Article Text

Abstract
The assessment of exercise-induced bronchoconstriction (EIB) in athletes requires the measurement of forced expiratory volume in 1 s (FEV1) before and after vigorous exercise or a surrogate of exercise such as eucapnic voluntary hyperpnoea (EVH) of dry air or mannitol dry powder. Exercise testing in a laboratory has a low sensitivity to identify EIB, and exercise testing in the field can be a challenge in itself particularly in cold weather athletes. The EVH test requires the subject to ventilate dry air containing ∼5% CO2 for 6 min through a low-resistance circuit at a rate higher than that usually achieved on maximum exercise. A ≥10% reduction in FEV1 is a positive response to exercise and EVH and, when sustained, is usually associated with release of inflammatory mediators of broncho constriction. Another surrogate, mannitol dry powder, given by inhalation in progressively increasing doses, is used to mimic the dehydrating stimulus of exercise hyperpnoea. A positive mannitol test is a 15% fall in FEV1 at ≤635 mg and reveals potential for EIB. Mannitol has a high specificity for identifying a clinical diagnosis of asthma. Once a diagnosis of EIB is established, the athlete needs to know how to avoid EIB. Being treated daily with an inhaled corticosteroid to reduce airway inflammation, inhaling a β2 agonist or a cromone immediately before exercise, or taking a leukotriene antagonist several hours before exercise, all inhibit or prevent EIB. Other strategies include warming up prior to exercise and reducing respiratory water and heat loss by using face masks or nasal breathing.
Statistics from Altmetric.com
Introduction
Exercise-induced bronchoconstriction (EIB) is the term used to describe the transient narrowing of the airways that follows vigorous exercise. The cause of EIB is likely due to the thermal and osmotic consequences of water lost by evaporation in humidifying large volumes of air in a short time.1 The mechanism whereby these dehydrating effects cause transient airway narrowing involves the release of inflammatory mediators that cause contraction of airway smooth muscle (ASM) with or without oedema.1 Diagnosis of EIB is commonly based on airway response to exercise. Alternatively, surrogates of exercise, such as dry air hyperpnoea or inhalation of mannitol dry powder, that mimic the dehydration effect of exercise hyperpnoea on the airways can be used (figure 1).2 Interventions that reduce the respiratory water loss during exercise, such as wearing face masks or inhaling warm humid air, inhibit EIB. Pharmaceutical agents that either reduce the numbers of inflammatory cells, or prevent the release of their mediators, or block the effect of the mediator on the ASM, inhibit EIB.

The events that lead to airway narrowing and a reduction in forced expiratory volume in 1 s in response to exercise, eucapnic voluntary hyperpnoea and mannitol. Reproduced with permission.2
Diagnosis of exercise-induced bronchoconstriction
