Article Text

Abstract
Background Cystic fibrosis (CF) is a genetic condition caused by variants in the cystic fibrosis transmembrane conductance regulator (CFTR) gene that primarily impacts the lungs. Treatments historically have been symptomatic to improve airway clearance and treat infection. However, CFTR modulator drugs have recently been developed that target the underlying defect. The triple combination of elexacaftor-tezacaftor-ivacaftor (ETI) was approved in 2020 in England for over 80% of people with CF aged over 12 years and in 2022 extended to those over 6 years. ETI treatment is associated with substantial improvements in lung function. The experience of children with CF starting on ETI or their views regarding future treatments have not been well studied. This study aimed to explore the opinions of children with CF, their parents/carers and healthcare professionals (HCPs) on the impact of ETI, airway clearance techniques (ACTs) and nebulised treatments.
Methods Semistructured qualitative interviews were performed with 10 children with CF, 7 parents/carers and 10 HCPs. Audio recordings were transcribed and analysed using reflexive thematic analysis.
Results Four main themes were identified: ‘Kaftrio changed my life’, ‘Your entire life is dictated by the CF timetable’, ‘Simplifying treatment-hopes and fears’ and ‘Kaftrio is a game-changer’ along with several subthemes and an overarching theme of ‘I still can’t get my head around how three tablets can do what Kaftrio done’.
Conclusions Despite the highly positive impact of ETI on the health of children with CF some concerns remain about the longer-term outcomes of reducing ACTs or nebulised treatments. ETI has prompted a shift in treatment for many and offers an opportunity to personalise approaches.
- Cystic Fibrosis
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Not applicable - is a qualitative study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Elexacaftor-tezacaftor-ivacaftor (ETI) treatment is associated with substantial improvements in lung function and other clinically important parameters in randomised clinical trials in people with cystic fibrosis (CF) and at least one F508del variant.
Simplifying treatment burden is a top priority for people with CF.
Airway clearance techniques (ACTs) and nebulised therapy are considered the most burdensome aspects of treatment.
What this study adds
The study has elucidated opinions regarding ACTs and nebulisers of children with CF prescribed ETI, their carers and healthcare professionals (HCPs) with four main themes identified.
Overall experiences have been positive and children wish to reduce or stop ACTs and nebulised treatment as soon as possible.
Carers and HCPs, however, expressed concerns about current lack of evidence to support simplifying treatment.
How this study might affect research, practice or policy
The shifts in treatment in children with CF prescribed ETI offers an opportunity to personalise approaches to ACTs and nebulised treatments.
It remains important that the longer-term effects of ETI are studied along with research into the optimal approaches to simplify ACTs and nebulised treatment.
Introduction
Cystic fibrosis (CF) is a multi-system, life-limiting genetic disorder caused by dysfunction of the CF transmembrane conductance regulator (CFTR) protein.1 CF primarily affects the lungs where reduced chloride and bicarbonate secretion cause abnormal airway surface liquid homeostasis.2 Hydration and clearance of mucus is impaired with infection and inflammation causing progressive bronchiectasis.
Treatments available have historically targeted downstream problems, such as airway clearance techniques (ACTs) and nebulised mucolytics to improve airway clearance and antibiotics to prevent or treat infection. These treatments are required two times per day and are part of a time-consuming regime. Children frequently report feeling overwhelmed by treatment as they grow older and that it impacts on their life and opportunities.3 4 A James Lind Alliance priority setting partnership identified simplifying treatment as the top research priority in CF.5 ACTs and nebulised treatment are rated as the most burdensome for people with CF.6
The development of CFTR modulators has heralded a new era of precision medicine in CF. These small molecule drugs target the underlying defect and improve CFTR function.7 Depending on the functional class of CFTR variant either a potentiator or combination of potentiator and correctors are prescribed. Potentiators increase the amount of time that the CFTR channel is open and improve gating defects. Correctors improve the trafficking of CFTR to the cell membrane when there is a problem with misfolding of the protein causing it to be degraded intracellularly.7 Over 80% of cwCF in the UK have at least one copy of the F508del variant where a combination of correctors and potentiator is used to firstly transport the F508del CFTR protein to the membrane and then increase the amount of time the channel is open.8 In this population the triple combination of elexacaftor-tezacaftor-ivacaftor (ETI), Kaftrio, has been demonstrated to substantially improve lung function, increase time to next pulmonary exacerbation and improve weight and quality of life in well-conducted randomised trials.9–12
ETI, along with ivacaftor, potentiator monotherapy that has been available since 2012 for 5% of the CF population with gating defects, is often referred to as ‘highly effective modulator therapy’ (HEMT). In August 2020 ETI was approved for patients over the age of 12 years in England and most recently, in January 2022, for those over 6 years of age.
