Article Text

Abstract
Introduction Deliberate exposure to medical ionising radiation should be as low as reasonably practicable but the reduction of radiation from CT should be balanced against diagnostic image quality. The ability of ultra-low-dose CT (uLDCT: similar radiation to chest X-ray) to demonstrate low contrast abnormalities (emphysema and interstitial lung abnormality (ILA)) is unclear.
The aim of this cross-sectional study was to analyse the lung parenchymal findings from uLDCT scans against physiological measures of respiratory function.
Methods WA Asbestos Review Programme participants were eligible if they had an uLDCT scan and lung function assessment between Janary and December 2018. All scans were performed using a single CT machine and reported using a standardised, semiquantitative synoptic report which includes emphysema and linear fibrosis (ILA) scores.
Results Of 1344 participants, median (IQR) age was 72.0 (65.0–78.0) years, the majority were males (84.9%) with mixed occupational asbestos exposure (68.1%). There were 721 (53.6%) with no abnormality, 158 (11.8%) with emphysema, 465 (34.6%) with ILA. Mean radiation dose was 0.12 mSv. There was statistically significant between group differences for all physiological parameters of lung function compared with controls. For instance, the emphysema score significantly correlated with obstructive forced expiratory volume in 1 s (FEV1)/forced vital capacity ratio (r=0.512), per cent predicted FEV1 (r=0.24) and lower diffusion of carbon monoxide (DLCO) (r=0.337). Multivariate modelling demonstrated that increasing age, emphysema and fibrosis scores predicted reduced DLCO (adjusted R2=0.30).
Discussion uLDCT-detected parenchymal lung abnormalities correlate strongly with significant changes on lung function testing suggesting the observed CT abnormalities are of physiological and clinical significance.
- imaging/CT MRI etc
- lung physiology
- emphysema
- occupational lung disease
Data availability statement
Data are available on reasonable request. Individual participant data that underlies the results in the article may be made available after deidentification to any investigator whose proposal has been approved by an independent review committee for this purpose.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Ultra-low-dose CT (uLDCT) delivers a radiation dose similar to chest X-ray (CXR) but the ability to reliably detect low contrast lung parenchymal abnormalities is unclear.
WHAT THIS STUDY ADDS
uLDCT can detect low contrast pulmonary abnormalities that correlate with physiologically significant pulmonary function abnormalities. uLDCT is likely appreciably more sensitive than CXR for detection of parenchymal lung abnormality for a similar radiation dose.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
For some conditions, a transition away from the ‘routine CXR’ towards uLDCT may be indicated.
Introduction
Deliberate exposure to medical sources of ionising radiation should be as low as reasonably practicable due to the risk of inducing cancer.1 A plain chest X-ray (CXR) is the most common imaging study requested by clinicians although a standard dose CT (SDCT) of the chest is substantially more accurate than the CXR for identifying almost all lung abnormalities, in particular recognition of parenchymal lung diseases such as emphysema and interstitial lung abnormalities (ILA).2 3 However, this entails a radiation dose typically around 20 times that of a two-view (posterior–anterior and lateral) CXR series, thereby theoretically resulting in 20 times the increased risk of a radiation-induced cancer.4
Any efforts to reduce effective radiation dose from CT scans should be balanced against the requirement for adequate diagnostic image quality. Put simply, the lower the radiation dose, the lower the signal-to-noise ratio and therefore, the lower the image quality. However, recent advances in CT machine hardware and image processing software have permitted dramatic radiation dose reductions with minimal loss of image quality, particularly on the high-end CT machines.5 6 High-contrast abnormalities like consolidation and lung nodules can be accurately diagnosed by both radiologists and computer aided detection using ultra-low-dose CT (uLDCT) with a low radiation dose of <0.2 mSv.7–9 Small studies have demonstrated that use of uLDCT can result in an 84% dose reduction compared with SDCT, but with a slight underestimation of emphysema quantification,10 which is improved by the use of image reconstruction.11 12 There is no evidence correlating low contrast abnormalities such as emphysema and ILA observed on uLDCT with measures of physiological function, presenting a knowledge gap.
