Article Text

Abstract
Background The ROX index (Respiratory rate-OXygenation) has been described as a prediction tool to identify the need for invasive mechanical ventilation (IMV) in community-acquired pneumonia (CAP) with acute hypoxaemic respiratory failure treated with high-flow nasal cannula in order to avoid delay of a necessary intubation. However, its use in predicting the need for ventilatory support in hospitalised patients with CAP has not been validated.
Methods This is a retrospective cohort study including subjects with CAP treated in the general ward, emergency service or intensive care unit of a third-level centre in Cundinamarca, Colombia, between January 2001 and February 2020. The ROX index was estimated as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate.
Results A total of 895 patients were included, of whom 93 (10%) required IMV. The ROX index proved to be a good predictor, presenting an area under the curve of receiver operating characteristics (AUROC) of 0.733 (95% CI 0.671 to 0.795, p<0.001) when determined by pulse oximetry and an AUROC of 0.779 (95% CI 0.699 to 0.859, p<0.001) when estimated by arterial blood gas (ABG) parameters, with an intraclass correlation of 0.894. The estimated cut-off point was 14.8; a score less than 14.8 indicates high risk of requiring IMV.
Conclusion The ROX index is a good predictor of IMV in hospitalised patients with CAP. It presents good performance when calculated through pulse oximetry and can replace the one calculated by ABG.
- pneumonia
- respiratory infection
- bacterial infection
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Community-acquired pneumonia (CAP) is a leading cause of hospitalisation and oxygen therapy is one of the initial therapeutic measures for this condition; however, its use as an invasive ventilatory support predictor in hospitalised patients with CAP has not been validated.
WHAT THIS STUDY ADDS
In this cohort of CAP-diagnosed subjects who were admitted to the emergency service, general ward or intensive care unit of a third-level hospital, the ROX index (Respiratory rate-OXygenation) was found to be a good predictor of requirement for invasive mechanical ventilation in adult patients with CAP.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights that the ROX index could be an easy-to-use bedside tool to predict the need for mechanical ventilation in patients with pneumonia due to the use of vital signs, which supports its use as a non-invasive tool for respiratory monitoring of patients with CAP.
Introduction
Community-acquired pneumonia (CAP) is a leading cause of hospitalisation and death in the world due to an infectious cause. Its global incidence ranges between 1 and 14 per 1000 person-years and it causes up to 2.5 million deaths annually.1–3 Between 22% and 42% of patients require hospitalisation and 10%–14% are admitted to an intensive care unit (ICU),4 5 with a 30-day mortality of between 10% and 12% in the general ward and up to 35% in the ICU, making it the most lethal infectious disease.1–4 6
Multiple scores have been developed to classify the severity of pneumonia and allow definition of the need for hospitalisation in regular wards or ICUs. The Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS) guidelines7 8 recommend two instruments for predicting mortality and evaluating the site of care in pneumonia: Pneumonia Severity Index or PSI9 10 and CURB-65 (confusion, urea nitrogen, respiratory rate, systolic or diastolic blood pressure, 65 years or older).10 11 After admission, it is also suggested to estimate scores that qualify the severity of the disease, such as the IDSA/ATS criteria which determine admission to the ICU, stating as major severity criteria the need for invasive mechanical ventilation (IMV) or the presence of septic shock requiring vasopressors.7 8 10 These criteria reflect the two most relevant complications of CAP which are associated with an increase in mortality2: ventilatory failure and shock.
Acute hypoxaemic respiratory failure (ARF) which accompanies severe CAP may manifest early with a decrease in arterial oxygen pressure (PaO2) and arterial oxygen saturation (SaO2), mainly due to the ventilation–perfusion mismatch mechanism leading to imbalances in gas exchange at the alveolar level; this alteration can occur in 58%–87% of patients with severe CAP.2 12 Oxygen therapy is one of the initial therapeutic measures for this condition and can be administered by low-flow and high-flow systems before providing positive pressure.13 14 Nevertheless, there are no tools for early identification of patients who require IMV.15 16 Recently, Roca et al17 18 validated the ROX index (‘Respiratory rate-OXygenation’) as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate (SpO2/FiO2:RR) and has shown promising performance in the successful prognosis of oxygen therapy with high-flow nasal cannula (HFNC).
However, its use as a predictor of ventilatory support in hospitalised patients with CAP has not been validated. The aim of the present study is to determine the validity of the ROX index as a predictor of requirement for IMV in patients with a diagnosis of CAP in whom HFNC was not administered.
Methods
Study design
This was a retrospective cohort study conducted on CAP-diagnosed subjects who were admitted to a third-level hospital (Clínica Universidad de La Sabana) located in the municipality of Chía, Cundinamarca (Colombia). Data were gathered between January and August 2020 from clinical records dated January 2001–February 2020.