Due to this step-change improvement in treatment outcomes the continued need for ACTs and nebulised mucolytics or antibiotics has been questioned. Surveys of people with CF in the HEMT-era have confirmed that reducing treatment burden is a priority13 and that ACTs and nebulised antibiotics are the treatments they wish to simplify the most.14 Lived experience pre-ETI was described as challenging by many with individuals striving for equality and expressing a wish to be able to access the same opportunities as healthy people.3 The feasibility of replacing ACTs with exercise has also been identified as one of the CF community’s top 10 research questions.5 A survey of healthcare professionals (HCPs) involved in CF care found that the majority supported the idea of a trial of replacing ACTs with exercise.15 Another study in Australia found that 43% of adults with CF believed exercise could substitute ACTs, with 44% having done so in the previous 3 months.16
While the clinical trial evidence of benefit with ETI is impressive, there is little work published that explores the lived experience of cwCF or the opinions of families and HCPs. This study aimed to understand the impact of ETI on the lives of cwCF and their attitudes towards ACTs and nebulised treatments. The opinions of multidisciplinary HCPs were also explored around implications for future clinical practice.
Methods
Participants and recruitment
Participants were recruited from a regional paediatric CF service in Northeast England. Three groups took part following informed written consent:
CwCF (aged 12–18 years) prescribed ETI at least 6 months, ACTs and nebulised mucolytics or antibiotics, purposively sampled to give maximal variation.
Parents or guardians of children in group 1.
HCPs from the CF multidisciplinary team, purposively sampled to give a range of disciplines.
Recruitment continued until data saturation occurred. In total, 27 participants took part (10 cwCF, 7 parents and 10 HCPs), characteristics are summarised in table 1. Median age of cwCF was 15 years (range 13–16).
Characteristics of participants
Qualitative interviews
Semistructured interviews were performed via video call for groups 1 and 2 and in person with HCPs between January and May 2022. Virtual interviews were chosen as advised by the ethics committee which approved the study due to the concurrent COVID-19 pandemic. The mean duration of interviews was 30 min. An interview topic guideline (online supplemental material) was developed to facilitate participant-led discussions. The first part of the interview asked about treatment routine pre-ETI and how they felt about it. The next part of the interview was related to the impact of ETI. This started by asking about any positive or negative impact on their everyday lives and then moved on to specific aspects such as treatment routine, social life and any concerns relating to it. Starting with the time before ETI allowed participants to compare the changes in their CF and treatment. The next section involved questions relating to their thoughts about simplifying ACT and nebulised therapy after ETI. The last section was about future research questions that participants would like studies to address. Finally, there was a discussion around a summary of the interview’s main themes and participants were given a chance to make any additional comments, mention any issues or other information. The interview consisted of open-ended questions with follow-up questions to allow participants to expand on their responses. Interviews were recorded and then transcribed anonymously by a professional transcriber verbatim.
Supplemental material
Data analysis
NVIVO (QSR International) software was used for coding and data management. Data were analysed using inductive thematic analysis, emphasising broad thematic patterns across the data and identifying semantic meanings. The six phases are well-defined yet iterative; the reflexive feature of this approach to thematic analysis requires continual movements between the phases with an attitude of inquiry and interpretation.17 Briefly, these included initial reading and familiarisation of the transcripts, coding and identification of candidate themes, followed by checking that themes reflected the entire dataset. Finally, themes were named and the story behind them considered before writing up the analysis. Codes and themes were discussed with the research team to ensure accurate reflection of the data. Each group of participants’ data were analysed individually and then compared with each other.
Patient and public involvement
This qualitative study focused on the opinions of patients and their families. There was no direct involvement of patients in the design of the study.
Results
Multiple insights were provided about the impact of ETI along with personal anecdotes and opinions. Commonalities in experience and some dissimilarities were identified. We described an overarching theme with four associated and interconnected themes, summarised in figure 1 that encapsulated the perspectives of all participants.
