Article Text

Abstract
Background Lung cancer is associated with poor health-related quality of life (HRQoL) and high symptom burden. This trial aimed to assess the efficacy of home-based rehabilitation versus usual care in inoperable lung cancer.
Methods A parallel-group, assessor-blinded, allocation-concealed, randomised controlled trial. Eligible participants were allocated (1:1) to usual care (UC) plus 8 weeks of aerobic and resistance exercise with behaviour change strategies and symptom support (intervention group (IG)) or UC alone. Assessments occurred at baseline, 9 weeks and 6 months. The primary outcome, change in between-group 6 min walk distance (6MWD), was analysed using intention-to-treat (ITT). Subsequent analyses involved modified ITT (mITT) and included participants with at least one follow-up outcome measure. Secondary outcomes included HRQoL and symptoms.
Results Ninety-two participants were recruited. Characteristics of participants (UC=47, IG=45): mean (SD) age 64 (12) years; men 55%; disease stage n (%) III=35 (38) and IV=48 (52); radical treatment 46%. There were no significant between-group differences for the 6MWD (n=92) at 9 weeks (p=0.308) or 6 months (p=0.979). The mITT analyses of 6MWD between-group differences were again non-significant (mean difference (95% CI): 9 weeks: −25.4 m (−64.0 to 13.3), p=0.198 and 6 months: 41.3 m (−26.7 to 109.4), p=0.232). Significant 6-month differences, favouring the IG, were found for HRQoL (Functional Assessment of Cancer Therapy–Lung: 13.0 (3.9 to 22.1), p=0.005) and symptom severity (MD Anderson Symptom Inventory–Lung Cancer: −2.2 (−3.6 to –0.9), p=0.001).
Conclusions Home-based rehabilitation did not improve functional exercise capacity but there were improvements in patient-reported exploratory secondary outcomes measures observed at 6 months.
Trial registration Australian New Zealand Clinical Trials Registry (ACTRN12614001268639).
- non-small cell lung cancer
- exercise
Statistics from Altmetric.com
Key messages
What is the key question?
Does home-based rehabilitation improve physical function (exercise capacity, physical activity and muscle strength) and patient-reported outcomes (including health-related quality of life (HRQoL) and symptom levels) compared with usual care during and following treatment for inoperable lung cancer?
What is the bottom line?
Home-based rehabilitation did not significantly change physical function, but significant improvements in HRQoL and symptom levels were reported by the intervention group at 6 months post-recruitment; adherence to the exercise programme was suboptimal.
Why read on?
There is limited high-quality evidence to support the use of rehabilitation in inoperable lung cancer, and this trial provides important evidence regarding the safety of home-based rehabilitation, patient-reported benefits and recommendations for the design of future rehabilitation trials.
Introduction
Worldwide, lung cancer is the second most frequently diagnosed cancer and the leading cause of cancer death, with an estimated 2 million new cases and 1.7 million deaths in 2015.1 Just over 80% of people are diagnosed after the disease has spread beyond the primary site.2 Five-year relative survival across all disease stages is 16% in Australia3 and 13% in Europe.4
Along with higher performance status, female sex, earlier disease stage and limited weight loss,2 higher functional exercise capacity at diagnosis is associated with improved survival. Each 50 m improvement in 6 min walk distance (6MWD) is associated with a 13% reduction in the risk of death.5 Observational studies demonstrate reduced functional exercise capacity, physical activity (PA) levels and muscle strength at diagnosis in people with lung cancer compared with healthy individuals, and these outcomes deteriorate further both during and following treatment.6 Inextricably linked with the decline in functional exercise capacity and muscle strength are the high symptom severity and distress experienced by people with lung cancer. Symptom burden, most notably cancer-related fatigue, cough and dyspnoea, is higher than reported in other cancers7 and has shown little change over a decade.8 Decline in physical function and PA as well as poorly controlled symptoms contribute to reduced health-related quality of life (HRQoL).6 9
Previous studies have demonstrated the safety of exercise interventions in advanced lung cancer, in both hospital and home settings.10–13 Exercise sessions frequently comprise aerobic and resistance training prescribed at moderate intensity. Studies of exercise interventions in advanced lung cancer have been subject to bias given they are often uncontrolled, pilot in nature or lack assessor blinding. Due to the progressive nature of the disease and its poor prognosis, study attrition rates are commonly high.13 14 Given the limited number of robustly designed studies in this area, further studies are needed to add to the evidence base regarding the effectiveness of exercise in this population of patients with unique needs.15
We undertook a randomised controlled trial (RCT) of home-based rehabilitation in inoperable lung cancer at the commencement of active treatment. The aims were to assess the efficacy of a rehabilitation package, compared with usual care (UC), on change in physical function (functional exercise capacity (primary aim), PA and muscle strength) and patient-reported outcomes including HRQoL.
