Article Text

Abstract
Background: Nitrite is the main oxidation product of nitric oxide (NO) in plasma. It sensitively reflects changes in endothelial NO synthase (eNOS) activity under fasting conditions and serves as an endocrine NO donor, contributing to the regulation of blood flow through reaction with haemoglobin. As NO is necessary to maintain an adequate vascular response to the increased demands of blood flow, it is believed to be important for vasodilation induced by exercise.
Objective: To investigate whether the capacity of the vasculature to produce nitrite is associated with exercise performance.
Design: With the use of chemiluminescence detection, nitrite concentrations in 55 healthy subjects (mean (SEM) age 40 (2) years; 22 men) were studied before and after an exercise test, and endothelial function was determined by measuring flow-mediated dilation of the brachial artery using high-resolution ultrasound. In a subset of subjects, the NOS inhibitor, NG-monomethyl-l-arginine, was applied to elucidate the effect of eNOS on changes in nitrite.
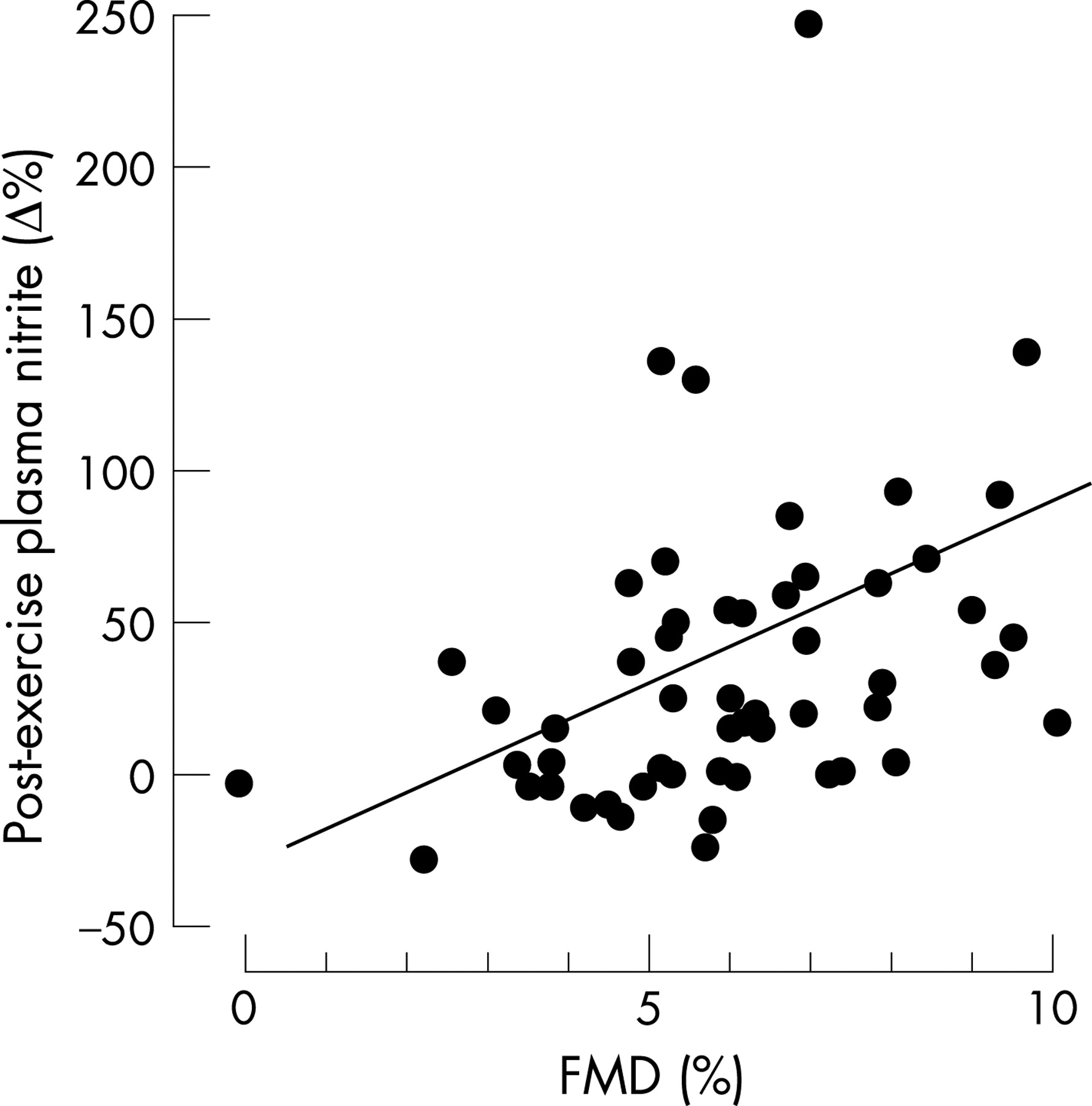
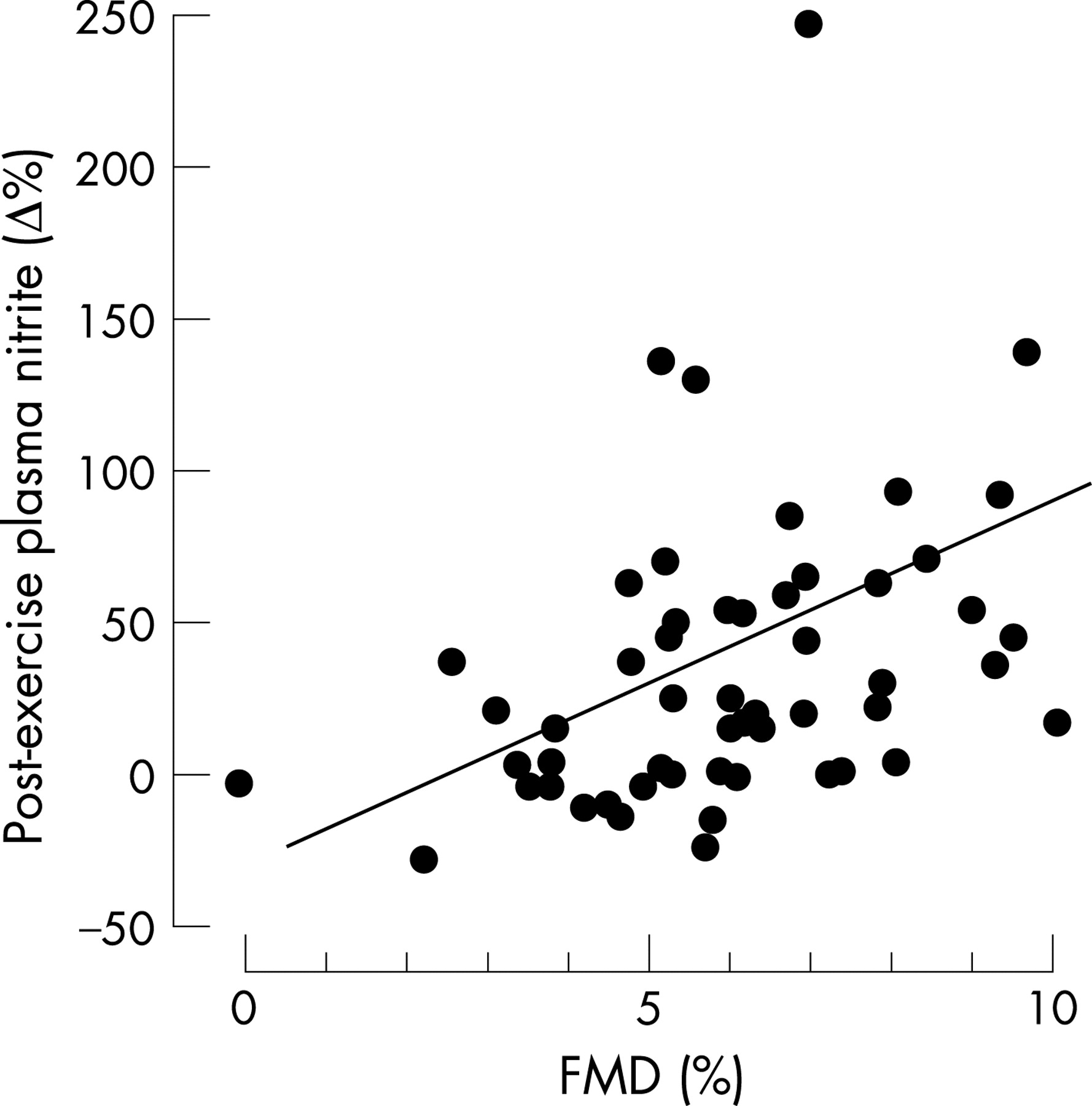
Results: Exercise significantly (p<0.001) increased plasma nitrite from 97 (6) to 125 (8) nM. The relative increase in plasma nitrite was related to flow-mediated dilation (6.1 (0.3)%; r = 0.36; p = 0.01). NG-Monomethyl-l-arginine blocked increases in nitrite. Post-exercise nitrite concentration correlated with exercise performance, as