Article Text

Abstract
Aims Cryptogenic organising pneumonia (COP) and acute fibrinous and organising pneumonia (AFOP) are recognised patterns of organising pneumonia (OP), a condition that resembles pneumonia but is not caused by infection. We have recognised granulomatous organising pneumonia (GOP) to be a similar histopathological entity where non-necrotising granulomata are intimately associated with the organising connective tissue. To what degree COP, AFOP and GOP represent distinct clinical and pathological disorders is unknown. This cross-sectional study sought to compare the pathological, clinical, and radiographical features of these OP patterns.
Methods Surgical lung biopsy specimens were reviewed for consecutive patients referred with OP to a metropolitan cancer centre. Clinical information and CT images were acquired from the hospital electronic medical record to determine the clinical and CT characteristics of each OP pattern.
Results Sixty-one patients (35 men, 26 women), mean age 61.5 years (range 8–85 years), were available for analysis. Of these, 43 patients (70%) had at least one prior cancer; 27 (44%) had received chemotherapy and 18 (30%) had received radiation. Approximately, half (32 patients) had respiratory symptoms, most commonly cough, dyspnoea and/or wheezing. While symptoms and mortality rates were not different among OP groups, AFOP patients more commonly had fever (p=0.04). GOP patients less commonly had received chemotherapy (p=0.03) and were more likely to present as masses/nodules (p=0.04).
Conclusions AFOP and GOP, a newly described OP form, possess clinical and pathological findings that set it apart from a COP, suggesting an emerging spectrum of OP.
- GRANULOMA
- LUNG
- INFLAMMATION
Statistics from Altmetric.com
Introduction
The term cryptogenic organising pneumonia (COP) continues to be used in the new American Thoracic Society (ATS)/European Respiratory Society (ERS) international multidisciplinary classification of idiopathic interstitial pneumonias because in many cases the aetiological factor cannot be determined. The histological pattern of OP is not specific and can be seen in association with multiple diseases known to injure the lung, such as collagen vascular disease, drug toxicity and infection.1 The pathological findings of COP include the characteristic fibromyxoid plugs within alveolar ducts and surrounding alveoli and mild-to-moderate interstitial chronic inflammation. The presence histologically of a granulomatous response, neutrophilic or eosinophilic infiltrate, hyaline membranes, necrosis and vasculitis should not be seen in COP.2 ,3 Treatment for COP typically rests with a prolonged course of systemic glucocorticoids with a clinical response in about 85% of patients.4–7
Several investigators have distinguished COP from similar idiopathic and organising pneumonias (OPs) that may be distinct in their pathological findings and steroid responsiveness. Youssem found that nearly 90% of patients with COP unresponsive to steroids also had histology showing a background of fibrosis.8 Yoshinouchi described two variants of COP.9 Patients with COP type II had Masson bodies containing fibrin and responded more poorly to steroids compared to those with COP type I who lacked fibrin. Beasley described 17 patients with acute fibrinous and organising pneumonia (AFOP), a form of acute lung injury in which intra-alveolar fibrin rather than granulation tissue in the form of fibromyxoid plugs, constituted the dominant histological finding.10 In that study, AFOP differed clinically and pathologically from COP in that mortality was higher, and organising fibrin balls were the dominant histological findings, involving from 25% to 90% of the air spaces with an average of 50%. AFOP differs from other forms of acute lung injury, such as diffuse alveolar damage (DAD), by the absence of classic hyaline membranes lining the alveolar spaces.
In addition to these patterns, we have observed that some cases of OP have non-necrotising, poorly formed granulomata intimately associated with the pneumonic process. Since the presence of granulomas would exclude the diagnosis of COP, we propose the term granulomatous organising pneumonia (GOP) to describe these cases that have pathological features of both granuloma and OP. To what degree AFOP and GOP represents simply histological patterns versus distinct entities with characteristic pathological, clinical and radiological features is uncertain.
To date, descriptions of patients with AFOP have concentrated on how the histopathology is distinct from other forms of acute lung injury; little is written about the clinical and radiographical features with direct comparison to a group of COP cases. The goal of this cross-sectional study is to compare and contrast the histological, clinical and radiographical features of COP, AFOP and GOP.
