Article Text

Abstract
Introduction Although cannabis is frequently used worldwide, its impact on respiratory health is characterised by controversy.
Objective To evaluate the association between cannabis use and respiratory-related emergency room (ER) visits and hospitalisations.
Methods A retrospective, population-based, cohort study was carried out, linking health survey and health administrative data for residents of Ontario, Canada, aged 12–65 years, between January 2009 and December 2015. Individuals self-reporting cannabis use within the past year were matched to control individuals (people who reported never using cannabis, or used cannabis only once, and more than 12 months ago) in upwards of a 1:3 ratio on 31 different variables, using propensity score matching methods. Respiratory-related and all-cause ER visits or hospitalisations, and all-cause mortality, were evaluated up to 12 months following the index date.
Results We identified 35 114 individuals who had either used cannabis in the past year or were controls, of whom 6425 (18.3%) used cannabis in the past year. From this group, 4807 (74.8%) were propensity-score matched to 10 395 control individuals. In the propensity score matched cohort, there was no significant difference in odds of respiratory-related ER visit or hospitalisation between cannabis users and the control group (OR 0.91, 95% CI 0.77 to 1.09). Compared with control individuals, cannabis users had significantly increased odds of all-cause ER visit or hospitalisation (OR 1.22, 95% CI 1.13 to 1.31) and there was no significant difference with respect to all-cause mortality (OR 0.99, 95% CI 0.49 to 2.02).
Conclusions Although no significant association was observed between cannabis use and respiratory-related ER visits or hospitalisations, the risk of an equally important morbidity outcome, all-cause ER visit or hospitalisation, was significantly greater among cannabis users than among control individuals. Therefore, cannabis use is associated with increased risk for serious adverse health events and its recreational consumption is not benign.
- clinical epidemiology
- tobacco and the lung
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The published literature on cannabis smoking and acute respiratory illness is extremely limited, with one previous study demonstrating that cannabis smoking is associated with higher frequency of protracted acute bronchitis episodes, and another study showing significantly greater outpatient visits for respiratory illness, but not hospitalisations.
WHAT THIS STUDY ADDS
Our population-based, retrospective, propensity score matched cohort study, involving 15 202 individuals and extensive covariate adjustment, showed no significant difference in the frequency of respiratory-related emergency room visits or hospitalisations between cannabis users (3.6%) and never-users (3.9%), but all-cause emergency room visits or hospitalisations were significantly greater among cannabis users (30.0% vs 26.0%). Respiratory-related reasons were the second leading aetiology for all-cause ER visits and hospitalisations among cannabis users.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Given that all-cause emergency visits or hospitalisations, which are a clinically important morbidity marker, were significantly greater among cannabis users than among control individuals, and respiratory-related reasons were the second most common cause for emergency visits and hospitalisations in the all-cause outcome, our results suggest that the worldwide rising use of recreational cannabis needs to be curtailed.
Introduction
Cannabis is the most commonly used psychoactive drug worldwide and its use is rising.1 Prevalent past-year use rate in the Canadian population in 2021 was estimated to be 25%.2 Although cannabis can be consumed in a variety of ways, smoking combusted cannabis is the most predominant route in Canada.2 Although cannabis contains similar types and quantities of volatile compounds (eg, ammonia, hydrocyanic acid, etc) and tar components (eg, phenols, naphthalene, etc) as tobacco (which are implicated in the development of tobacco smoking-related airway disease),3 data published on the association between cannabis smoking and airways health have been contradictory. On the one hand, cannabis smoking has been shown to be associated with the development of chronic bronchitis-type symptoms (including chronic cough, chronic sputum production and wheezing),4 and similar changes of bronchial inflammation are evident on bronchoscopy and endobronchial biopsies among cannabis and tobacco smokers.5 6 On the other hand, cannabis smoking has largely thus far not been found to be associated with pulmonary function test measures of airflow obstruction, such as declining forced expiratory volume in one second (FEV1) or reduced FEV1/forced vital capacity ratio as a result of a low FEV13 4 (with a few recently published exceptions7 8), or with thoracic CT evidence of emphysema.9
Cannabis smoking might theoretically predispose to acute respiratory illness in several ways: cannabis is known to destroy airway ciliated columnar epithelial cells and promote mucous-secreting goblet cell hyperplasia and such changes may predispose to acute respiratory tract infection6; δ-9 tetrahydrocannabinol has potential immunosuppressive effects, which may contribute to acute respiratory tract infection10 11; cannabis is frequently contaminated with pathogenic micro-organisms12 13; and, cannabis use can contribute to altered mental state14 and/or hyperemesis,15 which might then lead to an aspiration event. There is a paucity of data on the association between cannabis smoking and acute respiratory illness.16 17 Compared with non-cannabis smokers, one small study reported significantly higher frequency of protracted acute bronchitis episodes,16 and another study a significantly greater number of outpatient visits for respiratory illness (but not hospitalisations),17 among cannabis smokers.
