






Abstract
The aim of the study was to evaluate the double modality working of a new autofluorescence videobronchoscope SAFE-3000 for the detection and localization of precancerous and malignant lesions. From April to May 2009, 168 patients underwent SAFE-3000 bronchoscopy using ‘Twin Mode’ and ‘Multiple Image Xposition (MIX)’ technologies. The study considers only 97 patients with morphological alterations (visual score 2 or 3) of mucosa; four bronchial biopsies (two for every modality) have been performed on every patient. Histological diagnosis of the 388 biopsies revealed normal mucosa in 11 patients, four benign lesions, 27 precancerous lesions and 55 malignant lesions. The sensitivity of the ‘Twin Mode’ and ‘MIX’ techniques in the characterization of premalignant and malignant lesions was 96% vs. 100%. The specificity was 60% in both of these technologies. SAFE-3000 autofluorescence bronchoscopy allows an early diagnosis of preneoplastic or neoplastic lesions according to the careful analysis of the bronchial mucosa, due to the complementarity of two modalities ‘Twin Mode’ and ‘MIX’. Based on the relationship between the bronchoscopic goal and the histological results the MIX method contributes more of the new endoscopic technique findings.
1. Introduction
Bronchogenic carcinoma is a major cause of cancer death in western countries, striking both men and women owing mainly to exposure to tobacco smoke that is directly applied to the respiratory epithelium [1]. Surgery for lung cancer is curative in the earlier stages, despite the lack of specific symptoms. Several reasons explain the inoperability of lung cancer including location of the tumour, distant metastasis, respiratory insufficiency that increase the risk associated with the operation. The five-year survival in non-small cell lung cancer (NSCLC) after a complete resection at stage IA and B is between 63% and 83.7% and 46% and 76%, respectively [2, 3]. Survival decreases drastically at stage IIB and IIIA being between 39% and 49% and between 19% and 35.8% [2, 4]. Autofluorescence bronchoscopy (AFB) allows early diagnosis of premalignant and malignant lesions through the different concentration and distribution of both fluorophores and blood flow. Lam et al. [5] performed AFB (SAFE-1000 System Pentax; Tokyo, Japan) on 62 patients with white light bronchoscopy (WLB) negative for lung cancer but with atypical or malignant cells in sputum or bronchoscopic aspiration. The study carried out by AFB and WLB allowed to detect two carcinoma in situ (CIS) and one invasive cancer. In all AFB has a higher sensitivity than WLB (91% vs. 58%) but a lower specificity (26% vs. 50%). SAFE-3000 system makes it possible to acquire and see both the AFB and WLB images simultaneously, improving the quality of images and diagnostic ability. Aim of our study was to evaluate the new autofluorescence bronchoscope in early detection of premalignant lesion or bronchial cancer.
2. Materials and methods
From April to May 2009, 168 patients underwent AFB in our Institute, as routine analysis in lung cancer diagnosis. They were 142 males (84.5%) and 26 females (15.5%), with an average age of 55±3 years (range 40–78 years). Patients were selected among smokers during a provincial programme of lung cancer prevention (Table 1 ). We used SAFE-3000 System (Pentax, Asahi Optical, Tokyo, Japan), equipped with ‘Twin Mode’ and ‘Multiple Image Xposition (MIX)’ technologies. The evaluation of tracheobronchial tree was started by ‘Twin Mode’ and then completed by ‘MIX’ The visual score in endoscopic findings is defined as follows: 1=no abnormality; 2=indecisive abnormality, 3=probably abnormality; 4=definite invasive carcinoma. Four bronchial biopsies were performed on each patient, two with ‘Twin Mode’ and two with ‘MIX’ technology. The average time of examination length was 4±1 min.
Clinical status of patients referred by a work-related medicine programme
| Age | ≥40-year-old |
| Smoking | At least 10 years |
| Symptoms | Absent |
| First episode of haemoptysis | |
| High resolution CT of the thorax | Increase bronchovascular markings |
| Pulmonary opacity larger than 1 cm | |
| but smaller than 4 cm |
| Age | ≥40-year-old |
| Smoking | At least 10 years |
| Symptoms | Absent |
| First episode of haemoptysis | |
| High resolution CT of the thorax | Increase bronchovascular markings |
| Pulmonary opacity larger than 1 cm | |
| but smaller than 4 cm |
CT, computed tomography.
