





Abstract
In asthma patients, magnetic resonance imaging (MRI) and the lung clearance index (LCI) have revealed persistent ventilation heterogeneity, although its relationship to asthma control is not well understood. Therefore, our goal was to explore the relationship of MRI ventilation defects and the LCI with asthma control and quality of life in patients with severe, poorly controlled asthma.
18 patients with severe, poorly controlled asthma (mean±sd 46±12 years, six males/12 females) provided written informed consent to an ethics board approved protocol, and underwent spirometry, LCI and 3He MRI during a single 2-h visit. Asthma control and quality of life were evaluated using the Asthma Control Questionnaire (ACQ) and Asthma Quality of Life Questionnaire (AQLQ). Ventilation heterogeneity was quantified using the LCI and 3He MRI ventilation defect percent (VDP).
All participants reported poorly controlled disease (mean±sd ACQ score=2.3±0.9) and highly heterogeneous ventilation (mean±sd VDP=12±11% and LCI=10.5±3.0). While VDP and LCI were strongly correlated (r=0.86, p<0.0001), in a multivariate model that included forced expiratory volume in 1 s, VDP and LCI, VDP was the only independent predictor of asthma control (R2=0.38, p=0.01). There was also a significantly worse VDP, but not LCI in asthma patients with an ACQ score >2 (p=0.04) and AQLQ score <5 (p=0.04), and a trend towards worse VDP (p=0.053), but not LCI in asthma patients reporting ≥1 exacerbation in the past 6 months.
In patients with poorly controlled, severe asthma MRI ventilation, but not LCI was significantly worse in those with worse ACQ and AQLQ.
Abstract
MRI ventilation defects, but not LCI, are worse in patients with worse asthma control and asthma-related QoL http://ow.ly/4n9uip
Introduction
The primary goal of asthma therapy is to achieve and maintain disease control. Unfortunately, ∼50% of asthma patients remain poorly controlled with up to 10% of these patients experiencing life-threatening exacerbations [1]. The clinical and pathophysiological findings in poorly controlled asthma are heterogeneous, which makes treatment decisions complex. Previous work suggested that poor asthma control may be related to ventilation heterogeneity [2, 3]. Although the pathophysiological abnormalities responsible for ventilation heterogeneity are unclear, these may include luminal inflammation, mucus, albumin and fibrin, thickening of the airway walls, smooth muscle hyperplasia/hypertrophy, and mucous cell metaplasia. Ventilation heterogeneity measured using the lung clearance index (LCI) was first described over 65 years ago [4], and has endured as a measure of obstructive lung disease. Ventilation heterogeneity in asthma patients is elevated compared with healthy controls [5–7], is an independent determinant of airway hyperresponsiveness [8], improves with bronchodilation [5, 9] and inhaled corticosteroids [3, 10], and worsens during exacerbations [11].
Ventilation heterogeneity may be regionally identified and visualised using pulmonary imaging methods [12, 13] including inhaled gas magnetic resonance imaging (MRI) [14]. In asthma patients, MRI ventilation defects are temporally and spatially persistent [15], worsen in response to bronchoconstriction, and improve following bronchodilation [16]. MRI ventilation defects were also observed to be greater in number and size in older asthma patients with worse lung function and worse airway inflammation, hyperresponsiveness and airway wall thickness [17].
Until now, however, the relationship between ventilation defects and asthma control and quality of life has not been ascertained. Hyperpolarised noble gas MRI might have particular application in the evaluation of the peripheral airways in patients with severe asthma, because it provides regional information not provided by clinically available measurements. Therefore, the purpose of this study was to determine the relationship of MRI and LCI measurements of ventilation heterogeneity with asthma control, quality of life and exacerbations. We hypothesised that MRI ventilation defects and the LCI would be related to asthma control and quality of life in severe asthma patients, which is important because currently there are few intermediate end-points of asthma control that can be used to guide therapy.
Materials and methods
Study participants and design
Participants provided written informed consent to a protocol approved by a local research ethics board that was also registered (The University of Western Ontario Health Sciences Research Ethics Board, London, Canada, approval number 104200; clinicaltrials.gov identifier number NCT02263794). Patients between 18 and 70 years of age with a diagnosis of severe asthma, according to the Global Initiative for Asthma (GINA) treatment step criteria [18], and under the care of a respirologist were recruited from two academic tertiary care centres (Firestone Institute for Respiratory Health, McMaster University, Hamilton, ON, Canada and Robarts Research Institute, The University of Western Ontario, London, ON, Canada).
