Article Text

Abstract
Introduction Breathlessness is the cardinal symptom in both cardiac and respiratory diseases, and includes multiple dimensions. The multidimensional instrument Dyspnoea-12 has been developed to assess both physical and affective components of breathlessness. This study aimed to perform a clinical validation of the Swedish version of Dyspnoea-12 in outpatients with cardiorespiratory disease.
Methods Stable outpatients with cardiorespiratory disease and self-reported breathlessness in daily life were recruited from five Swedish centres. Assessments of Dyspnoea-12 were performed at baseline, after 30–90 min and after 2 weeks. Factor structure was tested using confirmatory factor analysis and internal consistency using Cronbach’s alpha. Test–retest reliability was analysed using intraclass correlation coefficients (ICCs). Concurrent validity at baseline was evaluated by examining correlations with lung function and several instruments for the assessment of symptoms and health status.
Results In total, 182 patients were included: with the mean age of 69 years and 53% women. The main causes of breathlessness were chronic obstructive pulmonary disease (COPD; 25%), asthma (21%), heart failure (19%) and idiopathic pulmonary fibrosis (19%). Factor analysis confirmed the expected underlying two-component structure with two subdomains. The Dyspnoea-12 total score, physical subdomain score and affective subdomain scores showed high internal consistency (Cronbach’s alpha 0.94, 0.84 and 0.80, respectively) and acceptable reliability after 2 weeks (ICC total scores 0.81, 0.79 and 0.73). Dyspnoea-12 showed concurrent validity with the instruments modified Medical Research Council scale, COPD Assessment Test, European Quality of Life-Five Dimensions-Five levels, the Functional Assessment of Chronic Illness Therapy-Fatigue, the Hospital Anxiety and Depression Scale, and with forced expiratory volume in 1 s in percentage of predicted value. The results were consistent across different cardiorespiratory conditions.
Conclusion The Dyspnoea-12 is a valid instrument for multidimensional assessment of breathlessness in Swedish patients with cardiorespiratory diseases.
- dyspnoea
- breathlessness
- multidimensional
- COPD
- asthma
- idiopathic pulmonary fibrosis
- heart failure
- internal consistency, reliability, concurrent validity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- dyspnoea
- breathlessness
- multidimensional
- COPD
- asthma
- idiopathic pulmonary fibrosis
- heart failure
- internal consistency, reliability, concurrent validity
Key messages
Can the Swedish version of the Dyspnoea-12 instrument be validated in a clinical population?
The Dyspnoea-12 is a valid instrument for multidimensional assessment of breathlessness in Swedish patients with cardiorespiratory diseases.
The multidimensional instrument Dyspnoea-12 assesses both physical and affective components of breathlessness and can now be used to compare patients with breathlessness in different cardiorespiratory diseases, both in clinical routine in Sweden and for research in multi-national studies.
Introduction
Breathlessness is a cardinal symptom in cardiorespiratory disease and is strongly associated with impaired health-related quality of life and increased mortality in chronic obstructive pulmonary disease (COPD),1–3 idiopathic pulmonary fibrosis (IPF)4–6 and heart failure.7 8 Reduction of symptoms is a major treatment goal in both chronic cardiac and respiratory diseases.
Breathlessness consists of multiple dimensions, such as the sensory quantity (intensity) and affective quantity (level of unpleasantness), the associated emotional responses and the functional impact of breathlessness.9 Treatment strategies of breathlessness may affect specific dimensions, and thus standardised multidimensional measurement is needed.10
The Dyspnoea-12 (D-12) instrument was developed to be a brief and concise instrument for the quantification of different dimensions of breathlessness across different cardiorespiratory diseases.11 The original English version has been validated by the developer in patients with COPD, heart failure, interstitial lung diseases, asthma, pulmonary arterial hypertension and lung cancer.11–15 D-12 is now also available in Arabic,16 17 Korean,18 Portuguese,19 Italian20 and Swedish,21 which is important to enable the comparison of results between countries.
The Swedish version of D-12 is linguistically validated,21 but still needs to be validated in clinical patients. The overall purpose of the present study was to perform a clinical validation of the Swedish version of D-12 in patients with cardiorespiratory disease. The primary aim was to validate the Swedish D-12 in terms of the underlying factor structure, internal consistency, test–retest reliability and concurrent validity. The secondary aim was to compare these psychometric measurement properties between patients with COPD and patients with other diagnoses.