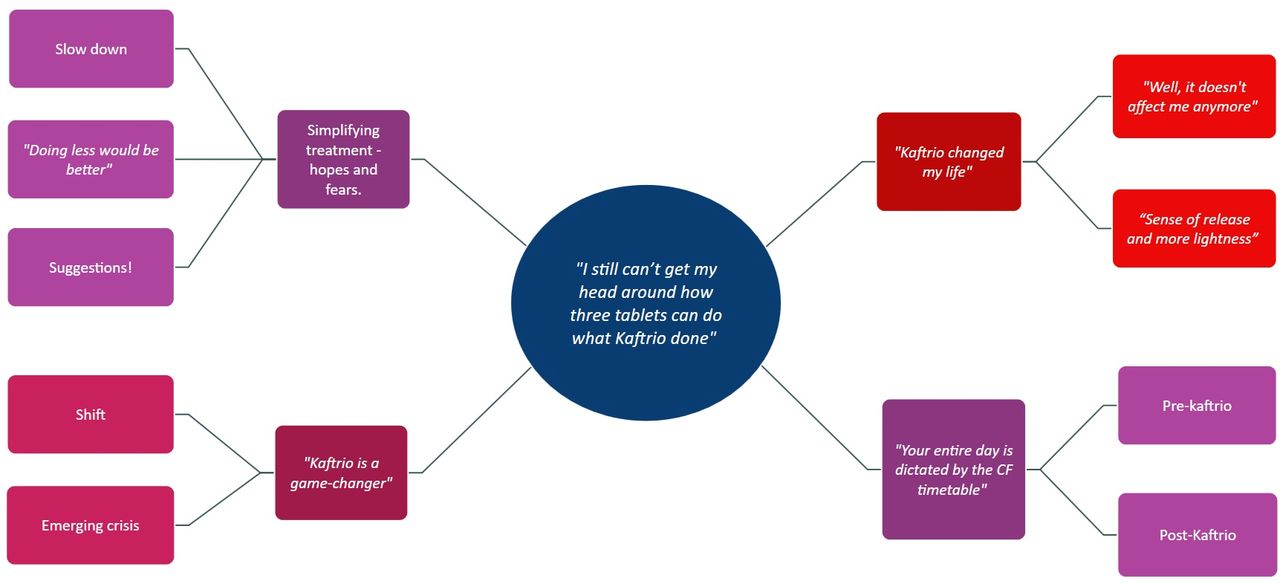
{kind=link}
Schematic summary of themes and subthemes. CF, cystic fibrosis.
Overarching theme: ‘I still can’t get my head around how three tablets can do what Kaftrio done’ (Helen, mother of a cwCF aged 12–15 years)
This quote from a parent illustrates the huge impact ETI has had and summarises the overall experience. Substantial improvements in physical health have led to wider benefits in terms of mental well-being and extended social lives and opportunities for cwCF. The introduction of ETI has also changed approaches to multidisciplinary care that are ongoing. The four associated themes are described below in the context of cwCF, their families and HCPs.
Theme 1: ‘Kaftrio changed my life’ (Elizabeth, cwCF aged 12–15 years)
Most participants emphasised the changes in their lifestyle after starting ETI and they compared this with the time before they were taking it. Two subthemes captured these changes.
Subtheme 1.1: ‘Well, it doesn’t affect me anymore’ (Arthur, cwCF aged 12–15 years)
As this young man indicated when asked about the difference he experienced after ETI, he described how the symptoms he had experienced had disappeared. He felt that CF does not affect his health any longer. The majority of cwCF interviewed felt that their respiratory symptoms, such as cough and shortness of breath, had reduced and that their lung function had improved. For example, Anna (cwCF aged 12–15 years) said: ‘I would say that it has made my lungs feel better. It’s been less coughing overnight, which I appreciate … and less mucus which I appreciate’. Being more active and awake, having more energy, not being tired and sleeping well were all frequently described. Maggie (cwCF aged 16–18 years) spoke about her health after ETI:
I’d say a bit because it’s made me a lot better, more awake … I was really tired before and I’d have like nine hours of sleep and still be tired and just like I need another nap. Now it’s like I can wake up and just have a day and then sleep at the end instead of needing breaks during the day. Which is nice.
