Article Text

Abstract
Objectives Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide. Exposure to occupational hazards is an important preventable risk factor but the contribution of specific occupations to COPD risk in a general population is uncertain. Our aim was to investigate the association of COPD with occupation in the UK population.
Methods In 2006–2010, the UK Biobank cohort recruited 502 649 adults aged 40–69 years. COPD cases were identified by prebronchodilator forced expiratory volume in 1 s/forced vital capacity<lower limit of normal according to American Thoracic Society (ATS)/ European Respiratory Society (ERS) guidelines. Current occupations were coded using the Standard Occupational Classification (SOC) 2000. Prevalence ratios (PRs) and 95% CIs of COPD for each SOC-coded job were estimated using a robust Poisson model adjusted for sex, age, recruitment centre and lifetime tobacco smoking. Analyses restricted to never-smokers and non-asthmatics were also performed.
Results Of the 353 occupations reported by 228 614 current working participants, several showed significantly increased COPD risk. Those at highest COPD risk were seafarers (PR=2.64; 95% CI 1.59 to 4.38), coal mine operatives (PR=2.30; 95% CI 1.00 to 5.31), cleaners (industrial: PR=1.96; 95% CI 1.16 to 3.31 and domestic: PR=1.43; 95% CI 1.28 to 1.59), roofers/tilers (PR=1.86; 95% CI 1.29 to 2.67), packers/bottlers/canners/fillers (PR=1.60; 95% CI 1.15 to 2.22), horticultural trades (PR=1.55; 95% CI 0.97 to 2.50), food/drink/tobacco process operatives (PR=1.46; 95% CI 1.11 to 1.93), floorers/wall tilers (PR=1.41; 95% CI 1.00 to 2.00), chemical/related process operatives (PR=1.39; 95% CI 0.98 to 1.97), postal workers/couriers (PR=1.35; 95% CI 1.15 to 1.59), labourers in building/woodworking trades (PR=1.32; 95% CI 1.04 to 1.68), school mid-day assistants (PR=1.32; 95% CI 1.01 to 1.74) and kitchen/catering assistants (PR=1.30; 95% CI 1.10 to 1.53). Associations were similar in analyses restricted to never-smokers and non-asthmatics.
Conclusions Selected occupations are associated with increased COPD risk in a large cross-sectional population-based UK study. Further analyses should confirm the extent to which these associations reflect exposures still of concern and where strengthened preventive action may be needed.
- COPD
- Occupations
Statistics from Altmetric.com
What this paper adds
Occupational hazards are important and preventable risk factors for chronic obstructive pulmonary disease (COPD). However, the specific occupations at higher risk in the general population are still unclear.
We found in a large population-based study in the UK that several occupations are at higher risk for COPD, including some never reported before such as cleaners. The validity of our findings was confirmed in analyses restricted to never-smokers and non-asthmatics.
We will next investigate the underlying potential occupational causal agents to confirm the extent to which these associations reflect exposures still of concern and where strengthened preventive action may be needed.
Background
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality, morbidity and disability worldwide.1 Although tobacco smoking is a major risk factor, it has been estimated that about 15–20% of COPD cases is attributable to occupational exposures (ie, dusts, gas, vapours, fumes, fibres).2 ,3 This percentage may be as high as 50% among never-smokers.4–7
Exposure to occupational hazards is both avoidable and involuntary; therefore, it is essential for public health impact and ethical reasons to identify the occupations at higher risk of COPD in order to apply preventive interventions to eliminate or at least reduce the burden of work-related disease.
Several occupations have been associated with increased COPD risk in previous epidemiological studies, but few are established a priori high-risk occupations, in particular, coal mining, farming and work that entails exposure to silica (such as quarry workers or ceramic or construction workers), cotton dust or cadmium fume.8
Most work-related causes of COPD were identified through the study of selected, highly exposed occupational cohorts with available workplace exposure measurements, but often limited information on potential confounding factors, in particular smoking. In contrast, the population-based studies that were able to adjust for potential confounders lacked quantitative occupational exposure data and had limited power to detect significant risk effects for the large variety of low-exposed occupations that may occur in a general population.2 ,3 ,8
To address these limitations, we conducted a cross-sectional analysis to identify the occupations associated with higher risk of COPD nested in the large population-based UK Biobank cohort. The UK Biobank study gave us a unique opportunity to achieve our goal because of the large sample size (over half a million participants), a wide variety of occupations and exposure levels in different industry sectors, availability of spirometry data, and detailed information on potential confounders, in particular tobacco smoking.