Methods
Design and population
This was a prospective, multicentre, cohort study of stable outpatients with any recorded cardiorespiratory condition resulting in persistent breathlessness. The underlying diagnoses were established according to existing guidelines, using spirometry, echocardiography or radiology when relevant.22–25 The patients were recruited at five Swedish outpatient clinics distributed across the whole country; the departments of respiratory medicine and allergy in Umeå, Uppsala, Stockholm and Karlskrona, and the departments of cardiology and respiratory medicine in Örebro. The target sample size was 180 which included patients based on previous validation studies.11–15 The patients were recruited from a prospective patient cohort with prescheduled outpatients’ appointments during the period of 29 August 2016 until 23 December 2017.
The cohort was created with the primary aim of clinically validating the Swedish versions of the two multidimensional instruments D-12 and Multidimensional Dyspnoea Profile (MDP) against other existing instruments. The clinical validation of the MDP is reported elsewhere.26
Inclusion criteria were age >18 years; a recorded chronic respiratory and/or cardiac disease; and self-reported breathlessness during daily life defined as a positive answer to the question ‘Did you experience any breathlessness during the last 2 weeks?’. Exclusion criteria were inability to write or understand Swedish adequately to participate; cognitive or other inability to participate in the study; or any serious disease with estimated survival less than 3 months. Exacerbations, or worsening of symptoms during recent weeks, were not an exclusion criterion.
Dyspnoea-12
D-12 is a brief questionnaire including 12 items with descriptors of breathlessness, each rated as no, mild, moderate or severe.11 The answer to each item is scored from zero to three to get a final total score of 0 to 36, with higher scores indicating worse breathlessness. The original paper demonstrated how the items also form a two part-structure, where the first seven items pertain to a physical subdomain with maximum score of 21, and the remaining five items pertain to an affective subdomain with maximum score of 15. The developer recommends that the instrument should not be used with more than three missing items.11 In the original validation paper, the time frame for assessment of breathlessness was ‘these days’. More recently, D-12 has been validated for assessment during ‘the previous 2 weeks’.27 A Swedish version of D-12 used in this project is available and was linguistically validated in cooperation with Mapi SAS, Language Services Unit, Lyon, France.21
Data collection and assessments
Data used in this study were obtained from three separate patient questionnaires and from a clinical questionnaire based on a record review by the responsible physician. The first and second patient questionnaires (Q1 and Q2) were completed at the baseline visit, separated by 30–90 min. The third patient questionnaire (Q3) was completed and returned by mail after 2 weeks.
The baseline patient questionnaire Q1 included data on sex, age, weight, height, smoking status, pack-years of smoking, self-assessed presence or absence of distressing breathlessness at rest or minimal exertion during the last 24 hours and a number of validated instruments and scales assessing symptoms during the previous 2 weeks. The instruments used in this study included D-12, the modified Medical Research Council (mMRC) breathlessness scale28; the COPD Assessment Test (CAT)29 30 ; the European Quality of Life-Five Dimensions-Five levels (EQ-5D-5L)31; the Hospital Anxiety and Depression Scale (HADS)32; the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue)33 and average severity of breathlessness on a Likert scale (no, mild, moderate, severe). CAT assesses disease-specific health status on a score from 0 to 40 (worst) and is in spite of its name validated for both COPD and IPF,29 30 and EQ-5D-5L transferred to an index using UK weights assesses generic health status, where index 1 is the best possible health status, 0 corresponds to being dead but negative scores may exist.31 HADS evaluates depression and anxiety using 14 items from 0 to 3 (worst) with a total score from 0 to 42 or in separate subdomains scores from 0 to 21,32 and FACIT-Fatigue assesses disease-related tiredness, or fatigue from 0 (no fatigue) to 52.33
The clinical questionnaire completed by the responsible physician collected available data on comorbid conditions, spirometry or ultrasound cardiography performed the previous last 12 months. As for lung function data, post-bronchodilation values of forced expiratory volume and forced vital capacity in percentage of predicted values (FEV1%pred and, respectively, FVC%pred) were used if available or replaced by pre-bronchodilation values.