During a single 2-h visit, all participants performed pre- and post-bronchodilator spirometry, LCI and MRI. Asthma control and quality of life were assessed using the Asthma Control Questionnaire (ACQ; seven-item version) [19] and Standardised Asthma Quality of Life Questionnaire (AQLQ(S)) [20], respectively. Borg and modified Medical Research Council dyspnoea scores were recorded. Clinical history of severe asthma exacerbations, emergency department visits and hospitalisations for respiratory symptoms were self-reported. As previously defined [21], a severe asthma exacerbation was a worsening of symptoms requiring treatment with oral or intravenous corticosteroids, or a doubling of inhaled corticosteroid (ICS) dose for ≥3 days, or any temporary increase in the dosage of oral corticosteroids (OCS) for subjects taking maintenance OCS. Methacholine challenge was performed within the 6 months prior to the study visit to determine the provocative concentration resulting in a ≥20% decrease in forced expiratory volume in 1 s (FEV1).
Spirometry, bronchial challenge and LCI
Spirometry was performed according to American Thoracic Society/European Respiratory Society guidelines [22] using a MedGraphics Elite Series plethysmograph (MedGraphics, St. Paul, MN, USA). For post-bronchodilator measurements, four 100 μg doses of Novo-Salbutamol HFA (Teva Novopharm Ltd., Toronto, ON, Canada) were delivered through a pressurised metered dose inhaler using an AeroChamber Plus spacer (Trudell Medical International; London, ON, Canada). All participants were instructed to withhold short-acting β-agonists for 12 h prior to their visit (overnight).
LCI measurements were acquired using 100% oxygen for nitrogen washout and the ndd EasyOne Pro LAB system (ndd Medical Technologies, Zurich, Switzerland) equipped with an ultrasonic flow and molar mass sensor. With the volunteer seated upright, the washout phase was initiated by switching from room air to 100% oxygen at end expiration. Tidal breathing of 100% oxygen was performed until the expired nitrogen concentration was <2.5% of the concentration at the start of the test. Functional residual capacity (FRC) was calculated from the cumulative volume of expired nitrogen divided by the difference between the end-tidal concentration at the start and end of the washout. The cumulative expired volume (CEV) was the cumulative volume of expired air during the washout. LCI was generated as the number of FRC lung turnovers (generated as CEV divided by FRC) required for a nitrogen concentration <2.5% of the concentration at the start of the test, as previously described [23]. Multiple-breath washout was performed in duplicate and LCI was reported as the mean of two manoeuvres.
Image acquisition
Anatomical proton (1H) and hyperpolarised 3He ventilation magnetic resonance images were acquired within 5 min of one another using a 3T MRI system (General Electric Healthcare, Milwaukee, WI, USA), as previously described [24]. Subjects were instructed to inhale 1.0 L of gas (100% N2 for 1H MRI and a 3He/N2 mixture for 3He MRI) from FRC, and coronal images were acquired under breath-hold conditions. 3He gas was polarised to 40% (Polarean; HeliSpin, Durham, NC, USA) and diluted with nitrogen gas to 5 mL per kilogram of body weight.
Thoracic computed tomography (CT) volumes were acquired with a 64-slice Lightspeed VCT system (General Electric Healthcare, Milwaukee, WI, USA) with subjects in breath-hold after inhalation of 1.0 L of nitrogen gas from FRC as previously described [25]. Using the manufacturer's settings and the ImPACT CT patient dosimetry calculator (based on the UK Health Protection Agency NRPB-SR250 software), the total effective dose was 1.8 mSv.
Image analysis
Quantitative MRI evaluation was performed by a single trained observer (with 5 years’ experience) using semi-automated segmentation software as previously described [24]. 3He MRI ventilation defect percent (VDP) was generated as the ventilation defect volume normalised to the thoracic cavity volume [24]. Thoracic CT images were analysed using Pulmonary Workstation 2.0 (VIDA Diagnostics Inc., Coralville, IA, USA) to generate three-dimensional airway trees. To confirm the spatial relationship between a ventilation defect and the corresponding airway of interest, CT airway trees were manually registered to the MRI using 3D Slicer software (www.slicer.org).