Materials and methods
The UK Biobank study is a large population-based prospective cohort of over half a million men and women recruited between 2006 and 2010 throughout the UK.9 ,10 A random sample of adults aged 40–69 years were identified from lists of those registered with the National Health Service in Britain, and who lived within specified distances from 22 health assessment centres. The reported response rate to the baseline UK Biobank survey was low (503 325/9.2 million invited=5.47%).9 Baseline assessment included collection of extensive epidemiological data through computer-assisted self-administered questionnaire and face-to-face interview (including age, sex, lifetime smoking history, current employment and doctor-diagnosed asthma), and physical health measurements (including height, weight and spirometry).
Spirometry data and COPD definition
Among the 502 649 participants who completed the baseline questionnaire, 457 282 participants (91%) had lung function testing. All spirometric measures were performed in accordance with most of the ATS/ERS guidelines11 using a Vitalograph Pneumotrac 6800. The spirometer was calibrated at the start of each day using the Spirotrac software supplied with the spirometer. A 3L calibration syringe was attached to the spirometer flow head and ‘spirometry’ in Vox was selected. The serial number of the calibration syringe was entered in a pop-up window and on-screen instructions were then followed. A calibration record was maintained. The spirometry testers were healthcare technicians or nurses certified to conduct the assessments. The Assessment Centre Manager oversaw that all Assessment Centre staff worked in accordance with the Biobank spirometry protocol (available at https://biobank.ctsu.ox.ac.uk/crystal/docs/Spirometry.pdf). Participants were allowed up to three attempts to provide two reproducible manoeuvres. Spirometer software compared the reproducibility of the first two blows and, if acceptable (defined as a ≤5% difference in both forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1)), the Biobank spirometry protocol specified that a third blow was not required. No postbronchodilator measures were performed. This deviation from the ATS/ERS guidelines was a pragmatic compromise between ‘depth’ and ‘breadth’ due to both the high number of quantitative measurements performed in each participant of the UK Biobank study and the very large study sample size. Spirometry flow curves from a random representative sample of these manoeuvres were examined alongside their stored Vitalograph ‘error’ messages, and from this review, error messages that indicated acceptable expiratory manoeuvres were identified. These were: ‘Blank’ (ie, no error message), ‘Accept’, ‘Accept Below6sec’ (acceptable blow, with plateau, even though expiration time less than 6 s) and ‘Below6sec’ (expiration below 6 s, but no other error message in the manoeuvre). Although this deviates from the ATS/ERS guidelines, a recent publication has suggested that strict end-of-test criteria are the ones most likely to lead to rejection of satisfactory manoeuvres.12 The highest value of both FEV1 and FVC from acceptable curves was identified. Participants who had smoked tobacco or used inhalers 1 h prior to testing were excluded from our analysis.
COPD was defined as FEV1/FVC<lower limit of normal (LLN; ie, the 5% lower tail of the normal distribution of average predicted FEV1/FVC in a reference healthy population). We used the Hankinson equation to calculate the predicted values for FEV1/FVC.13
Employment status and job coding
Employment status was recorded at recruitment for 496 894 of the 502 649 participants (99%). Those currently employed (n=281 247) were interviewed by trained operators and asked to provide additional information (eg, industry type, specific job tasks) that allowed the spot coding of their job. The interviewers manually codified the collected job descriptions using the four-digit Standard Occupational Classification (SOC), V.2000,14 including 353 occupations occurring in the general population. To classify more detailed job titles within each four-digit SOC code, ad hoc seven-digit SOC codes were created. In detail, in the SOC classification, within each four-digit SOC code, more specific jobs are included and listed in the coding index (26 160 entries). As no specific SOC codes are assigned to them, ad hoc seven-digit codes were created by combining the corresponding four-digit SOC code and an arbitrary ordinal number (from 001 to 999) generated after ordering the detailed job titles alphabetically within each four-digit major job category.
