COPD. COPD, chronic obstructive pulmonary disease.
Initial manifestations and cumulative incidence curves
In total, 5728 individuals without any CVD at baseline developed a first CVD during follow-up (529 patients with COPD and 5199 individuals without COPD). Of these, 527 developed more than 1 CVD (79 patients with COPD and 448 individuals without COPD). Ischaemic heart disease was the most common first presentation in patients with and without COPD (55.8% and 45.7%, respectively). Of the 529 patients with COPD who developed a CVD during follow-up, heart failure was the first presentation in 138 (26.1%) patients (compared with 12.5% in patients without COPD) (figure 4).
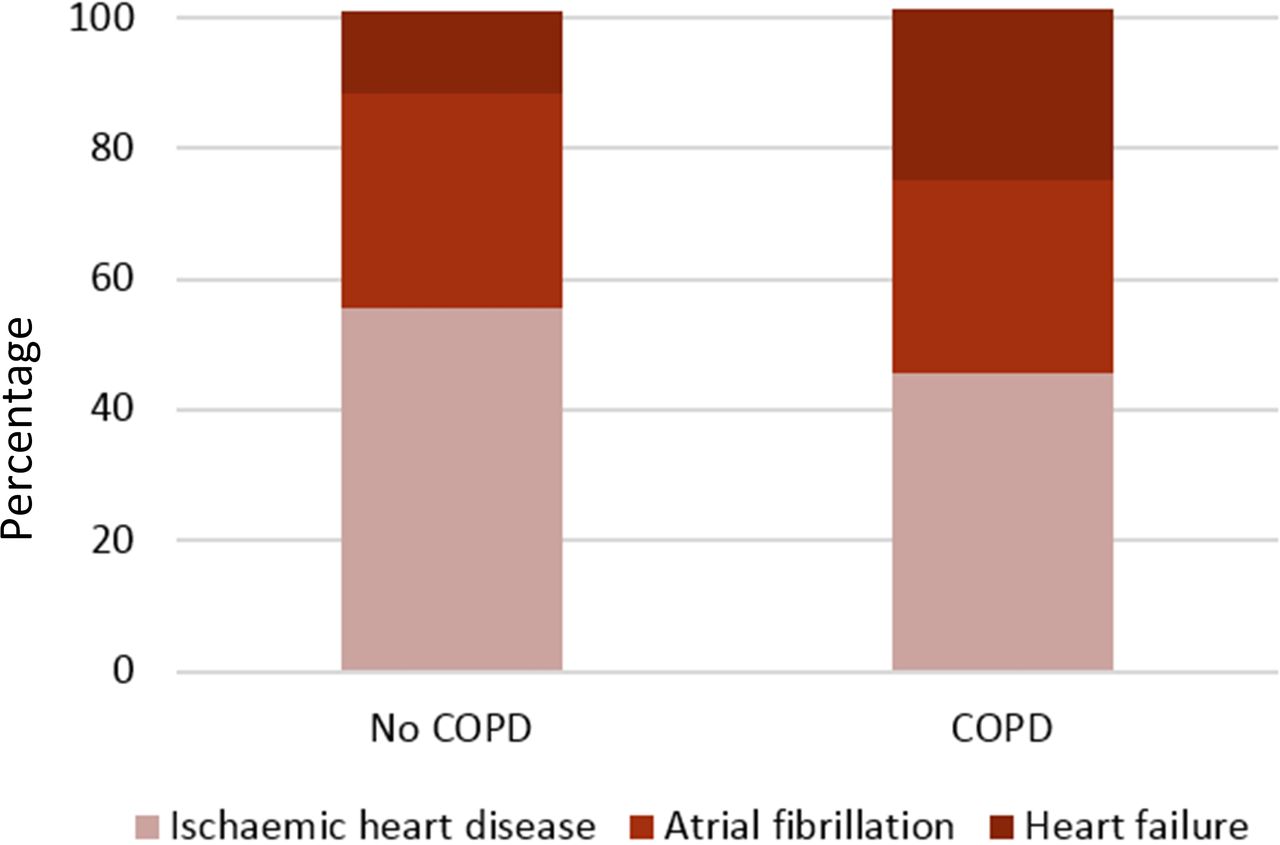
Distribution of the initial manifestation of cardiovascular disease in individuals with and without COPD. Total percentage exceeds 100% because some individuals were diagnosed with more than one cardiovascular disease at initial presentation (ie, atrial fibrillation and heart failure). COPD, chronic obstructive pulmonary disease.