Using linked health survey and health administrative data, our purpose was to evaluate the association between cannabis use and more serious, acute, adverse respiratory events, as identified by emergency room (ER) presentation or hospital admission for respiratory-related reasons.
Methods
Study design
This was a retrospective, population-based cohort study, linking health survey data with multiple Ontario health administrative databases, for January 1, 2009 to December 31, 2015. All databases are held and were analysed at ICES (formerly known as the Institute for Clinical Evaluative Sciences). ICES is an independent, non-profit research institute, whose legal status under Ontario’s health information privacy law allows it to collect and analyse healthcare and demographic data, without consent, for health system evaluation and improvement. Because sampling strategies were used in the collection of the health survey data to obtain a representative sample of the community-dwelling population aged 12 years and older,18 and because health administrative data are collected on all Ontario residents through the province’s single-payer public health insurance plan, our analysis can be considered population based. Ontario is Canada’s most populous province (~14.7 million people,~40% of national population) and is culturally diverse. Use of the data in this project is authorised under section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a research ethics board.
Data sources
Multiple health-related databases were linked at ICES using unique coded identifiers. Ontario data from the 2009–2010 and 2011–2012 Canadian Community Health Surveys (CCHS) were used. The CCHS is national, cross-sectional survey conducted by Statistics Canada every 2 years that collects a broad range of self-reported sociodemographic and health data on a nationally representative sample of the Canadian community-dwelling population aged 12 years and older.18 Although more recent CCHS cycles have been conducted beyond 2011–2012, these were not yet available for linkage with health administrative databases at ICES. Self-reported cannabis use was captured by the CCHS with the following questions: “Have you ever used or tried marijuana, cannabis or hashish?” (with possible responses including yes, just once; yes, more than once; or, no), and those who responded affirmatively were then asked, “Have you used it in the past 12 months?” (with possible responses including yes or no). Although information on route of cannabis receipt was not collected by CCHS, inhalation is by far the most predominant form of consumption.19 Although recreational versus authorised medicinal use was not distinguished by the CCHS, recreational purposes account for the bulk of cannabis use.20 The CCHS data were linked to the following health administrative databases: (1) the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD), which contains information on all hospital discharges; (2) the National Ambulatory Care Reporting System (NACRS) Database, which contains information on ER visits; (3) the Registered Persons Database, which contains information on demographics and mortality; (4) the Ontario Health Insurance Plan (OHIP) claims database, which contains information on all physician fee-for-service patient care claims, in both ambulatory and hospital settings; (5) the Ontario Mental Health Reporting System (OMHRS), which contains information on all mental health hospital admissions and (6) several validated, disease-specific databases created by ICES (outlined in the online supplemental file) using clinical and health administrative data.21–27
Supplemental material
Study population
Ontario residents aged 12–65 years, who participated in either the 2009–2010 or 2011–2012 CCHS, were included. Individuals aged 66 years and older were excluded, since a trivial number of cannabis users belonged to that age group (~1%). If an individual participated in both CCHS cycles (equating to ~0.2% of 2009–2010 and 2011–2012 CCHS participants), only data from the most recent cycle were considered.
