Article Text

Abstract
Background We assessed the relationship of body mass index (BMI), smoking, drinking and solid fuel use (r; SFU), and the individual and combined effects of these factors on wheezing symptoms (WS) and on diagnosed asthma (DA).
Methods We analysed 175 000 individuals from 51 nationally representative surveys, using self-reports of WS and DA as the measures of asthma. The fixed-effects and random-effects estimates of the pooled ORs between asthma and underweight (BMI <18.5 kg/m2), obesity (BMI ≥30 kg/m2), smoking, drinking and SFU were reported.
Results The pooled risks of all individual risk factors were significantly associated with WS and DA (with the exception of current smoking with DA in women and SFU with DA in both genders). Stronger dose–response relationships were seen in women for smoking amounts and duration; BMI showed stronger quadratic relationships. The combined risks were generally larger in women than in men, with significant risks for underweight (OR=2.73) as well as obese (OR=2.00) smokers for WS (OR=2.13 and OR=1.58 for DA, respectively). The magnitude of the combined effects from low/high BMI, smoking and drinking were also consistently higher among women than among men in WS and DA. SFU among underweight smokers also had positive association with WS (men and women) and DA (women).
Conclusions BMI, smoking, drinking and SFU—in combination—are associated with double or triple the risk of development of asthma. These risk factors might help explain the wide variation in asthma burden across countries.
- Asthma
- Asthma Epidemiology
- Tobacco and the lung
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
This is the first study to assess the combined effects of body mass index (BMI), smoking, drinking and solid fuel use (r; SFU) on wheezing symptoms (WS) and diagnosed asthma (DA).
BMI, smoking, drinking and SFU—in combination—are associated with double or triple the risk of development of asthma.
The magnitude of the combined effects from low/high BMI, smoking and drinking was consistently higher among women than among men in WS and DA.
Introduction
The rising health and economic burden of non-communicable respiratory diseases such as asthma over the recent decades presents a significant challenge to public health.1 As per the 2014 Global Asthma Report estimates, asthma is the 14th most important disorder in terms of extent and duration of disability, and currently affects about 334 million people.2 Asthma is a complex disease with multiple potential risk factors of genetic, environmental and behavioural nature, such as solid fuel use (r; SFU), tobacco smoking, alcohol and body mass index (BMI).3 These potential factors are currently underexplored, but have called for greater attention, especially given the international variations in asthma prevalence, and increasing burden in the low-income and middle-income countries (LMICs).1
Adverse health impacts of SFU, smoking, drinking and BMI, as an individual risk factor, on respiratory diseases have been reported in various study settings, although the impact on asthma is, in general, inconsistent. For example, some studies found a positive but unadjusted association between SFU and asthma or wheezing,4–7 while others found no significant effect.8–11 For BMI, most studies found an increase in BMI as a risk factor,12–14 and others suggested that weight loss in obese individuals may reduce asthmatic symptoms.15 ,16 The impact of alcohol consumption, independent of smoking, is also mostly conflicting, with either a U-shaped effect of the dose of alcohol,17 or no significant association.18 The literature also reports a greater incidence of asthma with exposure to tobacco smoke, but the evidence on frequency or severity of symptoms is not provided.19–22 Additionally, the combined effects of these risk factors have not been adequately/sufficiently explored, when individuals are exposed to multiple risk factors.
The concurrent impact of these risk factors may better help explain the wide variation in asthma prevalence across countries. These interactions can be steadily measured using individual participant data (IPD), but not very accurately from summary measures provided in published studies. Nationally representative studies, as used in our paper, enable reliable country-level projections of the proportion of asthma attributed to the aforementioned risk factors. We, therefore, conducted IPD meta-analyses of standardised national surveys in 51 countries chiefly to investigate combined effects of tobacco smoking, alcohol drinking, SFU and BMI on the risk of self-reported wheezing symptoms (WS) and on diagnosed asthma (DA).