In total, 18 322 free-text descriptions of current occupations could not be coded at the time of the interview, and one of the authors (SDM), after a manual quality control review (eg, spelling error check), automatically coded them into four-digit SOC codes using the Computer Assisted Structure COding Tool (CASCOT).15 In total, 11 751 four-digit SOC codes attained a CASCOT-generated coding quality score (certainty score) of ≥50% and so were retained for analyses as previously suggested.16
Our final study sample included the 228 614 participants with at least one acceptable spirometry from at least two attempts and a SOC coded current job as shown in the study flow diagram (figure 1). Only 32 participants had just one acceptable spirometry manoeuvre (0%) and sensitivity analyses showed that removal of this group did not alter our findings (data not shown), so they were included. In total, 68 449 (30%) participants had two acceptable manoeuvres, and 160 133 (70%) three or more.
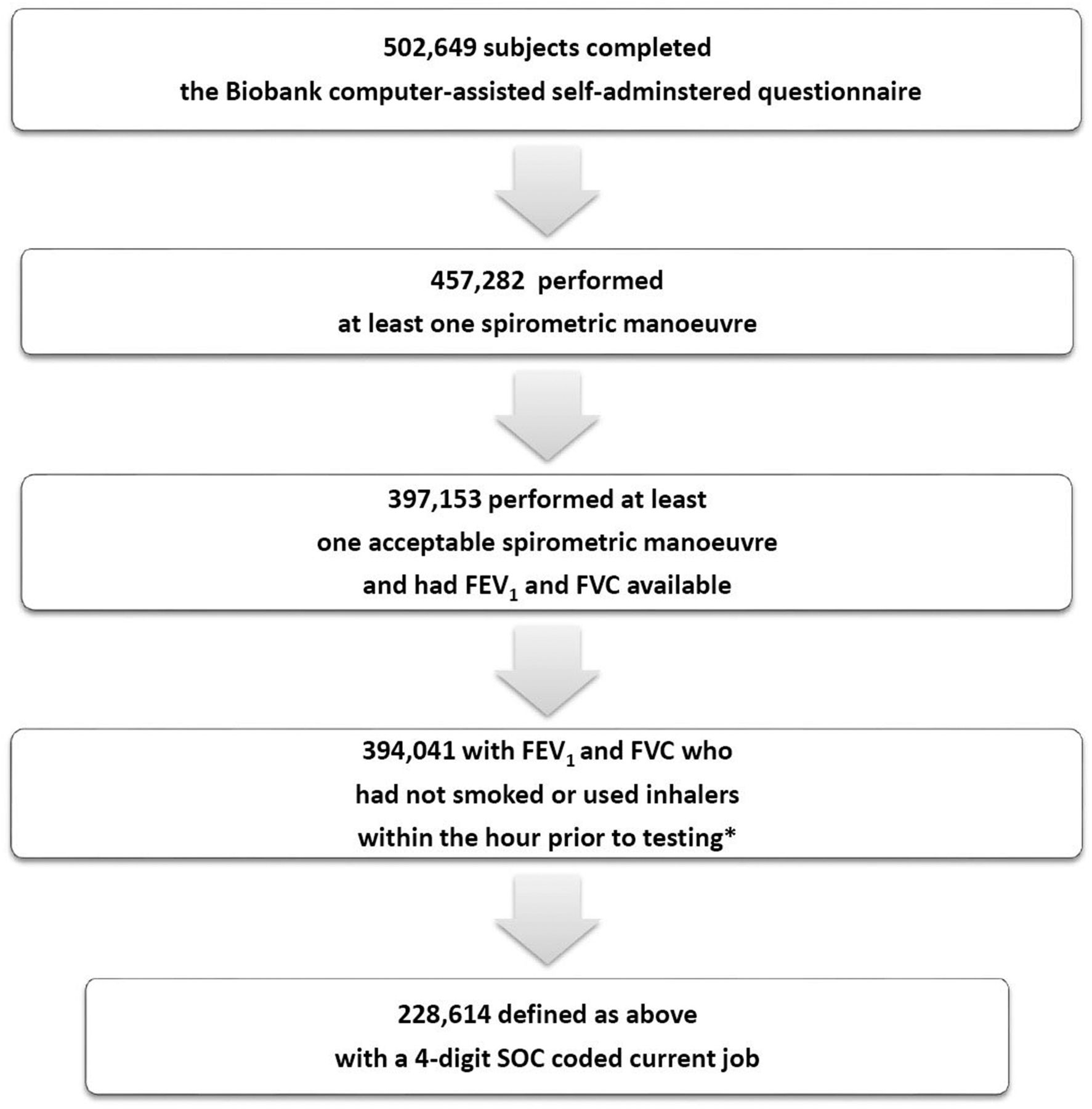
{kind=link}
Study flow diagram in the UK Biobank cohort. *Absolute contraindications to spirometry included chest infection in the last month (ie, influenza, bronchitis, severe cold, pneumonia); history of detached retina; heart attack or surgery to eyes, chest or abdomen in past 3 months; history of a collapsed lung; pregnancy (first or third trimester); and currently on medication for tuberculosis. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; SOC, Standard Occupational Classification.