Methods
Study participants
Participants were recruited by the trial co-ordinator and a research assistant who screened lung cancer clinic lists and attended multidisciplinary team meetings at three tertiary-care hospitals in Melbourne, Australia. Trial eligibility criteria are detailed in box 1. All participants provided written informed consent prior to baseline testing.
Trial eligibility criteria
Inclusion
Inoperable NSCLC diagnosis.
Non-surgical treatment planned for the primary lung tumour (eg, chemotherapy, radiotherapy or targeted therapy).
Commenced treatment ≤4 weeks prior to recruitment.
Aged ≥18 years.
Able to read and write English.
ECOG-PS of ≤2.
Clinical Frailty Scale score of <7.
Physician-rated life expectancy of >6 months.
Trial involvement approved by treating oncologist.
In cases of newly diagnosed recurrent disease, must have completed previous treatment >6 months prior to recruitment.
Exclusion
Concurrent, actively treated other malignancy (or 1-year history of other malignancy) other than in situ melanoma or non-melanoma skin cancer.
PA self-report indicates patient has met guidelines for the past month (150 min or more of moderate-intensity PA per week).
Current unstable psychiatric or cognitive disorder.
Participation in a land-based exercise programme prohibited by comorbidities or pelvic or lower limb bony metastases.
ECOG-PS, Eastern Co-operative Oncology Group Performance Status; NSCLC, non-small cell lung cancer; PA, physical activity.
Study design
This multisite, assessor-blinded, parallel-group RCT was powered for superiority. Conduct and reporting followed CONSORT and the Template for Intervention Description and Replication (TIDieR) guidelines.16 17 A trial protocol was published.18
Randomisation and blinding
After enrolment into the trial and following baseline assessment, participants were randomised (1:1) to receive either UC or usual care plus intervention (IG). The randomisation schedule was computer generated, using a block permuted design (randomly arranged blocks of six or eight) with stratification for treatment intent (‘radical’ vs ‘palliative’), and site of recruitment and allocation was concealed. Following baseline testing, a staff member with no trial involvement assigned patients to the trial groups. Outcome assessors and the trial statistician were blinded to group allocation. Due to the nature of the trial intervention, it was not possible to blind participants or intervention clinicians.
Procedures
All participants received usual care provided by their treating hospital, which did not involve any routine exercise advice or physiotherapy/exercise physiology consultation at the time of the trial. In addition, UC participants received monthly attention phone calls from a research team member. During these calls, participants were asked about their general well-being but were not provided with exercise or symptom management advice. IG participants received a home-based rehabilitation programme which was person centred and involved tailored exercise prescription, behaviour change strategies and early treatment initiation to manage symptoms. The 8-week programme commenced with a home visit and was followed by two telephone calls per week (one to review exercise programmes and the other for symptom management support). A further two home visits could be performed in place of exercise calls where participants were not meeting exercise goals. Between 9 weeks and trial completion, participants received monthly contact to review and progress exercise programmes. Walking was commonly chosen by participants as their preferred form of aerobic exercise and they were encouraged to begin with a minimum of 10 min walking twice weekly at a moderate intensity (aiming for a rating of 4, ‘somewhat hard’, on the modified Borg Dyspnoea Scale).19 Resistance training involved predominantly lower limb functional exercises using body weight as resistance, including sit to stand, squats, step-ups, heel raises and a wall press. American College of Sports Medicine guidelines were followed in prescription of resistance training, with training commenced at 80% of the 10-repetition maximum, performed in 8–10 repetitions, two to three sets, moderate intensity,19 two to three sessions per week.20 Each exercise session was scripted to standardise the content (including identification of past exercise behaviours, exercise preferences, goals and potential barriers) and delivered by four physiotherapists, with an average of 18 years’ general clinical experience. Symptom management telephone sessions used the Edmonton Symptom Assessment Scale21 at the start of each session to identify participant symptoms rated as ‘worst’. Sessions were scripted to ensure content included symptom impact on activity and current management strategies. Additional non-pharmacological management strategies were discussed and participants were encouraged to refer to the trial symptom management booklet during calls. The nurse who delivered the majority of symptom management sessions had 10 years’ clinical experience, six in oncology (refer to figure 1 and the online supplementary material for further details).