Methods
Data
The WHO implemented the World Health Surveys (WHS) between 2002 and 2004 in 70 countries,23 including 51 countries that collectively covered about 77% of estimated global asthma cases (19 countries were excluded from our study due to missing information on either education, smoking, SFU or drinking). WHS household samples were drawn from nationally representative sampling frames23 except in China, India and Russia, where the surveys were conducted in specific regions. Adults aged 18+ years were randomly selected from each eligible household. Our analysis focused on ages 18–44 years to reduce confusion between asthma-related symptoms and chronic obstructive pulmonary disease (COPD).24 Between these ages, about 55% of all global asthma cases were reported.2
Two main outcomes, WS and DA, were identified if there was a positive response to any of the following survey questions: ‘During the past 12 months, have you experienced any of the following: (1) attacks of wheezing or whistling breathing or (2) attack of wheezing that came on after you stopped exercising or some other physical activity?’ to define WS; and ‘Have you (ever) been: (1) diagnosed with asthma (an allergic respiratory diseases) or (2) treated for it or (3) taking any medications or other treatment for it during the past 2 weeks?’ to define DA. Our reference population consisted of those who answered at least one of the questions above, but did not report a positive response to any of them. Those who did not answer any of the questions above were excluded from the analysis.
Four exposures were studied. Current smoking was defined as daily or occasional smoking. Among current smokers, daily consumption was classified as 1–10, 11–20, 21+ cigarettes per day, and the duration as 1–10, 11–20 and 21+ years of daily smoking. Drinking was defined based on a positive answer to a single question ‘Have you ever consumed a drink that contains alcohol (such as beer, wine, etc)?’ BMI was calculated from self-reported body weight and height. Low and high BMI were defined as <18.5 kg/m2 for underweight (BMIuw) and ≥30 kg/m2 for obese (BMIobs), with dose–response analysis examining BMI scores of <18.5, 18.5–24.9, 25–29.9 and ≥30 kg/m2. SFU was defined as the household combustion of solid fuels (such as dung, charcoal, wood or crop residues) for cooking.
Statistical analysis
We used logistic regression to relate the ORs and the corresponding 95% CIs for WS and DA, separately. Analyses were stratified by gender and adjusted for age, level of education (no formal education or less than primary vs primary education completed or more), fruits and vegetable consumption, and, where relevant, self-reported current smoking, alcohol use, BMI, type of cooking fuel and WHO regions were further adjusted. To analyse the effect sizes when individuals were exposed to multiple risk factors of asthma, combinations of BMIuw/obs, smoking and drinking or SFU were used in logistic regression models.
The OR for each exposure category is accompanied by CI derived only from the SE of the log risk in that one category. Hence, each OR, including that for the reference group, is associated with a group-specific CI that can be thought of as reflecting the amount of data only in that one category.25 The 95% group-specific CI for OR is (OR/K, OR×K), where K=exp (1.96×SE) and SE is the SE of the log risk. If the reference group with OR=1 and another group with OR=R have, respectively, group-specific CIs (a, b) and (c, d), then the CI for R that allows for the variation in both of the groups is (√[cd/k], √[cdk]), where log (k) is given by √(log2 [d/c]+log2 [b/a]); since k>d/c, this CI is wider than (c, d).
Statistical heterogeneity between country-specific surveys was assessed using I2 statistic. For the analysis in which we found no significant heterogeneity (<50%), effect estimates were given a weight equal to the inverse variance of the country-specific survey (fixed-effects model). For those analyses in which we noted significant heterogeneity, we used a random-effects model to assign the weight of each country-specific survey according to the DerSimonian and Laird method.26 With dose–response analysis data (smoking, BMI), the risk estimates for each category were pooled using the inverse variance weighted method to derive a single estimate for each range of dose, and trend test was performed to validate if a trend of ORs exists. In order to assess the effect of study quality on the reported effect estimates, we conducted sensitivity analyses in which we compared pooled effect estimates for subgroups stratified by smoking status, SFU and no use, and country's income status (LMIC vs high-income country (HIC)). Sensitivity to additional SFU-related information, such as stove type, availability of chimney and separate kitchen, was also tested. All analyses were conducted using R V.3.2.0 and STATA V.12.1.