determined by maximally reached stress power (r = 0.37; p<0.007), and inversely with age. Multivariate analysis showed that both age and post-exercise nitrite concentration were independent predictors of stress endurance and power.
Conclusion: The results suggest a role for plasma nitrite in the adaptation of haemodynamics during exercise. An impaired increase in plasma nitrite may limit exercise capacity.
- nitrite
- exercise capacity
- nitric oxide
Statistics from Altmetric.com
Endothelium-derived nitric oxide (NO) is crucial for the maintenance of vascular homoeostasis. Nitrite is the main oxidation product of NO in plasma and sensitively reflects acute and chronic changes in endothelial NO synthase (eNOS) activity in healthy volunteers under fasting conditions.1 2 Increases in local plasma nitrite after ischaemia of the forearm vasculature have been shown to reflect endothelial function.3 As endothelium-derived NO is necessary to maintain an adequate vascular response to the increased demands of blood flow during exercise,4 endothelial function is believed to be important for vasodilation induced by exercise. The fall in blood flow resistance is a major factor in the increase in cardiac output during exercise. This reduction in systemic vascular resistance is mediated by endothelium-induced vasodilation. It has been shown that exercise increases NOX (the sum of nitrite and nitrate) concentrations.5 6 NOX concentrations are, however, influenced by various NO-independent factors.2 Thus, the impact of exercise on vascular NO formation and whether changes in nitrite formation influence exercise is still not known.
In this study, we investigated whether the capacity of the vasculature to produce nitrite is associated with exercise performance. We determined plasma nitrite concentrations at rest and after an ergometric exercise test in 55 healthy volunteers and correlated the results with exercise performance, as well as with NOS-dependent endothelial function. To determine whether changes in nitrite were dependent on NOS, we repeated the exercise tests under conditions of systemic NOS inhibition.
METHODS
Study subjects
We studied 55 healthy subjects (mean (SEM) age 40 (2) years; 22 men) without clinical evidence of cardiovascular risk factors. All were asymptomatic, normotensive (as defined by systolic blood pressure <140 mm Hg and diastolic blood pressure <90 mm Hg), non-diabetic (as defined by fasting glucose concentrations <126 mg/dl), normocholesterolaemic (as defined by total cholesterol concentrations <240 mg/dl and low-density lipoprotein cholesterol concentrations <160 mg/dl), and non-smokers.7–9 The subjects had no noteworthy medical history and were not taking regular or incidental medication, including contraception or hormone replacement therapy. Table 1 summarises the clinical characteristics. The study protocol was approved by the local ethics committee, and written informed consent was obtained from all subjects.
