Article Text

Abstract
Background Both chronic inflammation and cardiovascular comorbidity play an important role in the morbidity and mortality of patients with chronic obstructive pulmonary disease (COPD). Statins could be a potential adjunct therapy. The additional effects of statins in COPD are, however, still under discussion. The aim of this study is to further investigate the association of statin use with clinical outcomes in a well-described COPD cohort.
Methods 795 patients of the Cohort of Mortality and Inflammation in COPD (COMIC) study were divided into statin users or not. Statin use was defined as having a statin for at least 90 consecutive days after inclusion. Outcome parameters were 3-year survival, based on all-cause mortality, time until first hospitalisation for an acute exacerbation of COPD (AECOPD) and time until first community-acquired pneumonia (CAP). A sensitivity analysis was performed without patients who started a statin 3 months or more after inclusion to exclude immortal time bias.
Results Statin use resulted in a better overall survival (corrected HR 0.70 (95% CI 0.51 to 0.96) in multivariate analysis), but in the sensitivity analysis this association disappeared. Statin use was not associated with time until first hospitalisation for an AECOPD (cHR 0.95, 95% CI 0.74 to 1.22) or time until first CAP (cHR 1.1, 95% CI 0.83 to 1.47).
Conclusions In the COMIC study, statin use is not associated with a reduced risk of all-cause mortality, time until first hospitalisation for an AECOPD or time until first CAP in patients with COPD.
- COPD Exacerbations
- COPD Pharmacology
- Pneumonia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the association of statin use and clinical outcome in a well-described chronic obstructive pulmonary disease (COPD) cohort?
Statins could be a potential adjunct therapy in COPD. However, the association of statin use with clinical outcome in COPD is still under discussion.
In a large well-described COPD cohort, statin use resulted in better overall survival, but after exclusion of immortal time bias no differences on clinical outcome were observed between groups with and without statin use.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic disease accompanied by increased morbidity and mortality. It is estimated that COPD is the third leading cause of death worldwide.1 COPD is characterised by acute exacerbations of COPD (AECOPD) which can accelerate the already existing gradual decline of lung function and increase the risk of death.2 AECOPD are associated with increased risk of hospitalisations, lower quality of life and increased healthcare costs. Effective therapy or interventions to prevent this morbidity and mortality include, for instance, inhalation medication, smoking cessation, supplemental oxygen therapy, pulmonary rehabilitation and lung transplantation.
Underlying chronic and systemic inflammation plays an important role in the pathophysiology of COPD and its progression.3 ,4 The majority of patients with COPD have associated comorbidity, which is partially the cause of the increased mortality seen in COPD.5 ,6 The high concurrence of COPD with cardiovascular morbidity is mainly because of common risk factors.2 There is a rationale for a treatment that has a positive effect on this ongoing (systemic) inflammation as well as on the, sometimes not yet recognised, cardiovascular morbidity in patients with COPD.
Statins are inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase. Besides a proven effect on reducing cardiovascular disease by treating hypercholesterolaemia, they have other pleiotropic anti-inflammatory effects as well.7 ,8 In the lung, statins have an effect on bronchial remodelling, emphysema development and recruitment of inflammatory cells. Effects are systemically observed on various biomarkers and cytokines such as high-sensitivity C reactive protein (hsCRP), interleukin-6 (IL-6), interleukin-8 (IL-8) and tumour necrosis factor α (TNF-α).9
Various mainly retrospective studies and reviews have been performed to establish the effect of statin use in patients with COPD.10–20 These studies reported a reduced mortality,14 ,20 ,21 reduced exacerbations with or without hospitalisation,13 ,15 ,16 reduced lung function decline17 ,19 and lower levels of hsCRP18 as a marker for systemic inflammation. Even improvement of pulmonary hypertension and dyspnoea during exercise by the use of a statin in patients with COPD with pulmonary hypertension is observed.22 Nevertheless, the first large randomised trial, the STATCOPE study, showed no beneficial effects of statin use in reducing the frequency or severity of exacerbations in patients with COPD.23
The role of statins on outcome in patients with COPD is therefore still not defined.