The patient questionnaires Q2 and Q3 were reduced forms including D-12 and the Global Impression of Change (GIC) assessing change in breathlessness from Q1 on a 7-point scale from very much worse to very much better, where GIC=4 denoted no change in breathlessness.
Statistical analyses
Descriptive statistics were used to present baseline patient characteristics. D-12 total and subdomain scores, CAT scores, EQ-5D-index, HADS total, anxiety and depression scores and FACIT-Fatigue scores were calculated. Subdomain scores were calculated when all items within the subdomain were completed. The factor structure of D-12 was analysed using confirmatory factor analysis. Model fit was assessed using the root mean square error of approximation (RMSEA)34 and Bentler’s comparative fit index (CFI).35 Internal consistency was analysed using Cronbach’s alpha. Test–retest reliability was analysed using intraclass correlation coefficients (ICCs) with two-way mixed analysis of variance for patients who reported unchanged breathlessness (GIC=4) at follow-up. A potential learning effect, due to the fact that the patient is getting familiar with the questionnaire, was evaluated by comparing the test–retest reliability between Q1/Q3 and Q2/Q3. Agreement was evaluated using the Bland-Altman method. Concurrent validity was evaluated using Pearson’s correlation coefficient of the baseline D-12 total and subdomain scores with: FEV1%pred, mMRC, CAT, EQ-5D-index, HADS (total, anxiety and depression scores) and the FACIT-Fatigue scale. The validity analyses were performed in the main study population, and in the subpopulations of patients with COPD and non-COPD. Statistical significance was defined as p<0.05.
Ethical considerations
Written informed consent was obtained from all participants and the protocol was approved by the Regional Ethical Board at Lund University (DNr: 2016/16). D-12 was used in this project with the permission of the copyright holder, Professor Janelle Yorke, UK.
Results
A total of 182 patients were included. The main underlying diagnoses in the study population were COPD (25%), asthma (21%), heart failure (19%) and IPF (19%). Other conditions mainly included different hypoventilation conditions. Mean age of the study population was 69 years, 53% were women and 10% were current daily smokers. Further details of the study population have been presented elsewhere.26 The mean D-12 total score (±SD) was 16.0 (±9.2), the mean physical domain score was 9.8±5.3 and the mean affective domain score was 6.1 (±4.4). There were no substantial differences between the mean scores for the single items within the respective domains (data not shown).
Follow-up data were available for 179 patients (98%) after 30–90 min and for 162 patients (89%) after 2 weeks. An attrition analysis showed no significant differences in baseline characteristics for the populations completing Q1 and Q3 (data not shown). The actual mean time between Q1 and Q3 was 17 (SD 8; range 3–58) days.
The factor analysis was consistent with the previously proposed two component structures of D-12: the physical and the affective subdomains. Model fit was good (RMSEA=0.080) and CFI=0.969). The factor loading for each item is shown in table 1. The analysis identified one component with an eigenvalue of 7.0, explaining 61% of the variance, and a second component had an eigenvalue of 1.3 explaining another 11% of the variance.
Confirmatory factor analysis of the Swedish Dyspnoea-12
Internal consistency and test–retest reliability for D-12 in the entire population and in patients with and without COPD are shown in table 2. Internal consistency was very good for the D-12 total score, good for the physical domain and acceptable for the affective domain. The test–retest reliability for the D-12 total and domain scores was acceptable (range 0.73–0.81). There was no evidence for a learning effect, as the ICCs were slightly higher between Q1 and Q2 (table 3). The correlation and agreement between D-12 total score at Q1 and Q2 are shown in figure 1.
