
Abstract
Airway calibre is an important determinant of air flow and respiratory work both at rest and during exercise. While much is understood about control of airway calibre at rest, less is known about the dynamics and changes in airway resistance during exercise, especially in those with asthma. This article provides an overview of the current understanding provided by the literature that has addressed airway resistance during exercise in normal non-asthmatic individuals and in those with asthma.
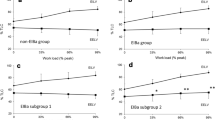
There are many interesting studies that provide some insight into this issue. In general, non-asthmatic individuals appear to have near maximally or maximally dilated airways at rest and, thus, have little change associated with exercise, at least during short duration exercise of <15 minutes. However, potent bronchodilating influences are in operation during the exercise as shown by exercise data from normal subjects with pharmacologically pre-constricted airways. In contrast, dynamic exercise has consistently demonstrated improved airway calibre in asthmatic individuals. Again, the exercise has typically been <15 minutes. Data from longer duration exercise (20–30 minutes) are lacking in normal subjects but suggest declining pulmonary function over time during exercise in asthmatic individuals after the initial bronchodilation. However, the lack of non-asthmatic controls and small subject numbers in these studies leave much remaining to be studied in this regard. Handgrip exercise in asthmatic individuals also elicits bronchodilation raising interesting questions as to potential mechanisms.
Isocapnic voluntary hyperpnoea matched to exercise hyperpnoea levels induces bronchodilation in asthmatic individuals during both short- and longer-term bouts up to 20 minutes. This result in longer-term isocapnic hyperpnoea apparently deviates from the response of asthmatic individuals to the hyperpnoea of longer-term dynamic exercise raising interesting questions. Voluntary hyperpnoea is important to this discussion as this technique is often used to assess the prevalence of exercise-induced asthma.
While much is yet to be understood, dynamic, and possibly isometric, exercise is a powerful bronchodilator, at least over a short period of up to 15 minutes. It remains to be determined how airways respond to dynamic exercise of >15 minutes in both normal and asthmatic individuals and the mechanisms operating in the various circumstances. Additionally, attention to resting pulmonary function in asthmatic individuals must be given as those with constricted airways may differ in response to exercise, or to voluntary hyperpnoea, from those with normal airway function at rest.





Similar content being viewed by others

References
DuBois AB, Botelho SY, Comroe JH. A new method for measuring airway resistance in man using a body plethysmograph: values in normal subjects and in patients with respiratory disease. J Clin Invest 1956; 35: 327–335
Stubbing DG, Pengelly LD, Morse JL, et al. Pulmonary mechanics during exercise in subjects with chronic airflow obstruction. J Appl Physiol 1980; 49: 511–515
Stubbing DG, Pengelly LD, Morse JL, et al. Pulmonary mechanics during exercise in normal males. J Appl Physiol 1980; 49: 506–510
Kagawa J, Kerr HD. Effects of brief graded exercise on specific airway conductance in normal subjects. J Appl Physiol 1970; 28: 138–144
Michaelsen ED, McDonnell J, Morgan W, et al. Pulmonary mechanics by spectral analysis of forced random noise. J Clin Invest 1975; 56: 1210–1230
Johnson BD, Beck KC, Zeballos RJ, et al. Advances in pulmonary laboratory testing. Chest 1999; 116: 1377–1387