Methods
Permission to collect data was obtained by the Institutional Review Board (institutional approval #WA0536-11(1)). Cases diagnosed with COP, AFOP and GOP between January 1990 and June 2009 were retrieved from electronic medical record files at the Memorial Sloan-Kettering Cancer Center, a tertiary care cancer centre in New York City. COP is defined by patchy intraluminal fibroblastic plugs in distal air spaces such as alveolar ducts, alveoli and within the bronchioles, having no identifiable aetiology. AFOP is characterised by a pattern of OP where the predominant histological finding is the presence of intra-alveolar fibrin balls and type II pneumocyte hyperplasia, thus resembling an acute lung injury pattern, but lacking hyaline membrane formation. GOP is characterised by a pattern of OP in close association with small, poorly formed non-necrotising granuloma. The granulomatous reaction must be confined to the same peribronchiolar location and within the OP pattern. Cases were excluded from the category of GOP if: (1) granulomatous inflammation was the dominant finding, and with OP appearing to represent a secondary scattered reaction around the granulomata, (2) if there were areas of confluent granulomatous reaction or (3) if there were areas of granulomatous reaction away from foci of OP.
Cases were included based on surgical biopsy reports and if CT scans were available and had been performed within 30 days of biopsy. Cases were excluded if lung tissue was acquired from the same lobe as a confirmed malignant tumour or if tissue acquisition was limited to transbronchial biopsy and/or percutaneous needle aspiration, due to the small size of tissue acquired through these modalities. Cases were also excluded if a specific cause of OP (ie, collagen vascular disease) was known and/or another cause of granulomatous inflammation (ie, sarcoid, Crohn's disease or vasculitis) could not be ruled out by best clinical judgment.
Pathology review
All pathology was reviewed by two board-certified pathologists (ALM and WDT), blinded to other data. Pathological features were evaluated on paraffin-embedded H&E-stained sections. Grocott methenamine silver and Ziehl–Neelson stains were performed in all cases. Brown–Brenn and/or Brown–Hopps bacterial stains were evaluated in 45 cases. Immunohistology for viral antigens (cytomegalovirus (CMV), adenovirus and Herpes virus) was available for six patients. The cases were also evaluated for association with interstitial fibrosis on the following scale: 0=no fibrosis, 1=mild fibrosis characterised by mild thickening of the alveolar septae, 2=moderate fibrosis characterised by mild thickening of alveolar septae with mild distortion of the pulmonary alveolar structure and 3=severe fibrosis characterised by permanent fibrosis and distortion of the pulmonary parenchyma. The presence of alveolar fibrin deposition was interpreted as focal (less than 10% of the total OP area) or diffuse (more than 10% of the OP area). The amount of inflammatory infiltrate was scored as mild (inconspicuous lymphoplasmacytic infiltrate in the interstitium), moderate (conspicuous lymphoplasmacytic infiltrate involving the pulmonary interstitium and the peribronchial areas) or severe (dense lymphoplasmacytic infiltrate in the pulmonary interstitium, peribronchial and perivascular spaces). The presence of alveolar type II pneumocyte hyperplasia was recorded as focal, diffuse or prominent. The presence of conspicuous neutrophils or eosinophils was not seen in the inflammatory infiltrate in these study cases.
Clinical review
Electronic medical records were reviewed for demographic information, including age, sex and race; any prior malignancy and associated therapy; any known collagen vascular disease; medications taken at the time of biopsy; any known inorganic dust exposure, including coal, silica and asbestos; pets or bird exposure and any prior haematological transplantation. Patients were considered to have ‘active cancer’ if they received any cancer therapy within 1 month of lung biopsy or if they had histologically confirmed malignant cells within 1 year of biopsy. Smoking extent was quantified using pack-years (ie, the product of the average number of packs smoked daily and the total number of years smoked). Patients were considered ex-smokers if they had refrained from all smoking for at least 1 month prior to biopsy.
Radiology review
CT scans were reviewed by two board-certified thoracic radiologists (RTH and TAI), each blinded to the other's findings and other data. When the results were discordant, the investigators met as a group to reach consensus on the specific abnormality present. Radiographical features associated with each OP case were recorded, including location of the abnormality(s) (central, peripheral or diffuse), and the presence or absence of specific changes associated with OP as described in the medical literature, including any nodule/mass,11 consolidation,12 ,13 ground-glass component13 and air bronchograms.14 A pulmonary nodule or mass was defined as a radiographically distinct solid lesion surrounded on all sides by pulmonary parenchyma. Nodules and masses are themselves distinguished by size; nodules are less than 3 cm in greatest diameter and masses equal or exceed 3 cm. As the size of OP is sometimes difficult to quantify, and has not been definitively linked with prognosis, nodules and masses were grouped together for the purpose of this analysis. Also recorded was the presence or absence of radiographical findings not classically associated with OP, including hilar/mediastinal adenopathy, honeycombing, pleural effusion(s), cavitation, reverse halo sign, bronchiectasis and/or fibrosis.