With increasing implementation worldwide of screening for early lung cancer using low-dose CT of the thorax (LDCT: usually 1.0 mSv-1.5 mSv effective dose), the need to ensure that exposure to ionising radiation is as low as reasonably practicable has increased importance given that a lung cancer screening programme may entail a 25-year screening period of individuals already at raised risk of malignancy.13 This assumes greater significance with occupationally exposed cohorts where the majority of individuals have had exposure to at least two carcinogens (eg, asbestos and tobacco smoke),14 highlighting the need to mitigate future carcinogen exposure in individuals already at high risk of cancer(s).
Early recognition and diagnosis of emphysema and ILA has important health implications for individuals and, further, the presence of emphysema or fibrosis independently raises an individual’s risk of lung cancer.15 16 This may present with a mixed deficit on lung function and rapid symptom progression, and is an increased risk for lung cancer. Reliable recognition of parenchymal abnormalities using an investigation with a high sensitivity and as low a radiation dose as achievable, as part of general respiratory investigations or in a lung cancer screening population, is thus highly desirable. A CXR series is not sensitive enough for subtle parenchymal lung disease.17
The Western Australia Asbestos Review Programme (ARP) has been studying asbestos-exposed individuals since 1990. In 2012, LDCT was adopted in preference to CXR as part of the annual review and since this time the programme has implemented uLDCT chest scans. The aim of this study was to analyse the lung parenchymal findings from the uLDCT scans against physiological measures of respiratory function to establish how reliably chest CT at ultra-low doses can demonstrate parenchymal pathology.
Methods
Study design
The establishment and history of the ARP has been described in detail previously.18 19 Briefly, participants are required to have ≥3 months cumulative asbestos exposure history and/or the presence of pleural plaques on imaging to be eligible. Originally, the cohort was established to monitor the health of crocidolite (blue asbestos) workers from the Wittenoom mine (Pilbara, Western Australia) and local Wittenoom township residents; the majority of the ARP is now composed of a mixed-occupation cohort, with mixed-fibre asbestos exposures.
The ARP annual health assessment includes health and lifestyle questionnaires, lung function, blood tests and radiographic imaging.18 20 Postbronchodilator forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and diffusion of carbon monoxide (DLCO: ‘gas transfer’) were performed in accordance with the ATS/ERS recommendations and Global Lung Initiative reference values.21 22 Tobacco smoking history including duration and pack-year exposure was recorded from a standard questionnaire administered at enrolment and updated at each annual visit.
Subjects
ARP participants were eligible for this cross-sectional study if they had an annual review between 1 January 2018 and 31 December 2018. All subjects must have had an uLDCT screening scan and lung function assessment, usually performed within 1–2 days of each other.
Protocol for LDCT screening scans
All CT scans were performed prone at 1.5 mm slice thickness using a Siemens SOMATOM Definition FORCE machine (Siemens Healthcare, Munich, Germany), including spectral shaping of the X-ray beam with a tin filter (facilitates a ~20%–30% reduction in radiation dose due to its effect eliminating radiation energies at the extremes of the spectrum which do not contribute to image quality), ultra-sensitive exotic compound detector material (Stellar Detector) and level 3 generation denoising interactive reconstruction software (‘ADMIRE’). The scan factors were a patient size-dependent tube voltage of 100–120 kVp and tube current-time product of 20–40 mAs. Estimated radiation exposure was measured using the dose-length product and used a conversion ‘k’ factor of 0.014 to estimate millisieverts (mSv).23
All LDCT scans were routinely reported by one of three specialist thoracic radiologists blinded to exposure history, using a standardised, semiquantitative synoptic report which was adapted from the Kusaka International Classification of HRCT for Occupational and Environmental Respiratory Diseases (ICOERD: analogous to the International Labour Organisation classification of respiratory disease).24 This system provides a score depending on the features or severity for different abnormalities, for instance, presence of nodules, pleural plaque, emphysema, linear opacities (which represent fibrosis) and honeycombing.