A diagnosis should not be based on respiratory symptoms because they are neither sensitive nor specific for identifying EIB in athletes.3,–,6 The diagnosis of EIB in athletes is made by measuring changes in forced expiratory volume in 1 s (FEV1) following exercise, or a surrogate for exercise such as eucapnic voluntary hyperpnoea (EVH) or mannitol.7 Exercise can be performed in a laboratory but sports-specific exercise in the field, under the usual environmental conditions for the athlete, is more likely to reveal EIB.8 The EVH test requires voluntary hyperpnoea of dry air at high ventilation. EVH is a very potent challenge and not recommended as a first challenge for those with an established diagnosis of asthma.9
For those with a diagnosis of asthma, an initial challenge with dry powder mannitol may be used because the progressive dose-response protocol avoids the large falls in FEV1 often experienced following exercise or EVH.10 Challenge with mannitol is less sensitive than EVH11 (figure 2), but it is highly specific for identifying the bronchial hyper-responsiveness of clinical asthma.10 If the mannitol test result is negative, then if the subject has asthma it is likely only to be mild, and an EVH test is suitable.12
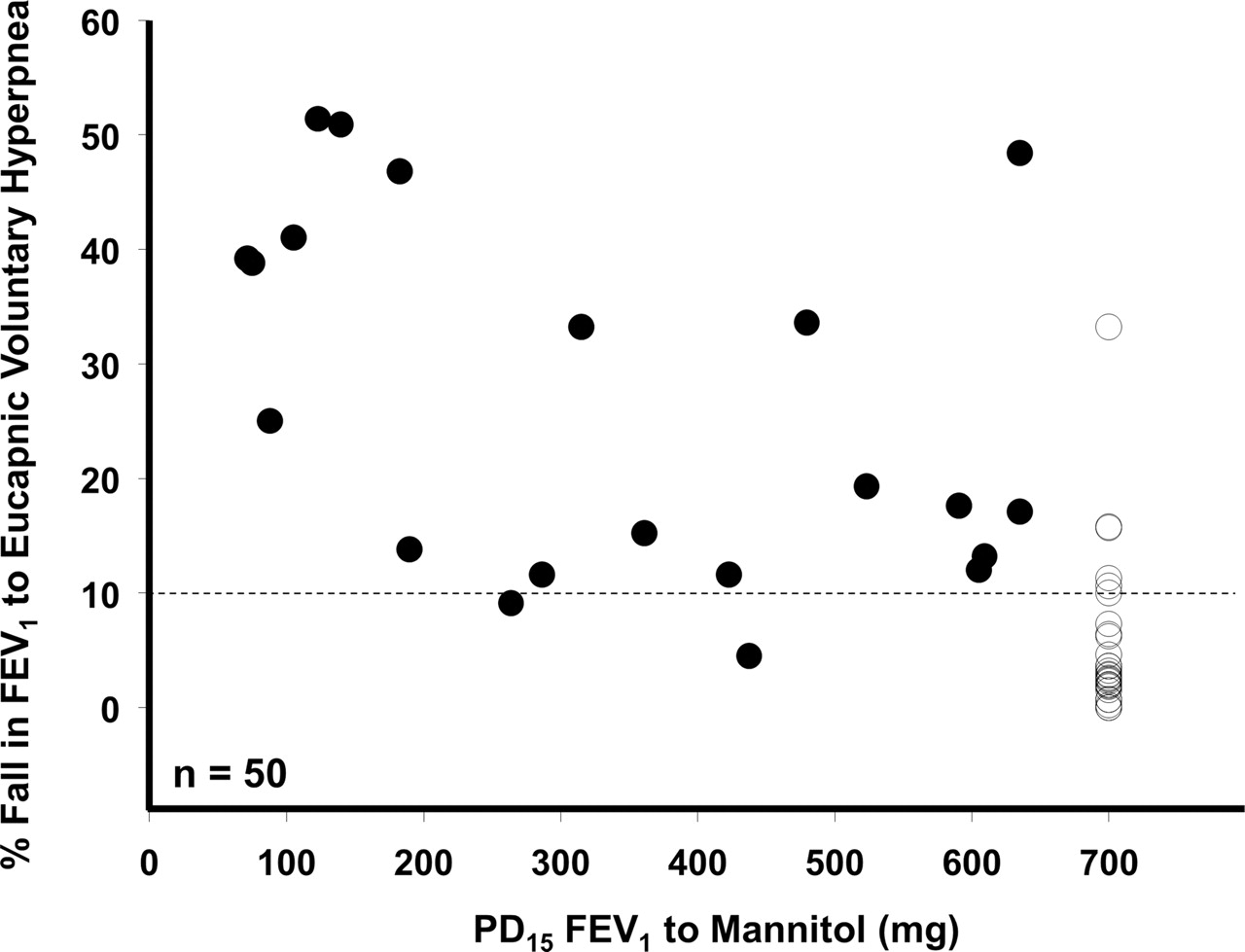
Provoking dose of mannitol to induce a 15% fall in forced expiratory volume in 1 s in relation to the fall following 6 min of eucapnic voluntary hyperpnoea (EVH) of dry air. Note that three or four subjects are negative to mannitol and positive to EVH, and two subjects are positive to mannitol and negative to EVH. The data are drawn from those in the online repository.11
Exercise challenge testing to identify EIB
There is a high rate of false-negative tests for EIB when exercise testing is carried out in a laboratory.8 This is due to the many factors that can affect the airway response to exercise and to the natural variability of EIB.13 The type, duration and intensity of exercise, the temperature and water content of the air inspired, and the time since exercise last provoked airway narrowing all affect the severity of the response. Further, many medications need to be withheld for appropriate periods.14
The best protocol to detect EIB in the laboratory involves a rapid increase in exercise intensity over about 2 to 4 min to achieve a high level of ventilation. The intensity of the exercise is best measured by ventilation, but if this is unavailable heart rate can be used. Most protocols recommend breathing medical grade dry air with a nose clip in place while running or cycling at a load sufficient to raise the heart rate to 80% to 90% of predicted maximum (∼ 220-age in year).13 For athletes, the ventilation needs to be as high as possible and probably >25 times the FEV1 instead of the usual 17.5 to 21 times FEV1. The athlete should continue to exercise at that high level for an additional 4 to 6 min. These targets are more rapidly achieved with running exercise, compared with cycling. Sports-specific exercise that produces the symptoms, performed either in the laboratory or in the field, is probably the most relevant for testing elite athletes.8 However, environmental conditions, such as humidity and temperature levels, pollen count and pollution level, may greatly affect the response in the field.