Statistical methods
Data were tested for normality using the Shapiro–Wilk normality test and when data were not normal, nonparametric tests were performed. Univariate relationships were evaluated using linear regressions (r2), Pearson correlations (r), and when the data were not normal, Spearman correlations (ρ). To determine if VDP was an independent predictor of ACQ, AQLQ and exacerbations in the past 12 months, multivariate regression models were generated using the stepwise approach and SPSS 20.0 software (IBM, Armonk, NY, USA). To ascertain if VDP was an independent predictor of exacerbations in the past six months, a multivariate zero-inflated Poisson regression model was generated using the PROC COUNTREG procedure in SAS 9.4 software (SAS Institute, Cary, NC, USA). Unpaired t-tests and Mann–Whitney tests were performed to compare ventilation heterogeneity in subjects stratified by ACQ (≤2 or >2) and AQLQ scores (≥5 or <5) and previous 6-month exacerbation history (<1 or ≥1 exacerbations). All results were considered statistically significant when the probability of making a Type I error was <5% (p<0.05).
Results
Participant characteristics
Table 1 provides a summary for the 18 participants (nine from each academic tertiary care centre, six males/12 females, mean±sd 46±12 years) with severe asthma; the data for each participant is provided in table S1. The mean±sd duration of asthma was 31±15 years (range 7–57 years), pre-bronchodilator mean±sd FEV1 was 68±24% predicted (range 33–103% pred) and mean±sd FEV1/forced vital capacity was 65±15% (range 35–88%).
Study participant characteristics
Asthma medications and control parameters are summarised in table 2; a listing of these data is also provided in table S2. Despite receiving medium-to-high dose ICS and long-acting β-agonists (GINA treatment step 4–5) [18], all 18 participants had poorly controlled disease as evidenced by their ACQ score (mean±sd 2.3±0.9, range 1.0–4.3). Of these, eight participants (44%) were prednisone dependent (dosage ranging from 2.5 to 50 mg·day−1). One or more severe asthma exacerbations were reported by nine (50%) and 15 (83%) participants in the previous 6- and 12-months respectively.
Asthma medications and control
Ventilation heterogeneity and asthma control
Pre-bronchodilator measurements were used to evaluate the relationship between ventilation heterogeneity and asthma control, while post-bronchodilator ventilation heterogeneity measurements are provided in the supplementary material (figures S2 and S3). 3He MRI ventilation images co-registered to the corresponding 1H anatomical MRI for six representative participants show there were a greater number and volume of 3He MRI ventilation abnormalities in patients with a worse ACQ score (figure 1). As shown in table 1, for all participants, mean VDP was 12±11% (range=1–35%) and mean LCI was 10.5±3.0 (range=6.3–17.5). Data for the individual participants shows abnormal VDP and LCI in 13 participants, and a normal VDP and LCI or normal VDP and abnormal LCI in five asthma patients (table S1).

Hyperpolarised 3He magnetic resonance imaging (MRI) of representative patients with severe asthma. Centre coronal slice 3He MRI ventilation in blue co-registered to anatomical 1H MRI in grey-scale for six representative severe asthma patients. S07: 55 year-old female, forced expiratory volume in 1 s (FEV1)=77% pred, Asthma Control Questionnaire (ACQ)=1.4, lung clearance index (LCI)=9.7, ventilation defect percent (VDP)=2%; S17: 39 year-old female, FEV1=66% pred, ACQ=1.7, LCI=6.7, VDP=3%; S16: 48 year-old male, FEV1=78% pred, ACQ=2.3, LCI=8.6, VDP=8%; S06: 45 year-old male, FEV1=34% pred, ACQ=2.7, LCI=11.5, VDP=14%; S13: 56 year-old male, FEV1=34% pred, ACQ=3.1, LCI=17.5, VDP=33%; S04: 60 year-old female, FEV1=47% pred, ACQ=4.3, LCI=14.0, VDP=35%.
