Article Text

Abstract
Background Diffuse pulmonary ossification is a specific lung condition that is accompanied by underlying diseases. However, idiopathic dendriform pulmonary ossification (IDPO) is extremely rare, and the clinical features remain unclear. In this study, we aimed to report the clinical characteristics of IDPO.
Methods We conducted a nationwide survey of patients with IDPO from 2017 to 2019 in Japan and evaluated the clinical, radiological, and histopathological findings of patients diagnosed with IDPO.
Results Twenty-two cases of IDPO were identified. Most subjects (82%) were male, aged 22–56 years (mean (SD), 37.9 (9.1)) at diagnosis. Nearly 80% of the subjects were asymptomatic, and the condition was discovered during a medical check-up. However, 36% of the subjects showed a decline in forced vital capacity (%FVC) predicted <80% at diagnosis. The typical radiological features of high-resolution CT (HRCT) are calcified branching structures that are predominantly distributed in the lower lung fields without any other conspicuous finding. Histopathological analysis also showed dendriform ossified lesions from the intraluminal areas to interstitial areas. Notably, during the follow-up period of 20 years, disease progression was found in 88% on HRCT and more than 50% on pulmonary function tests (FVC and/or forced expiratory volume in 1 s). Two cases with rapid decline of 10% /year in %FVC predicted were observed.
)) at diagnosis. Nearly 80% of the subjects were asymptomatic, and the condition was discovered during a medical check-up. However, 36% of the subjects showed a decline in forced vital capacity (%FVC) predicted <80% at diagnosis. The typical radiological features of high-resolution CT (HRCT) are calcified branching structures that are predominantly distributed in the lower lung fields without any other conspicuous finding. Histopathological analysis also showed dendriform ossified lesions from the intraluminal areas to interstitial areas. Notably, during the follow-up period of 20 years, disease progression was found in 88% on HRCT and more than 50% on pulmonary function tests (FVC and/or forced expiratory volume in 1 s). Two cases with rapid decline of 10% /year in %FVC predicted were observed.
Conclusions IDPO develops at a young age with gradually progressive phenotype. Further research and long-term (>20 years) follow-up are required to clarify the pathogenesis and clinical findings in IDPO.
- Rare lung diseases
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
This is no comprehensive study of idiopathic dendriform pulmonary ossification (IDPO), which is an extremely rare, but noteworthy pulmonary disease.
WHAT THIS STUDY ADDS
We clarified the onset, pulmonary function, clinical course and prognosis, in addition to radiological and histopathological details, and clearly showed the progressive phenotype in the radiological and physiological examinations, although DPO has been reported to be a stable disease.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We will pay more attention to IDPO in the clinical practice and research.
Introduction
Diffuse pulmonary calcification and ossification are rare and asymptomatic conditions involving lung tissues.1 The histopathological changes of both calcification and ossification are known to be accompanied by underlying pulmonary or extrapulmonary diseases,1 and previously, many cases were recognised and diagnosed during autopsy.1–3
Pulmonary ossification is pathologically observed as a condition involving bone formation with or without marrow components appearing in the bilateral lung parenchyma.1 The first case was reported in 1856 by Luschka.4 Early representative reports of autopsy cases showed the presence of underlying diseases such as pulmonary diseases, including idiopathic pulmonary fibrosis (IPF), chronic obstructive pulmonary disease, pneumoconiosis, aspiration pneumonia, acute respiratory distress syndrome, tuberculosis, inhalation of foreign bodies and cardiac diseases, including congestive heart failure and mitral stenosis with chronic pulmonary venous congestion, endocrine diseases (ie, hyperparathyroidism, diabetes mellitus and acromegaly) and malignancies.2 3 5 Recent reports have also demonstrated frequent detection of diffuse pulmonary ossification in high-resolution CT (HRCT) of fibrotic lungs, especially in the case of IPF.6 7
However, since the 1970s, the number of reports of idiopathic cases with diffuse pulmonary ossification has increased. Although Green et al reported a suspected case of idiopathic diffuse pulmonary ossification without any cause in 1970, radiological and histological descriptions were insufficient.8 Ikeda et al reported a similar case with branching-type diffuse ossification in open lung biopsy specimens.9 In the 2000s, several cases of idiopathic cases of pulmonary ossification in the absence of underlying pulmonary or systemic diseases were reported.10–18 The information from these reports indicates the homogenous clinical features such as male-predominance, asymptomatic disease and branching-type ossification on HRCT scans and/or histological findings, but, to our knowledge, there is no comprehensive study on the clinical features including onset, pulmonary function, complications, clinical course, biomarkers and prognosis, in addition to radiological and histopathological details.