Measurements of FEV1 are made usually in duplicate at 3, 5, 10, 15, 20 and 30 min after exercise, and the higher of the two reproducible values is recorded. The difference between the prechallenge FEV1 value and the lowest FEV1 value recorded within 30 min after the challenge is expressed as a percentage of the prechallenge value and is called the % fall index. The criterion to diagnose EIB in athletes is ≥10% fall in FEV1 and preferably this level of severity should be present at two consecutive time points after challenge. The severity of EIB can be graded as mild, moderate or severe if the % fall in FEV1 from prechallenge value is ≥10% but <25%, ≥25% but <50%, and ≥50%, respectively.
Surrogates for exercise to identify EIB
Eucapnic voluntary hyperpnoea
EVH is an excellent surrogate for exercise because the ventilation achieved voluntarily is higher than that achieved during maximum exercise. Thus, the rate of false-negative tests is very low with EVH.15 The 6-min EVH protocol was developed and validated for use in defence force recruits.9 16 The ‘standardised’ protocol requires the subject to inspire a dry gas containing 4.9–5% carbon dioxide, 21% oxygen and nitrogen at a ventilation equivalent to 30 times FEV1 or more. In elite athletes, in whom maximal ventilation is often known, 85% of maximal ventilation is recommended.17 While some subjects may fail to achieve the target, the minimum ventilation rate for a valid test for untrained subjects is 21 times FEV1.18 After the test the measurements are made at the same time interval as for exercise (see above), and a sustained ≥10% fall in FEV1 following EVH is consistent with EIB. A positive EVH test is associated with an increase in urinary excretion of the same inflammatory mediators (ie, prostaglandins and leukotrienes) as exercise, although the values in athletes tend to be lower than in recognised asthmatics.19 20
Dry powder mannitol
Inhaling dry powder mannitol increases the osmolarity of the airway surface and causes release of the same inflammatory mediators as exercise and EVH.21 22 The commercially available kit comes with prepacked capsules containing 5, 10, 20 or 40 mg of mannitol and an inhaler device.12 The FEV1 is measured in duplicate 60 s after each dose. A positive test result is 15% fall in FEV1 at ≤635 mg. This value represents the mean plus two SDs of the % fall in healthy non-asthmatic subjects.10 Repeatability of the test is ±1.0 doubling dose. Recovery of FEV1 from mannitol-induced bronchoconstriction is spontaneous.10 12 There is a good relationship among the PD15 to mannitol, the % fall to exercise and EVH in those with known asthma, not taking inhaled steroids.23 The response is not as strong in those taking inhaled steroids or in those without a definite diagnosis of asthma.23 The sensitivity of mannitol to identify subjects with ≥10%, ≥15% and ≥20% fall in FEV1 on at least one of two exercise tests was 64.1%, 75.3%, 82.7% when the mannitol test time was ≤35 min.12 In this group of subjects the EIB was very mild (median fall of 15.5%).12
Hypertonic saline
Hypertonic (4.5%) saline is also used to identify bronchial hyper-responsiveness and potential for EIB in known asthmatics.24 A large volume ultrasonic nebuliser is required, and the aerosol is inhaled via a two-way valve for increasing time intervals (0.5, 1, 2, 4 and 8 min).25 The amount of aerosol administered is measured as a change in weight of the nebuliser. A 15% fall in FEV1 to ≤23 g is a positive response.25 The sensitivity of a PD15 to 4.5% saline to identify EIB (≥10% FEV1 fall) was 53.9% with a specificity of 84.7% in 348 children.26
Methacholine and histamine