The ICOERD system divides the lung fields into three zones (upper, mid, lower) and severity of emphysema and fibrosis is classified within each zone, on a scale of zero (none) to with a maximum score of 3 (marked abnormality), giving a maximum score of 18 for both lungs. The magnitude of ILA is assessed by the parameter, ‘linear opacity score’, with a score ≥1 considered positive for the presence of ILA (or possible fibrosis).25 Similarly, an ‘emphysema sum score’ ≥1 was considered diagnostic of emphysema; subjects with normal parenchyma scores were regarded as a comparator group.
Quantitative asbestos exposure estimates
Mixed occupational exposure: A validated Australian-specific asbestos job-exposure matrix, which estimates asbestos exposures for 224 occupations in 60 industries over four time periods between 1943 and 200326 27 was used to estimate the cumulative asbestos exposure for individuals based on detailed job histories obtained from all participants. Wittenoom exposure: Between 1948 and 1966, periodic measurements of airborne dust concentrations were taken from the mine, mill and township and cumulative exposure was calculated, as described previously.28
Patient and public involvement
Consumer representation influenced the concept and planning for this project as part of the National Centre for Asbestos Related Diseases consumer engagement process.
Statistical analysis
Descriptive analysis was performed on the continuous variables of interest and frequencies were assessed for the dichotomised variables. In order to maximise numbers of cases, all cases of emphysema and fibrosis were analysed, that is, not excluding those with combined disease within each cohort. Wilcoxon signed-rank test was performed on non-normally distributed data to analyse for significant differences between the two scans and paired t-test was performed on normally distributed data. Pearson’s correlation was tested between the variables, linear sum (fibrosis) scores vs total asbestos exposure, as well as between dichotomised variables of fibrosis and emphysema vs FEV1, FVC, FEV1/FVC ratio and DLCO. Multiple regression analysis was carried out to examine the effect of the independent variables age, smoking, asbestos exposure, fibrosis scores and emphysema scores, on the dependent variable DLCO. Statistical significance was accepted with a p<0.05. Data were analysed using SPSS Statistics, V.24 (SPSS).
Results
A total of 1344 participants were identified with paired uLDCT and lung function, table 1 presents the baseline data. Median (IQR) age was 72.0 (65.0–78.0) and as expected, there was a male predominance (1141, 84.9%) with the majority reporting mixed occupational, mixed asbestos fibre exposure (915, 68.1%). Just under two-thirds of the cohort (876, 65.2%) reported ever-smoking with a modest median tobacco exposure of 19.5 (IQR 8.4–39.0) pack-years. For the whole cohort, mean (SD) FEV1 was 91.3% (18.8) predicted, FVC 96.7% (17.1), FEV1/FVC ratio 0.71 (0.09) and actual DLCO 23.3 (7.3) mL/min/mm Hg.
Demographics and baseline data
There were 721 (53.6%) subjects with no CT parenchymal abnormality, 158 (11.8%) with emphysema, 465 (34.6%) with linear fibrosis and 94 (7.0%) noted to have both fibrosis and emphysema. The demographic characteristics of the normal parenchyma group and subjects with emphysema or fibrosis are presented in table 1. Subjects with emphysema were older, had more ever and current smokers and a greater tobacco exposure compared with those with no abnormality. Subjects with fibrosis were older and the cumulative asbestos exposure was not statistically different to controls (p=0.959).