Differences in study design, immortal time bias, lack of correction for confounders and unclear definition and measurement of statin use are possible explanations for the difference in outcome. The large COMIC cohort (Cohort of Mortality and Inflammation in COPD) of patients with well-defined COPD whom we followed prospectively for more than 3 years offers a well-documented medication history and therapy adherence during the study including statins. The study is powered for mortality and with available lung function, global initiative for chronic obstructive lung disease (GOLD) stage, smoking status and other predictors such as the age, dyspnoea, obstruction (ADO) score and body mass index, obstruction, dyspnoea (BOD) index, the aim of this analysis is to establish the independent association of statin use with morbidity and mortality in these patients with COPD.
Methods
Settings and study population
This study was part of the COMIC study, a single-centre cohort study from Enschede, the Netherlands. From December 2005 until April 2010, 795 patients were included with a follow-up period of at least 3 years. The COMIC study was approved by the hospital's medical ethical committee. All patients provided written informed consent. The COMIC study started before the introduction of trial registries. The study was initiated to investigate the relationship between the immune response after influenza vaccination in patients with COPD and mortality. Different papers concerning COPD have been published with this COMIC study.24–26
For inclusion in the COMIC study, patients had to meet the following criteria: (A) a clinical diagnosis of COPD according to the GOLD guidelines; (B) current or former smoker; (C) age ≥40 years; (D) no medical condition compromising survival within the follow-up period or serious psychiatric morbidity; (E) absence of any other active lung disease (eg, sarcoidosis); (F) no maintenance therapy with antibiotics; (G) ability to speak Dutch. Patients were enrolled when visiting the outpatient clinic in stable state (stable state group) or when hospitalised for an acute exacerbation in COPD (AECOPD group). To be included in the AECOPD group, patients had to be hospitalised for an AECOPD and be able to produce an adequate sputum sample on the day of hospitalisation. To be included in the stable state group, patients had to meet the following criteria: no use of antibiotic and/or prednisolone 4 weeks prior to enrolment and no exacerbation less than 4 weeks before study entry. All patients were treated according to standard care.
Definition of statin use
Statin use was recorded from patients' pharmacy records. Since chronic medication in the Netherlands is usually prescribed for a period of 3 months, statin use was defined as having a statin for at least 90 consecutive days after inclusion in the cohort. When a patient was on a statin at inclusion but follow-up was for less than 90 days, the patient was defined as a statin user when he or she used the statin for at least 90 consecutive days prior to inclusion. The patient who started a statin after inclusion for a period of less than 90 days was not defined as a statin user.
Outcomes
The primary outcome parameter was 3-year survival, based on all-cause mortality. Date of death was verified from the municipal administration.
Morbidity was defined as time until first hospitalisation for an AECOPD and time until first community-acquired pneumonia (CAP). AECOPD was defined as an acute negative change from baseline, reported by the patient, in dyspnoea and/or sputum volume and/or colour of sputum (yellowish or greenish sputum) and/or cough, which may warrant additional treatment of prednisolone with or without antibiotics by a physician in a patient with underlying COPD. Pneumonia was defined as an acute respiratory tract illness associated with radiographic shadowing on a chest radiograph consistent with infection which was neither pre-existing nor of any other known cause. All X-rays were double read by a radiologist and a chest physician. In case of doubtful shadows in the report, the X-ray was presented to another chest physician for final judgement.
Demographic data including data on common comorbidities like myocardial infarction, congestive heart failure and diabetes mellitus were collected from medical records. At baseline, spirometry was performed according to standardised guidelines27 and smoking status was determined by the Vlagtwedde questionnaire.28 Patients completed the modified Medical Research Council Dyspnea Questionnaire (mMRC).29 The BOD comprises body mass index, obstruction, dyspnoea, exercise (BODE) without exercise capacity measurement.30 The components were scored according to the same cut-offs as in BODE.31 The BOD therefore ranges from 0 to 7.32 The original and updated ADO score ranges, in increasing severity, from 0 to 10 and from 0 to 14 points, respectively. 33 ,34 All measurements were performed in stable state.