We conducted a nationwide study to clarify the clinical findings of idiopathic cases of pulmonary ossification in Japan. Pulmonary ossification is morphologically classified into two subtypes: branching (dendriform) and nodular type. Most of the papers which evaluated idiopathic ossifications, found out dendriform type as the most common form, therefore, we need to use the same term, idiopathic dendriform pulmonary ossification (IDPO), for the findings of our patients.
Methods
Patients
We conducted a nationwide survey in Japan from 2017 to 2019 to understand and clarify the pathophysiology of IDPO. First, a questionnaire was sent by mail to 1791 hospitals with over 200 beds in Japan. Second, we collected the data of these of patients suspected the diagnosis with IDPO: clinical features, data of blood and pulmonary function tests (PFTs) (online supplemental table 1), chest radiography and HRCT scans, and pathological specimens. This study followed the strengthening the reporting of observational studies in epidemiology (STROBE) statement.19 The PFT and HRCT data were collected at two time points, at the time of diagnosis and latest, to evaluate disease progression. Two pulmonologists verified the clinical features, two radiologists independently examined radiological features, and two pathologists examined pathological features and defined IDPO by ruling out patients suspected of other diseases or secondary DPO.
Supplemental material
Radiological analyses
HRCT images were evaluated by two thoracic radiologists for the extent and distribution of calcified lesions and of all other related findings. The extent of parenchymal findings was semi-quantified as follows: 0, none, 1, <10%, 2, 10%–30%; 3, 30%–50%; 4, >50%. Serial changes in HRCT findings were also examined at two time points: time of diagnosis and latest follow-up, when available.
Histopathological analyses
Two pathologists independently evaluated the types and distributions of calcified lesions and other findings from lung tissues resected by surgical biopsy or autopsy.
PFTs and biomarkers
PFTs were performed according to the European Respiratory Society guidelines20 and calculated following the lambda, mu, sigma method.21 The data on vital capacity (VC), forced VC (FVC), forced expiratory volume in 1 s (FEV1) and diffusing capacity of the lung for carbon monoxide (DLco) were collected from each hospital. The data of DLco were available in 16 patients. An obstructive defect was indicated by a low FEV1/FVC ratio, defined as <70% and a FVC predicted of >80%. The %FEV1 predicted and %DLco values were also calculated. A restrictive defect was indicated by a FVC predicted of <80% and a FEV1/FVC ratio >0.8. The PFT data were collected at two time points: time of diagnosis and latest follow-up. The change in each parameter (%FVC predicted, %FEV1 predicted or %DLco predicted) was calculated as relative change: (%/year) = {baseline (%) – latest (%)}/baseline (%)/interval period measured (year).
The biomarker of KL-6, which has been used for the interstitial lung diseases (ILD) was analysed if available.22
Statistical analyses
Fisher’s exact test was performed to compare categorical variables, Welch’s t-test was performed to compare continuous variables, and Mann-Whitney U test was performed to compare the two groups. All p values were two sided and p values of ≤0.05 were considered to be statistically significant. All statistical analyses were performed with EZR (Saitama Medical Centre, Jichi Medical University; Kanda, V.1.51), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria, V.2.6–2).23 Precisely, it is a modified version of the R commander designed to add statistical functions frequently used in biostatistics.23
Patient and public involvement
The patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Selection of patients with IDPO
The answers to the primary questionnaire were recovered from 402 of 1791 hospitals (22%); 33 hospitals had 55 patients suspected of IDPO and 51 patients in 29 hospitals were eligible for analysis (figure 1). In the secondary survey of the patients, we collected clinical data of 39/51 (76%) patients in 25 hospitals. One patient was excluded because of other disease (pulmonary osteochondroma). Seven patients were excluded because they underlying lung diseases such as interstitial pneumonia, bacterial pneumonia, tuberculosis, non-tuberculous mycobacterial infection, mitral stenosis and congestive heart failure, as per their medical records. Radiologically, one patient was further excluded because of asbestosis. As a result, 30 patients were diagnosed using clinical and radiological data. These patients were defined as radiological IDPOs. In addition, six patients were excluded because there were no pathological specimens, and two patients were excluded due to histopathologically confirmed underlying diseases. Finally, 22 cases were determined to be clinically, radiologically and histopathologically diagnosed with IDPO (figure 1). All patients were diagnosed by surgical lung biopsy. Among the 22 patients, the cases of nine patients have already been reported in various journals.12 24–29

Flow chart of selection of patients with IDPO in the study. DPO, dendriform pulmonary ossification; IDPO, idiopathic DPO.