Results
Of the 174 556 adults aged 18–44 years from 70 countries interviewed in the WHS, 112 711 individuals (men: 52 154; women: 60 557) from 51 countries and six WHO regions (including 41 LMICs) met our selection criteria. More women (27%) than men (22%) had less than primary education (table 1). Men showed a higher incidence of smoking and usage of alcohol than women. More women than men were underweight (men: 9%; women: 11%) or obese (men: 6%; women: 9%); both were comparable in the incidence of WS (men: 6%; women: 7%) and DA (men: 4%; women: 5%). Regionally, South-East Asia and the Western Pacific Region had the highest proportions of underweight population (men: 23% and 11%; women: 29% and 18%); the Americas, Europe and the Eastern Mediterranean region had the highest proportions of overweight population (men: 35%, 37% and 24% ;women: 28%, 22% and 27%); the Western Pacific Region had high prevalence of male smokers (60%) while African regions had highest proportions of SFUs (men: 69%; women: 73%). The gender-specific prevalence of smoking, drinking, and BMIuw and BMIobs were generally consistent with global reviews of the country-specific data (see online supplementary table S1).
Supplementary tables
Number of individual participants included in the study (total N=121 711) by WHO region and their characteristics; data from the World Health Surveys for the years 2002–2004
When all risk factors were treated individually, BMIuw, BMIobs, current smoking and ever drinking showed significant association with WS and DA for men and women, except for smoking with DA in men (see online supplementary table S2). When stratified by current smoking status (see online supplementary table S3), compared with obese non-smokers, obese smokers had higher risk of WS and DA. On the contrary, underweight SFUs compared with non-SFUs had an increased risk for WS and DA (see online supplementary table S4). Drinking had a stronger effect on the risk of WS and DA in LMICs than in HICs, while smoking in HICs had stronger effect on risk of WS (see online supplementary table S5).
Significant linear trends between current smoking status, increasing dose and duration of smoking and WS were consistently found in all stratifications, although such trends were not observed with DA, except for women when stratified by gender. Significant quadratic trends (U-shaped relationships) between BMI categories and both health outcomes were also observed in all population, except in HICs (see online supplementary tables S1–S5).
Combined effects of low/high BMI, smoking, drinking and SFU
Owing to sample size restrictions, we conducted two separate combined effect analyses: a combination of BMIuw/obs, smoking and drinking in all 51 countries; and a combination of BMIuw/obs, smoking and SFU in 41 LMICs. In both analyses, risks in each exposure level were calculated relative to those who did not smoke or drink, with a BMI range of 18.5–29.9 kg/m2 (control group).
In men and women with WS, combined effects of low/high BMI, smoking and drinking were significant (figure 1A). In underweight and obese men, concurrent smoking and ever drinking showed twofold higher risk compared with the control group (BMIuw OR=2.02 (1.62 to 2.50); BMIob OR=1.99 (1.54 to 2.57)). In women with WS, risks were twofold and threefold with both drinking and smoking in underweight and obese women, respectively (BMIuw OR=2.28 (1.58 to 3.29); BMIob OR=3.09 (1.10 to 2.90)). For DA, also, smoking, drinking and low/high BMI in combination had higher risks in men and women (figure 1B). In men with DA, risks were significant for drinking and smoking (BMIuw OR=1.59 (1.18 to 2.15); BMIobs OR=1.63 (1.14 to 2.31)). Women who concurrently drank and smoked showed significantly higher risk of DA in underweight and obese categories (BMIuw OR=1.89 (1.18 to 3.03); BMIobs OR=2.26 (1.51 to 3.38)). In WS and DA, the magnitude of the combined effects from low/high BMI, smoking and drinking were consistently higher among women than that among men.

(A) Risk of BMI, smoking and drinking on wheezing symptoms. (B) Risk of BMI, smoking and drinking on diagnosed asthma. BMI, body mass index.