Goldman MD. Clinical application of forced oscillation. Pulm Pharmacol Ther 2001; 14: 341–350
Arets HGM, Brackel HJL, Van der Ent CK. Applicability of interrupter resistance measurements using the MicroRint™ in daily practice. Respir Med 2003; 97: 366–374
Delacourt C, Lorino H, Fuhrman C, et al. Comparison of the forced oscillation technique and the interrupter technique for assessing airway obstruction and its reversibility in children. Am J Respir Crit Care Med 2001; 164: 965–972
Bovino MJ, Rundell KW, Baumann JM, et al. Airway resistance and maximal expiratory flow during exercise [abstract]. Med Sci Sports Exerc 2004; 36: S227
de Bisschop C, Pichon A, Guenard H, et al. Accounting for flow dependence of respiratory resistance during exercise. Respir Physiol Neurobiol 2003; 136: 65–76
Beck KC, Hyatt RE, Mpougas P, et al. Evaluation of pulmonary resistance and maximal expiratory flow measurements during exercise in humans. J Appl Physiol 1999; 86: 1388–1395
Mead J, Gaensler EA. Esophageal and pleural pressures in man: upright and supine. J Appl Physiol 1959; 14: 81–83
Burns CB, Taylor WR, Ingram RH. Effects of deep inhalation in asthma: relative airway and parenchymal hysteresis. J Appl Physiol 1985; 59: 1590–1596
Marthan R, Woolcock AJ. Is a myogenic response involved in deep inspiration-induced bronchoconstriction in asthmatics? Am Rev Respir Dis 1989; 140: 1354–1358
Briscoe WA, DuBois AB. The relationship between airway resistance, airway conductance and lung volume in subjects of different age and body size. J Clin Invest 1958; 37: 1279–1285
Vincent NJ, Knudson R, Leith DE, et al. Factors influencing pulmonary resistance. J Appl Physiol 1970; 29: 236–243
Clement J, Bobbaers H, Van de Woestijne KP. Influence of flow amplitude on pulmonary resistance determined near zero flow. Respir Physiol 1980; 41: 61–69
Johnson BD, Weisman IM, Zeballos RJ, et al. Emerging concepts in the evaluation of ventilatory limitation during exercise: the exercise tidal flow-volume loop. Chest 1999; 116: 488–503
Verges S, Devouassoux G, Flore P, et al. Bronchial hyperresponsiveness, airway inflammation, and airflow limitation in endurance athletes. Chest 2005; 127: 1935–1941
Costello RW, Fryer AD. Cholinergic mechanisms in asthma. In: Barnes PJ, Gruenstein MM, Left AR, et al., editors. Asthma. New York: Lippincott-Raven, 1997: 965–984
Pichon A, Roulaud M, Denjean A, et al. Airway tone during exercise in healthy subjects: effects of salbutamol and ipratropium bromide. Int J Sports Med 2005; 26: 321–326
Warren JB, Jennings SJ, Clark TJ. Effect of adrenergic and vagal blockade on the normal human airway response to exercise. Clin Sci (Lond) 1984; 66: 79–85
Warren JB, Dalton N. A comparison of the bronchodilator and vasopressor effects of exercise levels of adrenaline in man. Clin Sci (Lond) 1983; 64: 475–479
Melillo E, Woolley KL, Manning PJ, et al. Effect of inhaled PGE2 on exercise-induced bronchoconstriction in asthmatic subjects. Am J Respir Crit Care Med 1994; 149: 1138–1141
Walters EH, Bevan C, Parrish RW, et al. Time-dependent effect of prostaglandin E2 inhalation on airway responses to bronchoconstrictor agents in normal subjects. Thorax 1982; 37: 438–442
Dahlen B, Roquet A, Inman MD, et al. Influence of zafirlukast and loratadine on exercise-induced bronchoconstriction. J Allergy Clin Immunol 2002; 109: 789–793
Anderson SD, Brannan ID. Exercise-induced asthma: is there still a case for histamine? J Allergy Clin Immunol 2002; 109: 771–773
Finnerty JP, Holgate ST. The contribution of histamine release and vagal reflexes, alone and in combination, to exercise-induced asthma. Eur Respir 11993; 6: 1132–1137
Bousquet I, Godard P, Michel FB. Antihistamines in the treatment of asthma. Eur Respir 11992; 5: 1137–1142