Clinical characteristics of IDPO
The characteristics of the IDPO cases are shown in table 1. Of the 22 patients, 18 (82%) were men. The average age at diagnosis of IDPO was 37.9 years. Eighteen patients (82%) were never smokers. Only two cases (9%) were familial (second degree relatives). Most patients (17/22, 77%) were diagnosed at a medical check-up without any symptoms. Four patients (18%) were diagnosed with respiratory symptoms, including cough (four cases), dyspnoea on exertion (three cases) and sputum (two cases). Medical follow-up had been performed for an average period of 6.36 years (0.01–18.7). One patient developed a pneumothorax. Laboratory data at the time of diagnosis were not specific (data not shown). There were no endocrine or electrolyte disorders, including hypercalcaemia and hyperparathyroidism. Impaired pulmonary function was determined by %FVC predicted <80%, FEV1/FVC <70% and %DLCO predicted <80% that were observed in 8/22 (36%), 2/22 (9%) and 10/16 (63%) patients, respectively, at the time of diagnosis. Restrictive, obstructive and mixed defects in PFTs were found in 7/22 (32%), 1/22 (5%) and 1/22 (5%). Elevation of KL-6 was observed in 3/22 (17%) patients, with the highest value being 882 (U/mL).
Demographic and clinical characteristics of IDPO patients
The radiological characteristics of IDPO
The typical findings of chest radiography and HRCT are shown in figure 2. Chest radiographs showed bilateral linear, reticular and nodular shadows, predominantly distributed in the middle and lower lung fields. HRCT also demonstrated linear opacities and nodules, accompanied by a partly calcified lesion with a lower lobe predominance. To further clarify the HRCT findings, systematic and semiquantitative evaluations were performed by two radiologists (figure 3, (online supplemental table 2), independently. Regarding the craniocaudal distribution of nodules in the lungs, lower field predominance was seen in 18/22 (82%), while diffuse or random distribution was found in 4/22 (18%) (figure 3A). In the horizontal distribution, diffuse in 19/22 (86%), peribronchovascular in 6/22 (27%), peripheral in 1/22 (5%) and random in 1/22 (5%) were observed, respectively (figure 3B). Notably, all patients had fine calcified nodules, calcified short lines and branching structures with or without calcification (figure 3C). In 12/22 (54.5%) cases, fine calcified nodules and calcified branching structures extended in 10%–30% of the lung fields. There were a few interstitial lung changes such as thickening of bronchovascular bundles, pleural thickening or irregularity, non-septal linear opacity and ground glass attenuation (figure 3C). Subpleural curvilinear shadow/line, consolidation and cystic changes were not observed.

Representative images on chest radiography and HRCT of IDPO at the diagnosis. Three cases of IDPO showing the different calcified scores on HRCT and dysfunction on PFTs. Case 1: the low calcified score (total score; 3) without the dysfunction (A), case 2: the high calcified score (total score; 5) without the dysfunction (B), and case 3: the high calcified score (total score; 5) with the dysfunction in PFT (C). Chest radiographs show bilateral reticulonodular shadows (A–C: top), which are most prominent in case 3 (C). Lung window HRCT images show bilateral, diffuse linear and branching structures (A–C: middle) with mild architectural distortion in case 3 (C). On bone window CT images (A–C: bottom), those structures are seen as calcified (arrows) or non-calcified (arrow heads) lesions. (D–F) Lung window images (WW: 1500 HU, WL: −600 HU), (G–I) bone window images (WW: 2000 HU, WL: 500 HU). HRCT, high-resolution CT; HU, hounsfield unit, IDPO, idiopathic dendriform pulmonary ossification; PFTs, pulmonary function tests; WL, window level; WW, window width.