Inclusion and exclusion criteria
Subjects were eligible for inclusion in the study if they met the following criteria: age ≥18 years, acute respiratory symptoms (≤15 days of evolution) and diagnosis of pneumonia according to the IDSA/ATS7 8 and British Thoracic Society4 guidelines for CAP, determined by presence of symptoms (cough, dyspnoea, fever, pleuritic pain and/or altered state of consciousness) or signs suggestive of pulmonary infection (heart rate (HR) ≥100 beats per minute, respiratory rate (RR) ≥20 breaths per minute, temperature ≥38°C, rales or wheezing on auscultation), associated with radiological findings on chest X-ray and/or chest CT compatible with pneumonia (alveolar and/or interstitial pulmonary opacities, unilateral, bilateral or multilobar pulmonary consolidation) and requirement for antibiotic treatment. Subjects who needed immediate mechanical ventilation prior to admission were excluded.
Analysed variables
Information was obtained on demographic variables, duration and characteristics of the clinical features at presentation, comorbidities through the Charlson index, vital signs, findings on physical examination, laboratory tests (complete blood count, serum creatinine, urea nitrogen, glucose, serum albumin), pulse oximetry measurements and arterial blood gas (ABG) values, diagnostic imaging findings (chest X-ray and/or chest CT), FiO2 and SpO2 at admission, and measured FiO2 to maintain an SpO2 >90% consistently. In addition, ICU stay, IMV requirement, vasopressor therapy or systemic corticosteroids, and death were considered as outcomes within 28 days. At the time of admission, the ROX index (SpO2/FiO2:RR) was calculated from oximetry records and ABG measurements (SaO2/FiO2:RR). CURB-65 was also estimated. The criteria for IMV were altered Glasgow Coma Scale (GCS) score <12 and severe haemodynamic instability with vasopressor support or persisting or worsening respiratory condition, defined as at least two of the following criteria: failure to achieve correct oxygenation (PaO2 <60 mm Hg despite FiO2 of 100%), respiratory acidosis (arterial partial pressure of carbon dioxide (PaCO2)>50 mm Hg with pH <7.25), RR greater than 30 breaths per minute or inability to clear secretions.17 18 A specialist in internal medicine or critical care was in charge of ordering the initiation of IMV in the emergency service and general ward prior to the failed attempt at non-IMV.
Biases
With the aim of reducing information and transcription biases, data were verified by at least two members of the research group directly from the electronic medical records.
Sample size
The sample size was calculated according to the results of Roca et al,17 18 where sensitivity of 70.1% and specificity of 72.4% were reported, with an outcome frequency of 10%, requiring a minimum of 806 subjects for a precision of 10% and a reliability level of 95%. Records were entered in a non-probabilistic way and those who did not meet the inclusion criteria were substituted until the required sample size was reached.
Statistical analysis
Information was obtained directly from the electronic medical records, which were reviewed in a complete manner and compiled in the electronic data capture software Research Electronic Data Capture (REDCap). Later, it was downloaded into an Excel spreadsheet to perform the final analysis in the licensed SPSS V.25 program. An initial description of data per variable was made and records with a loss greater than 20% were excluded. Qualitative variables were summarised in frequencies and percentages. Quantitative variables, if their distribution was normal, were summarised in mean and SD, and if their distribution was not normal in median and IQR. A bivariate analysis was carried out comparing the quantitative variables using Student’s t-test or Mann-Whitney U test according to their distribution and the qualitative variables by χ2 test; subsequently, the variables with significant association in the bivariate analysis were analysed in a multivariate analysis to assess whether the ROX index was an independent factor for predicting IMV. Receiver operating characteristic curves (ROCs) were performed and the area under the curve of receiver operating characteristics (AUROC) was calculated for RR, SpO2, ROX index and CURB-65 and then compared with mechanical ventilation and death through the DeLong test. Sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio (LR+), negative likelihood ratio (LR−), number needed to diagnose and number needed to misdiagnose were calculated with their respective 95% CI, and a p value of less than 0.05 was considered to indicate statistical significance. Youden’s J statistic was used to determine the optimal cut-off point for the ROX index in the analysed cohort. The DeLong test was used to compare the ROX index and CURB-65 AUROCs.
Ethical considerations
Patients were not involved in the development of the research question, design, recruitment or intervention burden assessed; no patient advisors were required and data were analysed anonymously. The results will be disseminated to the scientific community in academic writing.