Determination of endothelium-dependent and endothelium-independent vasodilation
Endothelium-dependent dilation of the brachial artery was measured non-invasively by high-resolution ultrasound (SONOS 5500 with a 15 MHz linear-array transducer; Agilent, Andover, MA, USA) using standard techniques as previously described10 on a separate day from the ergometric exercise test. Briefly, baseline data for diameter and blood-flow velocity of the brachial artery 1–2 cm above the elbow were quantified after 10 min of supine rest in an air-conditioned room (21°C). Then a blood-pressure cuff was placed around the forearm distal to the cubital fossa and inflated to 200 mm Hg for a period of 5 min.11 Diameter and blood-flow velocity were measured immediately after deflation of the cuff as well as 60, 75, 90 and 120 s later. Maximal brachial artery diameter observed during this time period was used to calculate flow-mediated dilation (FMD). Endothelium-independent dilation of the brachial artery was quantified 4 min after sublingual administration of 400 μg glycerol trinitrate (Nitrolingual mite; Pohl, Germany). All ultrasound scans were performed by the same operator using the same equipment. An automated analysis system was used to measure diameters (Brachial Analyzer; Medical Imaging Applications, Iowa City, Iowa, USA), yielding low variabilities in our methodology as described elsewhere.3 Internal quality control was performed by an independent investigator blinded to the protocol (96% approved). FMD and endothelium-independent dilation were expressed as percentage change from baseline.
Ergometric exercise test
All subjects underwent an ergometric exercise test with a stepwise increase in force. Before the exercise test, a 20 G intravenous catheter was placed in the cephalic vein. Blood samples (5 ml) were taken before exercise (baseline) and 10 min after exercise termination (peak). The time of the peak (10 min) was determined in a subset of 15 subjects: blood was drawn consecutively for 60 min (data not shown).
Exercise was stopped when subjects were not able to continue, showed clinical symptoms that met the test termination criteria, or reached maximum heart rate (heart rate 220−age (years)).12 Maximal duration and power were the primary read-out of exercise capacity. Before, during, and after the exercise test, heart rate and 12-lead ECG were recorded continuously. Blood pressure measurements were obtained every minute throughout and until 5 min after the test.
The effect of NG-monomethyl-l-arginine (L-NMMA; Clinalfa, Schwalbach, Germany), a competitive NOS inhibitor, on changes in nitrite concentration after exercise was determined in a subset of five healthy subjects (mean (SEM) age 25 (2) years; two women). L-NMMA was administered intravenously via the right antecubital vein at a dose of 1 mg/kg/min for 3 min followed by a continuous infusion of 0.2 mg/kg/min until the end of the experiment.13 To ensure complete NOS inhibition, L-NMMA was continuously infused for 60 min before exercise, and FMD suppression was confirmed.2 13 Venous blood was collected from the left antecubital vein at baseline, after 60 min of L-NMMA infusion (before exercise test), and 10 min after cessation of exercise.
Measurement of nitrite and nitrate in plasma
All measurements were performed under fasting conditions between 07:00 and 09:00. Plasma concentrations of nitrite were determined using a tri-iodide/ozone-based chemiluminescence assay, essentially as described.14 In brief, blood was drawn into a prechilled, heparinised tube, and centrifuged immediately for 10 min at 800 g and 4°C. Plasma was divided into two aliquots: one was directly injected into the reaction mixture consisting of 45 mM KI and 10 mM I2 in acetic acid at 60°C actively purged with a helium stream in-line with an NO chemiluminescence analyser (88 CLD 77am sp and 88 AM; Eco Physics, Duernten, Switzerland). The other one was treated with 0.1 vol 5% sulfanilamide in 1 M HCl to scavenge nitrite for 15 min and then injected. The difference in the two peaks sensitively reflects the concentration of nitrite in the plasma sample. Nitrate was quantified after enzymatic reduction to nitrite by nitrate reductase using flow-injection analysis based on the Griess reaction.15 16
Statistical analysis
Differences were assessed by repeated measurements analysis of variance, with p values for multiple comparisons adjusted by the Bonferroni criterion. Univariate correlations were Pearson correlations. A multivariate regression analysis was performed to determine independent predictors of maximal stress (in W) and duration of stress. Standardised coefficients were calculated as a measure of the relative predictive value. Statistical significance was assumed if a null hypothesis could be rejected at p = 0.05. All analyses were performed with SPSS 11.0.1 (SPSS Inc, Chicago, Illinois, USA).