Radiological findings
Mean dose length product was 8.9 (SD 1.9) mGy/cm or 0.12 (SD 0.03) mSv. Pleural plaque was present in 802 (59.7%), subpleural linear opacities in 559 (41.6%) and honeycombing in 33 (2.5%). Median (IQR) emphysema score 4.0 (2.0–8.0) and linear fibrosis score was 4.0 (2.0–6.0). A total of 220 indeterminate nodules were recorded (137 ground glass). Examples of the CT scans are presented in figure 1. There were four confirmed cases of lung cancer and no cases of mesothelioma.
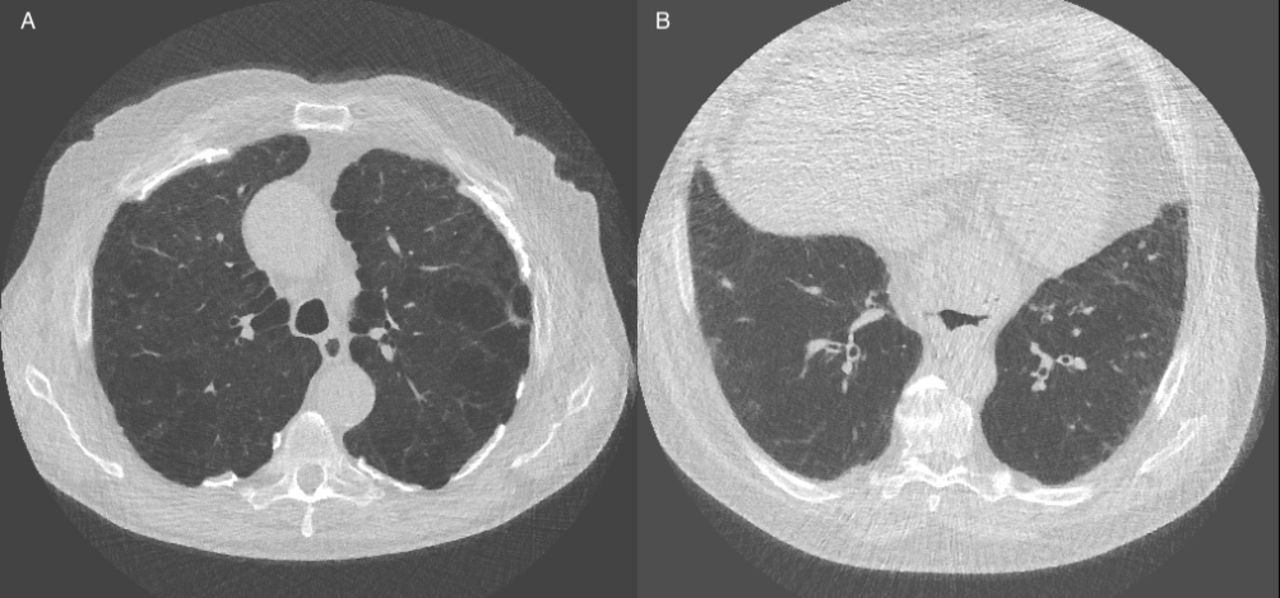
(A) 1.5 mm thick axial image on lung algorithm of an 80-year-old man from a CT scan performed at a radiation dose of 0.12 mSv. Both high and low attenuation abnormalities are well seen with severe emphysema and bilateral calcified asbestos related pleural plaque. (B) 1.5 mm thick axial image on lung algorithm of a 78-year-old man from a CT scan performed at a radiation dose of 0.13 mSv demonstrating mild bilateral subpleural basal linear (fibrotic) opacities.