Clinical status of patients referred by a work-related medicine programme
| Age | ≥40-year-old |
| Smoking | At least 10 years |
| Symptoms | Absent |
| First episode of haemoptysis | |
| High resolution CT of the thorax | Increase bronchovascular markings |
| Pulmonary opacity larger than 1 cm | |
| but smaller than 4 cm |
| Age | ≥40-year-old |
| Smoking | At least 10 years |
| Symptoms | Absent |
| First episode of haemoptysis | |
| High resolution CT of the thorax | Increase bronchovascular markings |
| Pulmonary opacity larger than 1 cm | |
| but smaller than 4 cm |
CT, computed tomography.
2.1. SAFE-3000 system
Is characterized by a videobronchoscope EB-1970 AK, with white light produced by a Xenon lamp and fluorescent light from a Diodo Laser (408 nm; 20–40 W). The diagnostic quality of system is strictly connected with ‘Twin Mode’ and ‘MIX’ technologies. These modalities exploit the variations in the microenvironments or the differences in the concentration of fluorophores and carrier molecules (flavin, porphyrin and nicotinamide adenine dinucleotide) between tumour and normal tissue. The first technique allows contemporary evaluation of images in both modalities (AFB and WLB) on the same screen (Fig. 1 ). The second technique is based on the AFB and WLB combination, stressing the contrast that exists between the autofluorescence signal and the information obtained thanks to white light (Fig. 2 ). The passage between ‘Twin’ to ‘MIX’ and vice versa carried out easily, pushing the buttons in the handle of bronchoscope (Fig. 3 ).

Bronchogenic carcinoma localized in the lateral side of the middle lobe bronchus. The ‘Twin Mode’ ensures the white light and autofluorescence study of neoplasm morphological aspects contemporarily. The tumour is highlighted in the triangular area of mucosa.
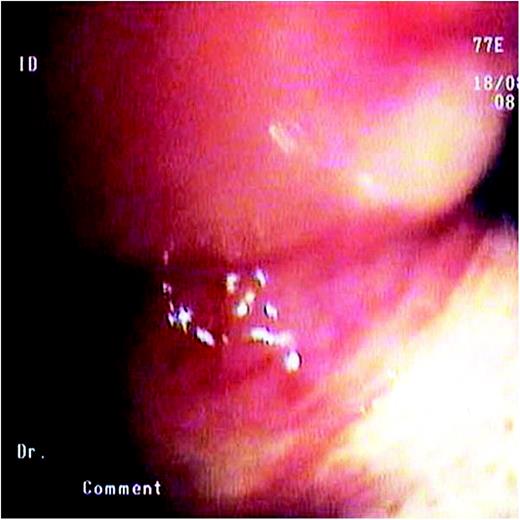
In the same endoscopic alteration the ‘MIX’ technology shows the vascolarization of lesion in one single image. MIX, Multiple Image Xposition.
SAFE-3000 autofluorescence videobronchoscope. This system allows bronchial visualization by white light and autofluorescence separately (B) and by ‘Twin Mode’ and ‘MIX’ technologies (C). A, up and down; D, picture capture; E, aspirator. MIX, Multiple Image Xposition.
2.2. Statistical analysis
Analysis was performed using SPSS 10.0. Data were entered into a data base using SPSS Data Entry II (SPSS Inc, Chicago, IL, USA) and were expressed as mean±and standard deviation (S.D.). We tested the ability of ‘Twin’ and ‘MIX’ technologies in early finding premalignant and malignant lesions. The McNemar test was used for analysis of variance. The sensitivity and the specificity were evaluated by Byte test. All P-values <0.05 were considered to indicate significance and confidence interval (CI) at 95%.
2.3. Follow-up of dysplasia
Patients underwent SAFE-3000 AFB and bronchial biopsies at two, four and eight months for moderate dysplasia and at two and four months for severe dysplasia. Progression or persistence to high-grade lesions led to pulmonary excision.
2.4. Follow-up of CIS and early invasive cancer
Patients were monitored with monthly chest X-rays for the first four months and then at 12 months from intervention; computed tomography (CT) of the thorax by month 6; CT total-body every 12 months from the second year; SAFE-3000 AFB at month 12.