We evaluated the relationship of VDP with ACQ and AQLQ scores and previous exacerbations in three ways. First, we stratified patients by ACQ score (ACQ≤2, n=7 and ACQ>2, n=9), AQLQ score (AQLQ≥5, n=7 and AQLQ<5, n=9) and by the number of self-reported exacerbations in the past 6 months (<1 exacerbation, n=9 and ≥1 exacerbation, n=9) (figure S1). There was significantly worse VDP (18±13% versus 6±5%; p=0.04), but not LCI (11.2±3.6 versus 9.4±2.4; p=0.3), in the subgroup of asthma patients with ACQ scores >2. There was also significantly worse VDP (18±13% versus 6±5%; p=0.04), but not LCI (11.4±3.3 versus 9.1±2.6; p=0.2), in the subgroup of asthma patients with AQLQ scores <5. There was a trend towards worse VDP (17±13% versus 8±5%; p=0.053), but not LCI (11.2±3.8 versus 9.7±1.8; p=0.30), in asthma patients reporting ≥1 exacerbation in the past 6 months. There were similar results post-bronchodilator (figure S2). Secondly, as shown in figure 2, we also evaluated linear relationships for VDP with LCI and also with ACQ score. Figure 2 shows that VDP was correlated with LCI (r= −0.86, p<0.0001) and ACQ score (r=0.62, p<0.01), while there was a trend for a relationship between LCI and ACQ score (r= −0.49, p=0.052). Similar findings are also shown in figure S3 for the post-bronchodilator data. Finally, to ascertain the independent relationship of VDP with asthma control, a multivariate model was investigated using a step-wise approach with ACQ score as the dependent variable and VDP, LCI and FEV1 as independent variables (table 3). VDP was the only variable entered into the regression equation that was a significant determinant of the ACQ score (β=0.62, p=0.01). LCI and FEV1 did not enter into the equation at step two of the analysis. Multivariate analyses for AQLQ and exacerbations (at 6 and 12 months) were also not significant.

Relationship between ventilation heterogeneity and asthma control. a) Ventilation defect percent (VDP) was significantly correlated with lung clearance index (LCI) (r=0.86, p<0.0001). b) VDP was significantly correlated with Asthma Control Questionnaire (ACQ) (r=0.62, p=0.01). c) There was a trend for an LCI–ACQ correlation (r=0.49, p=0.052). Dotted lines indicate 95% confidence intervals.
Multivariate regression model explaining asthma control
Discussion
We tried to answer the question: is ventilation heterogeneity related to asthma control? To do this we evaluated MRI ventilation defects and LCI in 18 severe asthma patients. We observed that: 1) VDP and LCI were strongly correlated; 2) there was significantly worse VDP, but not LCI, in asthma patients with an ACQ score >2 and AQLQ score <5; and 3) in a multivariate model that included FEV1, VDP and LCI, VDP was the only independent predictor of asthma control.
Based on previous results, we hypothesised that MRI ventilation defects might be related to asthma control. This notion was strengthened because previous multiple-breath washout studies suggested that poor asthma control was related to increased ventilation heterogeneity [2, 3]. It is important to note that we do not think that LCI can be directly related to static inhaled MRI measurements of ventilation defects, because these manoeuvres probably measure different, but related, features. Given the number of mechanistic differences in the measurements themselves, we were surprised to observe such a strong correlation between VDP and LCI. In the case of airway narrowing or gas trapping, which are common in severe asthma, long time constants for lung filling and emptying are expected. Accordingly, it is important to consider the temporal resolution of both approaches relative to the time constants for lung segment filling and emptying. For example, inert gas washout measurements are made over a time-course of many minutes of normal tidal breathing. In contrast, MRI ventilation defects are typically measured during a single 8–10 s inhalation breath-hold providing a visual snapshot of where the inhaled gas goes in that time period. Therefore, LCI heterogeneity relates to longer time constants for lung emptying, while MRI ventilation heterogeneity as we measured it reflects delayed lung filling. It is important to note that regional fractional ventilation maps previously developed [26] probe 3He washout over ∼5 breaths (<0.5 min). The temporal resolution of this approach employed by Horn et al. [26] may better reflect LCI measurements made over a time-course of many minutes of normal tidal breathing. In addition to differences in temporal resolution, there may be differences in the apparent spatial resolution of the methods. In principle, LCI measurements may be influenced by any or all of the conducting and acinar lung zones [27]. For ventilation MRI, there is somewhat coarse spatial resolution (3×3×15 mm) and this may result in an underestimation of very small ventilation defects. Supporting this notion, subjects S07 and S14 reported relatively well-controlled disease (ACQ=1.4 and 1.0), but abnormal LCI and relatively homogeneous MRI ventilation (table S1). Another, previously proposed [27], explanation suggests that even small ventilation defects may increase LCI well beyond the upper-limit of normal, resulting in an