Supplemental material
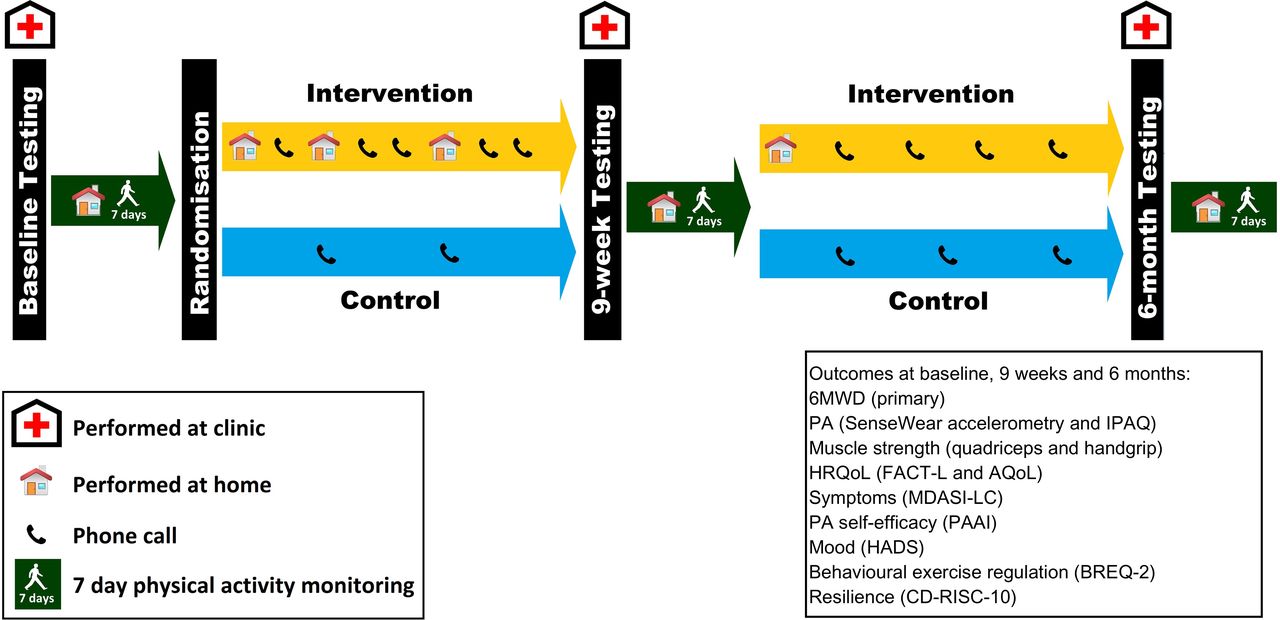
Trial design. Outcome measure testing occurred at three time points and was followed by a 7-day period of objective physical activity monitoring. Following randomisation, the intervention group (IG) received 8 weeks of weekly physiotherapy and nursing contact. On completion of 9-week testing, a physiotherapy home visit was performed with the IG and regular physiotherapy support to maintain exercise behaviours was provided by phone until trial completion at 6 months. 6MWT, 6 min walk test; AQoL, Assessment of Quality of Life; BREQ-2, Behavioural Regulation of Exercise Questionnaire, version 2; CD-RISC-10, Connor-Davidson Resilience Scale 10-item version; FACT-L, Functional Assessment of Cancer Therapy–Lung; HADS, Hospital Anxiety and Depression Scale; HRQoL, health-related quality of life; IPAQ, International Physical Activity Questionnaire; MDASI-LC, MD Anderson Symptom Inventory–Lung Cancer; PA, physical activity; PAAI, Physical Activity Assessment Inventory.