Results
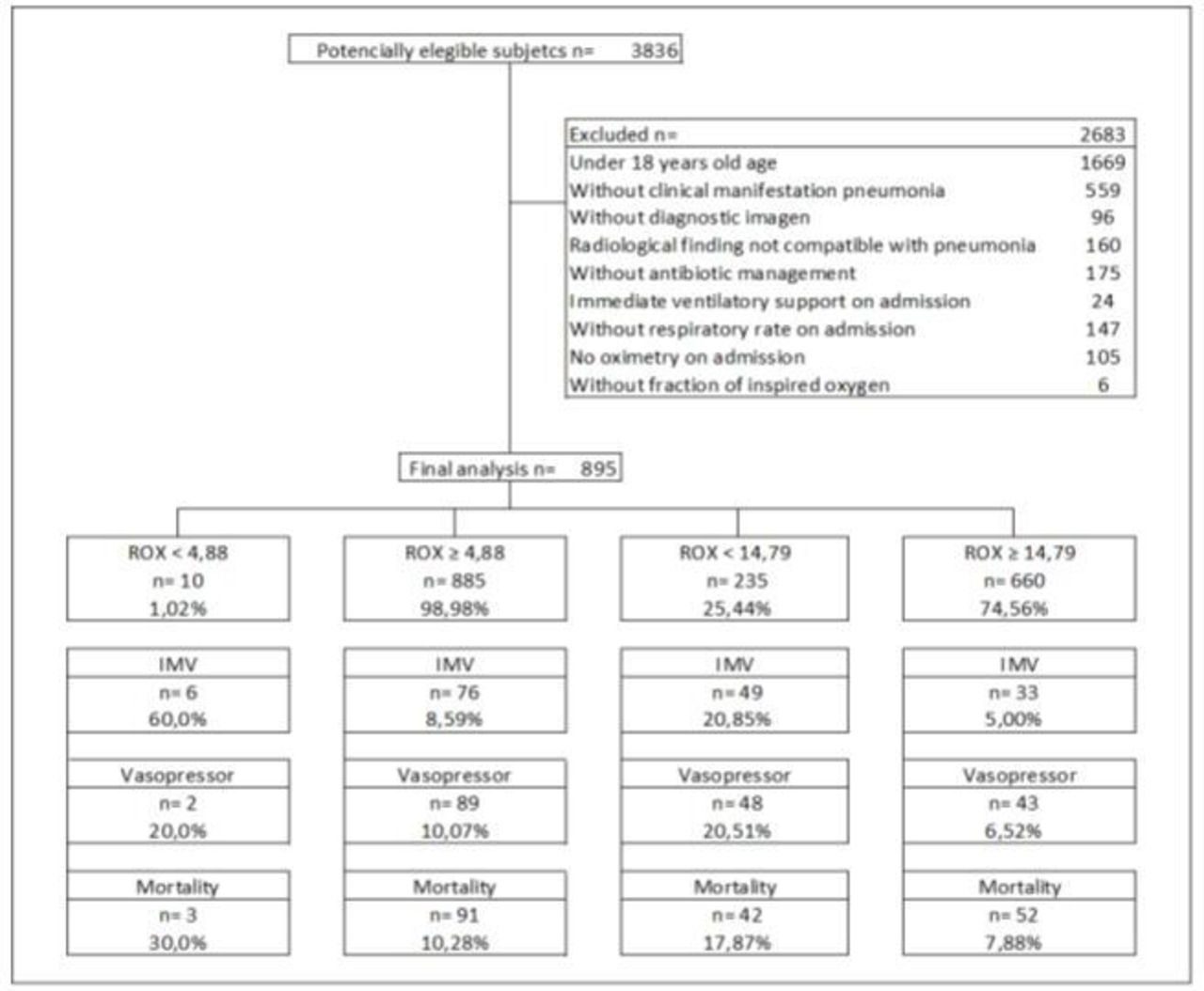
From the 3836 potentially eligible patients, a total of 895 subjects entered the final analysis. A higher percentage requirement for IMV and vasopressor support as well as a higher mortality in patients with lower ROX index regardless of the cut-off point were noted (figure 1). The data are reflected with the cut-off point found by Roca et al17 18 and according to the cut-off point with the best performance for the studied population.