3. Results
The visual endoscopic results were as follow: a) mucosa thickening with a light increase of blood flow (visual score 2: 15 patients, 9%); b) suspicious area with a localized increase of blood flow (visual score 3: 79 patients, 47%). In three patients (1.8%) there were differences in visual score between ‘Twin Mode’ (classified 2) and ‘MIX’ (classified 3) technologies. Six patients (3.5%) did not show mucosa abnormalities (visual score 1), so mucosa biopsy was not done. The AFB highlighted in 65 patients (38.7%) an endobronchial vegetative mass (visual score 4). Seventy-one patients (42%) with visual score of 1 and 4 were excluded from the study, that was performed in 97 patients (58%) with visual score of 2 and 3. The anatomo-pathological evaluation of 388 bronchial biopsies carried out in 97 patients has shown a normal mucosa in 11 patients (11%), four benign lesions (4%), 27 premalignant lesions (28%) and 55 malignant lesions (57%). No complications were highlighted during the procedure. Table 2 showed that no patients classified 3 displayed a normal histology but three patients classified 2 by ‘Twin’ were neoplastic. ‘Twin Mode’ allowed us to obtain positive biopsies performed for malignant and premalignant lesions in 79 out of 82 patients. In three patients with visual score discrepancy between ‘Twin Mode’ and ‘MIX’ modality (2 vs. 3 score, respectively) we found one CIS and two adenocarcinomas by the ‘MIX’ technology biopsies only. Among the 32 early invasive cancers at stage IA (T1a N0M0) [6], 19 were squamous cell carcinomas (Fig. 4 ) and 13 adenocarcinomas. Seventy patients with a severe dysplasia still evident at endoscopic check performed at the second and the forth month, a CIS or lung cancer underwent lobectomy. The average time of hospitalization was 6±2 days. Postoperative histological evaluations confirmed the preoperative bronchial diagnosis. The follow-up after 10 months does note metastasis. Twelve patients with moderate dysplasia revealed a stabilization of lesions at eight months.
Histological diagnosis of bronchial biopsies
| Pathological results | Patients | Percentage | Pre-biopsy visual score |
| Normal | 11 | 11% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Bronchitis | 3 | 3% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Tuberculosis | 1 | 1% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Moderate dysplasia | 12 | 13% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Severe dysplasia | 15 | 15% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Carcinoma in situ | 23 | 24% | 3 |
| Detected by ‘MIX’ | |||
| only in one patients | |||
| Early invasive carcinoma | 32 | 33% | 3 |
| Detected by ‘MIX’ | |||
| only in two patients | |||
| Total | 97 | 100% | – |
| Pathological results | Patients | Percentage | Pre-biopsy visual score |
| Normal | 11 | 11% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Bronchitis | 3 | 3% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Tuberculosis | 1 | 1% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Moderate dysplasia | 12 | 13% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Severe dysplasia | 15 | 15% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Carcinoma in situ | 23 | 24% | 3 |
| Detected by ‘MIX’ | |||
| only in one patients | |||
| Early invasive carcinoma | 32 | 33% | 3 |
| Detected by ‘MIX’ | |||
| only in two patients | |||
| Total | 97 | 100% | – |
Histological diagnosis of bronchial biopsies
| Pathological results | Patients | Percentage | Pre-biopsy visual score |
| Normal | 11 | 11% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Bronchitis | 3 | 3% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Tuberculosis | 1 | 1% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Moderate dysplasia | 12 | 13% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Severe dysplasia | 15 | 15% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Carcinoma in situ | 23 | 24% | 3 |
| Detected by ‘MIX’ | |||
| only in one patients | |||
| Early invasive carcinoma | 32 | 33% | 3 |
| Detected by ‘MIX’ | |||
| only in two patients | |||
| Total | 97 | 100% | – |
| Pathological results | Patients | Percentage | Pre-biopsy visual score |
| Normal | 11 | 11% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Bronchitis | 3 | 3% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Tuberculosis | 1 | 1% | 2 |
| ‘Twin’ and ‘MIX’ | |||
| Moderate dysplasia | 12 | 13% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Severe dysplasia | 15 | 15% | 3 |
| ‘Twin’ and ‘MIX’ | |||
| Carcinoma in situ | 23 | 24% | 3 |
| Detected by ‘MIX’ | |||
| only in one patients | |||
| Early invasive carcinoma | 32 | 33% | 3 |
| Detected by ‘MIX’ | |||
| only in two patients | |||
| Total | 97 | 100% | – |
Squamous cell carcinoma. The diagnosis of malignancy is based on cell atypia and invasiveness.