Statistical analysis
We performed a cross-sectional analysis to examine the association of COPD with current occupation (four-digit SOC-coded job) using all participants not working in each specific job as the reference group. A Poisson regression model with a robust error variance was used to estimate prevalence ratios (PRs) and 95% CIs. Poisson regression is preferable in this context to a standard binomial model that may present convergence problems when the prevalence of the outcome is high or if one or more of the covariates are continuous.17–19 We included in the models as covariates a set of a priori potential confounders (sex, age, recruitment centre, tobacco smoking) and then tested, one by one, other potential covariates (such as type of tobacco smoking and body mass index) using a threshold of 10% to estimate their potential bias impact on risk estimates. The final model included, as adjustment covariates, age (5-year categories), sex, recruitment centre (22 categories) and lifetime tobacco smoking (ever/never, pack-years and years since quitting). For jobs found associated with increased COPD risk, we performed further analyses by sex to identify gender-specific occupational risks and by duration of employment (10-year categories) in each job as proxy for exposure–response test for trend.
Taking advantage of the large sample size, the associations identified in the main analyses were then tested in sensitivity analyses among (1) lifetime non-smokers (to rule out residual confounding by tobacco smoking) and (2) those who did not report a doctor's diagnosis of asthma (to decrease the chance of disease misclassification given that only prebronchodilator spirometry measures were available). Finally, within each occupation associated with COPD risk, we tried to identify specific job titles at increased risk using a more detailed seven-digit SOC code.
All analyses were performed using Stata V.13 (StataCorp, 2013, Stata Statistical Software: Release 13, College Station, Texas: StataCorp LP).
Results
Of the 228 614 study participants included in the analysis, about 52% were women; in both sexes, the average age at recruitment was 52 years. The majority were lifetime non-smokers (n=129 858; 57%), both in men (n=57 805; 53%) and women (n=72 053; 61%), and among ever-smokers, a minority were current smokers (n=20 968; 9%), both in men (n=11 335; 10%) and women (n=9633; 8%). About 11% of participants reported that a diagnosis of asthma had been made at some point during their life (table 1). When compared with all Biobank participants not included in this analysis, no significant differences in these factors were detected, except for age which is explained by exclusion of retired participants (mean 59.8, SD 7.4; data not shown). The overall prevalence of COPD in our sample was 8.9% corresponding to 20 289 cases (9566 in men, 8.7%; and 10 723 in women, 9.0%).
Selected characteristics of the study participants (n=228 614), overall and by sex, in the UK Biobank study, 2006–2010, UK
Main analysis
Among the evaluated 353 SOC-coded occupations, 25 showed a statistically significant increased risk of COPD and 10 occupations, mostly managerial, showed a statistically significant decreased risk (see online supplementary table S1). We focused the following analyses on the 14 jobs with a moderate COPD increased risk (PR≥1.30), and with at least five exposed persons in both cases and non-COPD participants. These occupations are listed in decreasing order of risk strength in table 2.
PRs and 95% CIs of COPD risk spirometry defined as FEV1/FVC<LLN for exposure to current job codified as four-digit SOC code 2000 in the UK Biobank study (n=228 614)
Supplementary tables
For these 14 occupations, analyses stratified by sex were performed (see online supplementary table S2). In some male-dominated jobs (eg, seafarers and coal miners), there were too few women to calculate reliable risk estimates. In women, packers, bottlers, canners, fillers (PR 1.77; 95% CI 1.16 to 2.69); cleaners, domestics (PR 1.45; 95% CI 1.28 to 1.64); school mid-day assistants (PR 1.37; 95% CI 1.04 to 1.80); and kitchen and catering assistants (PR 1.27; 95% CI 1.06 to 1.53) remained at significantly increased COPD risk. In men, all associations were confirmed except for school mid-day assistants, where too few exposed cases prevented calculation of risk estimates.