Outcomes
Participants completed outcome assessments at baseline, 9 weeks and 6 months post-recruitment. Demographic and clinical variables were collected at baseline. The primary outcome was the change in functional exercise capacity (6MWD) from baseline to 9 weeks, measured with the 6 min walk test (6MWT) at each site. The 6MWT was performed using a standardised protocol according to American Thoracic Society guidelines.22 Increased distance walked indicates improved functional exercise capacity; the minimal clinically important difference (MCID) is 22–42 m in lung cancer.23 Secondary outcomes included PA (accelerometry and self-report), HRQoL, symptom severity and distress, anxiety and depression, PA self-efficacy, motivation to exercise and resilience. A priori, intervention adherence was defined as completion of at least twice-weekly aerobic exercise for at least six of the initial eight trial weeks.18 Adherence data were obtained from self-report (exercise diary and data collected during weekly contact). Figure 1 and the online supplementary information provide further details. Exploratory survival analyses were censored during data analyses (2 February 2018). Where participants were unable to return to their treating hospital, assessments were conducted in the participants’ homes. Outcomes were assessed by 11 blinded research assistants: physiotherapists (n=8), exercise physiologists (n=2) and one nurse. Complete health economic analyses and exploratory subgroup analyses of inflammatory markers and muscle mass will be reported separately.
Statistical analysis
Based on pilot data, the calculated sample size was 92 participants to detect a mean difference in the primary outcome, 6MWD change from baseline to 9 weeks, of 48 m with a SD of 68 m.6 This provided 80% power at a two-tailed level of significance of 5%, with an attrition rate of 30%.
A statistical analysis plan was developed by the trial statistician prior to database unlocking (online supplementary information). Data were analysed using SPSS V.24, R V.3.5.0 and Minitab V.18. An intention-to-treat (ITT) analysis for the 6MWD was performed for all 92 participants using a composite score, with participants in their original assigned groups. This composite score comprised (1) observed 6MWD values for participants who completed the test, (2) an assigned value of 100 m for those who died prior to follow-up (100 m being less than the minimum observed value of participants who completed the test) and (3) an imputed value for living participants with missing data. The Mann-Whitney U test was used to analyse the 6MWD difference between groups at 9 weeks (the primary outcome) and 6 months. All subsequent analyses, except survival, used modified ITT (mITT) principles; only participants who provided data for at least one follow-up outcome measure were included in further data analyses using multiple imputation.24 Participants who did not provide data beyond baseline were excluded from mITT analyses. Where participants had partial follow-up data, multiple imputation was undertaken to control for the possible bias associated with missing data. This included data imputation for participants who did not provide 6-month data but had provided at least partial 9-week data and were not known to be deceased. Participant death was the most common reason for lack of follow-up data. It is widely accepted, and accords with common sense, that the imputation of missing data on a patient-reported outcome (eg, quality of life) for a deceased participant is inappropriate.25 mITT analyses excluded participants who had died prior to each follow-up.
The changes in primary and secondary outcomes, from baseline to 9 weeks and baseline to 6 months, were compared between groups using standard t-tests in the mITT analyses. Covariates included in these analyses included prior outcome measure scores and baseline characteristics (online supplementary file). To assess for the interaction effects between group and time, linear models with trial group, time (9 weeks or 6 months) and baseline outcome as explanatory variables were used for each outcome. All tests of significance performed are described in the Results section and no adjustment was made for the number of outcomes assessed.26 Survival analysis included all participants with comparisons between the two trial groups using Kaplan-Meier curves and the log-rank test. The estimate of the HR for survival, with 95% CI and p value, was obtained from Cox’s proportional-hazards model. Details of per-protocol and subgroup analyses are provided in online supplementary material.