Therapy adherence of statin use was defined as follows: theoretical duration of exposure was calculated using information on dispensing date, total supply and dosage regimen. We computed the total number of days for which patients had collected medication during follow-up and divided this by the total number of days between the first and last medication collection during follow-up plus the day's supply of the last refill.35 This was expressed as a percentage and adherence was deemed good if it was >75%.
Statistical analysis
Continuous variables are expressed as mean (±SD) or as median (IQR), and categorical variables as counts (percentages). Time from inclusion to event (all-cause mortality, first hospitalisation for an AECOPD, first CAP) was analysed by Kaplan-Meier survival curves and compared between statin and non-statin users with log-rank tests. Univariate and multivariate Cox proportional hazard regression models were used to establish the association of statin use with survival, time until first hospitalisation for an AECOPD and time until first CAP. First, we studied in univariate analyses the association between statin use and potential confounders such as lung function parameters, GOLD stage, body mass index (BMI), comorbidity and sex. Next, we studied in multivariate Cox proportional hazard regression models the association between the outcome parameters (mortality, time until first hospitalisation for an AECOPD, time until first CAP) on the one hand and statin use on the other hand, and added all potential confounders (ie, variables that were associated with statin use and the outcome parameter of the specific models with a corresponding p value <0.10). We started the multivariate model with all potential confounders. Variables with the highest p value were eliminated step by step until the fit of the model decreased significantly, based on a −2 log likelihood. All tests were two sided and a p value of 0·05 was considered statistically significant. Data were analysed using SPSS, V.22 (SPSS Inc. Chicago, Illinois, USA).
Sensitivity analysis
By including patients who started a statin 3 months or more after inclusion for a period of at least 90 consecutive days, there is a possibility of introducing immortal time bias. Therefore, a sensitivity analysis was performed where these patients were excluded from analysis to prevent the immortal time bias.36
Results
Baseline characteristics
Our COMIC cohort included 795 patients. Six hundred and sixty three patients (78%) were enrolled when visiting the outpatient clinic in stable state and 172 patients (22%) were enrolled when hospitalised for an acute exacerbation in COPD. 253 patients (32%) were defined as statin users. Of those, 62 patients (25%) started a statin ≥3 months after inclusion for a period of at least 90 consecutive days. The baseline characteristics of these two groups are displayed in table 1.
Baseline characteristics of 795 individuals with COPD
Statin users were more often male and had significantly more cardiovascular morbidity, a higher BMI and a better lung function. Eighty-five per cent of the statin users had a good therapy adherence to statins defined by a therapy adherence percentage >75%.