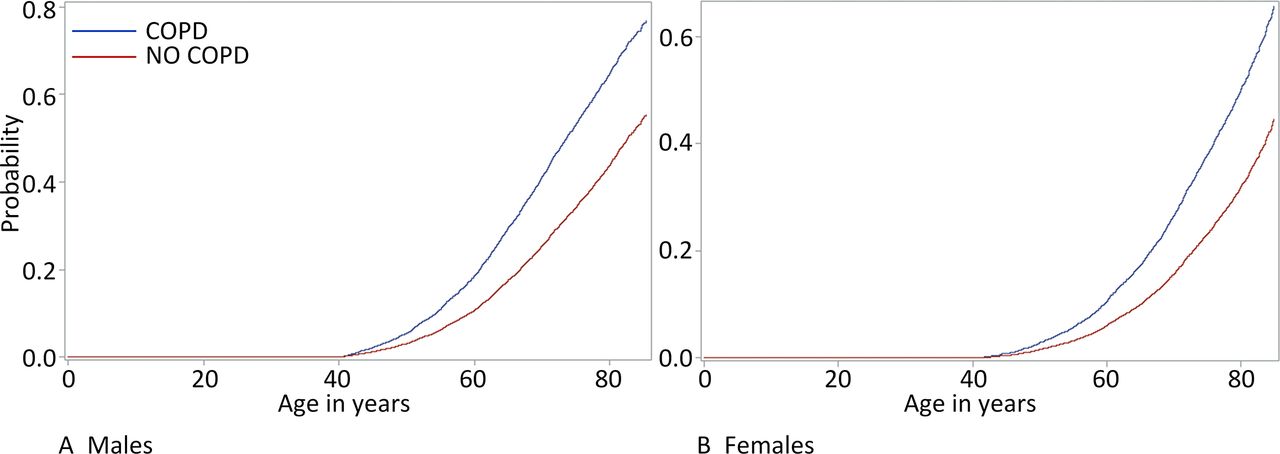
Figure 5A,B show the estimated cumulative proportion of patients with events up to 80 years, for patients with and without COPD at age 40.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of patients with at least one cardiovascular event up to 80 years, for males with and without COPD (A) and for females with and without COPD (B). COPD, chronic obstructive pulmonary disease.
Discussion
Our results, based on 137 028 community adults registered with a general practitioner without COPD and 6223 labelled with COPD followed-up for a mean of 3.9 years, show that the age-adjusted and sex-adjusted incidence of ischaemic heart disease, atrial fibrillation and heart failure is higher in individuals with COPD than those without.
Although the absolute incidence of ischaemic heart disease, atrial fibrillation and heart failure increased steadily with age, the rate ratios declined, with the highest ratios found in the youngest patients. This decline in rate ratios with age may in part be explained by the competitive risk of death, which is likely higher in patients with COPD,8–12 but also reaffirms that age remains the most important risk factor for all CVDs. For example, simulation studies showed that, in a hypothetical population of individuals with ideal risk factor profiles, heart failure incidence will only be about 25% less than in the real-world population, simply because age will eventually take its toll.13 Our data should prompt physicians to be vigilant for signs of early CVD in the younger age groups as well, since the potential gains of early recognition in terms of quality-adjusted-life years are highest in these patients. Moreover, acute events (eg, acute myocardial infarction, acute heart failure and ischaemic stroke) could be prevented or postponed.
The high incidence rate ratios in young patients suggests that COPD may not only increase the risk of CVD, but also accelerates its progression. The process of ‘accelerated ageing’ seen in COPD has been observed previously.14 Several mechanisms that play a role in the development of COPD can also be linked to the onset of CVD. These mechanisms include the degradation of elastin in lungs and arteries,15 and the loss of sirtuins; antiageing proteins that regulate processes such as transcription and apoptosis.16 A range of chronic proinflammatory processes that occur in patients with COPD, lead to systemic endothelial inflammation and facilitate atherosclerosis and other CVDs.4 5 17 Lastly, in a recent population-based study including 24.675 participants, the effect of traditional risk factors on the future development of heart failure was stronger in younger individuals (<55 years old). Known and modifiable risk factors explained 75% of the population attributable risk in young patients, but only 53% in older patients.18
As reported previously, incidence rates of ischaemic heart disease and atrial fibrillation were consistently higher in males than in females. For heart failure, incidence for males also tended to be higher, although the difference between the sexes was less pronounced. Interestingly, all sex differences became insignificant or disappeared altogether in the COPD groups, suggesting that COPD may negate some of the cardiovascular protection that (premenopausal) females normally have.19 ,20 This seems to be in line with the finding that females are more sensitive to smoking than males. In a systematic review and meta-analysis of data from more than 2.4 million people, the relative risk of coronary heart disease conferred by cigarette smoking was 25% greater in females, independent of other risk factors.12 The pathophysiological basis by which cigarette smoking is more hazardous in females is not clear. Because females who smoke also have double the risk of lung cancer compared with males who smoke, it has been postulated that females might extract a larger quantity of carcinogens from the same amount of cigarette smoke.12 21 22
Comparison with other literature
Despite a relative paucity, there are a number of studies that already reported an increased incidence of ischaemic heart disease, atrial fibrillation and heart failure in patients with COPD.11 23–30 For example, a study among almost exclusively male outpatient Veterans in the USA executed between 1991 and 1997, showed that the IRR in patients with COPD compared with those without COPD was 4.01 (95% CI 3.80 to 4.24) for coronary artery disease, 4.74 (95% CI 4.27 to 5.26) for atrial fibrillation and 5.94 (95% CI 5.50 to 6.42) for heart failure.29 In a US cohort of patients aged 45–64 years, an inverse relation was found between the incidence of heart failure and forced expiratory volume in 1 s (FEV1).30 Airflow obstruction and reduced FEV1 also increase the risk of atrial fibrillation, independently of race, sex, smoking and several other CVD risk factors.31