Supplemental material
Results
Between 5 December 2014 and 19 December 2016, 824 patients were screened and 180 met eligibility criteria. Figure 2 and online supplementary figure S1 outline the flow of participants through the trial. Age was the only characteristic that was significantly different between eligible participants who declined (n=88), versus those who consented (n=92) to trial involvement, with those who declined being older (mean difference (95% CI) 6.4 (2.9 to 9.9) years, p=0.0004). Ninety-two participants were randomised (45 IG, 47 UC) and follow-up assessments were completed by July 2017. Table 1 provides participant characteristics. The mean age of participants was 63.5 years with 52% having stage IV disease and 46% receiving radical intent treatment. Baseline outcomes are presented in table 2. Multiple imputation data were available for the primary outcome (6MWD change from baseline to 9 weeks) in 84% (38/45) and 85% (40/47) of the baseline IG and UC samples, respectively (online supplementary material). Missing data at follow-up were primarily due to death (online supplementary file and online supplementary table S1). Fourteen participants did not provide data beyond baseline due to death (n=8) and withdrawal from the trial (n=6). Online supplementary table S2 presents characteristics and baseline measures of participants with (n=78) and without (n=14) follow-up data. The 78 participants (40 UC, 38 IG) with follow-up data were included in 9-week mITT analyses. There was no difference between groups in response to treatment on imaging (χ2=3.6, p=0.61) or need for chemotherapy dose reduction (χ2=0.00, p=1.00). In total, nine participants withdrew from the trial prior to completion (4 IG, 5 UC). Those who withdrew were older (mean (SD) 71.2 (9.0) years vs 62.7 (12.2) years, p=0.04) and had higher scores on the Colinet Co-morbidity Scale (median (IQR) 9.0 (9.0–9.0) vs 8.0 (7.0–9.0), p=0.006) than those who did not withdraw.

Trial profile. Participants declined the 6 min walk test (primary outcome) at three 9-week assessments (n=2 usual care, n=1 intervention group) and six 6-month assessments (n=1 usual care and n=5 intervention group). Analyses are based on multiple imputation datasets.
Baseline characteristics of participants
Baseline outcomes of participants
Four participants (8.9%) received no intervention due to death (n=2) or withdrawal (n=2), and one received one physiotherapy home visit and two symptom management calls prior to disease progression, hospitalisation and death. Exercise adherence was 65% (26/40) and 53% (21/40) for aerobic and resistance exercise. Online supplementary table S3 provides details of the intervention delivered.
The ITT analyses involving all 92 participants for the 6MWD revealed no significant between-group differences at 9 weeks (the primary outcome, p=0.308) or 6 months (p=0.979). There were also no significant between-group differences in 6MWD change at either follow-up, in mITT analyses. Table 3 and figure 3 outline differences for the primary and secondary outcomes.
Between-group change scores from baseline for primary and secondary outcomes, modified intention-to-treat and per-protocol analyses

Within-group mean change (95% CI) from baseline to 9 weeks and baseline to 6 months: (A) 6 min walk distance, (B) symptom levels, (C) symptom distress and (D–F) health-related quality of life scores (FACT-L scale, Lung Cancer Subscale (LCS) and Trial Outcome Index (TOI)). Data represent the mean (95% CI) within-group change at 9 weeks (9-week minus baseline scores) and at 6 months (6-month minus baseline scores) within the usual care (blue) and intervention groups (orange), with the p value noted for significant between-group differences. For 6 min walk distance and FACT-L, increased scores indicate improvement. For MDASI-LC, decreased scores indicate improvement (reduced symptom severity and distress). FACT-L, Functional Assessment of Cancer Therapy–Lung; MDASI-LC, MD Anderson Symptom Inventory–Lung Cancer.
At 9 weeks and 6 months, the respective between-group mean differences (95% CI) were −25.4 m (−64.0 to 13.3), p=0.198 and 41.3 m (−26.7 to 109.4), p=0.232. Nine-week assessments occurred a median (IQR) of 42 (20.5–48.8) (UC) and 37 (27.0–44.5) (IG) days after completion of radical intent treatment. Follow-up 9-week and 6-month 6MWT assessment occurred in the hospital environment on 75% (56/75) and 80% (48/60) of occasions. Unblinding of assessors, due to participants discussing the intervention, occurred during 17% (13/78) and 6% (4/66) of 9-week and 6-month assessments. Within-group differences are reported in online supplementary table S4.