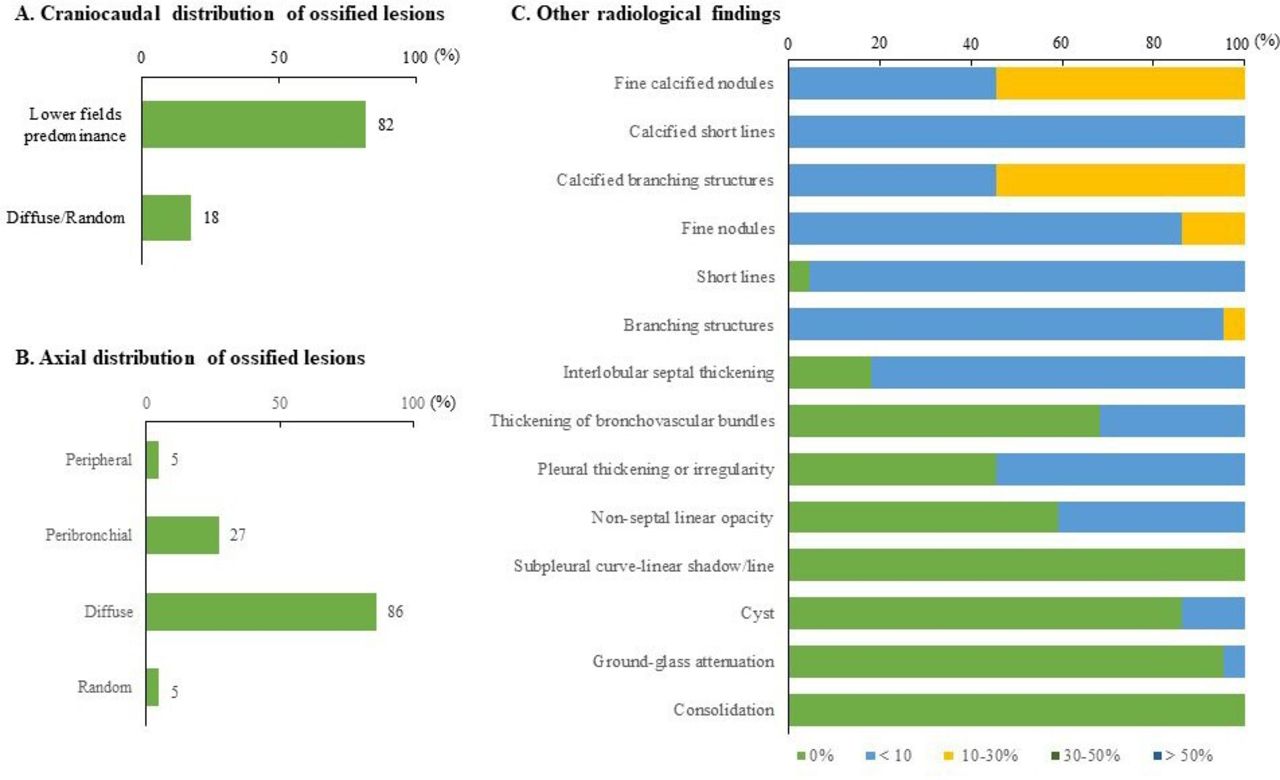
Radiological features of IDPO on chest HRCT. Two radiologists evaluated the HRCT findings of 22 cases of IDPO by using the score sheet (see online supplemental table 2). The data of craniocaudal distribution (A) and axial distribution (B) of ossified lesions were examined. Quantitative and qualitative assessments of calcified lesions, interstitial changes and other findings were performed (C). HRCT, high-resolution CT; IDPO, idiopathic dendriform pulmonary ossification.
When the analysis was performed for all 30 patients with radiological IDPO, similar results were obtained (online supplemental figure 1). Calcified branching structures were also observed in 10%–30% of the lung fields in 15/30 (50%) patients (online supplemental figure 1).