Statistical analysis
This is a cross-sectional observational study. Clinical characteristics, including subject demographics, cancer history, smoking status, pulmonary function tests and radiographical findings were compared among subjects with COP, AFOP or GOP. Fisher's exact test was used to assess categorical variables, and the Kruskal–Wallis method was used to assess continuous variables. p Values were calculated for each comparison and were considered statistically significant if less than 0.05.
Results
Data, including all clinical and pathological information, was available for 61 patients. Of these, 36 had COP, 10 had AFOP and 15 had GOP. Lung biopsy resulted from the workup of respiratory symptoms in 32 patients. Of the 29 patients without symptoms, lung biopsy resulted from the workup of abnormal imaging acquired through routine follow-up of non-pulmonary malignancies (nine patients), lung cancer screening (nine patients), routine preoperative chest X-rays (nine patients) or through the evaluation of non-pulmonary symptoms, such as shoulder or rib pain (two patients). All patients presented with multifocal areas of abnormality in the lung parenchyma with peribronchial and interstitial distribution (figure 1).

Photomicrographs illustrating cryptogenic organising pneumonia (COP), acute and fibrinous organising pneumonia (AFOP) and granulomatous organising pneumonia (GOP) at 40× and 100× magnification. COP is associated with loose plugs of fibromyxoid tissue within small air spaces close to a bronchiolus (thin arrows). AFOP is associated with reactive pneumocytes and presence of fibroblastic plugs associated with the fibrin deposition (dashed arrows). GOP is associated with poorly formed granulomata in close association with organising pneumonia (OP; thick arrows).
Pathological abnormalities are summarised in table 1. In all cases of COP, the classical loose organising fibroblastic plugs that characterise the pattern of OP were seen forming patchy lesions within distal air spaces, including alveolar ducts and alveolar spaces; focal peribronchiolar plugs were also seen. Focal fibrin deposition within the air space was seen in eight (22%) of all COP patients, and represented less than 10% of the lesional area. While focal type II pneumocyte hyperplasia was seen in 18 (50%) of all COP patients, prominent type II pneumocyte hyperplasia was seen in only 1 (6%). Lymphoplasmacytic infiltrate was present among 29 (81%) of the COP patients, occurring predominantly in the pulmonary interstitium and in the peribronchiolar areas. Associated fibrosis were seen in18 (50%) of all the COP patients (13 with mild fibrosis and 5 with moderate fibrosis).
Pathological abnormalities among OP patients
AFOP cases showed more homogeneous histological features than other OP variants. All cases showed prominent fibrin deposition in alveolar spaces representing more than 50% of the lesional area. Fibrin deposition was seen more commonly than in other OP forms and was more diffuse (p<0.01). Type II pneumocyte hyperplasia was also seen in all cases, commonly with a diffuse distribution. These findings suggested a pattern of acute lung injury. Moreover, mild or moderate lymphoplasmacytic infiltrate was seen among 8 of the 10 AFOP cases, in a predominant interstitium distribution. Mild thickening of the alveolar septae (mild fibrosis) was observed in only two (20%) cases.
All cases of GOP, as defined in Materials and Methods, showed OP as the dominant feature, but there were additionally multiple non-necrotising, poorly formed granulomata within areas of OP. The granulomata were small and non-confluent. They were seen in the pulmonary interstitium in close association with the characteristic loose fibroblastic plugs of OP. A peribronchiolar distribution was not noted. Special stains for acid-fast bacilli and fungi were negative. There was focal deposition of fibrin in 6 (40%) of all GOP patients, but fibrin deposition represented less than 10% of the area of OP. Type II pneumocyte hyperplasia was seen in nearly half of all GOP patients, and most commonly had a diffuse distribution. A lymphoplasmacytic infiltrate was seen among 11 patients (73% of the GOP patients), predominantly in a diffuse distribution, involving the pulmonary interstitium and in the peribronchioloar regions; moderate lymphoplasmacytic infiltrate was seen more commonly in GOP than other OP forms (p=0.01). Mild fibrosis characterised by mild thickening of the alveolar septae were seen in 10 (67%) of all GOP biopsies.