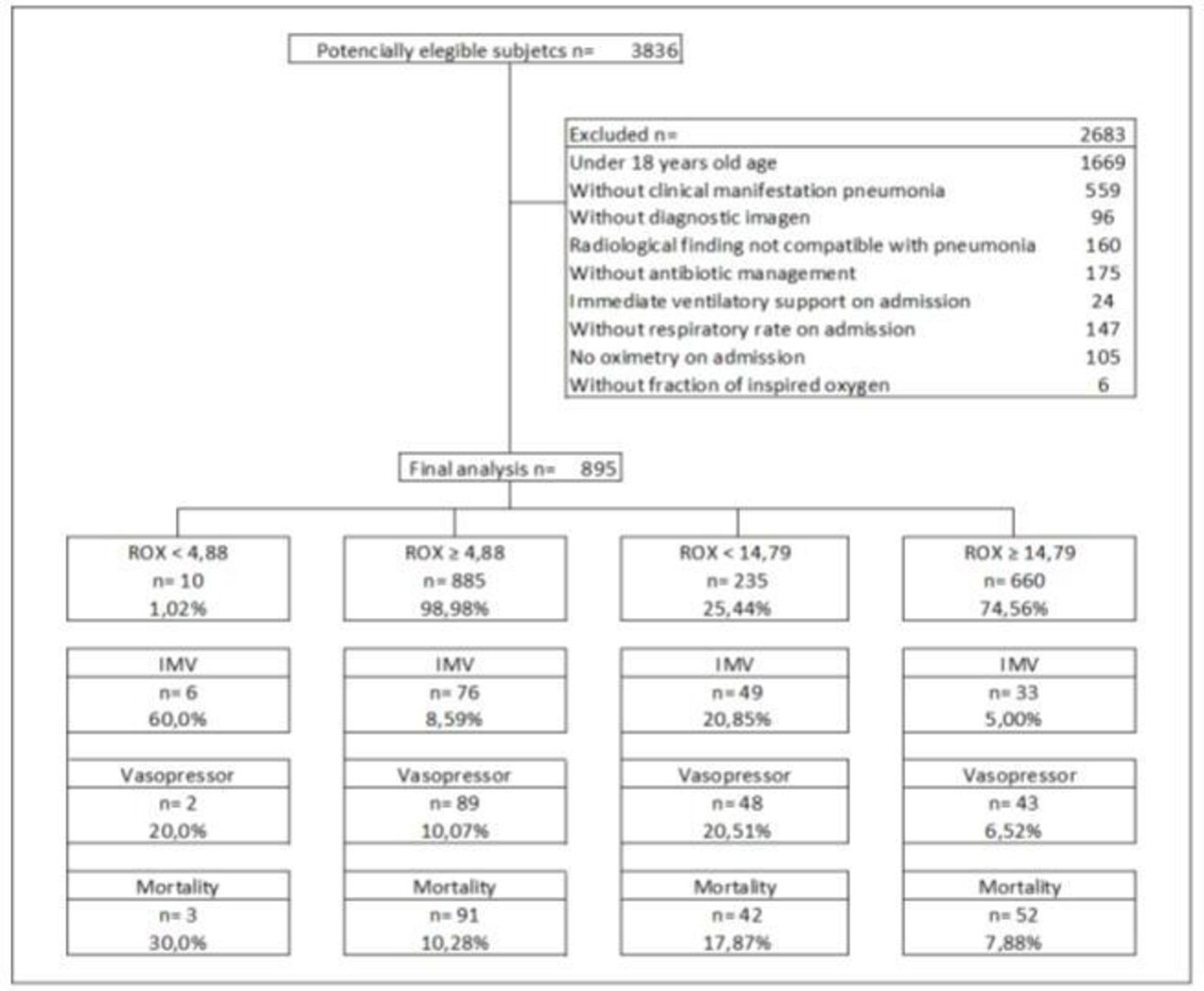
Flow chart of the study cohort. IMV, invasive mechanical ventilation, vasopressor support and mortality; ROX index, Respiratory rate-OXygenation index as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate.
The mean age of the selected patients was 67.01 years (SD 20.41) and 516 (58.1%) were men. No significant relationships were found with other prevalent conditions in the studied population (table 1). The most frequent clinical findings in the study population of 895 patients were cough in 733 (81.9%), dyspnoea in 615 (68.7%) and rales on auscultation in 457 (51.0%). Among the findings on physical examination at admission, a significant relationship was found between retractions (IMV: 36 of 93 (38.7%) vs non-IMV: 142 of 802 (17.7%), p<0.001), cyanosis (IMV: 15 of 93 (16.1%) vs non-IMV: 66 of 802 (8.2%), p=0.012) and altered state of consciousness (IMV: 28 of 93 (30.1%) vs non-IMV: 121 of 802 (15.0%), p<0.001). In addition, higher HR (mean (SD), IMV: 100.65 (22.28) vs non-IMV: 91.64 (19.41), p<0.001), higher RR (mean (SD), IMV: 24.83 (8.90) vs non-IMV: 21.39 (5.62), p<0.001), altered GCS (IMV: 74 of 93 (79.6%) vs non-IMV: 508 of 802 (63.3%), p=0.003) and higher FiO2 requirement (mean (SD), IMV: 41.10 (22.37) vs non-IMV: 25.85 (7.29), p<0.001) at admission were significantly related to use of IMV. Likewise, findings of multilobar involvement were evident on both chest radiographies (IMV: 47 of 93 (50.5%) vs non-IMV: 198 of 802 (24.8%), p<0.001) (table 1).