overestimation of disease severity. Supporting this view, subject S07 had an abnormal LCI (9.7) and only a single small hypoventilated region observed with MRI (VDP=2%). Importantly, this 55 year-old female was prescribed oral prednisone (7.5 mg·day−1) and ICS (budesonide >1000 µg), and was relatively well-controlled (ACQ=1.4). Postural effects should also be considered when comparing VDP and LCI measurements, because the MRI was performed supine, whereas LCI measurements were acquired upright. In a previous study in children, gas trapping was increased in supine asthma patients, but this was not the case for nitrogen washout derived measurements of ventilation heterogeneity [28]. Regardless, to mitigate potential postural effects, including atelectasis, imaging was completed within 5 min, which effectively minimises these effects [29]. Finally, differences between the physical properties of the gases would certainly influence resistance to flow within the airways. Based on previously published estimates, the density of N2 and the 3He/N2 mixture is 1.101 kg·m−3 and 0.609 kg·m−3, respectively, and the estimated viscosity of N2 and the 3He/N2 mixture is 1.984×10−4 Poise and 1.993×10−4 Poise, respectively [30]. Comparing these estimates to that of air, which has a density and viscosity of 1.140 kg·m−3 and 2.064×10−4 Poise respectively, suggests that N2 may be a better approximation of air than the 3He/N2 mixture.
The most important observation stemming from this study was that VDP was the only independent predictor of asthma control. This finding was supported by significantly worse VDP in asthma patients with ACQ score >2 and AQLQ score <5, and a trend towards worse VDP in asthma patients with more frequent exacerbations. This was not observed using LCI measurements, perhaps because of the small sample size and/or because LCI is inherently less sensitive to the underlying pathophysiology determining asthma control. Our results using MRI contradict a previous ventilation imaging study using single photon emission computerised tomography (SPECT) that reported no relationship between ACQ score and ventilation [12]. The negative SPECT results may stem from the inherently low spatial resolution of SPECT or the small sample size, or perhaps because the asthma patients were relatively well-controlled.
Our main finding of ventilation defect correlations with asthma control is novel, and leads us to speculate about the possible mechanisms underlying this relationship. We think that ventilation defects may influence asthma control and symptoms because these defects directly reflect hyperresponsive airways that are steroid insensitive. In addition, the fact that ventilation defects and the LCI are strongly related in these patients also suggests that trapped gas, slow filling and slow emptying regions are all critical features in these patients. It is noteworthy that, in the asthma patients studied here, the magnitude of bronchodilator reversibility was strongly related to baseline VDP (r= −0.77, p=0.0002). Unfortunately, there were an insufficient number of patients eligible for methacholine challenge to investigate the relationship between baseline VDP and hyperresponsiveness.
Globally, asthma patients who are poorly controlled and corticosteroid insensitive pose a considerable management burden and complexity as well as an enormous healthcare burden [31]. Unfortunately, there are limited clinical, physiological or pathological data for these patients. Here we observed that ventilation defects and bronchodilatory response persisted and asthma was not adequately controlled in a small group of severe asthma patients, despite receiving large doses of ICS and/or OCS. Several possible mechanisms for corticosteroid insensitivity in asthma have been proposed [32], but the relationship between steroid insensitivity and ventilation defects has yet to be explored. In the current evaluation, despite receiving medium-to-high dose ICS and long-acting β2-agonist therapy, all 18 participants had poorly controlled disease suggesting treatment resistance. Of these, eight participants (44%) were prednisone dependent (dose ranging from 2.5 to 50 mg·day−1). Pre-bronchodilator VDP was not different between prednisone-dependent and prednisone-independent asthma patients (p=0.15, data not shown). However, there was a significantly greater improvement in VDP post-bronchodilator in prednisone-dependent patients (p=0.02, data not shown). In addition, as might be expected, the post-bronchodilator change in VDP was related to pre-bronchodilator VDP (r= −0.77, p=0.0002), such that patients with worse VDP improved the most. Taken together, these data lead us to postulate that in most asthma patients VDP is a measure of severity and regional airways disease, but in asthma patients with very poor control, VDP regionally identifies severely narrowed airways that are hyperresponsive and highly prone to closure and collapse. Such responses lead to the intolerable symptoms that accompany poor asthma control. This also suggests that, clinically, the severity and regional location of ventilation defects may be used to guide therapy and patient management decisions and perhaps to improve asthma control.