In addition, we examined these occupations by employment duration (see online supplementary table S3); the majority of the 14 occupations showed a significant positive trend except for coal mine operatives, horticultural trades, chemical and related process operatives, and school mid-day assistants. For some occupations, the few participants among exposed cases, in particular for the longest duration category, rendered the PRs estimates in each job duration category unstable.
Sensitivity analyses
Risks for 8 of these 14 occupations remained significantly increased with similar effect estimates when analyses were restricted to those reporting that they were lifetime non-smokers (n=129 858). Of note, there were too few non-smokers among coal mine operatives to conduct analyses and very few non-smokers among industrial cleaners and those in horticultural trades (with no effect observed and wide CIs). Restriction to lifetime non-smokers appeared to eliminate associations of COPD with labourers and those in woodworking trades. Restriction of analyses to those who reported never having a doctor's diagnosis of asthma (n=203 086) made little change to effect estimates, although in some cases (roofer, packers, horticultural trades, chemical, school mid-day assistants), associations became non-significant due to reduced sample sizes (table 3).
PRs and 95% CIs of COPD risk spirometry defined as FEV1/FVC<LLN for exposure to current job codified as four-digit SOC code 2000 in the UK Biobank cohort overall (n=228 614), never-smokers (n=129 858) and non-asthmatics (n=203 086)
The results of these sensitivity analyses for all the 353 SOC codes are available in the online supplementary tables S4 and S5. Of note, in the analysis restricted to never-smokers, significant associations with COPD were seen for glaziers, window fabricators and fitters (SOC code 5316; PR 2.04; 95% CI 1.11 to 3.76). Although rubber process operatives (SOC code 8115) and tyre, exhaust and windscreen fitters (SOC code 8135) showed significantly high risks (PR 7.71; 95% CI 2.74 to 21.67, and PR 6.27; 95% CI 2.15 to 18.28, respectively) estimates are based on only two exposed cases. Among non-asthmatics, those in welding trades (SOC code 5215) showed a significantly increased risk (PR 1.47; 95% CI 1.04 to 2.08).
More detailed analysis
In table 4, the risk of COPD for a more detailed job code (the seven-digit SOC code) within each of the 14 occupations is shown. Only significant/borderline risk estimates with at least five exposed individuals among both cases and healthy participants are listed in decreasing order of risk strength. In most of the occupations, there were too few participants in each seven-digit coded job title to allow estimation of risk. Although there was some variation in the risk estimates, there was no clear evidence that risk was different between the seven-digit coded job titles within a single broad job category (ie, the four-digit coded job title).
PRs and 95% CIs of COPD risk spirometry defined as FEV1/FVC<LLN for exposure to current job codified as seven-digit SOC code 2000 within each of the four-digit SOC codes for 14 occupations associated with a significant increased COPD risk, in the UK Biobank study (n=228 614)
Discussion
In a large population-based study of over 220 000 current workers in the UK, we found that several occupations were associated with an increased risk of COPD, not only after adjusting for tobacco smoking, but also restricting the analyses to never-smokers. In particular, we confirmed the known higher risks among coal miners, construction workers (roofers, floorers and labourers, but not bricklayers, masons) and industrial process operatives (food, drink, tobacco and chemicals).2 ,3 ,8 New findings, in order of strength, are seafarers, cleaners, postal workers, school assistants and kitchen assistants. In relation to the potential underlying causal occupational agents, diesel motor exhausts for seafarers and postal workers, irritant chemicals for cleaners, and cooking gas for kitchen workers can be hypothesised. We did not detect an increased risk in textile workers (three exposed cases), quarry workers and related operatives (two exposed cases), welders (except in non-asthmatics), or farmers (except possibly for farm managers) as previously reported.2 ,3 ,8 Our few missing associations are likely to be due to the scarce representation in our sample of these high-risk ‘dirty’ jobs as expected in a general population sample.20
Our study has several strengths. First, it is not restricted to an industrial sector but covers a broad variety of occupations and industry sectors in the general working population, giving a general picture of COPD risk and impact in relation to occupation in the whole country. Second, the large sample size which, to the best of our knowledge, is greater than any previous study conducted on occupations and COPD risk (as measured by lung function) in a general population. The large sample allowed sensitivity analyses among never-smokers and non-asthmatics strengthening the reliability of our findings by showing consistency of the results in subgroups free from potential residual confounding effect of tobacco smoking and disease misclassification with asthma, respectively. Also, we were able to perform analyses by sex, to evaluate potential gender-specific risks.