Baseline characteristics of the patients
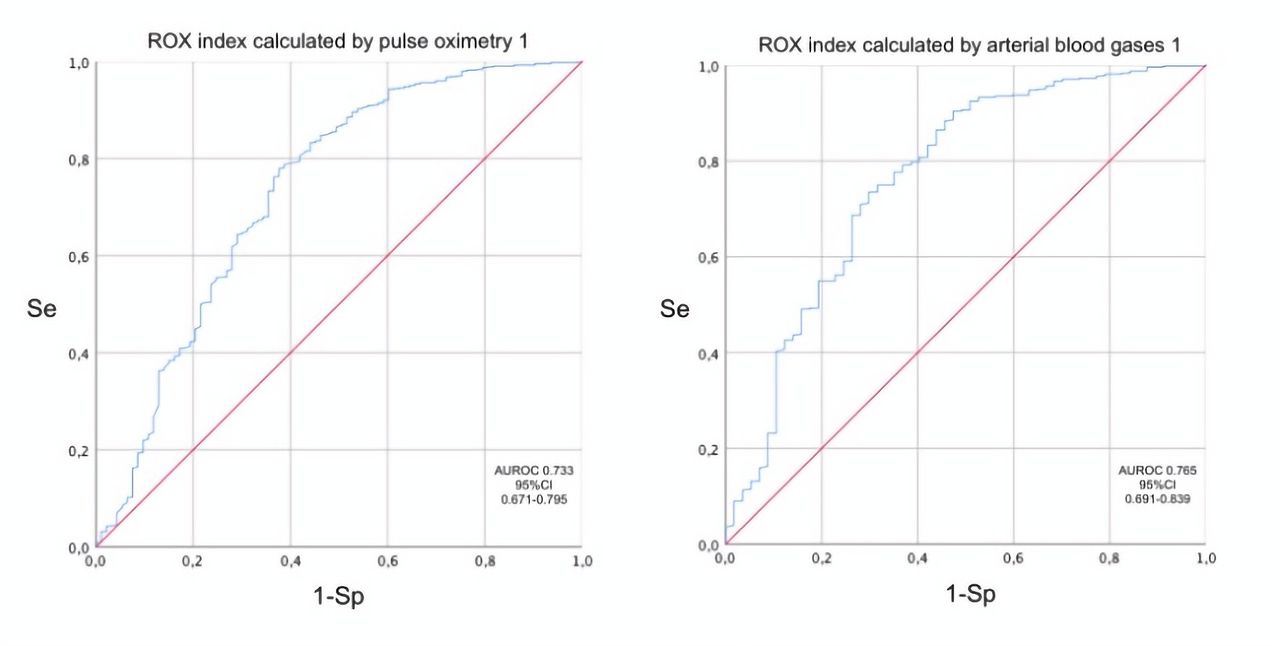
The ROX index among the studied population showed a similar behaviour regardless of the method of obtaining oximetry measurements (by pulse oximetry or ABG), with an intraclass correlation coefficient of 0.894 (figure 2). Lower mean values were evidenced in subjects who required IMV (ROX index by pulse oximetry: 13.4±6.4, p<0.001; ROX index by ABG: 11.5±6.0, p<0.001) compared with patients who did not require IMV (ROX index by pulse oximetry: 18.5±5.0, p<0.001; ROX index by ABG: 17.2±5.1, p<0.001) (table 2).

ROX index according to oxygen saturation measurements. AUROC, area under the curve of receiver operating characteristics; ROX index, Respiratory rate-OXygenation index as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate; Se, sensitivity; Sp, specificity.
ROX index calculation from pulse oximetry and ABG at admission
Among the studied population, it was found that those who required IMV had more cases of septic shock (IMV: 54 of 93 (58.0%) vs non-IMV: 49 of 802 (6.12%), p<0.001), required vasopressor support in greater proportion (IMV: 65 of 93 (69.8%) vs non-IMV: 26 of 802 (3.2%), p<0.001), more treatment with systemic corticosteroids (IMV: 50 of 93 (54.3%) vs non-IMV: 175 of 802 (21.8%), p<0.001) and longer ICU stay (IMV: 87 of 93 (93.5%) vs non-IMV: 53 of 802 (6.6%), p=0.003) compared with subjects who did not need IMV.
In the multivariate analysis, the ROX index is an independent factor for IMV prediction between the variables age, sex, cough, cyanosis, retractions, alterations in consciousness, pH, carbon dioxide partial pressure and multilobar involvement, with an adjusted OR of 1.12 (95% CI 1.06 to 1.18, p<0.001).