Exposed and control groups with index date definitions
The exposed group consisted of individuals reporting any cannabis use in the preceding 12 months. The control group included individuals who reported never having used cannabis, or having used cannabis only once and more than 12 months ago. Individuals who had used cannabis multiple times, but more than 12 months ago, were intentionally excluded, since our purpose was to compare outcomes associated with recent/active cannabis use with an uncontaminated control group of never or former trivial cannabis users. The index date for both the exposed and control group was the date of the CCHS interview.
Outcomes
Consistent with our objective to examine the association between cannabis use and more serious, acute, adverse respiratory events, our primary outcome was a respiratory-related ER visit or hospitalisation, defined as the recording of an International Classification of Diseases version 10 (ICD-10) diagnostic code for either upper or lower respiratory tract infection, respiratory failure, asthma or chronic obstructive pulmonary disease (COPD), as the reason for presentation/admission (see the online supplemental file for a comprehensive listing of ICD-10 codes considered). We considered codes for asthma and COPD in our primary outcome definition, since these are two commonly encountered chronic airway conditions, characterised by recurrent, acute respiratory exacerbations, which are sometimes serious enough to necessitate presentation to hospital. Secondary outcomes considered were all-cause ER visit or hospitalisation, and all-cause mortality. All outcomes were evaluated up to 12 months following the index date, or up to the date of death, whichever came first. We intentionally limited the time period in which to evaluate outcomes in our main analysis to 12 months following the index date, so as to be reasonably confident that any positive outcomes observed would be linked to exposure status at the time of the index date. The longer the time window used, the greater the likelihood for changes in cannabis exposure to occur among individuals classified in the exposed and/or control groups, which would then result in group contamination.
Propensity score matching
In order to minimise bias in our analysis from other variables, propensity score matching methods were used.28 A propensity score model for cannabis use was created, using logistic regression modelling, incorporating 31 different variables, including demographics, multiple physical and mental health comorbidities, markers of general healthcare use, previous respiratory-related ER visit or hospitalisation, tobacco smoking history and quantity, problem drinking and other substance use, previous contact with a respirologist, previous receipt of pulmonary function testing, previous respiratory-related medication use, previous influenza vaccine receipt and year of cohort entry. A full list of variables included in the propensity score can be found in table 1. The supplement contains a detailed description of the variables included in the propensity score. One exposed individual was matched upwards to a maximum of three control individuals (for the purpose of enhancing sample size). In accordance with published recommendations, we matched individuals on the logit of the propensity score using a width calliper equal to 0.2 of the SD of the logit of the propensity score.29 In addition to the propensity score, we hard-matched exposed and control individuals on the following variables in order to facilitate planned sensitivity analyses (described in more detail below): sex; respiratory-related ER visit or hospitalisation in the preceding year; tobacco smoking history status; and, pre-existing asthma or COPD.
Baseline characteristics of overall cohort, before and after propensity score matching
Sensitivity analyses
Several planned sensitivity analyses were undertaken. First, outcomes were examined stratifying by sex, since possible sex-related differences in the association between cannabis use and respiratory health have been up to now little explored.8 Second, outcomes were evaluated distinguishing by presence of a respiratory-related ER visit or hospitalisation in the year prior to the index date. Because respiratory exacerbations are known to be the best single independent predictor of future respiratory exacerbation risk in the setting of obstructive airways disease,30 we sought to further minimise the potential confounding effects of a history of respiratory infections/exacerbations, by evaluating outcomes in the subgroup of individuals without such a history. Third, because concurrent tobacco smoking is common among cannabis users,31 32 and tobacco smoking is well-known to influence respiratory-related morbidity and mortality risks, outcomes were evaluated among current/former versus never tobacco smokers, to further minimise potential bias by this factor. Fourth, we examined outcomes distinguishing by presence of asthma or diagnosis of COPD prior to the index date, in order to determine if risk of cannabis-related adverse respiratory events was greater among individuals with established obstructive airways disease, as some research has suggested.7 8 Presence of asthma or COPD diagnosis was based on previously validated algorithms of health administrative database coding,21 22 where the reference standard was expert panel review of information in patient primary care medical charts (for asthma, sensitivity = 84% and specificity = 76%21, and for COPD, sensitivity = 85.0%, specificity = 78.4%22). A final sensitivity analysis, evaluating outcomes over a longer 3-year follow-up period after the index date, is presented in the online supplemental file.
