Article Text

Abstract
Rational Corticosteroid therapy plays a key role in the treatment of COVID-19 patients with respiratory failure. However, a rebound phenomenon after steroid cessation rarely occurs. Here, we investigated the clinical features of patients with rebound after steroid therapy.
Methods In total, 84 patients with COVID-19 treated with corticosteroids were enrolled and analysed retrospectively. A rebound was defined as when a patient’s respiratory status deteriorated after the cessation of corticosteroid therapy, without secondary bacterial infection.
Results Subjects in the rebound group were more likely to having severe respiratory failure than those in the non-rebound group. While the duration of steroid therapy was longer in the rebound group (8 days vs 10 days, p=0.0009), the dosage of steroid and the timing of the start or termination of steroid therapy did not show any differences between the two groups (p=0.17 and 0.68, respectively). The values of soluble interleukin-2 receptor (sIL-2R) at the baseline and the values of C reactive protein (CRP) or lactate dehydrogenase (LDH) at the end of steroid therapy were significantly higher in the rebound group (937 vs 1336 U/mL; p=0.002, 0.63 vs 3.96 mg/dL; p=0.01 and 278 vs 451 IU/mL; p=0.01, respectively). No patient in the rebound group suffered from thromboses, and the causes of death were exacerbation of COVID-19, ventilator-associated pneumonia or sepsis. The prediction model using baseline features for the rebound phenomenon included four variables of age >68 years, required supplemental oxygen >5 L/min, lymphocyte counts <792 /µL and sIL-2R >1146 U/mL. The discrimination ability of this model was 0.906 (0.755–0.968).
Conclusion These findings suggest that severe respiratory failure has a higher risk for the rebound phenomenon after the cessation of corticosteroids, and the values of sIL-2R, LDH and CRP are useful to assess the probability of developing rebound. A multivariate model was developed to predict rebound risk, which showed acceptable discrimination ability.
- COVID-19
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the present study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Many clinical parameters, such as age, history of hypertension, lymphocyte counts and D-dimer, are known as predictors of COVID-19 progression. However, little is known about the clinical characteristics of COVID-19 patients with rebound pneumonia after corticosteroid therapy.
What this study adds
Severity of respiratory failure is associated with frequency of rebound phenomenon. Prolonged higher values of lactate dehydrogenase and C reactive protein at the end of steroid therapy increase the risk of rebound. The prediction model with selected baseline characteristics also provides good discrimination ability. Patients with rebound have a poor prognosis.
How this study might affect research, practice or policy
This study provides useful information to distinguish high-risk patients who will develop rebound after the cessation of corticosteroid therapy. A novel therapeutic approach, such as prolonged steroid treatment, might benefit such patients.
Introduction
The clinical course of COVID-19 consists of two phases, that is, a viral replication phase in the early stage and a hyperinflammation phase in the later stage.1 2 Different treatment strategies are preferred depending on the phase. Antiviral therapy, such as remdesivir, molnupiravir and neutralising antibody, are recommended to be initiated as soon as possible in the early viral replication phase, while anti-inflammatory therapy, such as corticosteroids, anti-IL-6 antibody and Janus kinase inhibitor, is considered to be more beneficial when administered in later hyperinflammatory phase.1–8 Among these therapeutic options, dexamethasone is a key drug for patients with severe COVID-19. The RECOVERY trial demonstrated that 6 mg of dexamethasone for up to 10 days reduced the mortality compared with usual care alone for severe illness.5 However, whether dexamethasone (6 mg) for up to 10 days is the most optimal approach is unclear, because almost all other ongoing randomised control trials with different therapeutic strategies using corticosteroids were halted after the RECOVERY trial.9 Therefore, there still remained many important clinical questions concerning the optimal dosage, duration or timing of corticosteroids therapy as well as the benefit of coadministration of antiviral drugs. Indeed, a case of rebounding COVID-19 pneumonia was experienced after the cessation of 6 mg dexamethasone for up to 10 days and was recovered after the readministration of steroids.10 11 This suggested that the duration or dosage of steroids therapy could be insufficient for some cases. Shionoya et al12 reported that the administration of steroids prior to antiviral drugs soon after symptom onset leads to a poor outcome but whether administrating steroid with or without antiviral drugs is associated with the rebound phenomenon is unclear. Many clinical parameters, such as age, coexisting diseases, lymphocyte count, D-dimer and lactate dehydrogenase (LDH), have been reported as predictors of COVID-19 progression since the COVID-19 pandemic began. Although prediction models using some of these parameters for the progression of COVID-19 have been well developed, there have been few reports about the rebound of COVID-19.13 14 One retrospective study reported that patients with rebound pneumonia tended to terminate steroids earlier in the disease process and showed a poor prognosis.15 Although the rebound phenomenon after corticosteroid therapy is an important problem in clinical practice, the clinical features of patients with rebound have not been well studied. The present study aimed to reveal the clinical features of patients with rebound pneumonia after corticosteroid cessation, to investigate risk factors and predictable markers and to propose novel therapeutic approaches for high-risk patients.