When comparing by the AUROC, it is noted that the ROX index (AUROC 0.73, 95% CI 0.67 to 0.79, p<0.001) has an independent performance superior to its variables, AUROC for SpO2 of 0.57 (95% CI 0.49 to 0.65, p=0.052) and AUROC for RR of 0.63 (95% CI 0.55 to 0.70, p<0.001), with DeLong test (p<0.001). Comparison using the DeLong test between the AUROC of the ROX index (0.73, 95% CI 0.67 to 0.79) and the AUROC of CURB-65 (0.52, 95% CI 0.45 to 0.59) in predicting IMV showed statistical significance (p<0.001). Likewise, oximetry values or arterial blood gases (ABG) obtained during the hospital stay were analysed (table 3). The performance of the ROX index according to FiO2 and independently of the oxygen delivery system used revealed better results in oxygen-enriched air administration starting with an FiO2 equal or greater than 0.28, as presented in table 3 and figure 3.

Variability of the ROX index performance according to FiO2. AUROC, area under the curve of receiver operating characteristics; FiO2, fraction of inspired oxygen; ROX index, Respiratory rate-OXygenation index as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate; Se, sensitivity; Sp, specificity.
ROX variables and ROX index for prediction of invasive mechanical ventilation and its performance according to FiO2
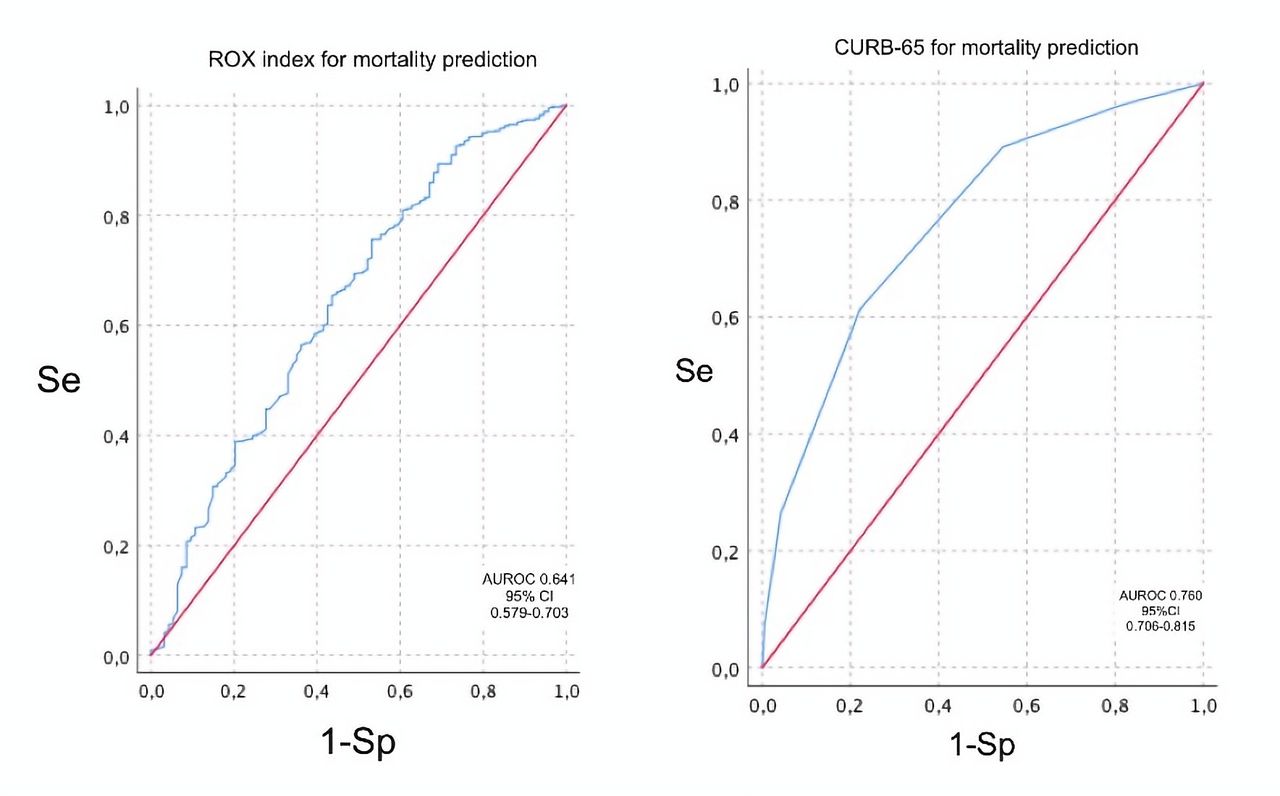
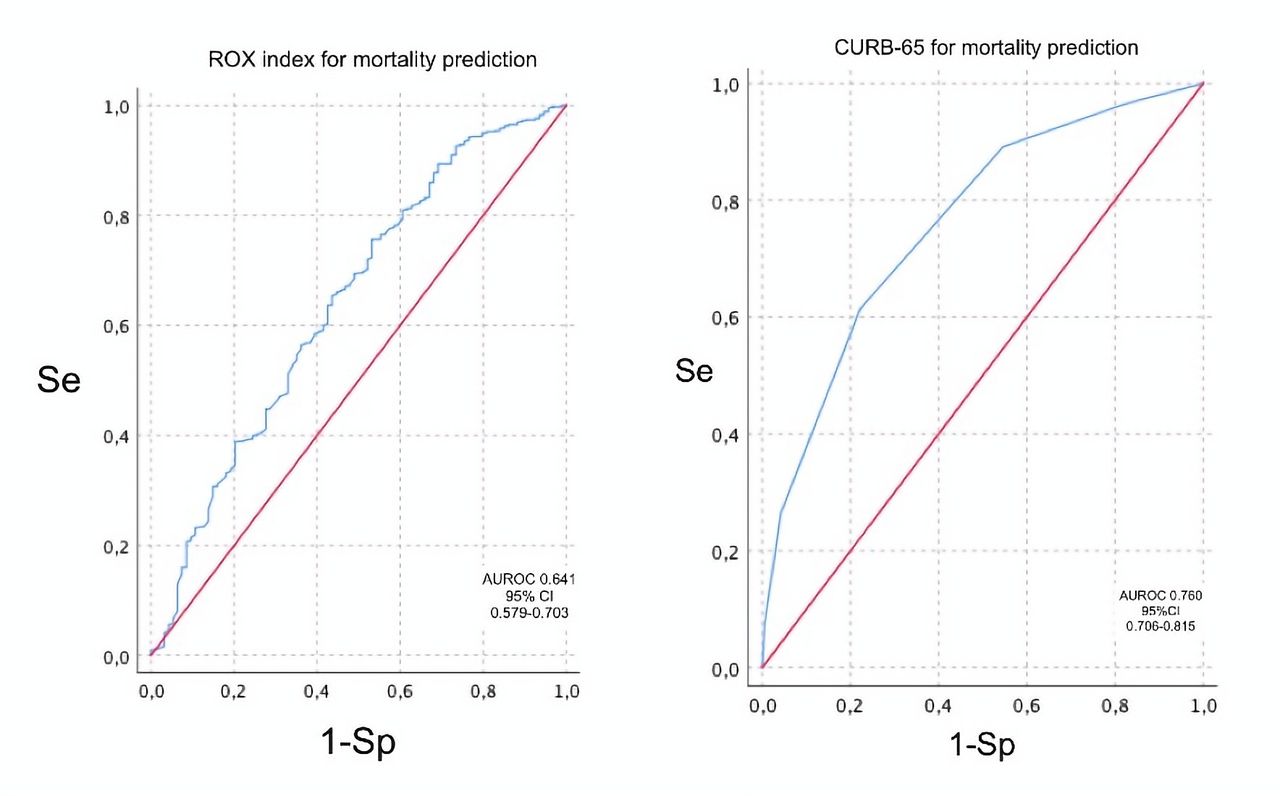
Opposite to other oxygenation indices, a similar but higher behaviour was evidenced compared with the PaO2:FiO2 ratio (AUROC 0.70, 95% CI 0.62 to 0.78, p<0.001) and higher compared with other indices such as the alveolar-arterial oxygen gradient (AUROC 