Survival
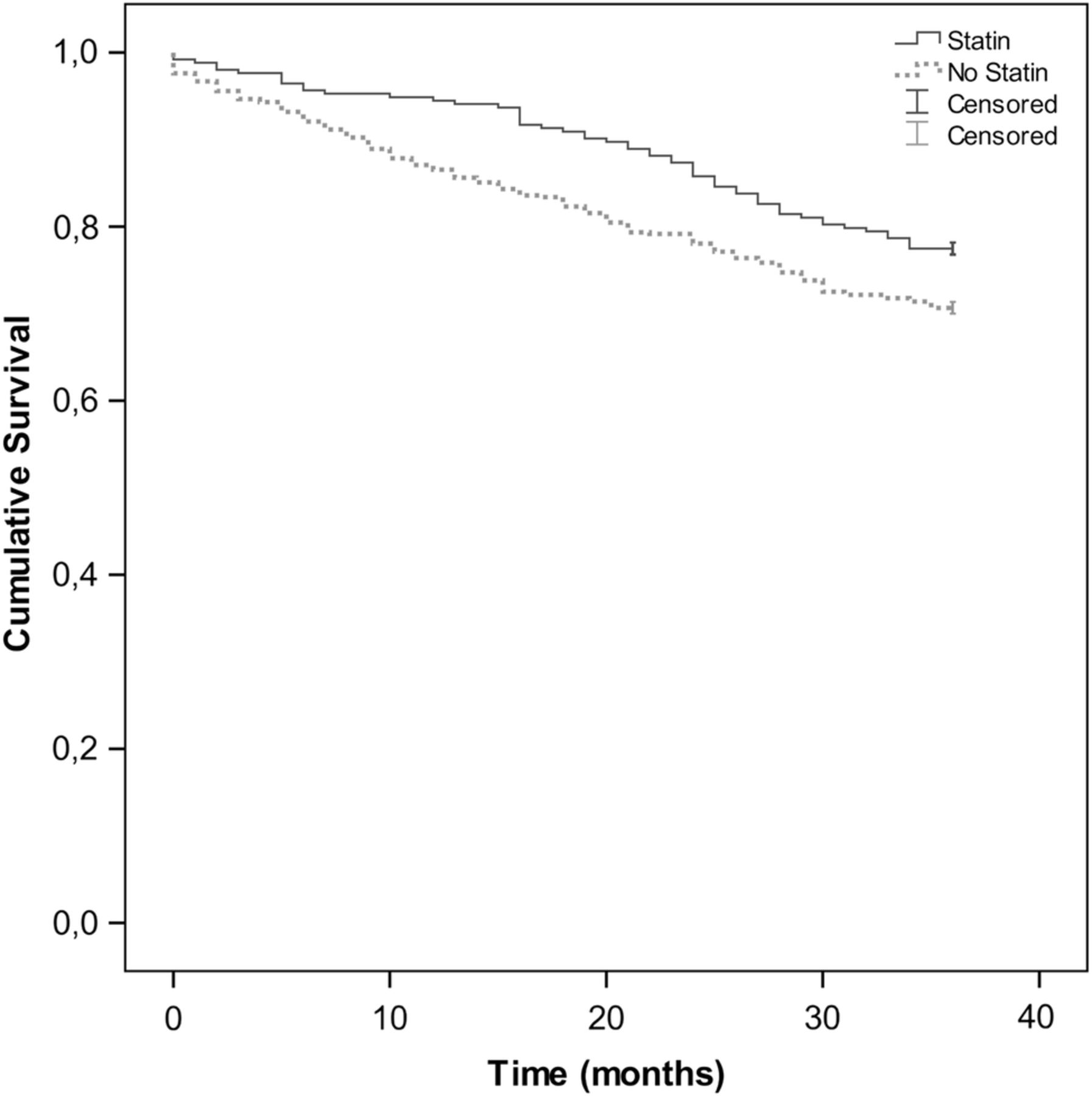
Median follow-up time was 3630–36 months. The cumulative survival after 1, 2 and 3 years is displayed in table 2. Statin users had a significantly better overall survival compared with the non-statin users (log-rank: p=0.028) with an HR of 0.72 (95% CI 0.53 to 0.97) in univariate analysis (figure 1).
Cumulative survival at 1, 2 and 3 years

Kaplan-Meier Survival Curve for statin use in patients with COPD. COPD, chronic obstructive pulmonary disease.
In a multivariate Cox regression analysis, statin use, corrected for the confounders sex, BMI, heart failure and FEV1 (L), resulted in better survival with an HR of 0.70 (95% CI 0.51 to 0.96).