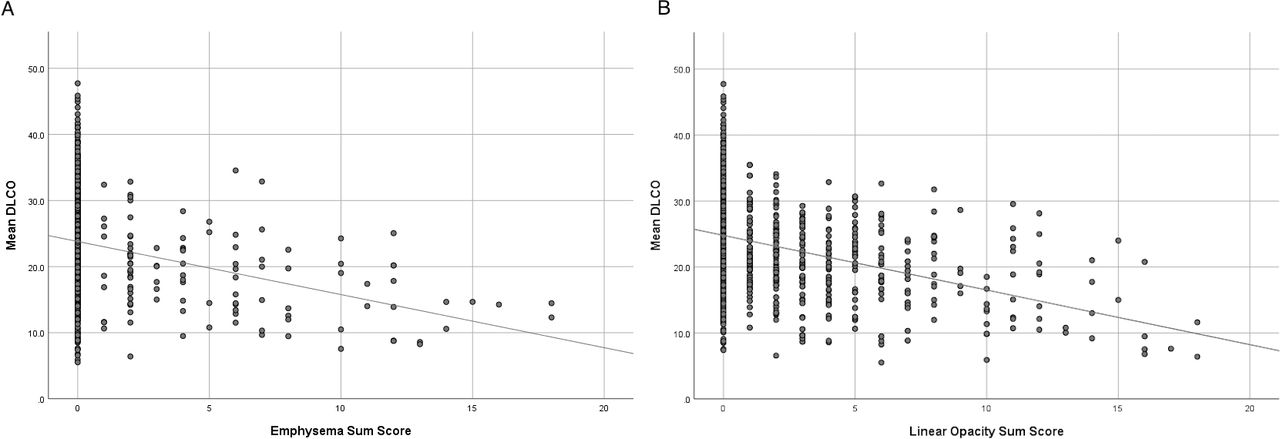
Table 2 presents the lung function data stratified by the radiological presence of emphysema and fibrosis. There was statistically significant between group differences for all physiological parameters compared with controls. The total emphysema score and obstructive FEV1/FVC ratio had a strong and significant correlation (r=0.512, p<0.0005), there was a moderate inverse correlation with per cent predicted FEV1 (r=0.24, p<0.0005) and a weak correlation with per cent predicted FVC (r=0.19, p=0.02). The linear fibrosis score correlated moderately well with per cent predicted FEV1 (r=0.21, p<0.0005) and per cent predicted FVC (r=0.21, p<0.0005), but weakly with FEV1/FVC ratio (r=0.095, p=0.001). There was a moderate correlation between emphysema score and lower DLCO (r=0.337) and linear fibrosis score and lower DLCO (r=0.362), both p<0.0005 (see figure 2).

{kind=link}
{kind=link}
Scatterplot and line of best fit comparing (A) emphysema sum score and DLCO (r=0.337; p<0.0005) and (B) linear opacity (fibrosis) sum score and DLCO (r=0.362; p<0.0005). DLCO, diffusion of carbon monoxide.
Lung function variables stratified by the presence of emphysema, fibrosis (mean, SD)
Multivariate analyses
Table 3 summarises the contribution to the multivariate model by the variables demonstrating that increasing age (as expected), emphysema and fibrosis scores predicted reduced DLCO (p<0.0005, adjusted R2=0.30).
Multiple regression results for gas transfer (DLCO)
Discussion
This large unique dataset demonstrates clearly that parenchymal abnormalities observed on uLDCT using prone images have a strong association with physiologically significant abnormalities in lung function. To our knowledge, this is the largest study to demonstrate the utility of uLDCT for low contrast parenchymal pathologies such as emphysema and fibrosis at a similar radiation dose to a CXR series. These findings complement previous observations on other asbestos exposed populations at higher radiation doses than this study.2 29–31
There has been previous concern that uLDCT had limitations with regard to identification of low-contrast pathologies such as emphysema and interstitial abnormalities compared with SDCT.32 A recent randomised trial of uLDCT versus CXR in the emergency department setting demonstrated that CT detected more (high and low contrast) lung abnormalities, but did not have an impact on short-term functional health measures at 28 days after admission.7 Given that previous studies have demonstrated that CXR has a low sensitivity for early physiological changes,17 30 our outpatient, community-based data suggest that prone uLDCT is likely a more accurate investigation for recognition of parenchymal abnormalities than CXR, at a comparable radiation dose. Therefore, there may be a role for uLDCT replacing the routine use of CXR for more general non-specific respiratory indications and perhaps longitudinal observation of abnormalities that are likely to be more accurately demonstrated on CT imaging. Cost and accessibility to the technology will present an issue in some countries and jurisdictions. uLDCT is unlikely to become a substitute for SDCT, as SDCT will still offer the best sensitivity for subtle parenchymal lung diseases.