Statistical analysis
Descriptive statistics with standardised differences were calculated for all baseline covariates among exposed and control individuals, in order determine the adequacy of the matching process. Logistic regression with the method of generalised estimating equations was used to estimate odds ratios (ORs) with associated 95% confidence intervals (CIs) for all outcomes in the propensity score matched cohort in the main analysis and sensitivity analyses. Number needed to harm (NNH) was determined by previously described methods.33
Patient and public involvement statement
Our study was conducted using deidentified data. There was no direct interaction with any individual participant, and therefore, members of the public were not involved in study design, recruitment or conduct of the study.
Results
Cohort derivation
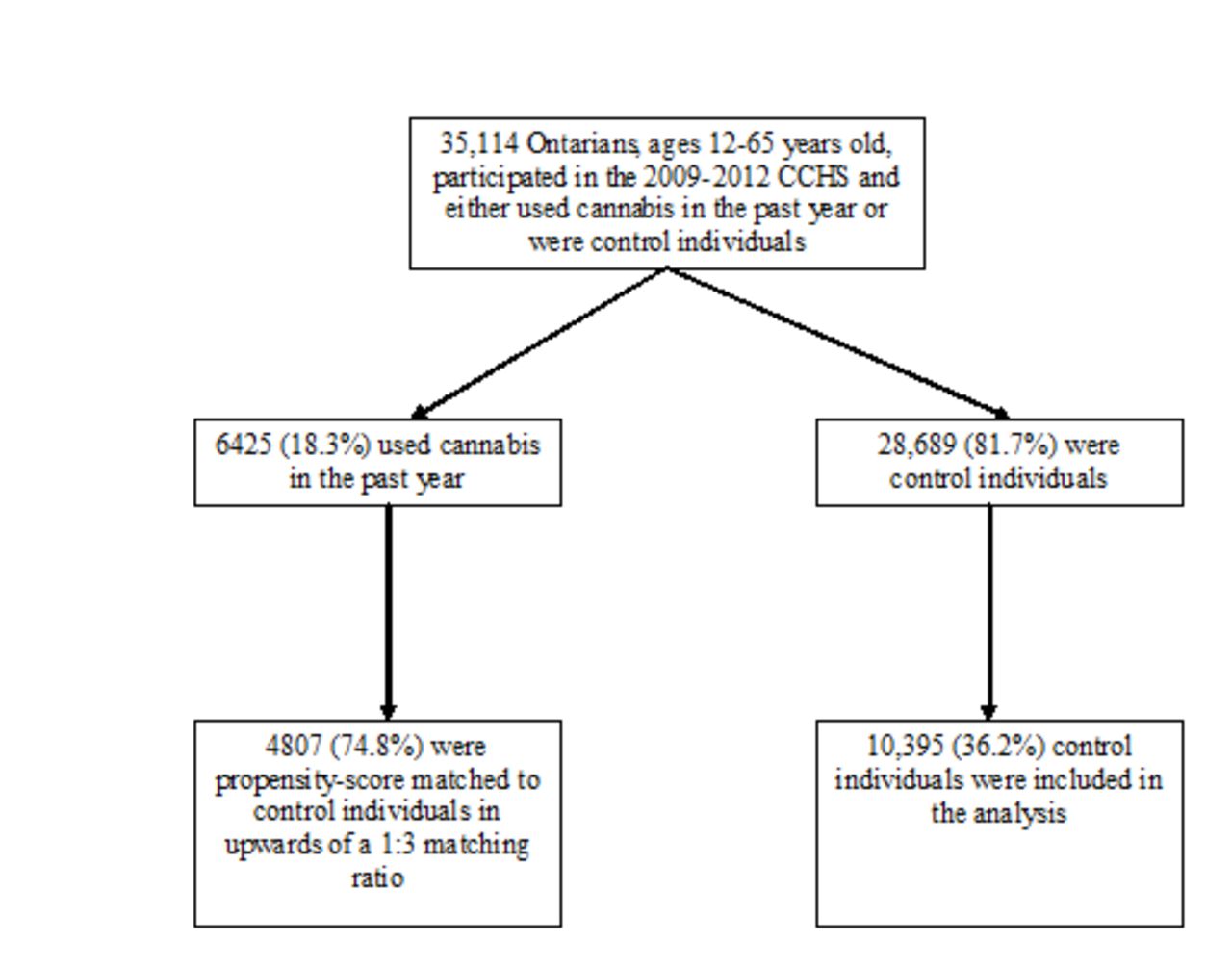
In the 2009–2010 and 2011–2012 CCHS, there were 35 114 individuals aged 12–65 years who had used cannabis in the past year or were control individuals. Of these, 6425 (18.3%) used cannabis in the past year, and from this group, 4807 (74.8%) were propensity score matched in upwards of a 1:3 ratio to 10 395 control individuals (figure 1). After propensity score matching, cannabis users and control individuals were adequately balanced on baseline characteristics, with standardised differences being below 10% for all variables (table 1). In the propensity score matched sample, cannabis use frequency among exposed individuals occurred as follows: 42.5% were using less than once a month; 18.1% were using 1–3 times a month; 9.4% were using once a week; 11.4% were using more than once a week; 10.5% were using every day; and, cannabis use frequency data were unavailable for 8.0%.