Dyspnoea-12 measurement properties for the Swedish Dyspnoea-12
Test–retest reliability for the Swedish Dyspnoea-12
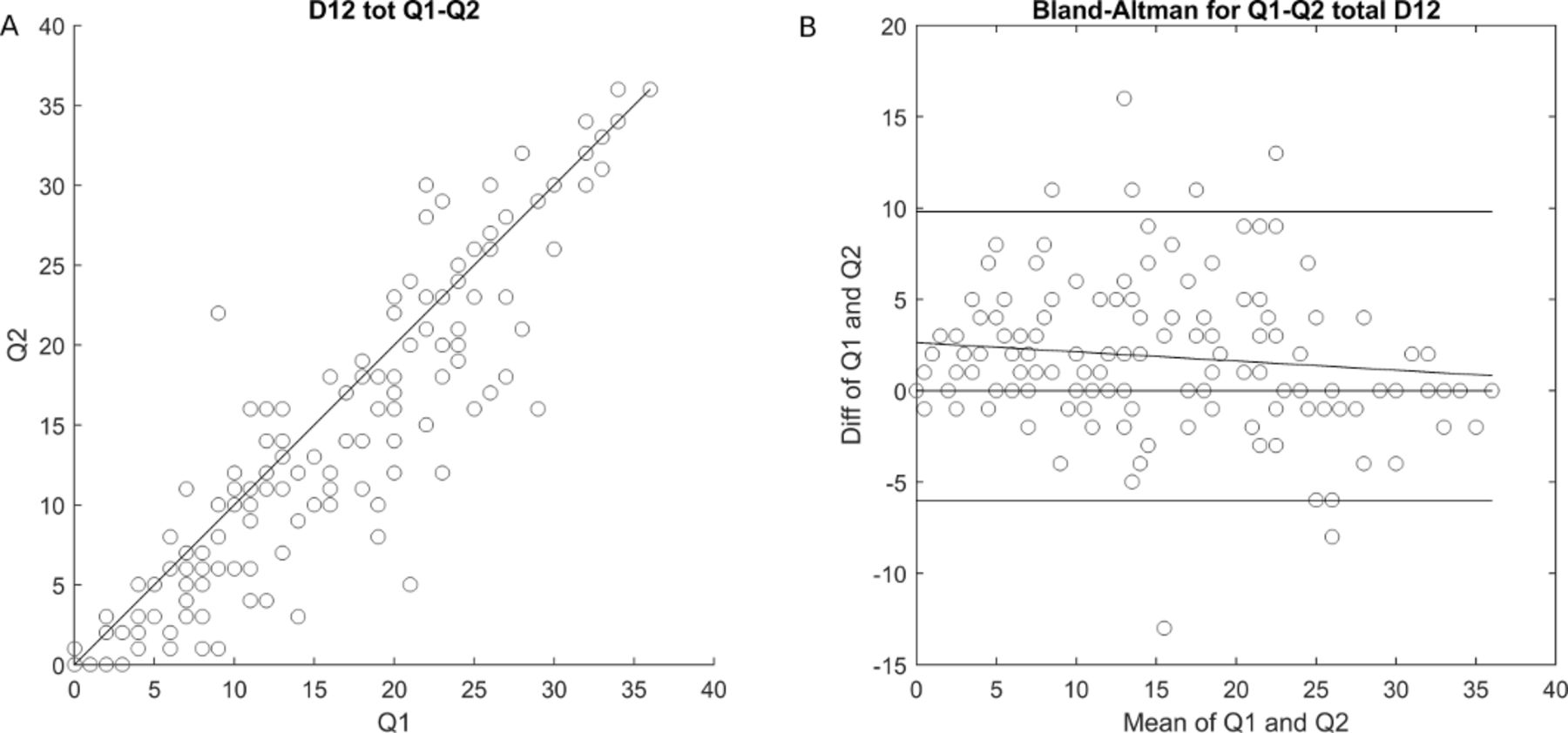
Correlation and agreement of the Swedish Dyspnoea-12, Correlation and agreement of the Dyspnoea-12 in patients with unchanged breathlessness, between baseline and after 30–90 min. (A) Scatterplot with a 45° line (no difference) and a simple linear regression line with Pearson’s correlation coefficient (r). (B) Bland-Altman plot with lines for mean bias and 95% limits of agreement.