The secondary outcomes of PA and muscle strength showed no statistically significant between-group differences at 9 weeks or 6 months (table 3). The change in HRQoL (FACT-L) was not significantly different between groups at 9 weeks; however, at 6 months, it showed significant differences favouring the IG (FACT-L total score mean difference (95% CI) 13.0 (3.9 to 22.1), p=0.005, FACT-L Lung Cancer Subscale (LCS) 4.7 (1.6 to 7.7), p=0.003 and FACT-L Trial Outcome Index (TOI) 10.4 (4.0 to 16.9), p=0.002). At 6 months, significant differences favouring the IG were also seen for symptom severity, MDASI-LC (−2.2 (−3.6 to –0.9), p=0.001) and the amotivation (−0.6 (−1.2 to 0.0), p=0.041) and identified regulation (0.8 (0.2 to 1.4), p=0.012) Behavioural Regulation of Exercise Questionnaire, version 2 subscales (items relating to the intention to engage in exercise and the recognition of exercise importance to achieve outcomes). There were no other significant between-group differences for secondary outcomes (table 3). Tests for the interaction between group allocation and time across the three time points (online supplementary table S5), using repeated measures analyses, were significant only for the 6MWD (difference between mean treatment effect (IG minus UC) at 6 months relative to 9 weeks (95% CI) 66.9 m (15.1 to 118.7), p=0.012), where across time the temporal patterns of 6MWD results were different between the two groups (online supplementary figure S2).
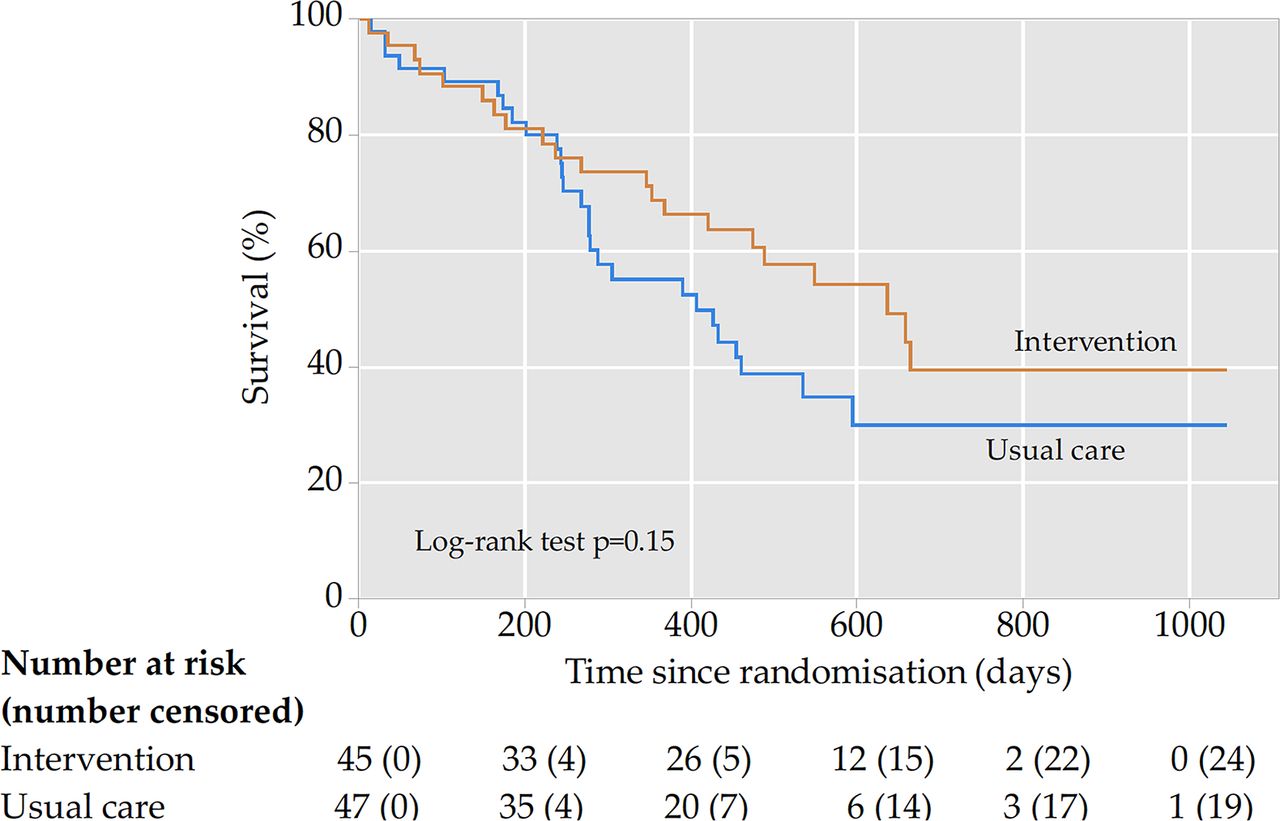
No trial-related serious adverse events occurred. The average survival follow-up was 1.1 years (IG) and 1.0 year (UC), during which time 48 deaths occurred (21 IG vs 27 UC). Median (95% CI) survival (days) from randomisation to time of censoring for data analyses was 636 (420.0 to 852.0) (IG) versus 406 (224.4 to 587.6) (UC), p=0.15 (figure 4). The 25th percentiles for overall survival were estimated to be 267 days (IG) and 245 days (UC) (75th percentile was not yet reached). Per-protocol and subgroup analyses results are provided in online supplementary material.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve for intervention and usual care groups, intention-to-treat analysis.
