Article Text

Statistics from Altmetric.com
A 51 year old man presented with a 1 year history of fatigue and night sweats, cough with clear sputum, central chest discomfort, and mild exertional dyspnoea. A detailed exposure history was negative. Laboratory investigations including tuberculin skin test, white cell count, ESR, C-reactive protein, urea, creatinine and electrolytes, protein electrophoresis, rheumatoid factor, antinuclear antibody, calcium, alkaline phosphatase and liver function tests were all normal. Urinalysis and 24 hour urine calcium excretion were normal. Echocardiography was normal. Detailed pulmonary function tests and arterial blood gases were normal except for an isolated reduction in the transfer factor (73% predicted).
The chest radiograph showed a reticulonodular pattern involving mainly the lower lobes. A high resolution chest CT scan showed a fine nodular pattern with foci of calcification (figs 1A and B). Transbronchial biopsy specimens were non-diagnostic. Thoracoscopic open lung biopsy was performed. Light microscopic examination revealed multiple foci of bone in a branching pattern randomly located within the alveolar airspaces. Bone marrow was identified within some fragments (fig 2). There was associated mild subpleural and focal small nodular interstitial scarring but no honeycombing or other features to suggest pulmonary fibrosis. There was no evidence of venous congestion or iron deposition. Congo red stains were negative and electron microscopy revealed no evidence of amyloid. There was no evidence of granulomas or malignancy.

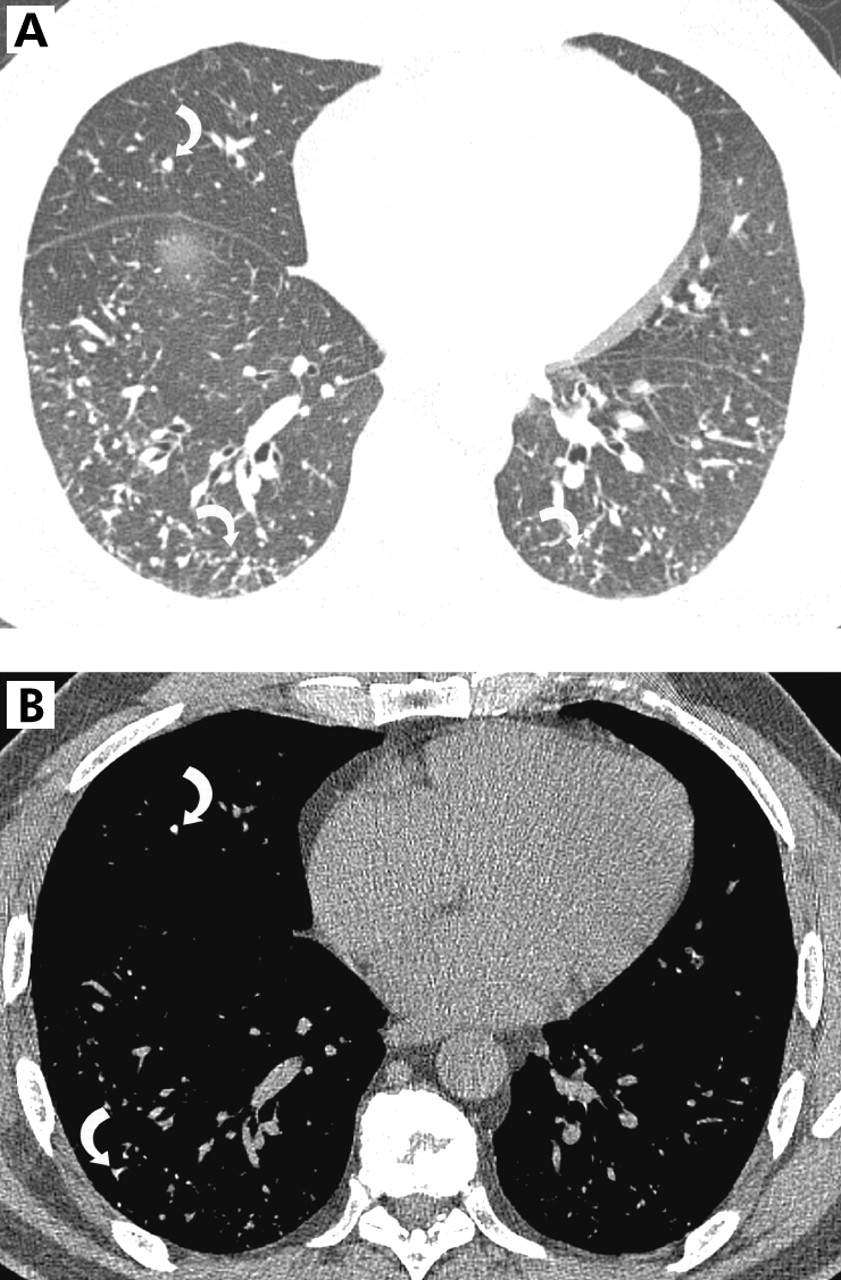
(A) High resolution CT scan showing small nodules and a few linear opacities (arrows). (B) Soft tissue window showing foci of calcification in some of the nodules and linear opacities (arrows).

{kind=link}
{kind=link}
Low power photomicrograph showing a branching fragment of bone containing marrow protruding into the alveolar airspaces. Note the outline of fat globules indicating marrow elements. On higher magnification images (not shown), haemopoietic elements including neutrophils and a megakaryocyte were identified (magnification ×100).
Learning points
-
Diffuse pulmonary ossification usually occurs in the context of a pre-existing pulmonary, cardiac or metabolic disorder. Idiopathic diffuse pulmonary ossification is a very rare disorder that usually occurs in men aged 40–60 years. Patients are usually asymptomatic but mild symptoms, restrictive pulmonary physiology, and impaired transfer factor have been described.
-
The presence of pulmonary calcification is often not apparent on the radiograph but can usually be seen on high resolution CT scanning.