The incidence rate ratio in patients with COPD versus patients without COPD was particularly high for heart failure, and less so for atrial fibrillation and ischaemic heart disease. Other cohort studies found similar results, but the underlying pathological mechanisms for the differential increase in heart failure risk remain debatable. One large population-based study showed a linear relationship between severity of airflow obstruction and impaired left ventricular filling without significant changes in left ventricular ejection fraction. Mechanisms of impaired left ventricular filling in COPD may include chronic systemic inflammation, alveolar hypoxia and the loss of the pulmonary capillary bed, resulting in pulmonary vascular changes and increased pulmonary arterial pressure.32 33 In addition, patients with COPD and CVD (eg, ischaemic heart disease) are systemically underprescribed cardiovascular medication, including β-blockers, statins and antiplatelet therapy, which may accelerate the development of heart failure, particularly in patients with prevalent subclinical cardiac dysfunction.34 Lastly, the effect of pulmonary hyperinflation on ventricular haemodynamics has been postulated as an explanation for the strong association between COPD and heart failure.35
In comparison with older literature, the percentage of women in the COPD group of the current study is relatively high. Until recently, COPD was considered a disease that primarily affects men, while women have been shown to be at greater risk of having unrecognised COPD.36 37 However, recent studies reported that the prevalence of COPD has become more similar for men and women, although it remains somewhat higher in men.38–41 The observed convergence between the sexes may in part be a reflection of better recognition of COPD in women, but likely also results from an increased proportion of women among smoking adults. In the Netherlands, the overall percentage of smoking adults has declined in both sexes since 1970, but this decline was greater in men than in women.42
Strengths and limitations
General practitioners in the Netherlands have a gatekeeper’s position, which makes routine primary care data such as provided by the Julius General Practitioners’ Network (JGPN) suitable to inform on the incidence of CVDs. Primary care data are more inclusive than billing codes or hospital care data, because patients with CVDs are increasingly often cared for in the primary care setting and may only visit a hospital in case of an acute event.
Several limitations should be noted, however. First, the presence or absence of outcome was based on ICPC-coding without further case validation. According to previous studies, the JGPN database produces reliable estimates of disease incidence and prevalence, referral and prescription rates7 but a risk of misclassification remains. In addition, given the high levels of unknown CVD in patients with COPD, both the incidence rates and the incidence rate ratios are likely underestimated. Selective screening studies in patients with COPD aged over 60–65 years showed a high prevalence of unrecognised heart failure of 21%.43 In 1535 Danish long-term smokers (59% of which had COPD), CT-scan screening resulted in a new diagnosis of coronary artery disease in 29% of the participants.34 Occult or unrecognised coronary artery disease is even more prevalent in patients with advanced COPD.44 Lastly, despite a large cohort size, a number of cases in lower age categories were small particularly in the COPD group, resulting in wider CIs.
Conclusion
The incidence of the major chronic progressive heart diseases is higher in individuals with COPD compared with those without, with the highest incidence rate ratio observed for heart failure. The largest risk differences for development of a CVD in patients with COPD versus those without, were found in the youngest age groups.
Data availability statement
Data may be obtained from a third party and are not publicly available. Our data will be returned to the JGPN after publication, in line with JGPN terms and conditions and privacy regulations. The JGPN committee will evaluate requests for data sharing and will make data available under strict conditions.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors FHR, RAdB, AWH, MH, MR, VWZ and AG designed the study. The data were analysed and interpreted by FHR, VWZ, LJS and AG. AG drafted the first version of this manuscript. All coauthors critically reviewed and revised the manuscript before providing final approval. FHR acts as guarantor for this study.
Funding This work was supported by the Dutch Heart Foundation [CVON2017-11].
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.