Methods
Study design and patient population
This was a single-centre, retrospective cohort survey that targeted patients with COVID-19. All patients were diagnosed with COVID-19 by a SARS-CoV-2 test with a PCR assay. The requirement for informed written consent was waived based on the ethics guidelines of Tohoku University Graduate School of Medicine, because this study was retrospective and did not involve any invasiveness. In total, 84 patients with COVID-19 admitted to the Tohoku University Hospital were enrolled in this study from 1 September 2020 to 31 July 2021. Systemic corticosteroid therapy, 6 mg of dexamethasone or the equivalent dose of other corticosteroids, was initiated if the patients’ respiratory status required supplemental oxygen (usually SpO2 <92%). Patients who did not receive systemic corticosteroid therapy or who were transferred to another hospital during the course of illness were excluded. The study was carried out in accordance with the Declaration of Helsinki.
Patients’ characteristics and medical information including age, sex, smoking status, laboratory findings, comorbidity and medication profile were obtained from the patients’ medical chart. The patients’ respiratory status was assessed by an original six-point ordinal scale: 1: death; 2: requiring invasive mechanical ventilation or extracorporeal membrane oxygenation; 3: requiring non-invasive ventilation or high-flow nasal canula (HFNC); 4: requiring higher flow rate conventional oxygen (>5 L/min oxygen by mask with/without reservoir); 5: requiring lower flow rate conventional oxygen (5 L/min or less oxygen); and 6: not requiring any supplemental oxygen.
The patients were classified into two groups, that is, non-rebound and rebound groups. The non-rebound group was defined as patients who were responsive to initial corticosteroid therapy and did not show a rebound phenomenon after the cessation of corticosteroid therapy. The rebound group was defined as follows: (1) patients who deteriorated more than one point on the ordinal scale or deteriorated after the cessation of systemic corticosteroid therapy and (2) bacterial coinfection was excluded as a cause of deteriorating respiratory status by routine clinical practices.15 The determination of rebound was performed by two independent pulmonologists or infectiologists. Patients without improving respiratory status at any time during the corticosteroid therapy were also excluded (n=2) because such patients had a steroid-resistance phenotype and were unable to be classified either of two groups previously.
Statistical analysis
Data of age, body mass index and laboratory findings were expressed as median and IQR (IQR (Q1–Q3)). The clinical characteristics were compared using Mann-Whitney U test or Fisher’s exact test. Variables with a p value <0.05 were regarded as candidates for the prediction model, and stepwise selection was applied to them to select candidate predictors. Multivariate logistic regression analyses were performed to evaluate the association between baseline features and the outcome. The receiver operating characteristics (ROC) curve was plotted to set the cut-off values at the best point of sensitivity and specificity and to calculate the area under the curve. For the association between respiratory status and rebound tendency, a linear trend was tested by the Cochran-Armitage trend test. Statistical significance was accepted as p<0.05. All statistical analyses were performed using JMP Pro V.16 software (SAS Institute, Inc).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Patient characteristics
A total of 213 patients were admitted to Tohoku University Hospital with COVID-19 during the study period. Among them, 129 patients were excluded because of mild severity without steroid therapy (n=125), changing hospital (n=2) or non-responsive to corticosteroid therapy (n=2), and then 84 patients (age: 68 (55–68) years old; female, 20 subjects (23.8%)) were finally enrolled in this study. Among them, four patients without respiratory support were treated with steroids because their oxygen saturation was 90%–91% at room air. The characteristics of the subjects with COVID-19 are summarised in table 1. Of 84 subjects treated with systemic corticosteroid, 12 patients (14.3%) were classified into the rebound group according to our criteria. Subjects in the rebound group were more likely to be older, had a greater severity of respiratory failure and a higher prevalence of diabetes and chronic kidney disease. Regarding the laboratory data, subjects in the rebound group had lower lymphocyte counts and higher values of soluble interleukin-2 receptor (sIL-2R) and D-dimer, while the values of lactate dehydrogenase (LDH), ferritin and C reactive protein (CRP) did not show any difference between the non-rebound and rebound groups. The administration rates of antiviral drugs or immunosuppressants other than corticosteroids were similar between the two groups, and the mortality was significantly higher in the rebound group (p=0.0003).