Subtheme 1.2: ‘Sense of release and more lightness’ (Helen, mother of a cwCF aged 12–15 years)
This subtheme focused on the psychological impact reported by children and their families. Many participants reported a positive change in their outlook towards their lives. Several children relayed how as long as they could remember they had experienced symptoms and that now they felt incredibly well comparatively. This healthy feeling meant for the first time they looked optimistically to the future. Rose (cwCF aged 16–18 years) talked about her feelings before and after ETI:
for such a very, very long time CF felt like a really untreatable thing, and everything you’re doing feels like you’re just trying to prolong something that- Like prolong a life that might not be as high a quality as a lot of people’s. But the Kaftrio has really been the first proper step towards an effective treatment, that actually does something more than necessarily prolonging … you feel more like other people and you feel more like you are healthy, even if you aren’t necessarily better properly.
Several parents also reported the positive impact of ETI on the quality of life of their child. Parenting an older cwCF can be challenging and arguments about taking of medication and doing ACTs frequent issues. Many parents have previously spent a huge amount of time caring for their children only to see them struggling as they got older due to increasing symptoms compounded by the stress of an ever-increasing treatment burden. After starting ETI their child was now much better than previously. A common emotion among parents was relief once they had confidence that ETI was working and was going to benefit their child. The following quote from Peter (father of a cwCF aged 12–15 years) illustrates the impact on their mental health of their child’s health improving with ETI:
even though [cwCF] was really well before and the health improvements that we’ve seen are probably minor compared to some of the improvements that other families have seen, it’s still an emotional safety net that has made us think, ‘Well, any issues that we probably were going to run into are going to be either milder or non-existent in the future’. It is a miracle drug.
Some cwCF expressed disappointment and frustration that they had not experienced as much benefit as some other people had. Several children had compared results with others who shared experiences on social media. For example, Ruby (cwCF aged 12–15 years) talked about her lung function and how she felt about not seeing the huge impact that she had been expecting
I don’t think there has been a huge impact. It’s probably in the 80s now, which is still good. It’s really good, but the difference, probably. I know some people who—well, I don’t say I know, I mean like on social media and stuff—that has gone from 30 to 90, like it has been incredible. Yes. I haven’t seen a huge impact from the lung function side … I think there are people who it has impacted their life and made a huge difference, and I think that’s amazing for them. For me, personally, yes, sports, for example, amazing. But apart from that, I haven’t really seen a huge impact. My doctors might say otherwise, but me personally, I think it has not really done that much.
The first theme, ‘Kaftrio changed my life’, highlights the physical and mental improvement reported by cwCF and their families and its influence on their day to day lives. The next theme that developed from the analysis related to treatment burden.
Theme 2: ‘Your entire life is dictated by the CF timetable’ (Martha, mother of cwCF aged 12–15 years)
This theme revealed the burden of treatment and the impact on their life before and after ETI. As patients get older this typically involves the addition of more treatments to daily routine. As CF care has advanced over the decades developments have typically involved an increase in treatment burden. The introduction of ETI is different and may actually be associated with a reduction in treatment.
Subtheme 2.1: before ETI
Most children started ACTs from an early age and maintained that routine throughout their lives. This schedule places a constant demand on families. Children felt that their lives were limited by the treatment. Although they understood the importance of ACTs and nebulisers in their care, they were often seen as a tedious process. This regime was also a constant reminder that they have CF making them feel different. Talking about this issue Anna (cwCF aged 12–15 years) said: ‘it can be a bit annoying. You know, in your daily routine it takes time to just organise your life around that, I suppose. It can be time-consuming every now and then, but apart from that, it’s good for my health’.
Commenting on the burden on parents or carers, Olivia (mother of a cwCF aged 12–15 years) emphasised the struggle with motivating their children to do their daily treatment saying:
that responsibility of having to get everything done all the time. Just, yes, how did we feel? (Laughter) Well, Dad used to be stressed because it was just the constant- With the Aerobika or whatever, to saying, ‘Blow’, ‘Blow’, ‘Count’, ‘Concentrate’, or with nebulisers, ‘Are you holding that properly?’, ‘Are you sucking it up?’, ‘Are you doing this?’, and it is the constant nudging to make sure that it is done in the right way.
A small number reported they were resigned to their daily routine. They believed that acceptance was the best way to manage the treatment around their lives. As Martha (mother of a cwCF aged 12–15 years) put it: ‘We sort of didn’t make it a big deal. You’ve got it, there’s nothing we can do about it, so you’ve just got to manage the treatments. You’ve got to do them, but try and do them in a way that doesn’t monopolise all of your day’.