Histopathological characteristics of IDPO
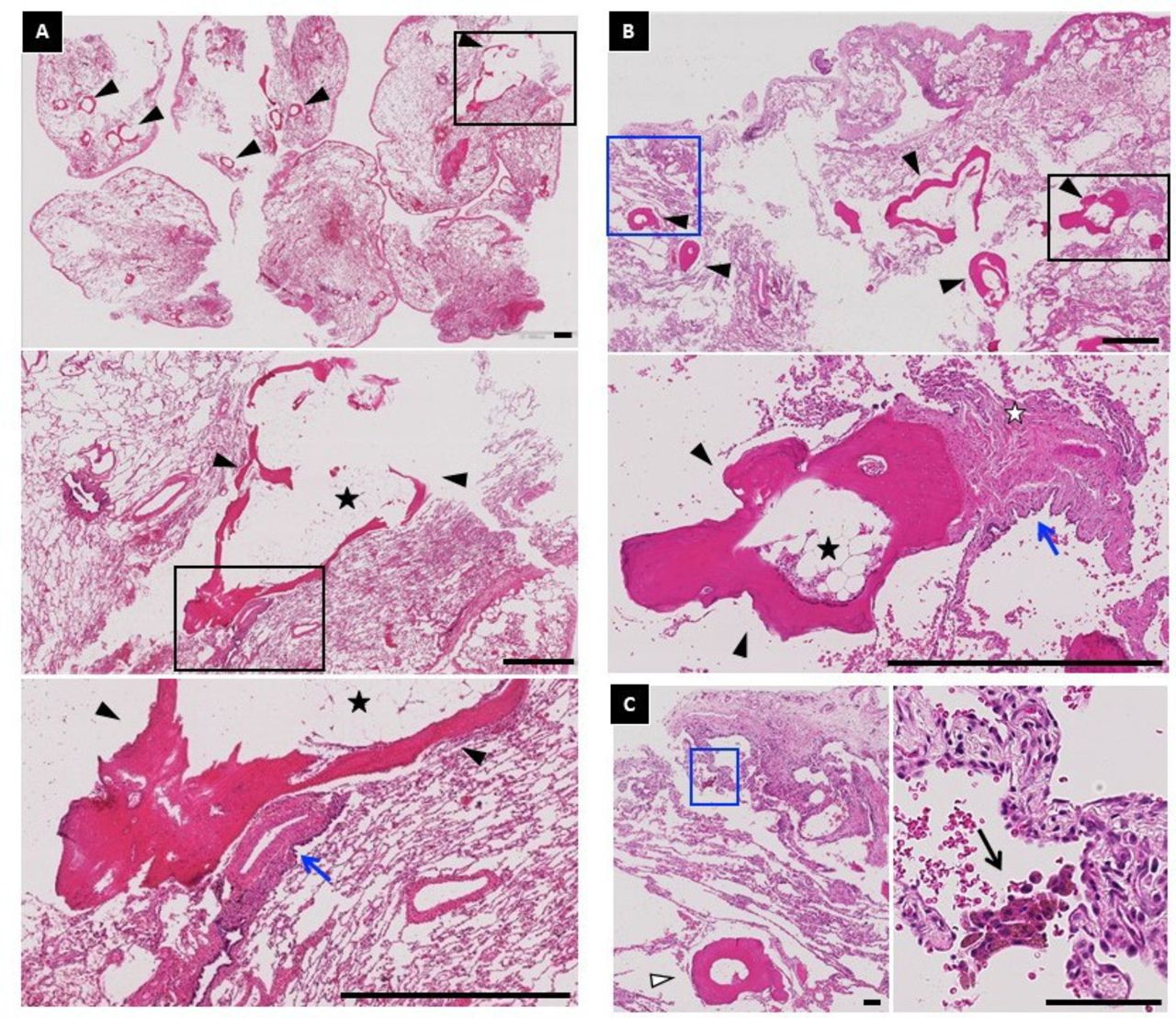
The typical histopathological findings are shown in figure 4. A considerable number of ossified lesions with bone marrow were observed in the lungs (figure 4A,B). On further examination by two pathologists, all patients were found to have dendriform ossified lesions (figure 5A, online supplemental table 3). The maximum size of the ossified lesions was 1.0–6.0 mm. The ossifications were distributed from intraluminal areas of the respiratory bronchioles to alveolar ducts in 13/22 (59%) to interstitial areas including the peribronchial region in 17/22 (77%), perivascular region in 13/22 (59%), subpleural region in 19/22 (86%), and interlobular region in 8/22 (36%) patients (figures 4A, B and 5B). Slight to mild fibrosis was found around the ossified lesion and subpleural region (figures 4A,B and 5C). The infiltration of inflammatory cells was mild, and emphysematous changes were absent in 15/22 (70%) patients (figure 5C). More than half of the patients showed mild to moderate numbers of histiocytes containing pigment granules and haemosiderin (figures 4C and 5C).