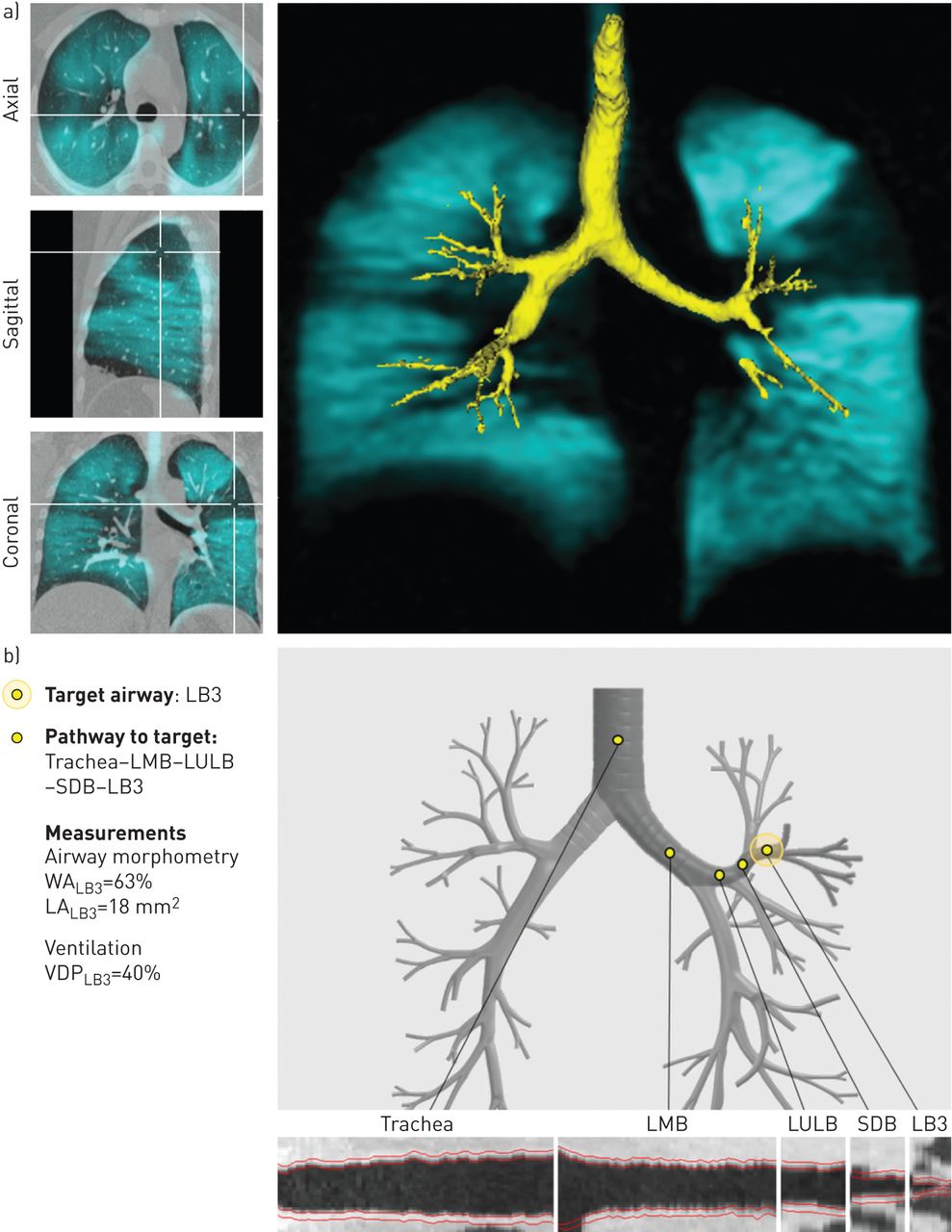
We think that treatment aimed at reducing ventilation defects may be used to improve control in severe asthma. To emphasise this point, an example of the spatial relationship between MRI ventilation defects and airways is shown in figure 3 for a representative asthma patient (S14) in whom all available drug treatments did not optimise control (table S2). Figure 3a shows a focal left upper lobe ventilation defect and its spatial relationship to the anterior segment of the left upper lobe. There was no evidence of right upper lobe or lower lobe ventilation abnormalities. In figure 3b, a graphical user interface intended for clinical use identifies the anterior segment of the left upper lobe, supplied by the LB3 segmental bronchus as well as quantitative measurements of LB3 morphometry and segmental VDP as a way to regionally guide and measure response to therapy.