Subtheme 2.2: after ETI
Most participants felt treatment burden had diminished since starting ETI. Some cwCF stated that it was now easier to manage their treatment without it having an impact on their day. Going to school had become easier without needing to wake up early to complete physio. Children were also now able to engage in more social activities. Elisa (cwCF aged 16–18 years) stated that:
When I was doing it twice a day it was quite a lot, because I’d have to be waking up. The whole set would take me about an hour, so I would have to wake up an hour earlier before school. Then when I got home it meant that if I wanted to go stay over at somebody’s or was busy, it was quite difficult to fit it in. I’d have to know before the morning to pack everything to go to someone’s.
Sonny (cwCF aged 12–15 years) commented: ‘I remember when I first started school again after it, I found it ridiculous how fast you can get ready in the morning without it. It took maybe 10, 20 minutes, just to do everything without tons of the stuff in the way’.
Even the children whose treatment routine had not changed felt that it was easier to complete now because they have more energy. There was also evidence of less tension among family members about managing treatment and trying to get everything done. The time that was now freed up was regarded as a welcome bonus and allowed them to enjoy more quality family time as expressed by Helen (mother of a cwCF aged 12–15 years) who said:
I mean, it has completely changed, like, the social side of the family. Because there aren’t the little niggles and the tensions in the way that there used to be, to try and get everything done within the timeframe. We’re a lot more relaxed, now, about things. And it seems like so much more manageable.
In another example, Peter (father of a cwCF aged 12–15 years) described how the daily stress had been taken away from his family allowing them to enjoy more quality family time: ‘Any pressure that’s taken off them in that way I think would be a massive improvement …. I think that would probably pay off for the change in quality of life that it would bring’.
In this theme, cwCF and their families emphasised the impact of treatment burden and compared it before starting on ETI with how it feels now. The reduction in treatment load had improved quality of life for many. Following on from this the third theme was associated with thoughts and opinions around simplifying CF treatment post-ETI.
Theme 3: simplifying treatment-hopes and fears
This theme developed when discussing opinions about the concept of reducing ACTs and nebulisers once established on ETI. Most cwCF have welcomed this, however, there is no high-quality evidence to support this practice and opinions differed among HCPs and families.
Subtheme 3.1: slow down
All HCPs interviewed explained that they start reducing other treatments gradually after seeing an improvement in children’s health. All HCPs recognised the importance of ACTs to maintain lung health. The lack of longer-term data has made decision-making difficult. Although HCPs understood how crucial reducing treatment burden is for the quality of life of many cwCF and their families. Suzi (a physiotherapist) commented that: ‘They [CFTR modulators] are new, we don’t know how long the effects are going to be, if they’re going to be sustained or not. That’s what makes me anxious, is that they are so new. I would love to think that we can reduce’. Another HCP Laura (a nurse specialist) said:
if it’s safe for us to do so and we can reduce that load and that burden on them then I am all for it. Because it is a very intense daily schedule that a lot of the kids have to go through, I wouldn’t want to do it myself and we’re asking them to do it every day, day in day our forever, essentially. Which if there is an option to reduce it down it’s going to make their quality of life so much better.
Like the HCPs, most parents expressed their hesitation to change their child’s routine and preferred to take things slowly. From their point of view, it was seen as safer to keep doing ACTs to keep children as healthy as possible. They believed that the routine of doing ACTs was helping children stay healthy and changing this idea was hard for some. Some had experienced what could happen if their child did not do ACTs in the past. As a result, some families found it easier to keep the routine going rather than disrupt it and risk needing to reintroduce it again. Some mentioned they needed a scientific answer and time to see the feasibility of simplifying physiotherapy yet maintaining their child’s health. This was summarised by Amy (mother of a cwCF aged 16–18 years) as follows:
I’m still very firmly of a mind that she must do it, she must do it to absolutely the best of her ability … for me, it’s easier just to carry on like that because for me I think it’s worse to have to start going up again with things. So, I would rather just do it absolutely maximally and then know you’ve done everything you can and then that’s just in the hands of whatever happens.
Martha (a mother of a cwCF aged 12–15 years) said:
I don’t want to be the person who stops doing the physio and then, six months later, research comes out saying you probably should have kept doing it. At the minute, I think we’re happy to just be patient, be grateful. The transformation is massive, so I kind of think I’ll never take that for granted.
Only a small number of cwCF themselves mentioned any uncertainty about reducing treatment being the right thing to do. Arthur (cwCF aged 12–15 years) comment illustrated this: ‘They offered me the chance, last time we were at clinic, to drop one physio completely. But I didn’t want to …. In case I stated coughing again’.