Patients characteristics
The details of patients with rebound are shown in online supplemental table 1. There was no apparent trend in the baseline features between lethal cases and non-lethal cases. All patients were administered with anticoagulant therapy and no patient suffered from severe thromboses. Causes of death were exacerbation of COVID-19 (n=2), ventilator-associated pneumonia (n=1) and sepsis due to catheter-related blood stream infection (n=1).
Supplemental material
Comparison of systemic corticosteroid therapy between the non-rebound and rebound groups
We first analysed whether the regimens of corticosteroid treatment showed any difference between the non-rebound and rebound groups.
The median duration of initial corticosteroid treatment was longer in the rebound group than in the non-rebound group (8 (7–10) days vs 10 (10–13.5) days, p=0.0009) (figure 1A). The median initiation time from symptom onset to first steroid administration did not show any difference between the two groups (7.5 (5–10) days vs 6.5 (3.3–8) days, p=0.17) (figure 1B). The median time from symptom onset to steroid cessation was also similar between the two groups (15 (13–18) days vs 15.5 (12.3–18) days, p=0.68) (figure 1C).
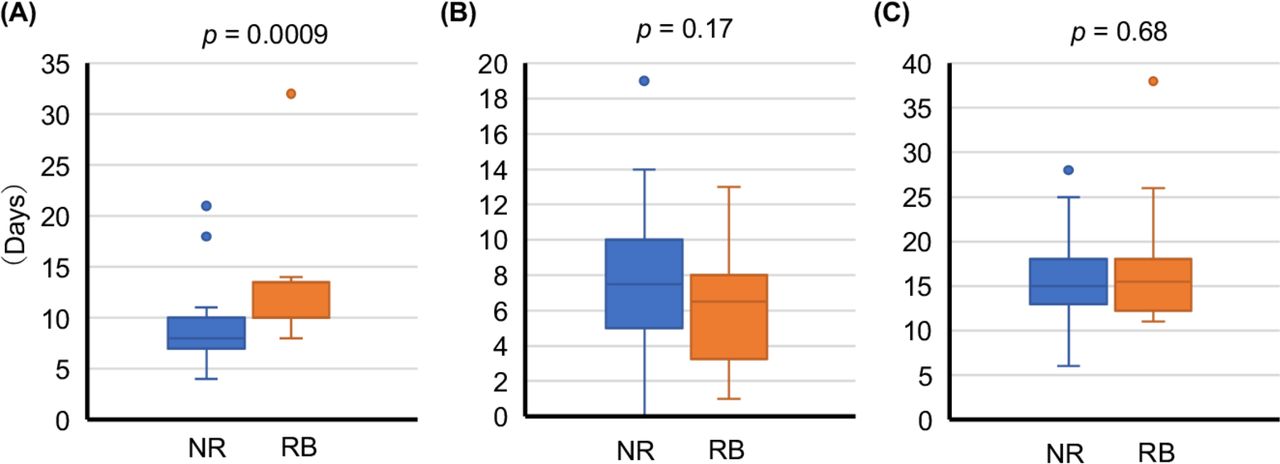
Comparison of the corticosteroid treatment between patients with and without a rebound phenomenon. Comparison of box plot: duration of steroid administration (A), days from symptom onset to initiation of steroid (B) and days from symptom onset to cessation of steroid (C) between non-rebound (NR) and rebound (RB) group. Boxes indicate median and IQR, and whiskers indicate minimum-maximum range. Data were analysed using Mann-Whitney U-test. Statistical significance was accepted as p<0.05.
Association between severity of respiratory failure and rebound tendency
We next investigated whether a greater severity of the respiratory status during the corticosteroid treatment was associated with a rebound tendency.
More than 90% of the subjects in the rebound group required a higher flow rate of oxygen (> 5 L/min), HFNC or invasive respiratory support, while almost 80% of the subjects in the non-rebound group had a lower flow rate of conventional oxygen (≤5 L/min) (figure 2A). While only 1.7% of the subjects with a lower flow rate of oxygen experienced a flaring of the COVID-19 pneumonia after the cessation of corticosteroid therapy, 33% of those with a higher flow rate of oxygen or HFNC, and 60% of those with invasive respiratory support experienced flare-up (Cochran-Armitage trend test p<0.0001) (figure 2B). These results suggested that more severe respiratory status was prone to rebound the pneumonia associated with COVID-19.