{kind=link}
{kind=link}
{kind=link}
Identification of potential therapy targets using magnetic resonance imaging (MRI) for a representative severe asthma patient (S14). a) Co-registration of 3He MRI ventilation (shown in blue) and computed tomography (shown in grey-scale) with airway rendering (shown in yellow). A focal ventilation defect in the anterior segment of the left upper lobe is shown in the axial, sagittal and coronal views. b) A graphical user interface displays the spatial relationship between the left upper lobe ventilation defect and the LB3 segmental bronchus along with the endobronchial pathway to the potential therapy target; quantitative airway morphometry measurements for this patient's LB3 segmental bronchus and segmental ventilation defect percent (VDP) are also provided. LMB: left main bronchus; LULB: left upper lobe bronchus; SDB: superior division bronchus; LB3: left bronchus three; WA: wall area; LA: lumen area.
We recognise our study has a number of limitations, including the small number of study participants. While the sample size is small, we note that MRI ventilation measurements are highly sensitive to airway and inflammatory abnormalities and therefore significant differences may be detected using small sample sizes. It is important to point out that clinical translation of 3He MRI is unlikely and that more immediate clinical impact will derive from 129Xe MRI methods that are currently undergoing regulatory approval worldwide. We also acknowledge that asthma patients were recruited from two major tertiary care centres, so exhaled nitric oxide fraction and sputum inflammometry were not available for the majority of patients. If these were available, we could try to tease out the relative contribution of luminal inflammation to ventilation heterogeneity and asthma control. Furthermore, we did not (for logistical reasons) evaluate a comparator group of well-controlled asthma patients or asthma patients with more moderate disease although, in a previous study in well-controlled asthma patients, the relationship between ventilation defects and asthma severity was determined [17].
There is strong evidence that poor asthma control is associated with an increased risk of severe asthma events [33]. Currently, airway inflammation serves as an intermediate end-point of asthma control/exacerbations [34–36], as do airflow obstruction [37], respiratory system reactance [38], and to a lesser extent, ventilation heterogeneity [2, 3]. In a relatively small group of severe asthma patients, we observed that VDP was independently predictive of asthma control and this leads us to speculate that ventilation defects may also serve as an intermediate end-point of asthma control. The hypothesis that ventilation defects drive symptoms and asthma worsening still needs to be rigorously tested, as does the hypothesis that asthma treatment aimed at reducing ventilation defects significantly improves asthma control. However, based on the current study in severe, uncontrolled asthma patients, we consider ventilation defects as the “canary in the coal mine”, reflecting airways that are already narrowed and hyperresponsive and regionally identifying lung regions that are highly prone to bronchospasm, revealing the source of symptoms and acute worsening in these patients.
Acknowledgements
We thank M. Kjarsgaard (Firestone Institute for Respiratory Health, McMaster University, Hamilton, Canada) for clinical coordination and clinical database management, H. Lim (Firestone Institute for Respiratory Health, McMaster University, Hamilton, Canada) for identifying and characterising the patients, A. Wheatley (Robarts Research Institute, The University of Western Ontario, London, Canada) for production and dispensing of 3He gas and D. Reese (Robarts Research Institute, The University of Western Ontario, London, Canada) for MRI of research volunteers.
Footnotes
Editorial comment in: Eur Respir J 2016; 48: 294–296.
This article has supplementary material available from erj.ersjournals.com
Clinical trial: This study is registered at clinicaltrials.gov with identifier number NCT02263794.
Support statement: This research was undertaken, in part, thanks to salary funding from the Canada Research Chairs program support of P. Nair (Canada Research Chair in Inflammometry), Canadian Institutes of Health Research (CIHR) New Investigator Award support for G. Parraga and Canadian Respiratory Research Network support for S. Svenningsen. Ongoing research funding from a CIHR Operating Grant (MOP 201309) and pilot study funding from the Canadian Lung Association are also gratefully acknowledged. Funding information for this article has been deposited with FundRef.
Conflict of interest: None declared.
- Received February 22, 2016.
- Accepted April 13, 2016.
- Copyright ©ERS 2016
References