Subtheme 3.2: ‘Doing less would be better’ (Sonny, cwCF aged 12–15 years)
Contrary to the HCPs and carers’ views, most children themselves expressed enthusiasm about taking this step and thought that reducing ACTs would improve their lives. It was clear that the majority were keen to reduce their treatment as soon as possible. There was eagerness among some individuals who had reduced some ACTs to move on to the next level and do none. For example: ‘I’d rather try a break, because if you don’t try it you’re not going to know. Even if it does go wrong, you can just go back to it’ (Elizabeth, cwCF aged 12–15 years).
Subtheme 3.3: suggestions
Participants were asked to put forward suggestions about what should happen to ACTs and nebulised treatments following improvements with ETI. Several children and parents proposed that ACTs should become ‘as required’ rather than daily. This would mean they would feel more empowered and be able to contribute to the decision about when to introduce ACTs based on their judgement. Helen (mother of a cwCF aged 12–15 years) said: ‘I think, depending on how you feel, it should be the patient’s decision. It’s their health so they should be able to determine whether they need to or not with the guidance of the doctors’. (Pippa, a cwCF aged 16–18 years) A parent commented: ‘I feel like the next step would just be on an as-and-when basis, rather than a daily routine’.
Several HCPs advocated for a shift in treatment protocols where approaches are personalised and tailored to an individual’s needs. Although they were generally supportive of this change, they highlighted the need to have a structured process and to track progress and document any changes. This was summarised in this quote:
I think what we are doing is probably trying to reduce things, a little bit at a time, and monitoring the effects of that … I think trying to find a balance somewhere, because I don’t want to be very much, right, it’s fine, you're really well, we’ll just stop all your treatment. So, maybe at one clinic, you might say, ‘Instead of doing 10 cycles of your PEP mask, you could do 8’. And then the next clinic, if everything is okay, we might put that down a little bit more And I have to admit, I’m going slowly, slowly, rather than just. Right, that’s fine, stop everything’ (Sarah, a physiotherapist)
Another suggestion was to encourage children to do more exercise as ACTs were reduced. Several participants mentioned they believed that exercise could be an alternative option that helps maintain physical health and provides a ‘safety net’ when simplifying ACTs. As Mary (a physiotherapist) commented:
I also think that my advice about exercise is becoming more important, because I suspect that people’s- And this is the way I’ll sell it to them, is that their ticket out of doing routine airway clearance or day-to-day physio is probably to move more. So, ‘I would be happy to reduce your airway clearance to once a day, if you do some exercise’.
A patient perspective on this was:
I think it should still go on, I think you sort of need exercise still and everything like that, so I don’t see a need to stop at all, I think it does still help and stuff like that. Because although the Kaftrio helps I feel like you need something with it, so they work hand in hand, I think you still need them both. (Maggie, a cwCF aged 16–18 years)
In summary, after experiencing an improvement in their health the majority of cwCF were keen to reduce or even stop ACTs. Parents and HCPs are receptive to the idea of treatment simplification and willing to give suggestions but prefer a more cautious approach and would like to see more research performed in this area. The final theme focused on changes in attitudes and models of CF care post-ETI.
Theme 4: ‘Kaftrio is a game changer’ (Sarah, a physiotherapist)
The final theme was the change in clinical practice that has developed and is still evolving in the HEMT-era. It can be summarised by the quote from one of the HCPs describing ETI as a ‘game changer’. This could be grouped into two subthemes.
Subtheme 4.1: shift
A common view was that a shift was noticed after ETI was introduced. One of the changes that HCPs reported was a change in the attitudes of children and families towards ACTs, especially in those who experienced significant health benefits.
There was a sense of growing confidence in individuals to decide on their own treatment. Some participants questioned the need for ACTs. After starting ETI some children have felt much healthier and along with parents voiced that they may not need to do ACTs, especially those who had no secretions. As Joan (a physiotherapist) summarised: ‘I think some of the families and patients have almost voted with their feet a little bit, stopped things and then come and told us’. A parent commented that: ‘he’s not producing thick mucus with the drug. So, if he’s not producing thick mucus, and he can cough things up himself, or he doesn’t have a cough, then he doesn’t need physio …. Or if it maybe potentially- I don’t know’ (Helen, mother of a cwCF aged 14 years).