{kind=link}
Flow diagram outlining derivation of the exposed and control groups. CCHS, Canadian Community Health Surveys.
Overall cohort analysis
In the propensity score matched cohort, odds of respiratory-related ER visit or hospitalisation was not significantly different between exposed and control individuals (OR 0.91, 95% CI 0.77 to 1.09, p=0.32) (table 2). However, compared with the control group, cannabis users had significantly greater odds of all-cause ER visit or hospitalisation (OR 1.22, 95% CI 1.13 to 1.31, p<0.0001, NNH 25). Examining the top 100 ICD-10 diagnostic codes recorded as etiologies for the all-cause ER visit and hospitalisation outcome among cannabis users revealed that respiratory-related were the second most common cause (14.2%), after acute trauma (15.1%) (table 3). All-cause mortality was not significantly different between the two groups (OR 0.99, 95% CI 0.49 to 2.02, p=0.98).
ORs and confidence intervals for outcomes in the overall propensity score matched cohort
Breakdown of all-cause emergency room visit and hospitalisation outcome for cannabis users for the top 100 ICD-10 diagnostic codes recorded
Sensitivity analyses
By sex
There was no significant difference in the odds of respiratory-related ER visit or hospitalisation between cannabis users and control individuals, among both men and women (table 4). However, compared with their respective controls, both men and women cannabis users had significantly higher and similar odds of all-cause ER visit or hospitalisation (men: OR 1.23, 95% CI 1.11 to 1.36; women: OR 1.23, 95% CI 1.10 to 1.37). Owing to the small sample size, we were unable to produce a reliable OR estimate for all-cause mortality for this sensitivity analysis and all others presented in table 4.