No organisms were detected in any of the study cases by special stains for fungi and acid-fast bacilli, or by immunohistochemical stain for viral antigens (CMV, adenovirus or Herpes virus).
Demographic information is summarised in table 2. Most patients were male, Caucasian and had some smoking history. The percentage of patients who were smokers, former smokers or active smokers was not different among OP groups. Among all 61 patients, 43 (70%) had a total of 51 malignancies. Eight had more than one type of malignancy. The most common malignancy was non-small cell lung cancer (six patients), followed by colon cancer, Hodgkin's lymphoma, non-Hodgkin's lymphoma and sarcoma (five patients each). Although no particular cancer was clearly associated with OP or any OP type, any history of cancer was common, as expected at a cancer centre. A lower percentage of GOP patients had cancer than either COP or AFOP, a finding that was statistically significant (p=0.05). Only about one-quarter of all patients received cancer treatment at the time of lung biopsy. GOP patients were less likely to receive chemotherapy (p=0.03). Among GOP patients who had received radiation, the interval between radiation and lung biopsy was longer than it was among other OP patients. However, the small number of GOP patients receiving radiation precluded any meaningful associations. There was no difference among OP variants in exposure to inorganic dust. Microbiology studies were positive in three patients, all of whom had Mycobacterium avium, including one with COP and two with AFOP; however, in all cases, the organism was thought by the clinicians responsible to represent colonisation rather than active infection.