Another reported issue was a shift in the level of adherence with other treatment. Several HCPs felt adherence had deteriorated after the introduction of ETI because children and families felt they could miss some without any harm. However, some HCPs argued that simplifying treatment had helped patients then be more focused and committed to ACTs and to have the energy to do it. As Mary (a physiotherapist) put it about adherence issues: ‘think the challenges are still there and they’re still the same, but they have been exaggerated, if you like. So, adherence has got a lot worse, because actually they feel great, and they don’t understand why they would necessarily need to do this’. Laura (a nurse) commented that: ‘the simpler we can make their treatment, the better, because they’re more likely to do it’.
‘Good luck getting me to do it again’ (Sonny, a cwCF aged 12–15 years). This was how one of the children expressed his feeling about doing ACTs again after getting used to a simplified regime. This was a challenge that was also recognised by one of the physiotherapists when a patient experiences an exacerbation and is required to do ACTs and use nebulisers: ‘Because I think they’ve almost had a taste of the good life, whereby they’re doing less. I think it’s very hard to then build back up again’ (Mary, a physiotherapist).
Another shift HCPs described was a change in the workload. Historically, physiotherapists mainly concentrated on ACTs, while after ETI, they have turned their attention more towards promoting exercise and a healthy lifestyle. Other responses to this question talked about focusing on cwCF who do not have access to ETI and those who have not experienced a dramatic clinical benefit from it. These opinions are summarised by: ‘And maybe we have got the airway clearance there. But I think more emphasis on keeping them healthy, in terms of chest as well as exercise tolerance and lifestyle, will potentially go more towards the exercise side of things’ (Kate, a physiotherapist). Along with: ‘There’ll still be some that need it because you’ll always get the extremes with different kids that have difficulties. You’ve got the kids with the other genes that don’t necessarily get it’ (Suzi, a physiotherapist).
Subtheme 4.2: emerging crisis
Despite the positive impact of ETI, there are new challenges facing the CF multidisciplinary team. Weight management is a new challenge, in the past maintaining good nutritional status was a major focus of care. The normalisation of dietary advice for people who had required a high calorie intake previously is a dramatic new recommendation. This was summarised by Ruby (cwCF aged 12–15 years) as: ‘Before Kaftrio, yes, you could eat anything you want, because you wouldn’t put weight on. Now, there was a period of time where I was getting really upset, because all of a sudden, I had got a lot of weight on’. An HCP commented that:
I think one of the other challenges that we’re seeing now is not necessarily always physio-related, but I think will have a massive impact on physiotherapy, will be weight. A lot of these patients are now gaining weight a lot more rapidly than what they would have done, and they’re still in a lot of the habits from younger ages, where they’ve had a lot of calories, and they’ve fortified a lot of their foods, and now they’re actually gaining weight (Mary, a physiotherapist).
Some cwCF and their families questioned ‘what is next?’. Talking about this issue, a participant said she worried if the benefits from ETI would be sustained in the long-term and wondered if her health would deteriorate in the future. A small number of participants stated that observing the results of ETI raised the expectation of having a genuine cure for CF in the future: ‘I think now that I’ve got the drug and, obviously, we don’t know how long it’s going to last for, I guess, it could be 10 years, it could be 20 years before it’s starting to decline … It’s just like you're thinking about it’ (Pippa, cwCF aged 16–18 years). Peter (father of a cwCF aged 12–15 years) said: ‘I think Kaftrio is the closest thing that we’ve had so far. I know it sounds greedy, but having something that’s better than that would always be great’.
Overall, the interconnected themes demonstrate that ETI has had a significant impact on the health and lives of cwCF and their families. Treatment burden has and is being reduced and there is motivation to simplify treatment further. This is feeding in to changes in clinical practice and attitudes towards treatment.
Discussion
This study aimed to increase understanding of the experiences of cwCF prescribed ETI and the opinions of their carers and HCPs about its impact. There was a particular focus around treatment burden, especially ACTs and nebulisers. The qualitative approach allowed an in-depth look at the experience of cwCF in this new era of care. Four main themes were identified relating to the improvement in the cwCF health and families day to day lives, the reduction in treatment burden, their perspectives on approaches to simplifying treatment and finally the shifts in CF clinical practice. The significant changes associated with ETI over a short period were encompassed by one overarching theme.