Suman OE, Morrow ID, O’Malley KA, et al. Airway function after cyclooxygenase inhibition during hyperpnea-induced bronchoconstriction in guinea pigs. J Appl Physiol 2000; 89: 1971–1978
Suman OE, Beck KC. Role of airway endogenous nitric oxide on lung function during and after exercise in mild asthma. J Appl Physiol 2002; 93: 1932–1938
Gotshall RW. Exercise-induced bronchoconstriction. Drugs 2002; 62: 1725–1739
Gilbert R, Auchincloss JH. Mechanics of breathing in normal subjects during brief, severe exercise. J Lab Clin Med 1969; 73: 439–450
Granath A, Horie E, Linderholm H. Compliance and resistance of the lungs in the sitting and supine positions at rest and during work. Scand J Clin Lab Invest 1959; 11: 226–234
Irnell L, Swartling S. Maximal expiratory flow at rest and during muscular work in patients with bronchial asthma. Scand J Respir Dis 1966; 47: 103–113
Stirling DR, Cotton DI, Graham BL, et al. Characteristics of airway tone during exercise in patients with asthma. J Appl Physiol 1983; 54: 934–942
Lefcoe NM. The time course of maximum ventilatory performance during and after moderately heavy exercise. Clin Sci 1969; 36: 47–52
Taylor EA, Trembath PW, Warrington SI. Influence of environmental temperature and humidity on bronchial responses during assessment of selectivity of beta-adrenoceptor antagonists in man. Br J Clin Pharmacol 1981; 12: 201–209
Freedman S. Exercise as a bronchodilator. Clin Sci (Lond) 1992; 83: 383–389
Freedman S, Lane R, Gillett MK, et al. Abolition of methacholine induced bronchoconstriction by the hyperventilation of exercise or volition. Thorax 1988; 43: 631–636
Marshall R, Mcllroy MB. The mechanical properties of the lungs in asthma. Clin Sci (Lond) 1956; 15: 345–351
Lane R, Freedman S, Guz A. A method for the continuous measurement and display of pulmonary resistance in man. Clin Sci (Lond) 1993; 84: 671–673
Eengstrom I, Karlberg P, Kraepelien S, et al. Respiratory studies in children VIII: respiratory adaptation during excercise tolerance test with special reference to mechanical properties of the lungs in asthmatic and healthy children. Acta Paediatr 1960; 49: 850–858
Todaro A. Exercise-induced bronchodilatation in asthmatic athletes. J Sports Med Phys Fitness 1996; 36: 60–66
Beck KC, Offord KP, Scanlon PD. Bronchoconstriction occurring during exercise in asthmatic subjects. Am J Respir Crit Care Med 1994; 149: 352–357
Suman OE, Babcock MA, Pegelow DF, et al. Airway obstruction during exercise in asthma. Am J Respir Crit Care Med 1995; 152: 24–31
Suman OE, Beck KC, Babcock MA, et al. Airway obstruction during exercise and isocapnic hyperventilation in asthmatic subjects. J Appl Physiol 1999; 87: 1107–1113
Crimi E Pellegrino R, Smeraldi A, et al. Exercise-induced bronchodilation in natural and induced asthma: effects on ventilatory response and performance. J Appl Physiol 2002; 92: 2353–2360
Fontana GA, Pantaleo T, Lavorini F, et al. Handgrip-induced airway dilation in asthmatic patients with bronchoconstriction induced by MCh inhalation. J Appl Physiol 2002; 93: 1723–1730
Karjalainen EM, Laitinen A, Sue-Chu M, et al. Evidence of airway inflammation and remodeling in ski athletes with and without bronchial hyperresponsiveness to methacholine. Am J Respir Crit Care Med 2000; 161: 2086–2091
Acknowledgements
No sources of funding were used to assist in the preparation of this review. The author has no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gotshall, R.W. Airway Response during Exercise and Hyperpnoea in Non-Asthmatic and Asthmatic Individuals. Sports Med 36, 513–527 (2006). https://doi.org/10.2165/00007256-200636060-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00007256-200636060-00005