While bronchial provocation testing with methacholine and histamine are used to aid in the diagnosis of asthma, the interpretation of the results with respect to identifying EIB is debatable. Numerous winter athletes positive to a methacholine challenge did not bronchoconstrict when exposed to indirect stimuli such as exercise, EVH or mannitol.5 The reason for this dissociation is not understood, but it may be linked to airway injury in the pathogenesis of the bronchial hyper-responsiveness to methacholine.27 In athletes who perform in cold dry air or in polluted environments (such as swimming pools or ice-rinks), methacholine or histamine challenge for diagnosis of EIB is therefore discouraged. The fact thatcross-country skiers with ‘ski asthma’ (ie, asthma-like symptoms and bronchial responsiveness to methacholine) did not respond to inhaled corticosteroid therapy, lends support to this recommendation.28
A study comparing EVH and methacholine in swimmers found the majority of those positive to EVH had a methacholine PD20 <2 µmol (equivalent to PC20 4 mg/ml).29 However, there are discordant findings where the EVH has been positive and the methacholine negative.4 30 The reason for this is not understood but good lung function is often associated with a negative methacholine test result.31 Further, the inflammatory mediators such as leukotrienes and prostaglandins, released in response to the indirect challenges, are 1000 and 100 times, respectively, more potent than methacholine and histamine.
A recent meta-analysis reported that neither mannitol nor EVH are sensitive enough to identify EIB in all subjects.32 The ‘gold standard’ was response to an exercise test. However, an exercise test is the least sensitive test to identify EIB in a laboratory, and it has poor repeatability over a short period.13 Further, a negative exercise test result was quite common in a person positive to EVH or positive to mannitol. The low sensitivity of laboratory-based exercise is the reason that EVH was originally used to evaluate armed forces recruits16 and elite athletes.9 Mannitol testing, in subjects with symptoms of asthma but without a definite diagnosis, revealed a frequency of a 15% fall in FEV1 1.65 times that achieved after a single exercise test.12 Mannitol, however, is not as sensitive as EVH to identify EIB in elite athletes.11
When no objective evidence of reversible airway obstruction or bronchial hyper-responsiveness is obtained in a symptomatic athlete, an alternative diagnosis, such as dysfunctional breathing or vocal cord dysfunction, should be considered.33 34 Furthermore, since seasonal variability affects the occurrence of bronchial hyper-responsiveness and EIB in various athletic groups (such as swimmers and runners), the timing of bronchial provocation testing should be carefully decided.35 36 Finally, for athletes who are taking inhaled corticosteroids daily, a negative test result may indicate satisfactory control of airway inflammation.37 38
Management of EIB
EIB severity is markedly reduced by inspiring warm humid air during exercise.39 Severe EIB can occur, however, when hot dry air is inspired.40 Thus, it is the water loss rather than heat loss that is the primary stimulus to EIB. The inflammatory cells involved are the mast cells and eosinophils. The mast cells occur superficially in the airways in large numbers in asthmatic and healthy subjects41 and contain mediators of bronchoconstriction such as histamine, prostaglandins and leukotrienes. Eosinophils may also be present in large numbers in the airways of asthmatics and are also a source of leukotrienes. The release of the same mediators, follows challenge with exercise, EVH and mannitol, and the same drugs are effective in inhibiting these three challenges.19,–,21 42,–,46 Release of neuropeptides from sensory nerves in the airways may also play an important role, but information is limited due to lack of approved antagonists.