Patient demographics
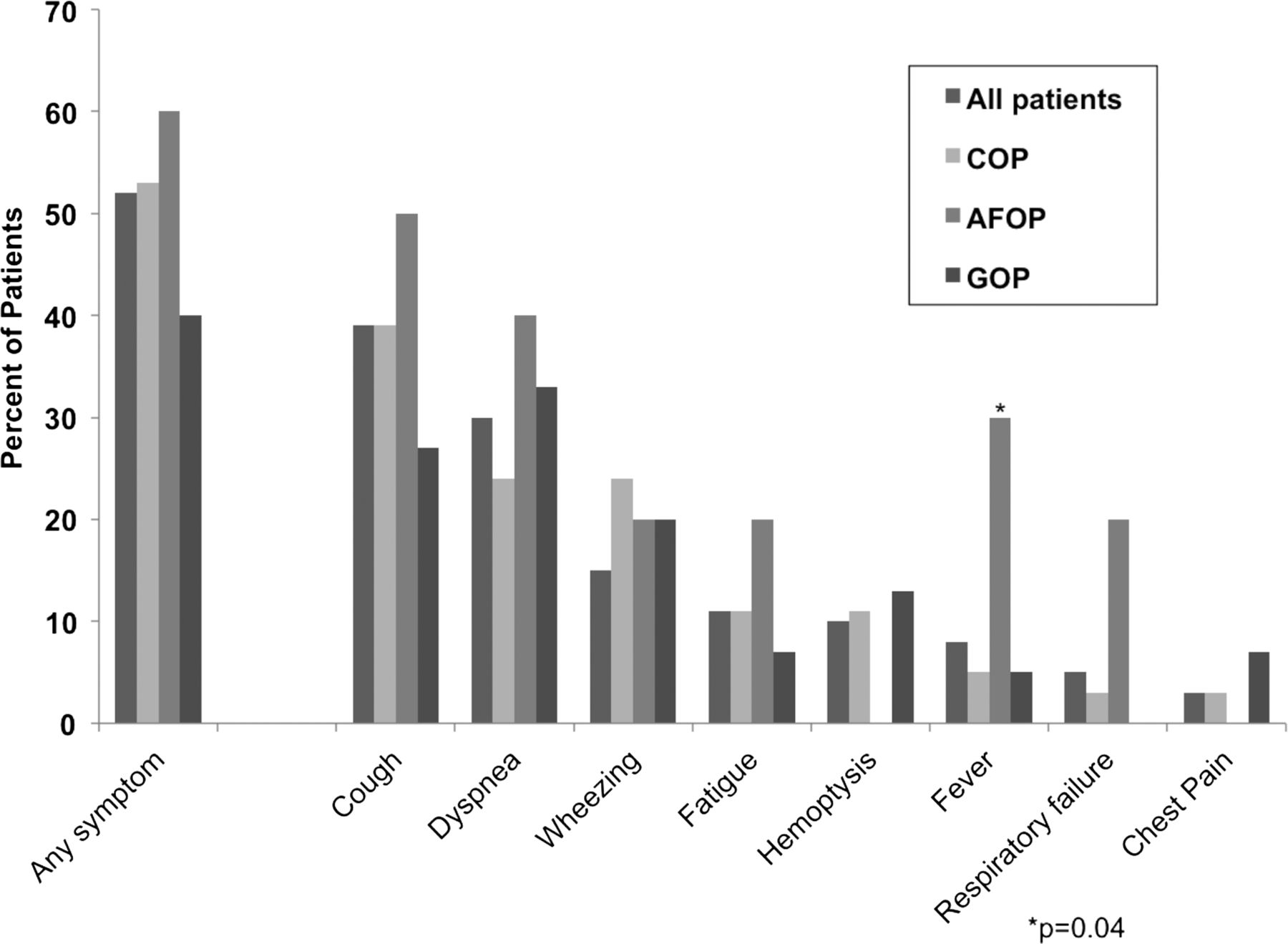
Approximately, half of all patients had respiratory symptoms at the time of biopsy (figure 2). The most common symptoms were cough and dyspnoea, followed by wheezing and fatigue. While there was no difference among COP, AFOP and GOP in overall symptom prevalence, a significantly higher percentage (30%) of AFOP patients suffered from fever compared to COP (5%) and GOP (6%; p=0.04). Two patients with AFOP and one patient with COP suffered respiratory failure requiring mechanical ventilation. Death occurred among 14 (23%) of all patients. Median time from biopsy to death was 205 days. Death was attributable to OP in only one patient with COP (2% of all patients, 3% of the COP patients), a 61-year-old woman with prominent interstitial fibrosis whose lung disease slowly worsened, despite receiving prednisone and macrolide antibiotics continuously for 29 months following lung biopsy. Among patients who did not die from OP, nine succumbed to their underlying malignancy, one died from infectious pneumonia, one from acute respiratory distress syndrome, and one from an intracranial haemorrhage. One patient died at home, and the specific cause of death was not determined.
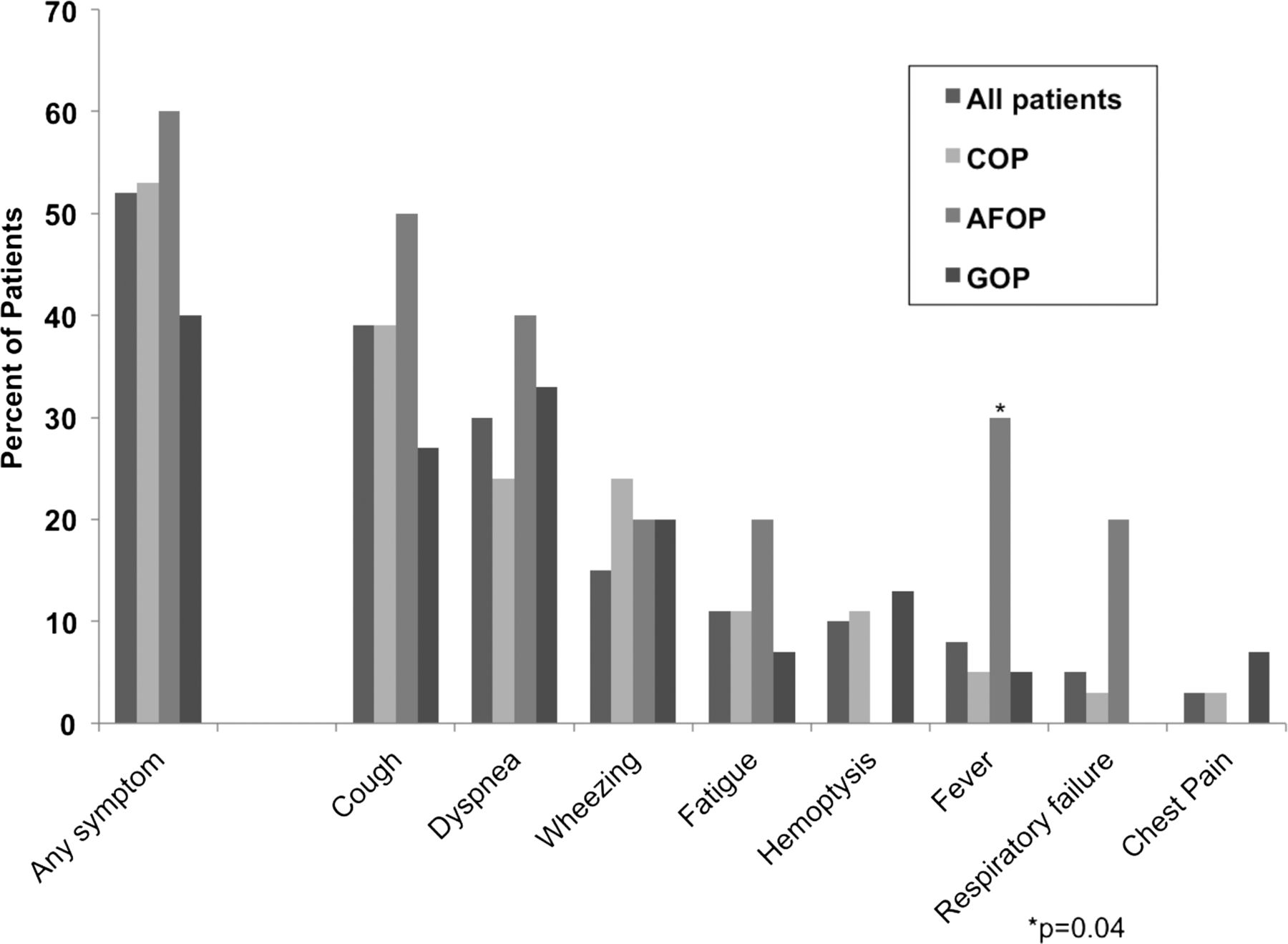
Symptoms experienced by patients with organising pneumonia (OP), expressed as the percentage of patients in each group.