Representative images of the histopathological findings of IDPO. (A, B) Low-power views of two specimens from two different IDPO cases. Black arrowheads point to the ossified lesions with branching structures. The ossified lesions with bone marrow (black stars) are visible. High-magnification views of the area are in the black rectangle. (C) The macrophages containing pigment granules (black arrow) were frequently observed. High-magnification views of the area are in the blue rectangle. (A, B) The ossified lesions surrounding fibrotic lesions (white star) are seen along with the bronchovascular bundles (blue arrows) and intraluminal areas (white arrowhead). Scale bars: 1 mm (A, B), 0.1 mm (C). IDPO, idiopathic dendriform pulmonary ossification.

Histopathological features of IDPO. Two pathologists evaluated the histopathological findings by using the score sheet (see online supplemental table 3). The type (A) and distribution (B) of ossified lesions was evaluated. The other findings such as fibrosis and infiltration of inflammatory cells were assessed (C). IDPO, idiopathic dendriform pulmonary ossification.
Clinical course of IDPO
The clinical course of IDPO remains unknown. Therefore, we collected clinical data from two time points, that is, at the time of diagnosis and latest, to evaluate disease progression. The average duration between the two time points was 6.36 years (0.01–18.7 years) (table 2). During the clinical course, three patients (14%) developed dyspnoea on exertion. However, there were no cases of oxygen therapy. HRCT was available in 17 patients with IDPO, whose images were available at two time points with an average interval of 6.52 years (0.11–17.2 years) and ossified lesions progression was found in 15 patients (88%) (online supplemental figure 2). The remaining cases were stable, and none of the cases showed spontaneous regression. PFTs were also measured in 17 patients with IDPO at two time points: at the time of diagnosis and latest follow-up (table 2, (online supplemental table 4). The mean interval between the two points was 6.78 years (0.58 to 18.1 year). At the latest PFTs, impaired pulmonary function showing %FVC predicted<80%, FEV1/FVC <70%, and %DLCO predicted <80% was observed in 9/17 (53%), 2/17 (12%) and 9/17 (53%) patients, respectively. A decline of more than 50 mL/year of FVC or 2.5% relative value of %FVC predicted/year was observed in 10/17 (59%) and 5/17 (29%) patients, respectively (table 2, figure 6A).30 Two patients (12%) showed a decline by more than 10% per year in %FVC predicted. A decline of more than 50 mL/year of FEV1 was observed in 10/17 (59%) patients (table 2, figure 6B). No patient showed a decline of more than 15% predicted per year in DLCO. Therapy with drugs was initiated in two patients with an inhaled steroid (one case) and long-acting β2 stimulants (one case).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serial changes of pulmonary function tests in patients with IDPO. The PFT data of 17 cases with IDPO were collected at two time points: at the diagnosis and latest follow-up. The changes in %FVC (A) and %FEV1 (B) predicted were plotted. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; IDPO, idiopathic dendriform pulmonary ossification; PFT, pulmonary function test.
Clinical course of physiological and radiological findings in IDPO
We compared the clinical factors at diagnosis between stable (FVC decline; <50 mL/year) and progressive (FVC decline ≥50 mL/year) groups to explore the predictive factors for disease progression (online supplemental table 5). Serum KL-6 level was significantly higher in the progressive group (mean (SD): stable, 227.4 (96.2) vs progressive, 479.4 (285.7); p<0.05). However, we could not detect any factors related to the progression of FEV1 (data not shown).