RESULTS
Baseline and exercise characteristics of study subjects
Table 1 lists the baseline characteristics of the subjects; all were within the normal range. Exercise significantly increased diastolic blood pressure (81 (1) to 90 (2) mm Hg; p = 0.002), mean arterial blood pressure (95 (1) to 119 (2) mm Hg; p = 0.037) and heart rate (67 (1) to 143 (3) beats/min; p = 0.003). The maximal stress achieved was 181 (6) W with a duration of 9.6 (0.4) min (table 2).
Effect of exercise on nitrite concentrations
The subjects exhibited a mean exercise duration of 9.6 (0.4) min and achieved 181 (6) W. Ergometric exercise increased plasma nitrite concentrations from 97 (6) to 125 (8) nM (p<0.001) without affecting plasma nitrate (22 (1) μM to 23 (2) μM; NS). FMD, measured at rest (6.1 (0.3)%) as a non-invasive marker of endothelial function and NO bioactivity, correlated with the relative increase in plasma nitrite after exercise (r = 0.355; p = 0.01; fig 1). Cholesterol concentrations and age showed inverse univariate correlations with the maximal stress achieved and the duration of exercise (table 3). Post-exercise nitrite concentrations correlated univariately with stress (r = 0.365, p = 0.007; fig 2). In a multivariate regression model, both age and post-exercise nitrite concentrations were independent predictors of exercise duration and maximal stress achieved (table 4).

Effect of NOS inhibition on nitrite concentrations after exercise
To determine whether the observed increase in nitrite concentrations after exercise was NOS-dependent, we studied the effect of NOS inhibition on nitrite concentrations after the exercise test in a subgroup. Exercise increased plasma nitrite by 29 (10)%. This increase in nitrite concentration was abolished during NOS inhibition (−16 (11)%) (fig 3).

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The key findings of this study are that (a) exercise stress increases plasma nitrite concentration in healthy subjects, (b) the increase in nitrite is NOS-dependent, (c) the relative increase in nitrite correlates with endothelial function, and (d) post-exercise nitrite concentration and age are independent predictors of stress duration and power.
Origin of plasma nitrite
Circulating nitrite is derived from endogenous and exogenous sources. Endogenous nitrite is an oxidation product of endothelium-derived NO. The oxidation of NO by molecular oxygen is second-order in NO, and NO may also be enzymatically oxidised to nitrite via caeruloplasmin.17 It has been shown that up to 70–90% of circulating plasma nitrite is derived from eNOS activity in humans and other mammals.1 Recent data suggest that a significant proportion of circulating nitrite is also transported within erythrocytes.18 Besides endogenous formation, nitrite is ingested in food, particularly processed meat.19 Ingestion of large amounts of inorganic nitrate increases plasma nitrite. This increase is mainly due to enterosalivary circulation of nitrate (as much as 25% is actively taken up by the salivary glands) and reduction to nitrite by commensal bacteria.19 This nitrite enters the gastrointestinal tract when saliva is swallowed.