Among all patients, 15 (25%) received one or more medications intended to treat OP. Seven patients received steroids alone, four received steroids with macrolide antibiotics and three received steroids in combination with both macrolide antibiotics and azathioprine. One patient received only macrolide antibiotics without steroids. GOP patients less commonly had any pulmonary symptom or required treatment, although this was not statistically significant. The overall percentage of patients receiving at least one treatment did not differ among the three OP types.
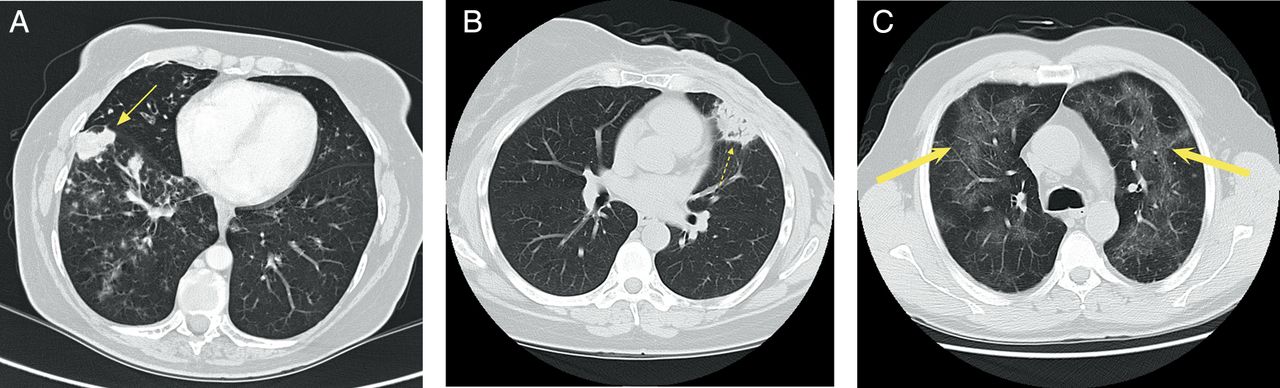
Radiological findings are summarised in table 3. Nodules/masses were the most common abnormality, present among 54 (89%) of all patients, and among all GOP patients. Nodules/masses were found significantly more commonly among GOP patients than those with COP and AFOP (p=0.04). Consolidation was present among 22 (36%) of all patients and air bronchograms were present among 16 patients (26%). While air bronchograms presented more commonly among AFOP patients, this difference was not statistically significant. Ground-glass opacities were present among 11 (18%) of all patients. Representative CT scans showing nodules/masses, consolidation and ground-glass infiltrates are shown in figure 3. Honeycombing, bronchiectasis, thoracic adenopathy and pleural effusions were uncommon, each occurring among less than 15% of patients. Cavitation was found among only two patients: one with COP and one with AFOP (3% of all OP patients).