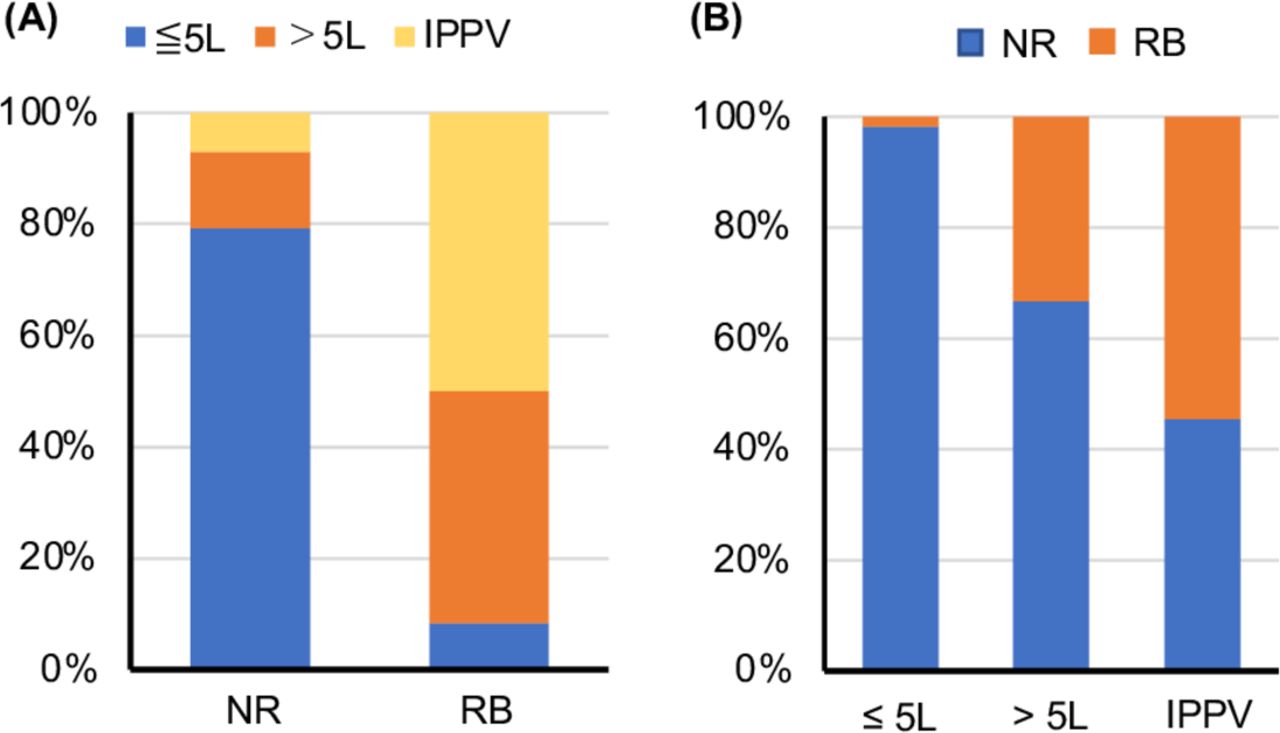
Association between rebound phenomenon and severity of respiratory failure. Bar graphs show the comparison of severity of respiratory failure between non-rebound (NR) and rebound (RB) group (A) and the rate of rebound phenomenon according to each respiratory status (B).