The findings highlight the major improvements in the health and lives of cwCF following the introduction of ETI. This supports a previous qualitative study which explored the influence of the older CFTR modulators on individuals’ outlook on life outside clinical health variables.18 There are similarities between the positive attitudes expressed by cwCF in this study and those described by adults on ETI.19 20 Despite the positive outcomes for many to date, there were also worries expressed about the longer-term. HCPs, carers and cwCF all articulated concerns about whether benefits would be sustained. Continuous evaluation of ‘real-world’ data is required to confirm long-term safety and efficacy and qualitative approaches also provide important insights.
One of the aims of this study was to understand the changes in treatment burden. Several studies identified the burden of treatment for cwCF both physically and psychologically prior to HEMT.21 22 A substantial amount of time was spent completing treatment and this caused many to feel different.23 A qualitative study found that keeping up with treatment is the most challenging aspect of CF for older children.24 This treatment burden has diminished with ETI as described by cwCF and their families.
A retrospective study looked at treatment patterns after starting ivacaftor and found a decrease in inhaled mucolytics and antibiotics prescribed.25 The wish to reduce treatment burden is shared by all but the safety of doing this must be ensured.5 14 Ongoing studies, including CF STORM, aim to examine the safety of discontinuing mucolytics in those on ETI.19 Most carers and HCPs favoured a cautious approach in the absence of high-quality clinical evidence to support doing this. Contrary to HCPs, most cwCF expressed willingness to reduce ACTs. Another important finding was that the attitude of cwCF towards physical therapy and nebulised treatment has changed, and they have started questioning their need for this treatment.
In the pre-HEMT era, Swisher and colleagues explored the attitudes of cwCF towards physical activity.26 They concluded that most cwCF recognised the importance of activity and ACTs and benefits for their health.26 A possible explanation for this difference in attitude might be the presence of mucus and secretions. Previously the results of ACTs and nebulised treatment were more immediately apparent. However, views have changed for many, possibly due to fewer problems with secretions. Educating cwCF and their carers about the rationale for ACTs and nebulised treatment has become doubly important. Encouraging exercise is one of the tools suggested to support physical health with the reduction of ACTs.15 Many participants believed that exercise might be used in place of ACTs, which is consistent with earlier research.16
Several studies have examined the feasibility of exercise replacing ACTs, but no study has proven its effectiveness.27 28 A previous study found that almost 50% of CF people who exercised omitted ACTs.15 Several participants described improved exercise tolerance and energy levels in our study and it is possible that exercise will now be easier to do. Adherence and monitoring of exercise is challenging, especially in the adolescent age group.29 Consistent with the literature, we found that a responsive and personalised approach to ACTs is likely to be the most effective solution.30 31 Engagement of cwCF in developing their treatment plan and empowerment to select options based on their preferences with the shared goal of maximising health will be crucial. Exercise has the added benefit of helping reduce undesired weight gain associated with ETI that was mentioned by several participants.
Most participants had positive expectations before starting it based on high profile experiences of older patients.20 Equally, it is important to be mindful that some experience greater benefit than others and that for around 10% of cwCF there is no HEMT option.32 Ongoing support for these groups is vital.
Limitations of our study include that it was single centre and that interviews were conducted on average 15 months after starting ETI, which may have made it harder to remember the time pre-ETI. On the other hand, a strength was the heterogeneity of age and gender of the cwCF interviewed and the involvement of three different groups to increase understanding from all perspectives.
Conclusion
This study has provided insight into what cwCF, their carers and HCPs have experienced with ETI. Despite the overall positive experiences, there are new challenges to be addressed. ETI has prompted a shift from traditional treatment approaches, especially regarding ACTs and nebulised therapy. This offers an opportunity to personalise treatment, but it remains important that longer-term effects are studied.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Not applicable - is a qualitative study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the East Midlands – Leicester Central Research Ethics Committee (21/EM/0210). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to all the cwCF, families and HCPs who gave up their time to take part in this study. The research was funded as part of a PhD studentship to MA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @malc_brod
Contributors MA: contributed to study design, performed interviews and data analysis wrote the first manuscript draft. NH, SG, IH, SV and CW: contributed to study design and commented on the manuscript. MB: conceived and designed the study, completed the final draft of the manuscript and will act as guarantor.
Competing interests MB: investigator-led research grants: Pfizer and Roche Diagnostics; speaker fees paid to Newcastle University: TEVA, Novartis, Roche Diagnostics, Vertex Pharmaceuticals; travel expenses to educational meetings: Boehringer Ingelheim, Vertex Pharmaceuticals, TEVA.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.