Continued
After combining low/high BMI with smoking and SFU statuses, significantly increased risk of WS was observed when individuals were also exposed to smoking and SFU (OR=2.09 (1.72 to 2.54)) among underweight men (figure 2A). In women, the risks of WS among underweight smokers who did (OR=1.88 (1.36 to 2.59)) or did not use SF (OR=2.73 (1.80 to 4.13)) were significantly higher than in the control group. Among all smokers, except for underweight men, SFU did not seem to add any significant risks of WS. In women with DA, the risk was twofold higher in non-SFU smoking underweight women (BMIuw OR=2.13 (1.25 to 3.64; figure 2B)). Among men, combined effects for DA were not significant with any combinations in either BMI group. Significant heterogeneities between four groups of dyads were also not observed among men.
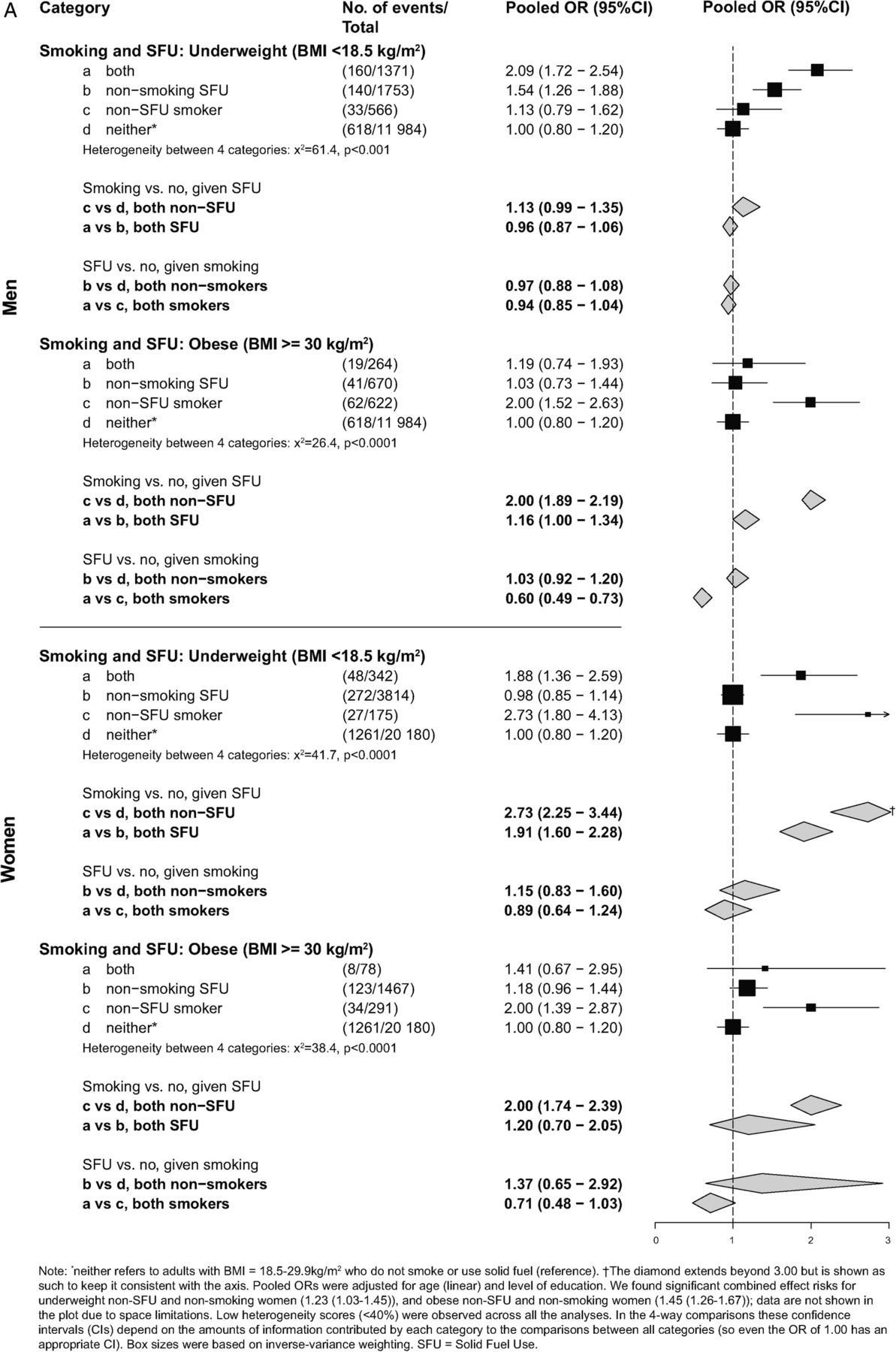
(A) Risk of BMI, smoking and solid fuel use on wheezing symptoms. (B) Risk of BMI, smoking and solid fuel use on diagnosed asthma. BMI, body mass index; SFU, solid fuel use.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continued
Discussion
Our pooled analyses showed that low/high BMI, smoking, drinking and SFU have a combined as well as independent effect on the risk of WS and DA in men and women. Risk estimates were in general greater for WS than for DA; this could be due to over-reporting of WS, which was self-reported, unlike DA, which was confirmed by a physician. Risks were also for the most part greater in women than in men, for WS and DA.
Similarly, for combined effects with low/high BMI, smoking and alcohol, women in general showed higher risk estimates for WS and DA. Results from our combined effect analyses indicated that both underweight and obese women who also smoke and drink are about 2.3 and 3 times more likely to experience WS, and about 1.9 and 2.3 times more likely to have DA, respectively, compared with women with a BMI range of 18.5–29.9 kg/m3 who do not smoke or drink. Drinking seemed to have a significant and stronger impact on WS and DA in non-smokers only. Smoking, on the other hand, significantly increased the risk of WS in drinking and non-drinking men and in non-drinking women, while being marginally or non-significant in drinking women, perhaps due to a much smaller sample size of women with both habits. The effect of smoking on DA was mostly non-significant among drinkers and non-drinkers, except for non-drinkers among underweight women, thus highlighting, contrary to previous studies, the significant impact of low BMI,15 ,16 and the non-significant effect of drinking, also inconsistent with some published findings.17