Discussion
This trial of home-based rehabilitation for people with inoperable non-small cell lung cancer (NSCLC) receiving active treatment demonstrated no statistically significant benefits in follow-up objective measures of physical function. At 6 months, statistically significant benefits favouring the IG were found for the patient-reported secondary outcomes of HRQoL (FACT-L), symptom severity and exercise motivation. As with previous studies in the area,27–32 there was significant heterogeneity with regards to participant treatment regimens and intent (curative or palliative), which we stratified for to promote balance between groups.
Our methods and results differ from those of Dhillon et al,33 who published the first adequately powered RCT of a PA intervention incorporating behaviour change techniques in advanced lung cancer. They reported no significant between-group differences in any measure (primary outcome fatigue). Ninety-five per cent of their sample had stage IV disease and participants were randomised 8.2 months post-diagnosis, resulting in significant attrition (55% (62/112) completed 6-month assessments).33 It is not possible to separate out the effects of each of our intervention individual elements; however, the earlier recruitment, symptom self-management support, home setting and phone coaching provided to encourage exercise behaviours until trial completion are key differences in the design of the two studies, which could account for the differences in findings. Given no significant between-group changes in physical function occurred, it is possible that improved symptom control and safe performance of exercise in the home environment allowed IG participants in our study to maintain family and social roles. This may have contributed to the significant improvements in IG participants’ HRQoL, when coupled with the reduced social isolation associated with increased contact from trial personnel and involvement of family and friends in the rehabilitation programme.
Although emerging evidence reports equivalence of home-based and centre-based pulmonary rehabilitation outcomes in COPD,34 in cancer, unsupervised home-based training does not appear to confer the same physical or HRQoL benefits observed following supervised programmes.35 We did not supervise the intensity at which IG participants performed exercise training. Despite verbal, video and written education during initial sessions and reinforcement of target intensities in follow-up telephone contact, it is likely that many participants were exercising at lower intensities than prescribed, which may have contributed to the lack of change in physical function. We employed several strategies to promote exercise adherence, but this remained suboptimal, with only half (53%) of the participants adherent to their prescribed resistance training. Our findings at 9 weeks may have been influenced by a significant effect of the toxicities of radical chemoradiation, which tend to peak towards the end of the course of 6 weeks of treatment and in the 2 weeks afterwards, preventing participants from exercising. In the future, therefore, we recommend measurement of trial outcomes at a later time point such as 12 weeks.
Given the greater decline in 6MWD observed in the IG compared with the UC group between baseline and 9 weeks (figure 3, table 3, online supplementary figure S2), which represented a clinically significant difference,23 we hypothesise a modified form of the participant’s preferred exercise may be more feasible for some participants during this period. Those who are unable to participate in specific structured exercise during initial treatment should receive PA education and counselling to stay as active as possible from diagnosis and during treatment. For these participants, it may be more feasible to commence structured exercise on completion of initial treatment. Proactive symptom monitoring should be embedded in care pathways for all patients.