0.68, 95% CI 0.59 to 0.77, p<0.001) (table 4) when evaluated for prediction of IMV. In contrast, if a comparison between the CURB-65 and the ROX index is made, the CURB-65 in our cohort still works as a better predictor of mortality in patients with CAP, as evidenced by the ROC in figure 4 and the AUROC values presented in table 5. Nonetheless, the ROX index appears to have superior accuracy in determining the need for IMV.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison between the ROX index and CURB-65 for predicting mortality. AUROC, area under the curve of receiver operating characteristics; CURB-65, confusion, urea level, respiratory rate, systolic or diastolic blood pressure, 65 years or older; ROX index, Respiratory rate-OXygenation index as the ratio of oxygen saturation/fraction of inspired oxygen to respiratory rate; Se, sensitivity; Sp, specificity.
Prediction of invasive mechanical ventilation by oxygenation indices and CURB-65
Comparison of the ROX index and CURB-65 in predicting mortality
Discussion
The ROX index was found to be a good predictor of the requirement for IMV in adult patients with CAP, presenting better performance in subjects with a supplemental oxygen requirement with FiO2 ≥28%. Compared with the CURB-65, the ROX index is a better predictor of IMV requirement, although it does not show a remarkable performance in predicting mortality. Finally, an intraclass correlation of very good magnitude was established between the ROX index calculated from pulse oximetry and ABG, which supports its use as a non-invasive tool for respiratory monitoring of patients with CAP.