Advances in CT machine hardware and image processing software have improved the capacity of uLDCT for identification of lower contrast pathologies, despite an increased signal-to-noise ratio. This is reflected in this study, which has demonstrated a strong association with the presence of low contrast abnormalities such as emphysema with a lower percentage predicted FEV1, obstructive FEV1/FVC ratio and lower DLCO (indicating alveolar unit loss). Similarly, an increasing fibrosis score was associated with a lower FVC, more restrictive FEV1/FVC ratio and lower DLCO. Subjects with both fibrosis and emphysema also had significant mixed physiological changes, as expected. There was a significant correlation between declining DLCO and increasing imaging-based emphysema and fibrosis scores, and multiple regression analysis also demonstrated that higher emphysema and fibrosis scores both independently predicted a lower DLCO. Overall, these data clearly demonstrate that uLDCT-detected parenchymal abnormalities are associated with clinically significant physiological changes in lung function. The combination of uLDCT with simple lung function tests will allow an early diagnosis of emphysema and fibrosis with clear clinical importance for both conditions.33–35
The ARP uLDCT project has been developed primarily for early lung cancer detection, and gold-standard approaches such as using two readers and formal consensus methods have, therefore, not been used, and this is acknowledged as a limitation of this study. However, the interstitial abnormality observed in the ARP cohort is likely to represent stable asbestosis with a previous longitudinal analysis over 5 years demonstrating radiological and physiological stability.36 The same report demonstrated a high Cohen’s kappa for presence of ILA varying between 0.91 and 0.95 across the three reporting radiologists, indicating very good agreement and indicating the likely reliability of the measurements for this study. Regarding generalisability, the ARP population represents predominantly an ageing blue collar workforce cohort with a comparable tobacco smoke exposure to populations of a similar age. The previous exposure to asbestos in this cohort will have raised the prevalence of ILA more than other populations,15 37 increasing the statistical power for more reliable identification.
This pragmatic study has not compared uLDCT with SDCT images as a ‘gold standard’ for radiological diagnosis, nor have the uLDCT images been compared with CXR, another limitation of the study. Instead, physiological markers of lung function including gas transfer, a highly sensitive marker of alveolar unit loss, have been used as corelates of pathology. In doing so, this study has demonstrated that uLDCT can reliably identify physiologically significant parenchymal lung abnormalities with a total radiation exposure similar to a CXR series and an order of magnitude lower than SDCT.
In conclusion, this study has shown in a large cohort that uLDCT-detected parenchymal lung abnormalities correlate strongly with physiologically significant changes on lung function testing. These data add to the expanding literature demonstrating the utility of uLDCT, now for the reliable diagnosis of low contrast lung pathology. We contend that a transition away from the ‘routine CXR’ towards uLDCT may be indicated.
Data availability statement
Data are available on reasonable request. Individual participant data that underlies the results in the article may be made available after deidentification to any investigator whose proposal has been approved by an independent review committee for this purpose.
Ethics statements
Patient consent for publication
Ethics approval
Research ethics committee approval was obtained from the University of Western Australia Health Research Ethics Committee reference RA/4/1/2119 and all subjects provided written informed consent. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Deceased BM deceased.
Contributors FB study concept and design, data analysis, manuscript writing, guarantor of integrity of the study, EJAH study concept, data analysis. CK data analysis, manuscript writing. AR data analysis. BA and CM data collection. PF, NdK and BM study design, guarantors of integrity of the study.
Funding National Health and Medical Research Council; Charlies Foundation for Research; the Western Australian Department of Heath support the clinical investigations of ARP.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.