Discussion
In this study, we conducted a nationwide survey of IDPO to explore its clinical features and identified 22 cases in Japan. The physiological, radiological and histopathological examination revealed the unexplored phenotype of IDPO, which was preferentially observed in young males to be asymptomatic, but slowly and clearly progressive. In addition, we systematically evaluated the radiological and histopathological findings of IDPO.
Diffuse pulmonary ossification is a rare lung condition showing diffuse ossification in the lungs, even if the secondary cases were included. Several studies using autopsy data showed that the incidence of diffuse pulmonary ossification in all autopsies ranged from 0.16% to 0.4%.2 3 In addition, because most cases are secondary to underlying diseases,2 3 IDPO is believed to be extremely rare. In the present nationwide study, we identified 22 cases of IDPO and 30 cases of radiological IDPO in Japan. The data suggest that the prevalence of IDPO was at least 0.17 per million population. When we used the number of the radiological IDPO, the prevalence was found to be more than 0.24 per million population. On the other hand, a recent nationwide survey of pulmonary alveolar microlithiasis (PAM) in Japan showed that the prevalence was 0.06 per million population.31 These data suggest that IDPO has at least a 3–4 fold higher prevalence than PAM in Japan.
The average age of IDPO patients was 37.9 years in this study. An autopsy study reported that the median age was 70s.2 3 Other secondary cases of DPO were observed in patients in their 60s–80s.32 33 However, recent reports have shown that IDPO diagnosed by surgical lung biopsy was distributed among patients in their 20s–40s.16–18 25–29 In our study, the diagnosis was made in 5 patients in their 20s and 8 patients in their 30s. Most patients (77%) showed abnormalities on chest radiography at a workplace examination. These data suggest that the onset of IDPO may occur in patients in their 10s or 20s. In this study, two patients had familial IDPO. This fact, together with the report of other familial cases,10 strengthens the hypothesis for the aetiology related to a genetic disorder. At the time of diagnosis, IDPO was asymptomatic as reported, but showed a restrictive defect (%FVC predicted <80%) in 36%. In addition, impairment in %DLco predicted (<80%) was also found in 63% of patients. These data clearly suggest that IDPO lesions can cause lung dysfunction.
A systematic evaluation of HRCT and pathology in IDPO has not yet been attempted due to its rarity. This study clearly shows radiological characteristics specific to IDPO. We strictly excluded cases showing any underlying disease, clinically, radiologically and pathologically. Therefore, the specificity of IDPO seems to be high, and our cohort would be best to analyse the characteristics of definite IDPO. In fact, HRCT analysis demonstrated that calcified nodules with a calcified branching structure spreading until 30% of the lung fields was the only major finding in all HRCT data that we evaluated. Other findings showing interstitial pneumonia were absent or subtle (<10%) on HRCT, although mild fibrosis surrounding the ossified lesion was pathologically observed. The follow-up period in this study was up to 18 years. Therefore, we may understand that ossified lesions of IDPO are likely to be distributed in up to 30% of the lung area within approximately 20 years. The distribution of ossified nodules showed lower field predominance in 82% of the cases. Regarding the axial distribution, a diffuse pattern was predominant (70%), and there was no left/right difference.
We excluded only two cases in the final examination with histopathological findings of IDPO. In addition, HRCT findings in 30 cases of radiological IDPO were strongly similar to those of IDPO (22 cases). Because the HRCT findings of branching structures with or without calcification seem to be unique and specific for IDPO, it is likely to be diagnosed IDPO by clinical and HRCT findings without confirmation by histopathology, although further validation is required.
The histopathological findings were those of dendriform ossified lesions in all cases (dendriform or mixed (nodule and dendriform)), showing that ossification in IDPO was fundamentally dendriform. Ossifications existed across the intraluminal and interstitial areas. In addition, the analyses demonstrated that ossified lesions were distributed in the peribronchial, perivascular, interlobular and subpleural areas. This may suggest that the origin of the ossified lesions is not clear, but that the progression is directed not only into the alveolar space but also into interstitial areas. The detection of peribronchovascular distribution (22%) on HRCT may reflect the high frequency (56%) of the same distribution in histopathology. Further studies are required to elucidate the mechanisms involved in the formation and progression of DPO.