Comparison of laboratory findings obtained at the end of steroid cessation
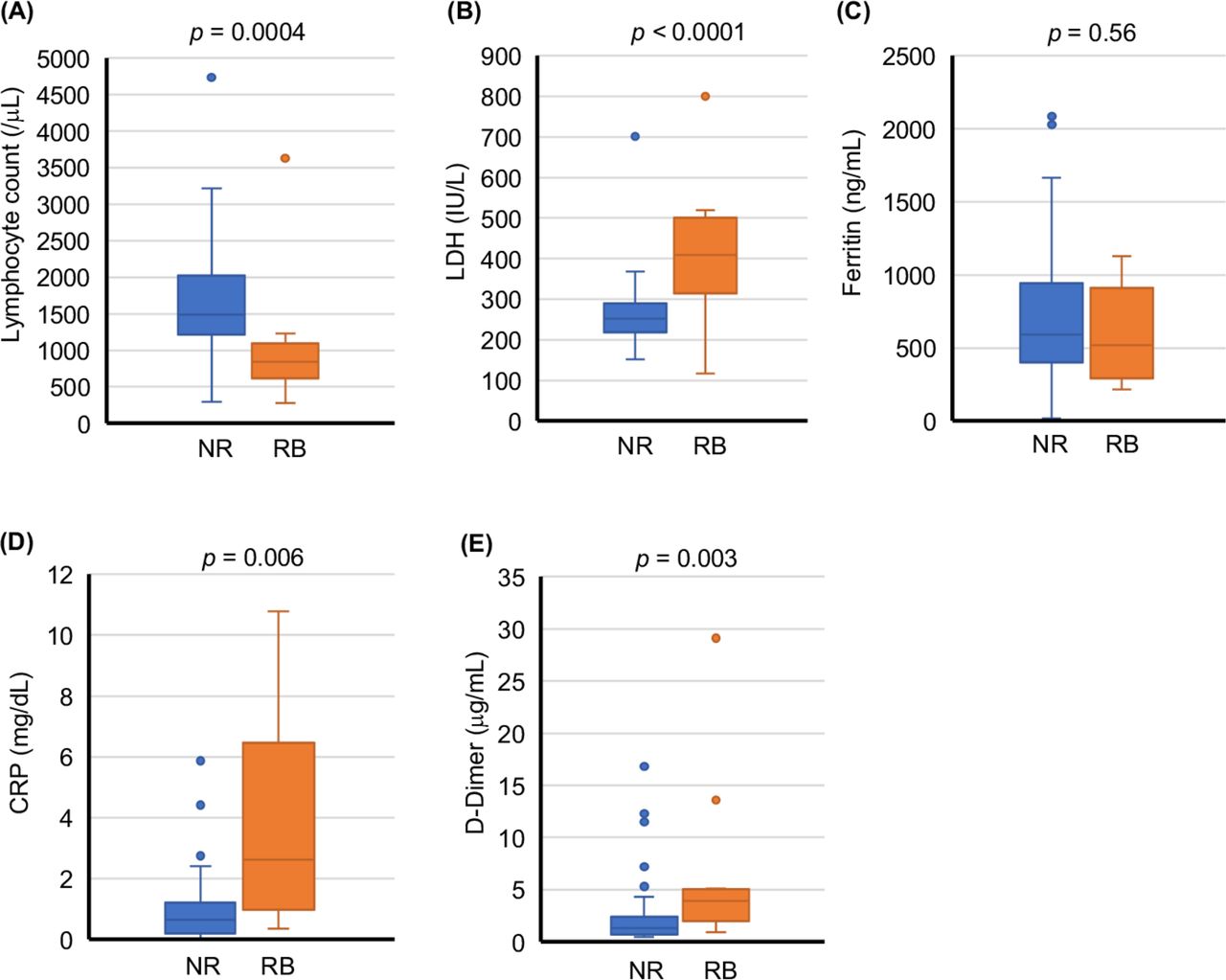
To estimate the risk for rebound after corticosteroid cessation, we compared the laboratory data obtained within 2 days before and after corticosteroid cessation. We chose five biomarkers, lymphocyte count, LDH, ferritin, CRP and D-dimer, to estimate the rebound risk because these biomarkers are known to have an association with the severity of COVID-19.16 17 Except ferritin, all other biomarkers showed significant differences between the two groups (figure 3). The lymphocyte count was lower in the rebound group (1490 (1212–2024) vs 841 (619–1091) /μL, p=0.0004) and the values of LDH, CRP and D-dimer were higher in the rebound group (LDH: 252 (218-290) vs 410 (315-500) IU/L, p<0.0001, CRP: 0.66 (0.19–1.22) vs 2.63 (0.97–6.45) mg/dL, p=0.006 and D-dimer: 1.3 (0.7–2.4) vs 3.9 (2.0–5.1) µg/mL, p=0.003) (figure 3A, B, D and E).

Comparison of the laboratory test associated with severe COVID-19 between the non-rebound (NR) and rebound (RB) groups. Comparison of box plot of the values of lymphocyte count (A), LDH (B), ferritin (C), CRP (D) and D-dimer (E) between the NR and RB groups. Boxes indicate median and IQR, and whiskers indicate minimum–maximum range. Data were analysed with Mann-Whitney U-test. Statistical significance was accepted as p<0.05.