Third, the occupational exposure assessment was based on job descriptions collected through personal interview by trained operators who coded each job title using standard occupational codes blind to COPD status, ruling out any differential misclassification. Fourth, we used a spirometry-based COPD definition using the LLN as the diagnostic cut-off because, in comparison to the fixed ratio (FEV1/FVC <70%), it is less likely to be biased in older ages as it is the case in our study base21 In addition, we tested an alternative COPD definition that comprised either ‘FEV1<LLN or FEV1/FVC<LLN’ to rule out any misclassification due to a potential dust-related FVC decline; the results remained substantially unchanged (data not shown). Finally, the available information on duration of employment within each job, allowed us to evaluate exposure–response relationships, again to support the reliability of our findings.
Nevertheless, we should acknowledge some study limitations: the cross-sectional design is susceptible to potential healthy worker effect (HWE), although this is likely to bias the risk estimate towards the null with a resulting underestimation of the true work-related COPD risk. In particular, given the older age of our study sample, the healthy worker survivor effect component of the HWE bias could have played a major role, because with ageing only the fittest tend to remain in high-risk jobs.22 To minimise this potential bias, we used as reference category all the workers not exposed to the specific job title under analysis instead of a fixed category of ‘white-collar’ workers who may be different in many (non-occupational) aspects from ‘blue-collar’ workers. Our study is large, but a large sample is not necessarily equivalent to representativeness. In fact, reported response rates to the baseline UK Biobank survey were low9 making unlikely that the UK Biobank cohort is representative of the UK working population in all aspects. Nevertheless, in epidemiology, it is recognised that internal more than external validity is required in order to assess causal associations.23
We have conducted a large number of tests (n=353) and cannot rule out that some reported associations may have arisen by chance. However, to apply a formal statistical correction method (eg, Bonferroni) to address the multiple testing issues might be too penalising. In fact, our approach was not completely agnostic, given the presence of some occupations suspected or a priori known to be associated with an increased COPD risk. Also, to reduce the number of false-positive associations, we have limited our sensitivity analyses to the 14 occupations showing not only formal statistical significance, but also moderate strength of association, and with sufficient numbers of exposed persons among both cases and healthy participants.
In relation to potential additional adjustments, we did not include education level as a covariate in the final model because occupation is a proxy for socioeconomic status (SES). It has been argued that to adjust for SES might result in overadjustment of risk estimates with unpredictable direction of the resulting bias.24 In addition, we did not include ethnicity in our final models. There has been some debate about whether adjustment for ethnicity is appropriate in studies with spirometry-defined COPD as the heath outcome as it may be a surrogate for other socioeconomic differences, such as income and access to healthcare, that are likely to be more important in determining individual lung function measurements.25 Almost all Biobank participants described themselves as ‘white’ (215 314; 94%). Adjusting for ethnicity made no material difference to our reported associations, and similarly restriction to ‘white’ participants did not change the results (data not shown).
In conclusion, we found that work in specific occupations may increase COPD risk in the general population. Given the large sample, and the consistency of our findings in sensitivity analyses, in particular in never-smokers, we are confident of the validity of these findings and that they deserve further investigation. We will next investigate the underlying potential occupational causal agents by applying a job exposure matrix approach, and collect information on lifetime job histories in further studies of the cohort. These planned analyses will provide important insight into the extent to which the associations we have detected reflect occupational exposures which are still of concern, and thus where preventive actions may need to be strengthened.
References
Footnotes
Contributors SDM developed the statistical plan, analysed the data, reported and interpreted the results and wrote the manuscript. DJ and AD contributed in designing the study, developing the statistical plan, interpreting the results and reviewing the manuscript. SH contributed in developing the statistical plan and reviewing the manuscript. DF contributed in reviewing the manuscript. SS contributed in interpreting the results and reviewing the manuscript. LR and PC are the co-principal investigators of the study, contributed in designing the study, developing the statistical plan, interpreting the results and reviewing the manuscript.
Funding This research was supported by contract OH1511 from the Health and Safety Executive (HSE).
Disclaimer The content of this paper contains the views of the authors, and not necessarily those of the funders Health and Safety Executive (HSE).
Competing interests None declared.
Patient consent Obtained.
Ethics approval UK Biobank has received ethics approval from the National Health Service National Research Ethics Service (Ref 11/NW/0382).
Provenance and peer review Not commissioned; externally peer reviewed.