Morbidity
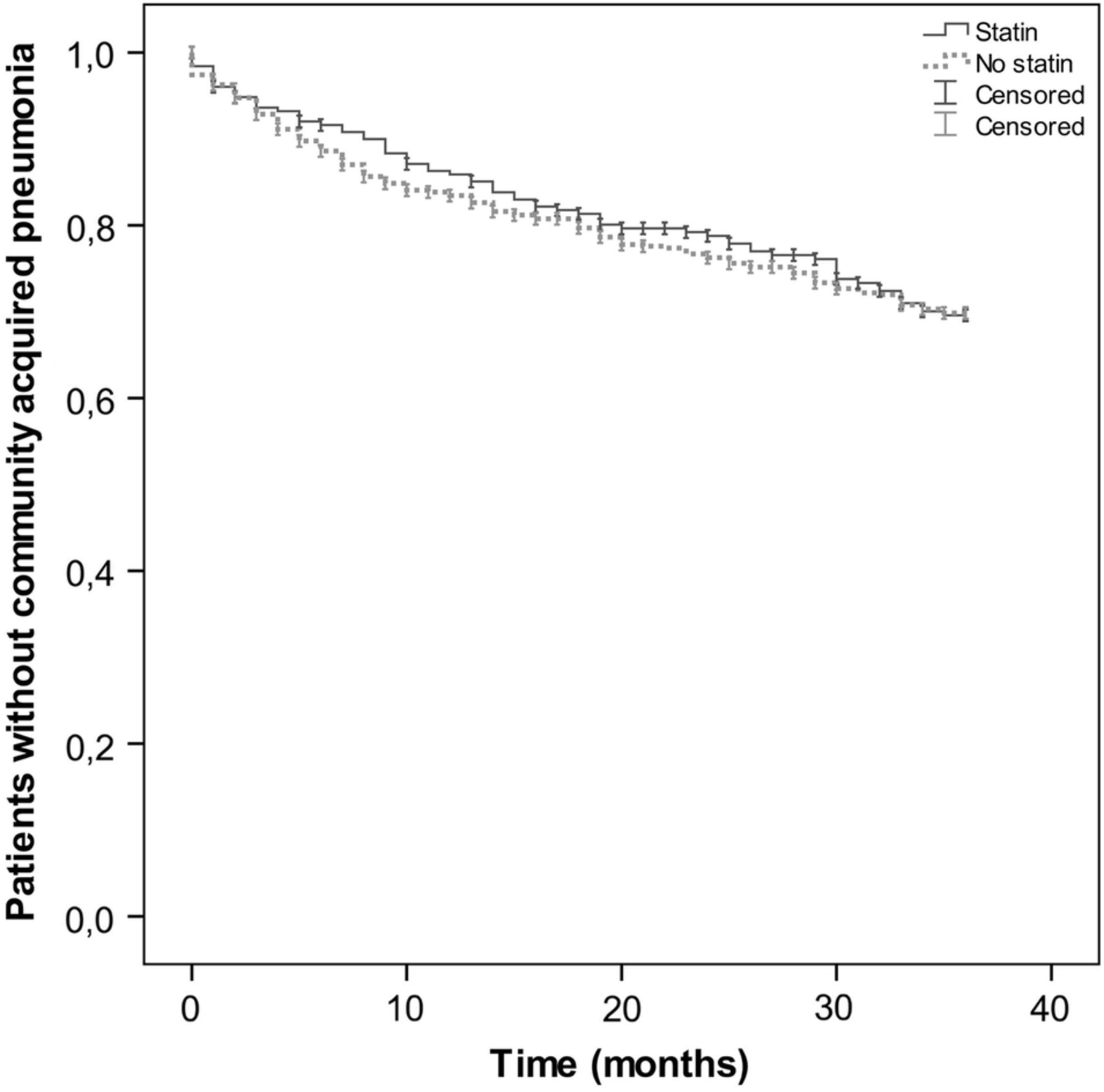
During the 3 years of follow–up, 344 patients (43%) had at least one hospitalisation for an AECOPD and 220 patients (28%) had at least one diagnosed CAP. In a univariate and multivariate Cox regression analysis, there were no significant differences between statin users and non-statin users in time until first hospitalisation for an AECOPD (log-rank: p=0.67) with a cHR of 0.95 (95% CI 0.74 to 1.22) (figure 2) and time until first CAP (log-rank: p=0.87) with a cHR of 1.1 (95% CI 0.83 to 1.47) (figure 3).