3.1. Statistical analysis
McNemar test did not demonstrate a statistically relevant difference between ‘Twin’ and ‘MIX’ modalities as regards early detection of premalignant and malignant lesions. ‘Twin Mode’ sensitivity was lower than ‘MIX’ one (P=0.001), while the specificity was the same. The positive predictive value, the negative predictive value and the diagnostic accuracy did not point out a statistically relevant difference (Table 3 ).
SAFE-3000 statistical evaluation of endoscopic double procedure
| Parameters | Twin | MIX | P-value |
| Sensitivity | 96% | 100% | <0.001 |
| 316/328 biopsies | 328/328 biopsies | ||
| Specificity | 60% | 60% | 0.146 |
| 36/60 biopsies | 36/60 biopsies | ||
| Positive predictive value | 90% | 90% | 0.268 |
| 316/352 biopsies | 328/364 biopsies | ||
| Negative predictive value | 67% | 100% | 0.156 |
| 24/36 biopsies | 24/24 biopsies | ||
| Diagnostic accuracy | 88% | 91% | 0.198 |
| 340/388 biopsies | 352/388 biopsies |
| Parameters | Twin | MIX | P-value |
| Sensitivity | 96% | 100% | <0.001 |
| 316/328 biopsies | 328/328 biopsies | ||
| Specificity | 60% | 60% | 0.146 |
| 36/60 biopsies | 36/60 biopsies | ||
| Positive predictive value | 90% | 90% | 0.268 |
| 316/352 biopsies | 328/364 biopsies | ||
| Negative predictive value | 67% | 100% | 0.156 |
| 24/36 biopsies | 24/24 biopsies | ||
| Diagnostic accuracy | 88% | 91% | 0.198 |
| 340/388 biopsies | 352/388 biopsies |
SAFE-3000 statistical evaluation of endoscopic double procedure
| Parameters | Twin | MIX | P-value |
| Sensitivity | 96% | 100% | <0.001 |
| 316/328 biopsies | 328/328 biopsies | ||
| Specificity | 60% | 60% | 0.146 |
| 36/60 biopsies | 36/60 biopsies | ||
| Positive predictive value | 90% | 90% | 0.268 |
| 316/352 biopsies | 328/364 biopsies | ||
| Negative predictive value | 67% | 100% | 0.156 |
| 24/36 biopsies | 24/24 biopsies | ||
| Diagnostic accuracy | 88% | 91% | 0.198 |
| 340/388 biopsies | 352/388 biopsies |
| Parameters | Twin | MIX | P-value |
| Sensitivity | 96% | 100% | <0.001 |
| 316/328 biopsies | 328/328 biopsies | ||
| Specificity | 60% | 60% | 0.146 |
| 36/60 biopsies | 36/60 biopsies | ||
| Positive predictive value | 90% | 90% | 0.268 |
| 316/352 biopsies | 328/364 biopsies | ||
| Negative predictive value | 67% | 100% | 0.156 |
| 24/36 biopsies | 24/24 biopsies | ||
| Diagnostic accuracy | 88% | 91% | 0.198 |
| 340/388 biopsies | 352/388 biopsies |
4. Discussion
The preclinic diagnosis of lung cancer is the basic principle for a radical surgical treatment and a good prognosis, even if there is a debated relationship between the diameter of cancer and survival. Gajra et al. [7] studied 246 patients with NSCLC stage IA and treated with excision. The diameter of neoplasm was ≤1.5 cm in 86 patients and between 1.6 and 3 cm in 160 patients. Survival at five years was 85.5% in the first group and 78.6% in the second one, with a disease-free survival (DFS) equal to 81.5 and 70.9%, respectively. Casali et al. [8], in a retrospective analysis carried out on 548 patients with NSCLC stage I treated with radical surgery, demonstrated that mortality is 57% higher in cancers with a diameter between 2 and 5 cm than in lesions <2 cm; this proportion was 60% higher in cancer with a diameter >5 cm compared to a lesion with a diameter between 2 and 5 cm. Li et al. [9] highlighted that the five-year survival of patients with tumour size <2 cm and of those with a lesion >7 cm was, respectively, 75.49 and 46.15% while the five-year DFS was 67.65 and 30.77%. It is obvious that the NSCLC excision at stage I can be considered the right instrument to obtain a complete recovery of patient. Unfortunately, only a minority of patients are diagnosed and treated at the curable stage. Our study shows that the advent of AFB SAFE-3000 allows more accurate detection of premalignant lesions and early stage invasive cancer. The technical innovation compared with previous models is represented by ‘Twin Mode’ and ‘MIX’ technologies that improve the performance of endoscopic procedure and its diagnostic accuracy. Airway exploration at the asset by ‘Twin Mode’ ensures