The prediction model using baseline features
Six variables with a p value <0.05 in the baseline features (age, respiratory status (supplemental oxygen >5 L/min), history of diabetes or chronic kidney disease, lymphocyte counts and values of sIL-2R) were selected as candidate predictors. The selected parameters with correspondent cut-off values by the ROC curve were: age >68 years, lymphocyte counts <792 /µL, sIL-2R >1145 U/mL and D-dimer >2.7 mg/mL. A prediction model comprising four predictors was obtained by applying the stepwise variable selection procedure. Multivariate logistic regression analyses showed supplemental O2 >5 L/min, age over 68 years, lymphocyte counts <792 /µL and sIL-2R >1146 U/mL were significantly associated with higher rebound tendency (OR: 42 (5–350); p=0.0006, 5.9 (1.2–28.9); p=0.03, 12.6 (2.5–63.4); p=0.002 and 13.2 (2.6–67.7); p=0.002, respectively) (table 2). The prediction performance of this model was acceptable as represented by an AUC of 0.906 (0.755–0.968) (figure 4).
Multivariate logistic regression analyses of the risk of rebound phenomenon

Receiver operating curve of the prediction model. Area under curve was 0.906 (95% CI 0.755 to 0.968). Variables included in this model: age >68 years, required supplemental oxygen >5 L/min, lymphocyte counts <792 /µL and sIL-2R >1146 U/mL.
Subanalyses of patients with severe respiratory failure
Since figure 2 showed that the subjects with severe respiratory failure were more likely to rebound compared with those with less severe respiratory failure, we compared the characteristics of only those with severe respiratory failure, who required >5 L/min conventional oxygen, HFNC or invasive respiratory support. Of the 25 subjects with severe respiratory failure, 11 (44%) were classified into the rebound group, which had a significantly higher prevalence of diabetes and chronic kidney disease, and higher values of sIL-2R compared with the 14 subjects in the non-rebound group (table 3). The treatment for COVID-19 other than corticosteroid was similar between the two groups. Notably, mortality was significantly higher in the rebound group (p=0.009) (table 3).
Characteristics of patients with severe respiratory failure
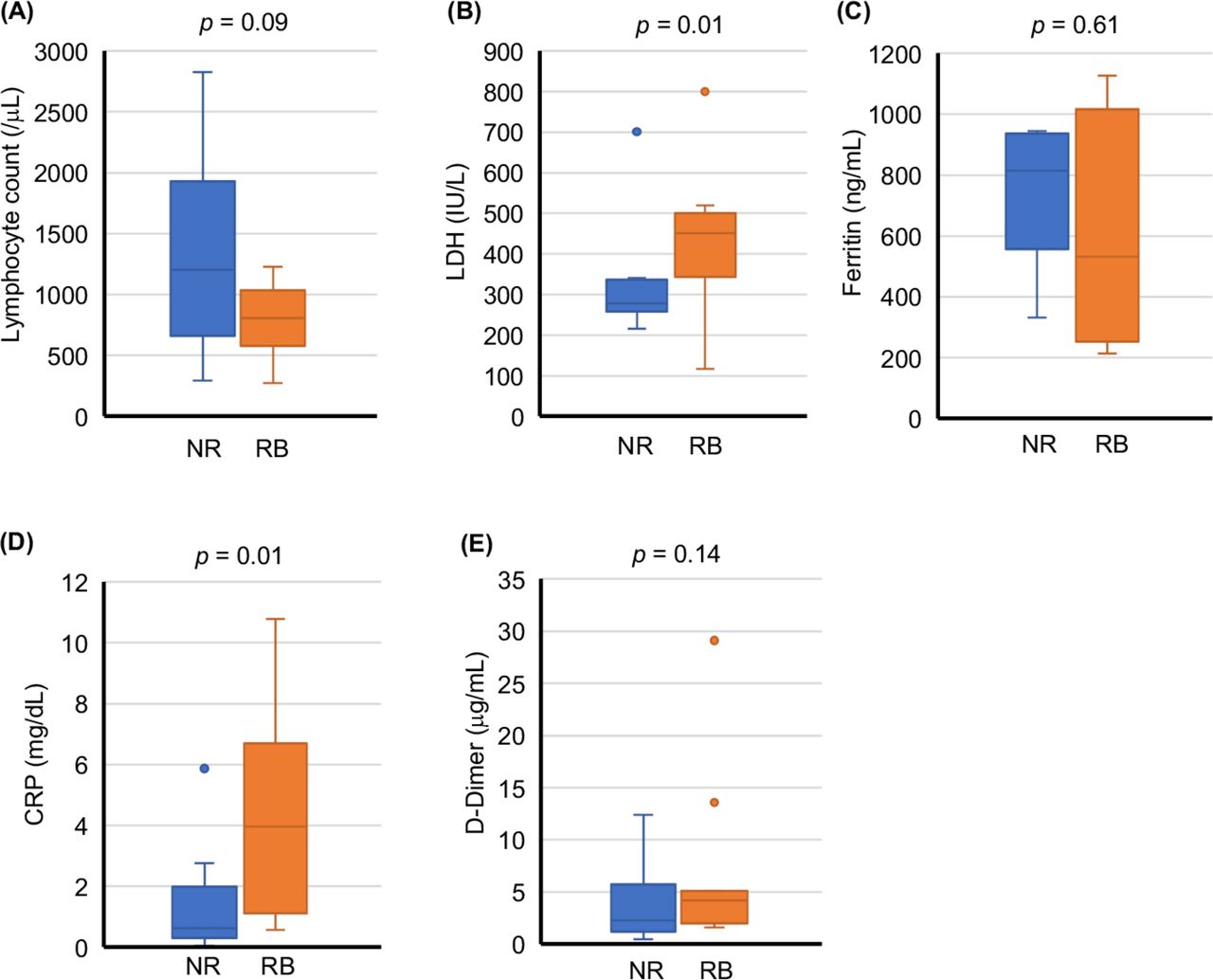