The other novel and critical findings are the clinical course of IDPO, which has been believed to be stable for a long time.24 34 This study demonstrated that IDPO is a slowly progressive disease that shows indisputable deterioration in HRCT and PFT over several years. Progression was observed in 88% of IDPOs on HRCT. An annual decline of 50 mL per year in FVC or FEV1 was found in 12/17 (71%) patients with IDPO. The FVC decline (5% of relative value per 2 years) compatible with the phenotype of patients with progressive fibrosing-ILDs (PF-ILD)30 was also observed in 5/17 (29%) patients. In fact, some IDPO patients were waiting for lung transplant (one in our study and one in the previous report).26 35 The analysis of a predictive factor for disease progression showed that the serum KL-6 level at diagnosis was higher in the progression group. Because KL-6 is known as a marker of interstitial pneumonias,22 disease progression in IDPO may be related to an increase in the number of ossified lesions as well as reactive fibrosis surrounding them, although remarkable findings at diagnosis were only ossified lesions.
However, all except two untraceable cases are still alive at the latest examination, whereas the time for follow-up was within 20 years. Regarding PAM which is a related disease to IDPO and causes respiratory failure, Tachibana et al reported the long-term (~49 years) follow-up was needed to identify the prognosis of PAM.36 To clarify the natural history of the clinical course of IDPO, long-term observational studies are required for more than 20 years.
There are several limitations to this study. First, the sample of 22 patients may be too small to conclude the clinical features of IDPO. Second, the follow-up period was too short to explore the natural history and prognosis of IDPO. Third, two evaluations of PFTs were not sufficient to show the true deterioration in %FVC and %FEV1 predicted, although the interval between the PFTs was at least 7 months or more. This study suggests that the onset of IDPO ranges from 10s to 20s. Notably, we did not encounter older patients with IDPO. This may be due to the strict exclusion of patients with any underlying disease. In general, the incidence of disease complications increases at middle to older ages. Therefore, it was difficult to distinguish whether IDPO developed other diseases at older age or secondary DPO. It is likely that this study excluded elderly IDPO cases during the screening, which could be another limitation of our study. In addition, we did not ask the occupational exposure in detail, and did not extensively investigate the biomarkers including autoimmune markers. Although IDPO cases were often reported from Japan, some has been diagnosed in other countries such as Canada,11 UK,14 China,16 Bahrain17 and USA,33 indicating that IDPO would be distributed worldwide.
In summary, we found the clinical, radiological and histopathological findings of IDPO by conducting a nationwide survey in Japan. The phenotype of IDPO was quite homogeneous, asymptomatically developed in young (male dominant) and slowly progressive, with frequently reported dysfunction data on PFTs. The calcified branching structure on HRCT and histopathological findings is a unique characteristic of IDPO. Serum KL-6 levels at diagnosis may be a predictive factor for disease progression. We should pay more attention to the possibility of IDPO, and a follow-up period of more than 20 years is needed to elucidate unsolved aspects such as prognosis.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional ethics committee of Tokushima University (approval No. 3084 and 3251), and then approved by each hospital. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YN and YT contributed equally.
Contributors YN provided initial ideas for the study. YN and YuT designed the study. YN, YaT, RE, TJ, YuT and AH designed the tables and figures, and wrote the first draft of the manuscript. YN and YaT performed the statistical analyses. YN, YoT, RE, TJ, YoT, AH, SH, KH, TS and NI interpreted the data. All authors contributed to the investigation and data collection and provided critical comments to correct and revise the manuscript. All authors have full access to all data and the final responsibility to submit for publication.
Funding This work was partly supported by a grant from the Ministry of Health, Labour and Welfare, the Study Group on Diffuse Pulmonary Disorders, Scientific Research/Research on Intractable Diseases in Japan.
Competing interests YI is a consultant and steering committee member to Boehringer Ingelheim, Roche, Taiho, and Savara, and has a lecture fee from Boehringer Ingelheim, Shionogi, Kyorin and Thermo Fisher.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.