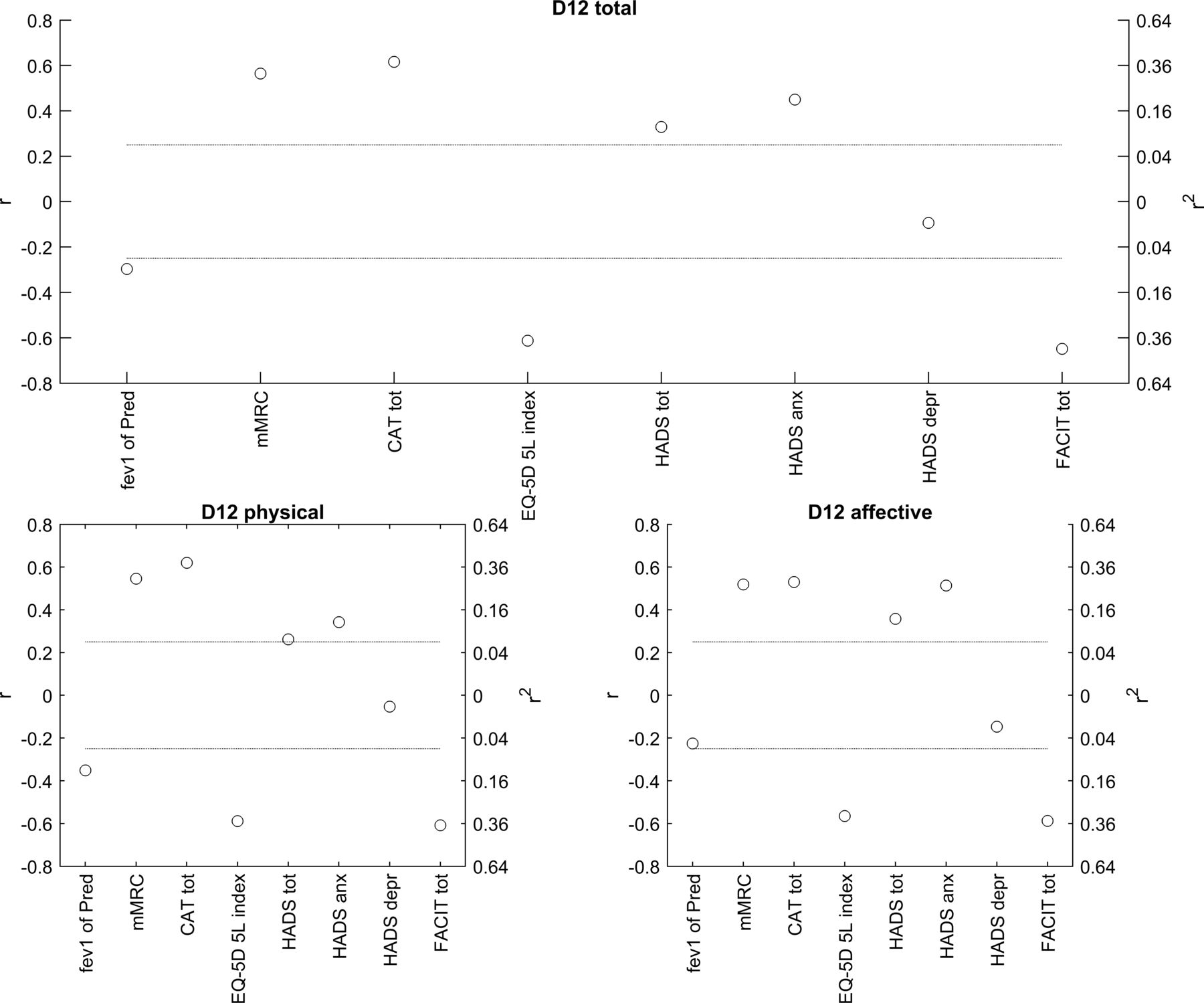
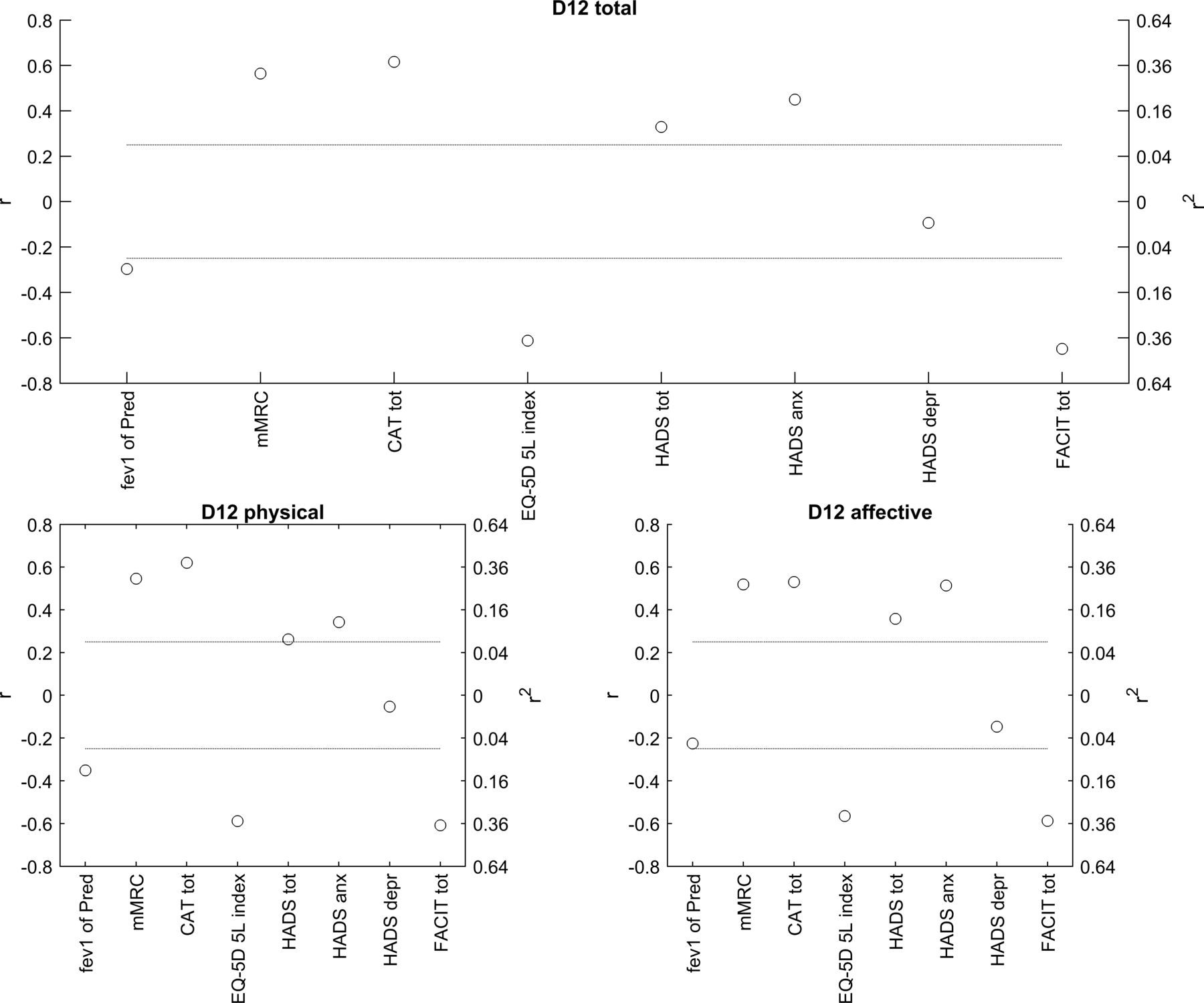
Concurrent validity estimates for D-12 total and subdomain scores in the main study population are shown in figure 2 and table 3, and for the subpopulations with and without COPD in table 3. Higher total score on D-12 correlated with mMRC, CAT, EQ-5D index, HADS total and anxiety scores and FACIT-fatigue. There was also a somewhat weaker correlation with HADS depression score and FEV1%pred (table 3). In the entire study population, the D-12 total and domain scores all correlated strongest with mMRC, CAT, EQ-5D and FACIT-fatigue, and the affective domain with HADS anxiety score. The same pattern was seen in patients both with COPD and with other underlying conditions.
{kind=link}
{kind=link}
Concurrent validity for the Swedish Dyspnoea-12. Correlations for the Dyspnoea-12 total and subdomain scores with patient-reported outcomes and FEV1%pred were analysed using Pearson’s correlation coefficient. The dotted lines correspond to an adjusted significance level of 0.002. CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; EQ-5D-5L, Euro-QoL-5 Dimensions-5 Levels; FACIT-Fatigue, Functional Assessment of Chronic Illness Therapy-Fatigue; FEV1%pred, forced expiratory volume in 1 s in percentage of predicted value; HADS, Hospital Anxiety and Depression Scale; mMRC, modified Medical Research Council.
Discussion
Main findings
The main finding of this study is that the D-12 is valid in terms of the factor structure, internal consistency, test –retest reliability and concurrent validity for multidimensional measurement of breathlessness in Swedish outpatients with cardiorespiratory disease. The measurement properties were similar between patients with COPD and patients with other diagnoses.