To predict the risk for rebound after corticosteroid cessation, we compared the laboratory data obtained within 2 days before and after corticosteroid cessation. In contrast with figure 3, only two biomarkers, LDH and CRP, showed significant differences between the non-rebound and rebound groups (LDH: 278 (259–337) vs 451 (344–501) IU/L, p=0.01, CRP: 0.63 (0.30–1.98) vs 3.96 (1.11–6.70) mg/dL, p=0.01) (figure 5B and D). The ROC curves for LDH and CRP were generated to set the cut-off value and calculate the AUC (online supplemental figure 1). The AUCs were 0.811 (95% CI 0.519 to 0.945) for LDH and 0.804 (95% CI 0.572 to 0.927) for CRP. The cut-off values were 344 IU/L for LDH and 0.92 mg/dL for CRP. In the univariate logistic regression analysis using these cut-off values, higher levels of LDH (>344) and CRP (>0.92) were associated with a higher rebound tendency (OR: 24.7 (2.9–212); p=0.0007 and 16.0 (1.6–166); p=0.02, respectively) (online supplemental table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of the laboratory test results associated with severe COVID-19 between severe COVID-19 patients with and without a rebound phenomenon. Patients with severe respiratory failure (n=25) were reanalysed. Comparison of box plot of the values of lymphocyte count (A), LDH (B), ferritin (C), CRP (D) and D-dimer (E) between the non-rebound (NR) and rebound (RB) groups. Boxes indicate median and IQR, and whiskers indicate minimum–maximum range. Data were analysed with Mann-Whitney U test. Statistical significance was accepted as p<0.05.
Discussion
Systemic corticosteroids play a central role in the treatment for COVID-19 with respiratory failure. However, rebound after the cessation of steroids rarely occurs.11 15 18 The clinical features of patients who rebound have not been elucidated, and predicting such an occurrence is difficult. In the present study, we revealed that subjects with greater severe respiratory failure were more likely to experience a rebound of pneumonia after the cessation of steroids (figure 2). Among subjects with severe respiratory failure (> 5 L/min supplemental oxygen, HFNC or invasive respiratory support), the coexistence of diabetes or chronic kidney disease was a risk factor for rebound (table 3). Additionally, the values of sIL-2R before steroid administration and the values of LDH or CRP measured at the end of steroid treatment were significantly higher in the rebound group (table 3 and figure 5). We further propose a potential prediction model (table 2 and figure 4). This model including age >68 years, required supplemental oxygen >5 L/min, lymphocyte counts <792 /µL and sIL-2R >1146 U/mL showed good discrimination ability (AUC=0.906). To our knowledge, this is the first study that assessed the characteristics of COVID-19 patients with rebound and predictors of rebounding COVID-19 pneumonia.