Kaplan-Meier Survival Curve for association of statin use with time until first hospitalisation for an AECOPD. AECOPD, acute exacerbation of COPD.

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier Survival Curve for association of statin use with time until first CAP. CAP, community-acquired pneumonia.
Sensitivity analysis
For the sensitivity analysis, the 62 patients who started a statin ≥3 months after inclusion for at least 90 consecutive days were excluded from the analysis. With the remaining 733 patients, no significant difference was seen in overall survival between the statin and non-statin users. Multivariate Cox regression analysis shows an HR of 0.82 (95% CI 0.59 to 1.16, p=0.26).
Discussion
In our large prospective cohort with patients with well-defined COPD, the use of a statin initially seemed to be associated with reduced mortality. However, when corrected for immortal time bias, statin use was not associated with all-cause mortality despite the different anti-inflammatory effects ascribed to statins. Statin use also was not associated with time until first hospitalisation for an AECOPD and time until first CAP.
This is in accordance with the first large randomised controlled trial by Criner et al.23 They randomly assigned 885 patients with COPD to either daily simvastatin 40 mg or placebo. No differences between exacerbation rate and time until first exacerbation were observed during follow-up between the two groups and, as part of the secondary outcome, no difference in mortality was observed as well.
Human and animal studies indicate that statins have an effect on pulmonary inflammation and remodelling.9 This effect is achieved by influencing different pathways such as neutrophil influx, matrix remodelling, apoptosis, oxidant response and mucus production. They modulate cytokine production such as TNF-α, IL-6 and IL-8, which also could reduce serum CRP and subsequently have an effect on systemic inflammation. By lowering the local and systemic inflammation and preventing further remodelling, this could be a potentially efficacious therapy in patients with COPD.
Subsequent and mainly retrospective and observational studies did show beneficial effects of statins on exacerbations and mortality. In a retrospective nested case–control study, Wang et al15 observed a 30% decreased risk of COPD exacerbations with hospitalisation in patients with COPD using a statin. In a nested case–control study by Mancini et al, a risk reduction for hospitalisation for COPD was seen with use of statin with an RR of 0.72.14 As part of the Rotterdam study, Lahousse et al18 demonstrated a beneficial effect of long-term statin use on all-cause mortality in COPD. Søyseth et al21 demonstrated in a retrospective cohort design a crude relative mortality ratio among statin users versus nonusers of 0.58 (95% CI 0.39 to 0.84).
Before the sensitivity analysis, our study demonstrates a positive association with all-cause mortality as well. However, after the sensitivity analysis, this supposed favourable association disappeared. An important explanation for this finding is immortal time bias. Immortal time consists of the time between inclusion and the moment of first starting the statin. The study subject had to survive this time before exposure to the statin could occur. In this period, the patient is classified as a statin user while in fact he or she is not (yet). With immortal time bias, a non-existing survival benefit is introduced.36 Besides this bias, a further examination of the 62 patients excluded for the sensitivity analysis shows that for seven of them the reason for starting a statin was a myocardial infarction, which was treated with percutaneous coronary intervention and/or pharmacological treatment. These interventions have a positive effect on mortality, and before the sensitivity analysis this positive effect could wrongly be attributed to the use of statins.
So, with our study, we have gathered additional evidence that statin use is not associated with clinical outcome in COPD. Other explanations for the difference in outcome between the previous studies and the recent STATCOPE study and our findings could be the following: First, the potential beneficial effects of statins may only be seen in some subsets or phenotypes of patients with COPD, such as those with coexisting cardiovascular disease or patients with systemic inflammation. In a nested case–control study by Ingebrigtsen et al,13 statin use was indeed associated with reduced odds of exacerbations in individuals with COPD but not in the patients with most severe COPD without cardiovascular comorbidity. These patients were excluded in the STATCOPE study. In our study, however, cardiovascular comorbidity was not an exclusion criterion and 27% of the included patients had one or more cardiovascular comorbidities; nevertheless, no favourable association of statin use was observed.