The ROX index was validated as a good predictor of IMV and success or failure on HFNC, with a reduction in the requirement for mechanical ventilation.19–22 HFNC has become a significant initial therapeutic alternative in ARF that, due to its characteristics, allows administration of FiO2 of between 0.21 and 1.0 and oxygen flows of up to 60 L/min.23–25 In this study, we have demonstrated that the ROX index is a good predictor of IMV in hospitalised patients with CAP, but with a higher threshold value than proposed by Roca et al17 (4.88 vs 14.79). The main reasons for using a higher threshold were the inclusion of conventional low-flow oxygen devices, the mean age of the population and the higher percentage of patients with less severe hypoxaemia, cared for in uncontrolled settings such as emergency rooms and general rooms.
Ferrer et al26 evaluated the usefulness of the ROX index in patients with a diagnosis of bilateral pneumonia with ARF due to SARS-CoV-2. The findings of the study showed that the ROX index is useful in assessing HFNC use in SARS-CoV-2 pneumonia, with a cut-off point of 5.35, after 24 hours with ventilatory support. On the other hand, Vega et al27 demonstrated that the ROX-12 discriminates HFNC success from failure in patients with COVID-19 and guides clinicians in their decision to intubate patients, with a cut-off point of 5.99. Our data are supported by current studies26 27 in which the ROX index has been evaluated with thresholds higher than those described by Roca et al.17 18
Moreover, the ROX index is a superior predictor for defining the requirement for IMV compared with the CURB-65. Although both scales assess breathing work by considering RR, the ROX index considers SpO2 and therefore reflects hypoxaemia, and in relation to the FiO2 required by the patient, it is a parameter that defines ventilatory failure.28 29 Furthermore, Spada et al30 documented the usefulness of the SpO2:FiO2 ratio as a predictor of IMV associated with non-invasive positive pressure ventilation, so the utility of the ROX index as a predictor of IMV is expected. Scores such as the CURB-65 evaluate the multisystemic involvement associated with severe pneumonia, so it remains a tool whose main use is prediction of mortality.11
The correlation between the ROX index calculated through SpO2 (by pulse oximetry) and SaO2 (by ABG) is good. Studies comparing SpO2:FiO2 and PaO2:FiO2 values suggest that taking this non-invasive measure could replace ABG measurements in patients with acute respiratory failure triggered by any cause, as evidenced by Cinesi-Gómez et al.31 Similarly, SpO2 and SpO2:FiO2 have been suggested for titration of FiO2 in patients requiring oxygen therapy with acute lung injury or established acute respiratory distress syndrome (ARDS); an SpO2:FiO2 ratio of 235 is related to a PaO2:FiO2 of 200 (oxygenation criterion for ARDS), with sensitivity and specificity of 85%32; this evidence supports that the correct use of SpO2 could reduce the amount of ABG performed in the ICU and emergency room, being cost-effective and reducing discomfort in patients.
A limitation of this study is that it was developed in a single centre, which limits generalisation of the results; however, the sample size achieved is considered to support our conclusions. From a technical viewpoint, the present study, being retrospective and supported by medical records, is limited by the quality of the information, adequate measurement of variables (SaO2, SpO2, FiO2), calibration of equipment used, as well as interobserver variability in the measurement of the RR; hence, there is a risk of loss of information. However, in order to prevent biases, different strategies were used during the design and statistical analysis stages, such as the double validation conducted by different investigators. The elevation above sea level at which the study was carried out (2640 meters above sea level) could be considered a limitation since oxygenation values at high altitudes over 2500 masl are expected to be less than those obtained at sea level in non-ventilated patients, as proven by previous studies33; notwithstanding, validation studies of oxygenation indices at this altitude do not seem to show large differences in measured values at sea level.33 Prospective studies are required to corroborate the performance of the ROX index in other causes of ARF or in younger groups.
Conclusions
The ROX index is an easy-to-use bedside tool because it only uses vital signs. It shows usefulness in predicting mechanical ventilation requirement in patients with pneumonia, mainly in those who receive supplemental oxygen with FiO2 greater than 28% through low-flow or high-flow oxygen delivery systems different from HFNC. Prospective studies are required to corroborate its performance and cut-off points in ARF caused by other diseases.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the institutional ethics committee of Clínica Universidad de La Sabana.
References
Footnotes
Contributors ABG had full access to all study data and takes responsibility for data integrity as well as for the accuracy of the included data analysis and especially any adverse effects. LFR, ABG, EAT, KDP, YFM, MH, GAC, LDS, LEB, CAM, JCC, JCA, PMA, MDH, APN, NT, AFP and GSM contributed substantially to the study design, data analysis and interpretation, and manuscript writing. LFR and ABG accepted full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors approved the manuscript for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.