Radiographical abnormalities among OP patients

{kind=link}
{kind=link}
{kind=link}
(A) Lung nodule/mass in a patient with cryptogenic organising pneumonia (COP). A never- smoker developed a cough after an upper respiratory infection which failed to clear with antibiotics. Chest CT scan demonstrated a spiculated mass 3.0 cm in diameter (thin arrow). She did not require treatment. (B) Consolidation in a patient with acute fibrinous and organising pneumonia (AFOP). A never-smoker developed consolidation in the anterior left lung on a routine surveillance CT scan, 3 years after undergoing surgery for renal cell carcinoma. Dyspnoea and cough improved with systemic steroids. Air bronchograms are also visible (dashed arrow). (C) Ground-glass infiltrates in a patient with GOP. A never-smoker developed an upper respiratory infection and fever 9 months after an autologous haematological transplantation for mantle cell lymphoma. He improved with systemic steroids (thick arrows).
Discussion
This review of 61 patients suggests a great deal of overlap among those presenting with COP, AFOP and GOP. The spectrum of demographic data, symptoms and radiographs are similar among these three groups. GOP is a new entity, which has not been described in any detail previously. GOP patients were more likely to have moderate lymphoplasmacytic infiltrate and uniformly present with nodules/masses on their radiographs; they were less likely to have had cancer and to have received chemotherapy. While the limited number of patients in this series complicates statistical conclusions, there was a trend towards GOP patients requiring medications less commonly than those with other OP forms. That the granulomatous process in GOP is intimately associated with the OP implies that they are part of the same process. Microorganisms were not found within the granulomatous inflammation in GOP patients, suggesting that the granulomata may be associated with an allergic or immunologic response. To what degree GOP represents a distinct variant of COP needs to be further evaluated in a larger case series. If the observation is confirmed that GOP patients have fewer symptoms, require less treatment, and are consequently less severely ill, the finding might provide insight into the role of the immune system in the pathogenesis of OP and offer avenues for further study.
In contrast to GOP, AFOP has been associated to date with a poorer outcome. AFOP has been thought to have pathological similarities to DAD and eosinophilic pneumonia (EP), and clinical outcomes similar to DAD. Although fibrin deposition is sometimes seen histologically in DAD, fibrin deposition in AFOP is more prominent; the original description of this disorder noted fibrin deposition involving 50% of air spaces on average.10 Moreover, fibrin is often organised into balls with AFOP and hyaline membranes are always absent. EP may be associated with prominent fibrin deposition, characteristic of AFOP and hyaline membranes and other features typical of DAD. However, unlike AFOP and DAD, EP is characterised by the predominance of eosinophils and, to a lesser extent, macrophages within the alveoli and interstitium.
Given the distinct pathology of AFOP, some have argued that it is a distinct clinical entity. We are aware of only one other series describing more than 10 individuals with this condition, and the pathology results described are similar to those presented here. However, in Beasley's series,10 fibrin deposition was noted among 25–90% of air spaces involved, with an average of 50%. We found greater than 50% involvement among AFOP patients. None of the COP or AFOP patients had more than 10%. This implies that a more precise definition of AFOP, requiring higher degrees of fibrin deposition, might be considered in the future. Beasley also noted death from pulmonary disease in 9 of the 17 patients with AFOP (53%). This far exceeds 5-year mortality rates reported among COP patients, which are generally thought less than 15%.15 While we found features that distinguish AFOP patients from other OP forms, we could otherwise not replicate Beasley's findings in that the rates of mortality and respiratory failure were overall very similar. One potential reason for better outcomes in this series is that many patients were asymptomatic at diagnosis, their AFOP resulting from the workup of incidental radiographical findings. In contrast, all patients reported by Beasley et al were symptomatic; at least five received mechanical ventilation and several had been diagnosed with DAD. We speculate that patients in Beasley's series had more advanced disease and/or may have been diagnosed later in the course of their illness.