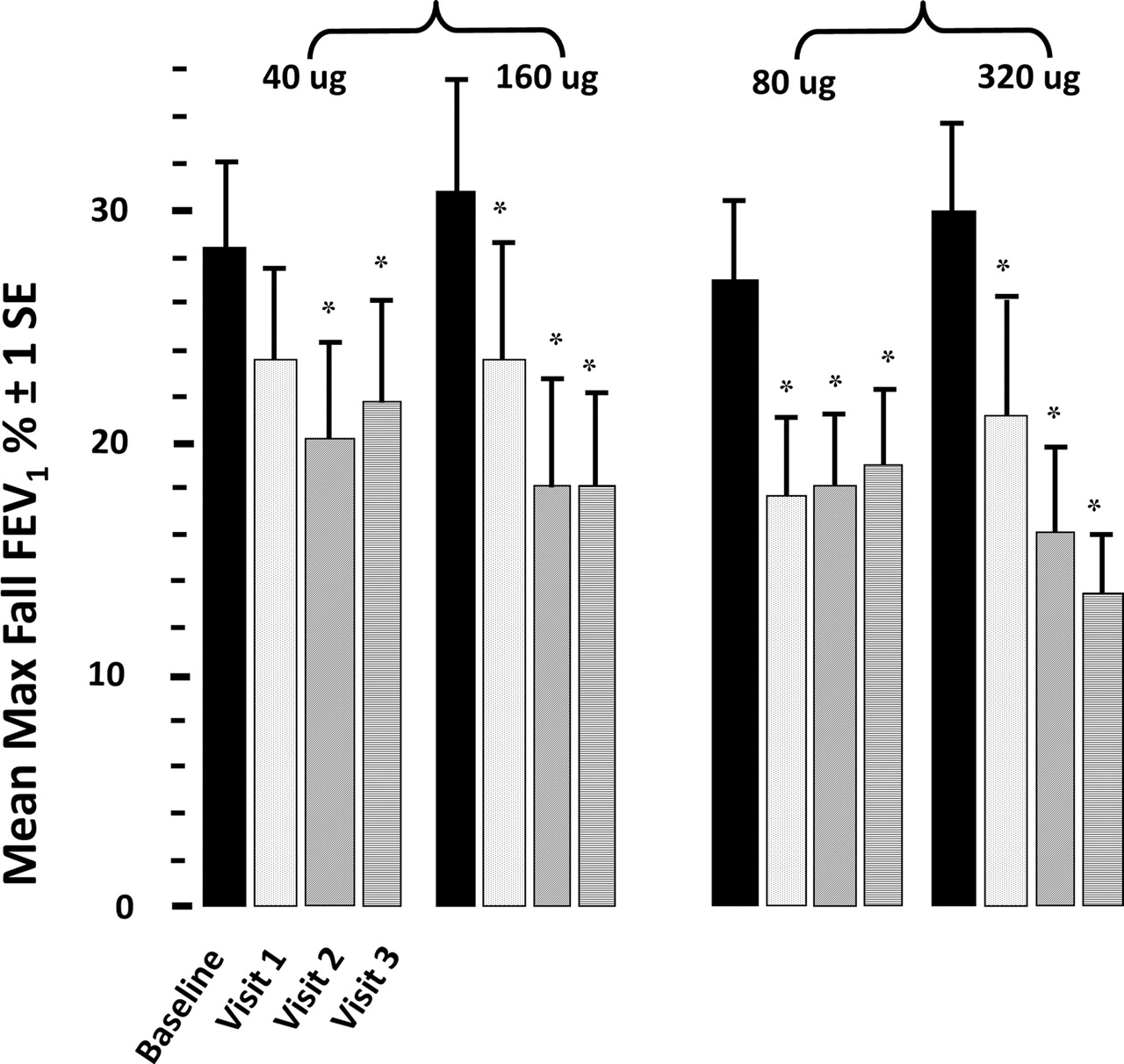
Inhaled corticosteroids alone, given on a daily basis, have been shown to reduce the severity of EIB in all studies although the effective dose and duration of treatment needed varies between the different preparations (figure 3).37 The doses that are clinically recommended usually take days to weeks.37 While very high doses, inhaled a few hours before exercise,20 are also effective, they are not clinically recommended. Further, the severity of EIB has been reduced in those asthmatics who have remained on inhaled cortico steroids (ICS)but withdrawn from their long-acting β2 agonist.47

Maximum decrease in forced expiratory volume in 1 s (FEV1) (max fall) in mildly symptomatic asthmatics aged 14–27 years in response to 8 min of running exercise while breathing dry air at Visit 1 baseline, Visit 2 after 1 week, Visit 3 after 2 weeks and Visit 4 after 3 weeks. The maximum decrease in FEV1 decreased after 1 week of therapy in all but the 40-μg dose, and in all subsequent weeks. Rate of improvement in the low-dose (40/80 μg) plateaued after 1 week of therapy while continuing to improve weekly in the high-dose groups (160/320 μg) *p<0.05. Redrawn from the original with permission.37
Inhaling a β2 agonist aerosol immediately before exercise is a highly successful method for preventing EIB.48 However, caution is needed using this approach in athletes who exercise many times a day.48 The reason is that tolerance develops to the protective effects of short-acting and long-acting β2 agonists when they are taken on a daily basis. The tolerance develops rapidly over days49 and is most evident as a reduction in the duration of the protective effect on EIB.50 51 In those taking these drugs on a daily basis there can be an increase in severity of EIB52 and a slower recovery of lung function following provoking stimuli.53 The tolerance does not appear to be controlled by simultaneous use of inhaled corticosteroids.54 Tolerance is probably due to desensitisation of β2 receptors, particularly on the mast cells,55 which is why it is more evident when these drugs are used every day to inhibit EIB.48
Cromone drugs such as sodium cromoglycate and nedocromil sodium, inhaled immediately before exercise, inhibit EIB by about 60%.56 The duration of this protective effect is short and usually <4 h. No tolerance to repeated dosing has been reported. The leukotriene antagonist montelukast also provides about 60% protection. Montelukast is not effective in all subjects, but for some the protection can last 24 h.51 Montelukast can be taken as a single dose, or as repeated daily doses. Tolerance does not occur if doses are repeated daily over weeks.51 Leukotrienes prolong the presence of EIB and the antagonists reduce the time to recover to the pre-exercise FEV1. Histamine antagonists provide limited benefit, however, one study has shown a good inhibition of EIB and even a reduction in mediator release when loratadine was used in combination with montelukast.57 As an alternative or adjunct to pharmacological treatments, fish oil has been reported to inhibit mild EIB and reduce release of mediators.58