tracheobronchial cleaning, avoiding the image alteration and localizing occulted cancer. The ‘MIX’ modality in the second one determines the dimension of lesion and targets biopsy. The possibility of comparing in real time, during the examination, synchronous images in AFB and WLB one next to the other (‘Twin Mode’) emphasizes each mucosa abnormality and identifies the site of bronchial biopsies. In addition to this, the interaction of these procedures (‘MIX’) allows to amplify premalignant and malignant lesions characteristics highlighting both morphological and topographical aspects. Ikeda et al. [10] have demonstrated that the sensitivity for CIS and dysplasia was 65% with WLB and 90% with SAFE-3000. Bota et al. [11] evaluated over two years the histological modifications of 27 severe dysplasia and 32 CIS with the lung imaging fluorescence endoscopy. In the first group, the 37% of patients shows the stabilization of the lesion, the 41% changes to normal and the 22% regressed to low-grade dysplasia. In the second group, 25 patients were treated at three months, five changed to a no dysplastic state and two to a moderate dysplastic state. At 24 months, two patients display recurrence of CIS, two low-grade lesions and three regressed to normal. The study suggests that the fluorescence endoscopy was necessary for the follow-up and treatment of different bronchial epithelium lesions. Our experience reveals that high-grade and low-grade lesions remained stable during follow-up. The increased sensitivity of SAFE-3000 system makes this instrument unique and essential in premalignant lesions follow-up, as these lesions need repeated bronchoscopic checks even if biopsies are negative. The possible stabilization in severe dysplasia or the development into carcinoma are rapidly detected allowing immediate treatment. The disadvantage of this new AFB model as regards conventional bronchoscopy is the lower specificity (60% in our study), related to the big number of mucosa alterations. Lee et al. [12], analysing 48 suspected bronchial carcinoma patients with SAFE-3000 (Pentax, Tokio), detected different levels of dysplasia in 22 bronchial biopsies among 126 of them, with a sensitivity and specificity rate of 86 and 94%. Although the relationship between endoscopic findings and histological results was statistically significant (r=0.77; P<0.0001), the length of the examination was too long (nine minutes per patient). In our experience, the procedural time was <five minutes, in order to avoid bronchospasm and respiratory distress. In addition, we experienced no airway bleeding following biopsies. The most characteristic point of the SAFE-3000 is its procedural simplicity, that reducing the duration of the examination and the number of complications. The results are linked to both technology combinations, which can to be employed easily in the same session. The capture of lesion extent is defined precisely; the multiple endobronchial biopsies are carried out based on the accurate visualization of the abnormal vascularization. Then, the optimal representation of the surfaces displays the best place for taking biopsy specimens. The diagnostic yield and the benefit to the patients are improved.
5. Conclusions
SAFE-3000 improves early detection of premalignant and malignant lesions by the complementarity of two image modalities and by the excellent bronchial mucosa representation. Even if the diagnostic accuracy of biopsies is strictly tied to the experience of the endoscopist, this system allows localization of the correct area for biopsies because of its high level of resolution. The ‘MIX’ modality leads to a marked improvement in sensitivity and better patient safety. The only disadvantage, in this period of budget reduction in the Health Service, is its high cost (€ 150.000) while there are no further costs for cleaning, preparation of material and maintenance. Although clinical data about the new videobronchoscope examination techniques do not exist in literature, we advice the routine use of SAFE-3000 as a screening for lung cancer.

{kind=link}
{kind=link}
{kind=link}
{kind=link}