Moreover, in the 2013 ATS/ERS updated the classification of idiopathic interstitial pneumonias, AFOP was recognised as a histological pattern rather than as a distinct form of idiopathic interstitial pneumonia because the published evidence at the time was regarded as insufficient to warrant recognition as a specific entity.1 In the analysis of the literature that existed at the time, it appeared that AFOP may be more of a histological pattern that can occur in lung biopsies from patients with a clinical radiological picture of either DAD or COP. So biopsies that only show an AFOP pattern from such patients may represent a sampling issue where the distinctive lesions of these entities were not biopsied. This could be another explanation for different perceived outcomes among populations with AFOP, and needs to be considered in future investigations.
It is also worth noting that some earlier reports of OP have found a lower proportion of patients presenting with nodules/masses than was seen here. Cordier for instance, reported nodules in only about one-third of OP patients.16 However, we are not the first to report that nodules/masses are prevalent among cancer patients. Mokhtari reported nodules/masses among over 70% of solid tumour patients developing OP.17 In contrast to some studies that distinguish nodules and masses based on size, we counted nodules and masses in the same group, which may have contributed to the apparent more frequent finding of this abnormality. The presence of GOP patients, who universally had nodules/masses in this series, may have increased the overall proportion of patients with nodules/masses.
Finally, the high prevalence of nodules/masses may reflect the circumstances around which medical imaging was sometimes pursued in this series. Among cancer patients, some OP cases were detected during routine medical surveillance, when they were otherwise asymptomatic. Nodules/masses that closely mimic cancer, detected among patients at the highest clinical risk for having malignant lung lesions, may be more likely to undergo surgical resection, resulting in some selection bias. This also suggests that caution is advisable to clinicians who care for cancer patients or who pursue CT imaging among asymptomatic high-risk patients, such as with lung cancer screening. Since the treatment and prognosis of OP and cancer is quite different, we feel the inclusion of OP in the differential diagnosis of nodules and masses is warranted in many circumstances. Likewise, our finding that fewer patients with OP required treatment might partly relate to our patient population. OP patients in other series may have been diagnosed with OP only after symptoms prompt clinicians to pursue imaging; therefore, it would not be surprising that a greater proportion requires treatment.
Strengths of this study include the number of patients studied with documented AFOP and GOP. We are aware of only one study where more AFOP patients were reported. There is no published literature to date on the clinical or radiographical manifestations of GOP patients, and therefore this is the first explorative study of its kind. It is worth noting that the number of patients studied remains small in absolute terms, which limits the vigour of any statistical analysis. Other potential limitations include that the targeted population studied is derived from a single urban cancer centre. OP patients examined, there may be different from those managed elsewhere since it is predominantly a cancer centre. The study is retrospective in design, rendering it susceptible to problems inherent to studies of this type, including confounding by indication. Likewise, the results described cannot imply causality. Cumulatively, these potential weaknesses limit the generalisability of these data to the general population.
In conclusion, based on these data, there is an emerging spectrum of OP that is distinct in histological manifestations. While we found some distinct differences in clinical findings, this series differs from prior work which suggested that some OP forms have a graver clinical course.
Take home messages
-
Several histological variants of OP have been proposed, but it is unclear how they differ clinically and radiographically.
-
GOP is a newly described variant of OP, characterised by a pattern of OP in close association with small poorly formed non-necrotising granulomata that must be confined to the same peribronchiolar location and within the OP pattern.
-
Patients present similarly among all forms of OP, but there were some important distinctions; AFOP patients were more likely to present with fever mimicking pneumonia, and GOP patients were more likely to present with nodules and masses mimicking malignancy.
-
As radiographical patterns in GOP often mimic malignancy, consideration of this OP variant may be warranted among patients under evaluation of lung nodules and/or masses.
References
Footnotes
-
All authors are jointly appointed to Weill Cornell Medical College, New York, NY, USA.
-
Correction notice This article has been corrected since it was published Online First. The provenance and peer review statement has been amended.
-
Handling editor Cheok Soon Lee
-
Contributors MBF: Data analysis and interpretation, manuscript writing and final approval of manuscript. SAD: Concept and design, data analysis and interpretation and final approval of manuscript. ALM: Pathological interpretation, manuscript writing and final approval of manuscript. DES: Concept and design and final approval of manuscript. RTH: Radiological interpretation and final approval of manuscript. TAI: Radiological interpretation and final approval of manuscript. YT: Statistical analysis, manuscript writing and final approval of manuscript. WDT: Pathological interpretation and final approval of manuscript.
-
Competing interests None.
-
Ethics approval Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Errata