The RECOVERY trial revealed that 6 mg of dexamethasone for up to 10 days reduced the mortality of patients with respiratory failure.5 However, there still remain several clinical questions concerning the use of corticosteroids. The optimal timing of initiation, dosage and duration of steroids administration have not been elucidated yet.9 Concerning the details of corticosteroids therapy in this study, the types and dosage of the corticosteroids administered did not show any difference between the rebound and non-rebound groups. The duration of corticosteroids therapy was significantly longer in the rebound group. These results suggested that insufficient therapy was not responsible for the rebound observed in this study. The RECOVERY trial also showed that subjects with symptoms persisting more than 7 days experienced a greater benefit from corticosteroids therapy than those with a more recent symptom onset.5 Imai et al15 also reported that early cessation of corticosteroid therapy entails risk of rebound. However, the number of days from symptom onset to the initiation of steroid therapy or to the cessation of steroid therapy did not show any difference between the rebound and non-rebound groups in this study (figure 1). A possible explanation for this difference is that the previous study had a higher proportion of subjects with mild severity, nearly 30% of total subjects, as compared with 5% in our study.
NIH (National Insitute of Health) recommends the combination of dexamethasone plus remdesivir for patients with severe respiratory failure based on a theoretical benefit without high-quality evidence (BIIb).19 A previous study reported that the administration of steroids prior to antiviral therapy soon after symptom onset could result in poor outcomes.12 Although steroids therapy with or without antiviral drug might influence the rebound phenomenon, the ratio of antiviral use was similar between the two groups in the present study. Likewise, some studies reported that the combination of steroids plus anti-IL-6 antibody or other immunosuppressants showed better outcomes than steroids monotherapy,3 6 and the use of other immunosuppressants in this study did not show any difference between the two groups.
The present study revealed that mortality was significantly higher in the rebound group than in the non-rebound group. The causes of death were not only respiratory failure due to COVID-19 pneumonia but also secondary infection after the rebound pneumonia. Severe thromboses were not observed in the rebound group. In line with our study, Imai et al15 also reported that the number of days for clinical improvement was longer in patients with rebound phenomenon. Since the rebound phenomenon is likely to contribute to a poor prognosis, novel therapeutic strategies for patients at high-risk for rebound will be necessary. One possible treatment option is extending the steroid therapy for high-risk patients, since the values of CRP at the end of steroid therapy were significantly higher, indicating that inflammation still persisted.
Although the actual cause of the rebound phenomenon is not clear, viral reinfection, viral reactivation and/or secondary organising pneumonia are considered possible causes.10 11 18 20 In the present study, all patients continued hospitalisation at the time of rebound and this suggests that there was no chance of reinfection. However, since we did not test for SARS-CoV-2 PCR repeatedly at the end of steroid therapy, viral reactivation might have occurred, leading to the rebound phenomenon. Likewise, we did not perform lung biopsy to determine the presence of secondary organising pneumonia and therefore could not exclude this possibility. Because the prognosis and response to readministration of corticosteroid were quite different among patients with rebound, there might be differences in the pathophysiology leading to rebound. A further clinical study will be necessary.
There are several limitations in this study. First, the sample size and the number of events observed in this study were relatively small. Second, since this study is a retrospective study, a prospective study with a larger sample size will be required to confirm these results. Third, we did not have any information about the strain or viral load of SARS-CoV-2. Whether viral factors influenced the rebound phenomenon is unclear. Delta variant has stronger virulence compared with other strains, and it might influence the rebound risk. However, all cases with rebound were before delta variant spreading in Japan. Fourth, our model was not validated by external cohort and might be at risk of overfitting. However, we tried to prevent overfitting by decreasing the number of predictors.
Conclusions
In conclusion, the present study revealed that COVID-19 patients with more severe respiratory failure, especially those with prolonged higher values of LDH or CRP, were at higher risk of rebound after the cessation of corticosteroid therapy. Our study also developed a multivariate prediction model for the rebound phenomenon. Since patients with rebound might have a poorer prognosis, we should investigate novel therapeutic strategies for high-risk patients.
Data availability statement
Data are available on reasonable request. The datasets generated during and/or analysed during the present study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The ethics committee of Tohoku University Graduate School of Medicine approved this study (approval number: 2021-1-386). The requirement for informed written consent was waived based on the ethics guidelines of Tohoku University Graduate School of Medicine, because this study was retrospective and did not involve any invasiveness.
Acknowledgments
The authors gratefully acknowledged Mr. Brent K. Bell for reading the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KM: study design, samples collection, analysis, interpretation of the data and drafting of the manuscript. HS, NT, YT, KS, DN, NK, SM, YO, CI, HS, MS, SK, SK, HK, HB, KO, KT and KT: sample collection. TT: interpretation of the data and drafting of the manuscript. HS: study supervision. KM accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish. All authors reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.