Comparison with previous literature
The factor analysis confirmed the two-component structure with a physical and an affective subdomain, with the same explanation of variance, as presented in the original validation study by Yorke et al.11 The descriptor ‘irritating’ within the affective subdomain somewhat surprisingly loaded more for the physical domain than for the affective domain. However, the value for the affective subdomain was just below statistical significance, which makes the pattern rather consistent with the original paper of D-12, where the item ‘irritating’ loaded in both subdomains. The item ‘my breath does not go in all the way’ did not load significantly for any subdomain, but there was a clear tendency for higher loading of the physical subdomain as expected. The descriptors ‘exhausting’ and ‘distressing’ loaded significantly for both subdomains but with higher values for the expected subdomains. We believe that although a careful translation and linguistic validation has been performed, there may be different nuances and meanings of some words in the English and Swedish language that can explain the small differences in factor analysis.
The internal consistency for D-12 total score was high and similar to the original validation study. The reliability was acceptable at 0.81 although it did not fully reach the optimal level of 0.90 which was reported in the original validation study.11 The concurrent validity was consistent with previously reported correlations of D-12 with HADS, mMRC, CAT and forced expiratory volume in 1 s, in the English, Arabic and Portuguese validation studies.11–13 16 17 19
What this study adds?
The present study validates the use of D-12 in Swedish, which will facilitate research of breathlessness across various languages and populations. It is also the first study validating D-12 with the time frame of the previous 2 weeks, with no evidence of a learning effect, in outpatients across a range of important cardiorespiratory diseases including COPD, asthma, heart failure, hypoventilation conditions, IPF and other interstitial diseases. Finally, the concurrent validity toward EQ-5D index and FACIT-fatigue is a novel finding.
Strengths and limitations
Main strengths of this study are that we have validated the instrument in a mixed clinical population with different cardiorespiratory diseases including severe stages and from multiple centres, which likely yields high external validity. Follow-up questionnaires had only a small amount of missing data. A limitation is that the number of patients in each of the diagnosis groups were relatively small and did not allow subgroup analysis except for the COPD group where the number was slightly higher. However, with reservation for the low power, the present analysis shows no evidence that the measurement properties of D-12 differ substantially between outpatients with COPD and other cardiorespiratory diagnoses.
Implications and future research
The results support that D-12 is valid for multidimensional measurement of breathlessness during the previous 2 weeks in outpatient with cardiorespiratory diseases. The absence of a learning effect indicates that the instrument can be used without training but with careful instructions. The validated Swedish version of D-12 may be used both in clinical routine in Sweden and for research in multinational studies. The D-12 is copyrighted by the developer but can, after permission, be used free of charge for non-industry funded research. Future research should investigate minimal clinically important difference of D-12 and its responsiveness as endpoint to adequately capture treatment effects in clinical trials.
We conclude that the Swedish version of D12 is a valid instrument for multidimensional assessment of breathlessness in cardiorespiratory diseases.
Patient and public involvement
The development of the research question and outcome measures was based on previous knowledge from the development of the original version of D-12 in UK, which included qualitative studies with patient interviews. The previously published linguistic validation of the Swedish D-12 also included an in-depth interview with five patients, with the intention to assess whether the questionnaire was comprehensible and acceptable for them. Recruitment to the present study took place in clinical praxis, and subsequently patients were not involved in the recruitment to and conduct of the study. Feedback of the results are forwarded to included patients at routine clinical visits.
Acknowledgments
Thanks to Karin Johansson, Örebro University Hospital, for help with recruitment, data input and quality checking; to Lisa Carlson, Karolinska University Hospital Solna, Stockholm; Annika Johansson and Frida Holmström, Umeå University Hospital; Tove Nilsson and nurses at the Respiratory Outpatient Clinic in Karlskrona for recruitment; and to Jonatan Blomqvist in Lund for help with data input and quality checking.
References
Footnotes
Contributors Conception and design: ME; Data collection: ME, MS, CJ, AB, JaS, HI, JoS; Statistical analysis: HB, AB-H; First draft: JoS; Interpretation, revision for important intellectual content and approval of the version to be published: all authors.
Funding The translation was funded by unrestricted grants from the Swedish Respiratory Society, the Swedish Heart−Lung Foundation and the Swedish Society for Medical Research.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request.