Lahousse et al18 demonstrated that when stratified to the level of systemic inflammation, long-term statin use was associated with a significantly reduced all-cause mortality if the hsCRP level was >3 mg/L. We have not measured the hsCRP and therefore cannot make this stratification.
Second, in observational studies, a healthy user effect or non-healthy non-user effect is possible, as well as the risk of bias other than the immortal time bias, such as confounding bias. Besides, in some studies, patients with COPD are included because of ICD codes in various large registries, while often no lung function data to confirm COPD diagnosis are present. Moreover, different definitions of statin use are used where sometimes having one prescription of a statin is enough for one to be defined as a statin user. This makes it difficult to compare the studies with each other and to make a clear judgement of the clinical effects of statin in COPD.
The strength of our study is that we have a heterogeneous, well-defined, unselected COPD population with accurate lung function measurements and comorbid conditions, which we followed prospectively for a minimum of 3 years. With sufficient events during follow–up, the power of the study was large enough to identify relevant differences in the outcome parameters between the patients with COPD who used a statin or not. In addition, we have a well-defined definition for statin use, and for the sensitivity analysis we excluded patients who started a statin late during follow-up to exclude immortal time bias. Removing the 62 patients to exclude immortal time bias has reduced our sample size, but, more importantly, reduced the HR in size as well. If we would want to achieve a study power of 80% with this HR, we would need to study 549 patients on statins and 1559 patients without statins. Therefore, we feel that the lack of statistical significance is not so much caused by the lower number of patients, but due to the fact that, when excluding immortal time bias, the protective effect of statins is reduced. With the high percentage of therapy adherence of statins, a possible association could be attributed to the actual use of statins. Although pharmacy records give an indication of the amount of dispensed medication and not the actual amount of medication taken, we believe that with the 3 years of follow-up there will not be a large difference between them.
A limitation of our study is that statin use was not randomised, so there is a risk of selection bias. In the baseline characteristics, one can see that the statin group, as expected, has significantly more cardiovascular morbidity. Surprisingly, they have a slightly but significantly better lung function. Nevertheless, corrected for these and other potential confounders, statin use in the multivariate Cox regression model still was not associated with mortality and morbidity.
A healthy user effect implies the fact that using a statin could be a marker for relatively better health that may result in better overall survival. However, in our study, owing to the significantly more prevalent cardiovascular comorbidity in the statin group, there is no indication for a healthy user effect. In the non-statin group, there were eight patients with comorbid myocardial infarction who surprisingly have not been prescribed a statin. The reason therefore is unknown. This could imply a bias of non-healthy non-user effect in the analysis, although the number of eight patients is small.
In conclusion, statin use seemed to be associated with a reduced risk of all-cause mortality in patients with COPD, but in the sensitivity analysis this association disappeared. Statin use also was not associated with time until first hospitalisation for an AECOPD or time until first CAP in patients with COPD. Until more new definitive randomised controlled trials determine otherwise, there is no indication to start a statin in all patients with COPD. Prescribing statins to patients with COPD should therefore be in accordance with nationwide guidelines.
References
Footnotes
Contributors EC contributed to the study design, data collection, statistical analysis and writing of the manuscript; he is the guarantor of the manuscript and takes responsibility for the integrity of the data and the accuracy of the data analysis. JvdP contributed to the study design, statistical analysis and writing of the manuscript. MB-K contributed to the study design, statistical analysis and writing of the manuscript. PvdV contributed to the writing of the manuscript. KKH contributed to the data collection and writing of the manuscript. KM contributed to the study design.
Funding GlaxoSmithKline.
Competing interests None declared.
Ethics approval METC Twente.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.