As with any form of pharmacological treatment, physicians are advised to check the prohibited list of the World AntiDoping Agency before commencing treatment on an elite athlete.59 The prohibited list is updated on a yearly basis and should therefore be checked.
There are other means used to reduce severity of EIB. Warm-up exercise before intense exercise has long been recognised as having an inhibitory effect on EIB,60 and this approach enhances the benefit of a β2 agonist.61 A refractory period (usually <2 h), follows EIB in about 50% of asthmatic subjects.62 The mechanism for this is unclear but it is unlikely that it is due to mediator depletion.22 As the refractory period is abolished in the presence of indomethacin and other non-steroidal drugs it has been suggested that it involves release of protective prostaglandins.63 Breathing via the nose rather than mouth reduces severity of EIB.64 Studies using face masks to reduce water loss and heat have been reported benefit. One study reported enhanced benefit from a β2 agonist in the presence of a face mask (figure 4).65

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in forced expiratory volume in 1 s in nine asthmatic patients after exercise at temperature of −10°C. Results were obtained after patients performed test either with no therapy, or with premedication with β2 agonist, or with heat and moisture exchanging filter alone or in combination with β2 agonist. Mean values (expressed in percentage of pre-exercise value) are shown. ‘B’ denotes ‘before’ exercise; bars represent standard error. Reproduced from.65
In conclusion, to provide athletes with the best level of medical care, it is essential that appropriate lung function testing is carried out. Alongside the usual clinical examination, bronchial provocation testing with exercise (or a surrogate) assists, in the making of the diagnosis and in the management of the disease.
References
Footnotes
-
Competing interests SDA is the inventor of the mannitol test known as AridolTM and OsmohaleTM. The intellectual property is owned by her employer Sydney South-West Area Health Service (SSWAHS) and is licensed to Pharmaxis Ltd (Frenchs Forest NSW AUS). SDA owns shares in Pharmaxis Ltd but no options. She receives a 10% share of the royalties paid to SSWAHS.
-
Provenance and peer review Commissioned; internally peer reviewed