ORs and confidence intervals for outcomes, according to selected subgroups
By prior respiratory-related ER visit or hospitalisation
In the subgroup of individuals who had not experienced a respiratory-related ER visit or hospitalisation in the year prior to the index date, no significant difference was observed in respiratory-related ER visit or hospitalisation odds among exposed versus control individuals (table 4). However, significantly greater all-cause ER visit or hospitalisation odds were observed among cannabis users (OR 1.22, 95% CI 1.13 to 1.32) relative to control individuals. In the subgroup of individuals who had experienced one or more respiratory-related ER visits or hospitalisations in the year prior to the index date, no significant differences were observed between the two groups with respect to any of the outcomes.
By tobacco smoking history
Among current/former tobacco smokers, exposed versus control individuals had significantly lower odds of respiratory-related ER visits or hospitalisations (OR 0.80 95% CI 0.65 to 0.99), but significantly higher odds of all-cause ER visits or hospitalisations (OR 1.16, 95% CI 1.06 to 1.26) (table 4). Among never-tobacco smokers, there was no significant difference in respiratory-related ER visit or hospitalisation odds for exposed versus control individuals, but significantly greater all-cause ER visit or hospitalisation odds were observed among exposed (OR 1.35, 95% CI 1.16 to 1.56).
By pre-existing asthma or COPD
There was no significant difference in odds of respiratory-related ER visits or hospitalisations between cannabis users and control individuals in both the subgroup with pre-existing asthma and COPD and the subgroup without pre-existing asthma and COPD (table 4). However, in both subgroups, cannabis use was associated with significantly elevated odds of all-cause ER visits or hospitalisations (with pre-existing asthma or COPD: OR 1.16, 95% CI 1.00 to 1.35, p=0.05; without pre-existing asthma or COPD: OR 1.24, 95% CI 1.13 to 1.35).
Discussion
Our primary outcome, odds of respiratory-related ER visits or hospitalisations, was not significantly greater among cannabis users than the the control group in either the overall cohort, or in any of our sensitivity analyses. However, our population-based study demonstrated that cannabis use was associated with significantly increased all-cause ER visits or hospitalisations, which is arguably an equally clinically important morbidity outcome, with a relatively low NNH of only 25, and that respiratory-related reasons were in fact the second most common aetiology for all-cause ER visits and hospitalisations among cannabis users. Although the observation of no significant association between cannabis use and respiratory-related ER visits or hospitalisations may certainly be real, and somewhat at odds with the limited previous literature on the topic,16 17 the negative result might also be explained by several possible factors for which we were unable to adjust, including: insufficient cannabis smoke exposure among users included in our particular study (eg, previous research has shown that decline in lung function occurs only among cannabis smokers with >20 joints per year exposure history7 34); some of the reported cannabis use being non-inhalational (which would be less likely to cause respiratory-related illness than inhaled cannabis); and, possible secondhand cannabis smoke exposure among control individuals, thereby ‘contaminating’ the control group. It is also possible that our analysis might have been insufficiently powered to detect a significant signal with respect to the primary outcome.
As all-cause ER visits/hospitalisations were significantly elevated in association with cannabis use among the subgroup of individuals without a recent history of respiratory-related ER visits/hospitalisations, this strengthens the credibility of a true link between cannabis use and the outcome, since these individuals would probably have a lower a priori risk of presenting to hospital. Although all-cause ER visits/hospitalisations were not found to be elevated among cannabis users with a recent history of respiratory-related ER visits/hospitalisations, the much smaller sample size numbers in that subgroup potentially impeded the ability to detect a significant result. In contrast to some previous research demonstrating that combined cannabis and tobacco exposure is linked to worse outcomes,35 36 we surprisingly found that cannabis use was associated with significantly decreased odds of respiratory-related ER visits/hospitalisations in the subgroup of current/former tobacco smokers. However, in the same subgroup of current/former tobacco smokers, odds of all-cause ER visits/hospitalisations were significantly elevated among cannabis users, and reduced odds of respiratory-related ER visits/hospitalisations was not observed with cannabis use in the subgroup with pre-existing obstructive airways disease (and many individuals in that subgroup would be characterised by having a significant tobacco smoking history). Both sexes were at similar heightened odds for all-cause ER visits/hospitalisations in association with cannabis use, which is in contrast to some previous research demonstrating that men (but not women) cannabis smokers were more susceptible to worse health.8