Emerging role of nitrite as an endocrine modulator
During the last few years, the emerging role of NO as a bioactive endocrine form has dramatically changed our understanding of nitrite.20–22 In vivo, nitrite can be reduced to NO under acidic conditions.23–26 However, this will only occur at a pH of less than 7, which is seen in tissues during ischaemia.27 Moreover, xanthine oxidase may reduce nitrite to NO.28 Nitrite reduction by xanthine oxidase is greatly enhanced at low oxygen tension and acidic conditions such as those seen during ischaemia. Furthermore, nitrite is recycled into bioactive NO by reduction with deoxyhaemoglobin.23 It has been suggested that this mechanism ensures autoregulated NO generation in regions of poor oxygenation where deoxyhaemoglobin predominates.20 Under physiological and pathophysiological conditions, nitrite seems to be crucial for hypoxic vasodilation, signal transduction and modulation of mitochondrial respiration. Experimental studies have shown that nitrite protects against ischaemia–reperfusion injuries,29 regulates gene expression,22 and modifies nitrosation reactions.30 These studies suggest that maintenance of circulating nitrite concentrations is crucial for the associated cardioprotective effects.
What is already known on this topic
Nitrite is the main oxidation product of NO in plasma and sensitively reflects changes in NOS activity under fasting conditions.
What this study adds
These results suggest a role for endothelium-derived plasma nitrite in the adaptation of haemodynamics during exercise and that an impaired increase in plasma nitrite concentration may limit exercise capacity.
Increase in plasma nitrite after exercise: relation to endothelial function
We have shown that basal concentrations of plasma nitrite are reduced with increasing numbers of cardiovascular risk factors.31 In the present study, we have shown in healthy subjects that an ergometric exercise test increases plasma nitrite concentrations. The relative increase in plasma nitrite correlated with the FMD of the brachial artery and therefore with endothelial function. Whether such a biochemical approach with measurement of nitrite after physical stress would be suitable for determining endothelial dysfunction in cardiovascular diseases needs be further elucidated.
The reason why there was only a small increase in nitrite in some subjects cannot be fully explained. NOS activity may have been impaired leading to reduced formation of NO and thus nitrite. However, it cannot be excluded that these subjects may also have had a higher rate of nitrite consumption through reduction to NO, which may be a compensatory mechanism for dysfunctional NOS production of NO. After all, it seems that an impaired nitrite increase is linked to endothelial dysfunction.
Plasma nitrite and exercise capacity
It has been shown for patients with congestive heart failure that increases in endothelium-dependent vasodilation significantly correlate with changes in functional capacity32 and a small increase in stroke volume. Improved NO-mediated vascular function may therefore improve cardiac function and Vo2max, possibly by improving vascular compliance and decreasing afterload. In our study population, the concentration of plasma nitrite after exercise—that is, the capacity of the vasculature to produce NO and thus nitrite—together with age independently predicts the maximal stress achieved and duration of exercise. Whether increases in plasma nitrite from a diet rich in nitrite and nitrate,33 application of organic nitrates or infusions of nitrite20 can influence exercise performance is not known. Further studies to determine whether NOS-derived formation of NO or reduction of nitrite to NO are involved are necessary to elucidate what is involved in the increase in blood flow as a result of exercise.
Study limitations
Exercise may alter a variety of determinants of microcirculatory flow that affect conversion of NO to nitrite. Preliminary studies measuring Po2, Pco2, lactate and arterial–venous gradients of nitrite, as well as eNOS expression, are needed to identify enzymatic and non-enzymatic mechanisms of nitrite increase. Moreover, studies on patients with cardiovascular disease must follow to elucidate the effect of, for example, medication, coronary artery disease and the respective cardiovascular risk factors on nitrite changes. Future studies using measurement of cardiac function and Vo2 are required in which the effects of exogenous nitrite on improvement in exercise capacity can be examined.
Acknowledgments
We thank Dominik Semmler for excellent technical assistance.
REFERENCES
Footnotes
Funding: TR and MK were supported by grants from the Deutsche Forschungsgemeinschaft (DFG RA 969/4-1 to TR and DFG Ke 405/5-1 to MK, and GRK 1089/project 3 to TR, CD, MK). TL received a grant from the Hans-und-Gertie Fischer Stiftung. CH is a scholar of the American Heart Association.
Competing interests: None.
- Abbreviations:
- eNOS
- endothelial NO synthase
- FMD
- flow-mediated dilation
- L-NMMA
- NG-monomethyl-l-arginine