For IG participants, routine assessment of symptoms using the Edmonton Symptom Assessment Scale as well as discussion and education regarding symptom management may have resulted in earlier initiation of symptom-management strategies, prompting increased discussion of symptoms with treating oncologists and other health professionals, thus improving symptom control. Enhanced symptom self-reporting has been shown to improve HRQoL, to extend tolerance to chemotherapy treatment, to reduce emergency department use and to improve overall survival in advanced cancer.36
Our person-centred intervention involving tailored assessment, early treatment initiation and ongoing support from experienced clinicians led to improvements in outcomes of importance to patients: HRQoL and symptom severity. The FACT-L TOI, which showed significant improvements in the IG at trial completion, incorporates the key elements targeted by the intervention, symptoms and physical and functional well-being and is recommended for future studies. Although HRQoL was a secondary outcome and the trial was not specifically powered for this outcome, the observed changes in this trial were of clinical relevance. Lower 95% CI limits for HRQoL approached the MCID and were similar to clinically meaningful differences reported with medical therapies for advanced NSCLC: two to three points and five to seven points for the FACT-L LCS and FACT-L TOI, respectively.37
There are several limitations of this trial. The 6MWD MCID in lung cancer (42 m) was not established at the time the trial commenced; therefore, we used a mean difference of 48 m (pilot data) for the sample size calculation. Also, these data showed higher variability than what had been accounted for. It is possible, therefore, that the trial was underpowered to detect significant 6MWD differences. A ceiling effect may have been present for the 6MWD as functional exercise capacity was relatively well preserved at baseline. Use of the incremental shuttle walk test should be considered in future studies to minimise ceiling effects.22 Our findings of improved patient-reported outcomes at 6 months may be a result of the increased healthcare team contact the IG received compared with UC, rather than the intervention. We did not prevent participants allocated to the UC group from exercising. Increased awareness regarding the benefits of PA, including media promotion, occurred during the 2.5 years of the trial and may have led to increased treating team education on an ad hoc basis, potentially diluting the effects of the trial. Also, reliance on patient self-report during follow-up telephone contact made assessment of IG exercise adherence and intensity difficult.
Conclusion
This trial of home-based rehabilitation resulted in significant improvements in patient-reported secondary outcomes at 6 months without significant changes in objective measures of physical function. We recommend future rehabilitation studies use outcomes which can be measured outside of the hospital setting at follow-up. Treatment designs should be flexible and include options to perform exercise in hospital, home, community or gym settings according to patient preferences. Predominantly home-based programmes should include occasional supervised hospital-based sessions or use effective, evolving COPD telerehabilitation technologies to ensure programme fidelity. Telerehabilitation technologies include ‘virtual’ rehabilitation groups using video conferencing and wearable technologies to enable remote monitoring of exercise sessions and the use of interactive web-based programmes to educate and support patients to be physically active and manage symptoms.38 Future studies should also be adequately powered to assess for possible impacts on survival times given the trend for increased IG survival seen in this trial. At 236 days, the median improvement in survival is likely to be clinically important in this population with inoperable disease. Further investigation of rehabilitation effects in NSCLC populations managed with immunotherapy or targeted therapy may also be warranted, given the demonstrated efficacy and increased use of these therapies.
Acknowledgments
The authors would like to thank the participants involved in this trial, along with Ms Polly Dufton, Ms Megan Howard, Dr Andrew Hancock, Ms Tina Griffiths, Ms Lucy Bucci, Ms Jennifer Jones, Dr Selina Parry, Dr Brooke Winzer, Ms Louise Lowe, the medical and radiation oncology teams and nurse co-ordinators at each site for the assistance they provided in completing this research.
References
Footnotes
Presented at This study was presentated at the European Respiratory Society Congress, 2018.
Contributors LD, SA, CLG, CFM, MK, LM and LI conceived the study and devised the design. IG devised the statistical analysis plan. LE co-ordinated the trial and was responsible for data acquisition. IG and LE undertook the data analyses and interpretation. LE drafted the manuscript. All authors critically reviewed the manuscript and approved the final version prior to submission. LE managed the manuscript submission.
Funding This trial was funded through a National Health and Medical Research project grant (APP1060484). LE is the recipient of a Victorian Government Olivia Newton John Cancer Wellness and Research Centre Supportive Care PhD scholarship, through the Victorian Cancer Agency.
Disclaimer The funders of the trial had no role in trial design, data collection, data analysis, data interpretation or writing of the report.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The Peter MacCallum Cancer Centre Human Research Ethics Committee (HREC/14/PMCC/27).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.