It is noteworthy that the leading aetiology of the increased all-cause ER visit/hospitalisation outcome among cannabis users was acute trauma (~18%). Because our present research focus was on the possible association between cannabis use and acute respiratory infectious illness, it was beyond our scope to further describe possible associations between cannabis use and physical trauma. However, there is a growing body of published literature linking cannabis consumption to increased risks of generalised body injury,37 motor vehicle accidents,38 falls39 and skeletal fractures (along with low bone mineral density).40
Our study has several limitations. Causation should not be inferred as the explanation for any of our positive findings, given the observational nature of our study. Unmeasured confounding might have accounted for any of our observed positive results. However, we minimised confounding factors by propensity score matching on a broad list of relevant covariates (including, but not limited to, tobacco smoking, multiple physical and mental health comorbidities, and previous ER visits/hospitalisations) and we performed several sensitivity analyses stratifying by some key variables (eg, tobacco smoking). While not all cannabis users in our exposed group might have consumed cannabis by inhalation (which is the route that would be most likely to cause respiratory-related illness), inhalation is known to be the most common route of receipt.19 Because cannabis use was based on self-report, there is potential for introduction of recall and social desirability biases. However, information on smoking is usually gathered by self-report. While the CCHS included a question that crudely captured frequency of cannabis use over the preceding year among exposed individuals, we were unable to perform a dose–response analysis, as reliable estimates could not be produced given small sample numbers in the frequency response categories. The high numbers of infrequent cannabis users in our exposed group might have contributed to our finding of no significant positive association between cannabis use and respiratory-related ER visits or hospitalisations. Information on quantity and potency of cannabis used was not collected by CCHS, and therefore, could not be accounted for in our analysis. About 25% of cannabis users in our study went unmatched, and therefore could not be included in the propensity score matched analysis, and it is unknown how their potential inclusion, if matched, would have influenced the results. We had access to cannabis use data only from the time prior to its decriminalisation in Canada (ie, October 2018). Cannabis use has increased in Canada following its decriminalisation (mostly among middle-aged and older adults),41 potentially affecting both the frequency and nature of related adverse events, but we were unable to perform an analysis before and after decriminalisation. We were also unable to adjust for possible secondhand cannabis smoke exposure among control individuals, as such data were not available to us. Although we considered a broad range of ages in this study (12–65 years), our findings may not apply to children or older adults who use cannabis. Relatively small numbers of cannabis users aged <20 years old and ages 50–65 years precluded evaluation for our adverse outcomes by these age groups of potential interest. Although our results are based on individuals from a single jurisdiction, Ontario, Canada, is culturally diverse.
In conclusion, no significant association was observed between cannabis use and respiratory-related ER visits or hospitalisations. However, after adjusting for a broad range of covariates, the risk of an equally important morbidity outcome, all-cause ER visits or hospitalisation,s was significantly greater among cannabis users than among control individuals, and respiratory-related reasons were the second most common cause for ER visits and hospitalisations in the all-cause outcome. Further research is needed to confirm our findings, but our results suggest that cannabis use is associated with increased risk for serious adverse health events, and therefore, its recreational consumption in the general population should be discouraged.
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email: das@ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Contributors NTV, JZ, CMR, C-WC and TT contributed substantially to the study design, data analysis and interpretation, and manuscript review and editing. JZ was responsible for all statistical analyses and NTV drafted the manuscript. NTV is responsible for the overall content of the manuscript as the guarantor.
Funding This research was funded by a research award grant from The Lung Association - Ontario. The Lung Association - Ontario received unrestricted funding from Tetra-Bio Pharma to independently administer the grant competition. The funding sources had no role in any aspect of the research or writing processes, which were authors' alone. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by: MOH; Canadian Institute for Health Information (CIHI); and, Cancer Care Ontario (CCO).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.