SFU showed a stronger impact on WS among non-smokers than among smokers for obese men and women, and for underweight women. For WS, smoking also showed a stronger impact on WS in non-SFU obese men and women. Most of these risks were not strong and often insignificant for DA among men and women, except for underweight female smokers who did not use solid fuel. These findings were consistent with the literature reporting a stronger association with increasing BMI, particularly in women.13 ,27
In a sensitivity analysis, we noticed a reduced (rather than increased) risk of DA in men and women using SF in less ventilated and non-separated kitchens (data not shown). This could be due to the reverse causality related to people taking medications for asthma, which may be reducing the expected impact of SFU and reduced ventilation. Under these same cooking conditions, the risk of WS was significantly higher for men (OR=1.49, 1.33 to 1.48; data not shown), further indicating the harmful effect of SFU and poor ventilation. Only a slight increase in risk was seen for women (OR=1.14, 1.00 to 1.46), contrary to our prediction of a higher risk since women are the primary SFUs and, in combination with poorly ventilated conditions, should show higher risks; a low estimate was perhaps because of a small sample size of women. A larger sample of women in more ventilated kitchens shows more clearly the impact of SFU on increased risk of WS (OR=1.25, 1.14 to 1.37).
We found a significant positive relation between smoking, and both, WS and DA, in men and women. The adjusted risks also increased with prolonged use and dose of smoking; the impact being greater on women than on men. These results are consistent with the published findings showing a higher incidence of asthma in current and ex-smokers, with higher dose and duration showing even greater risks.21 Finally, we also found a significantly higher risk for WS among men and women when exposed to SFU; ORs increase profoundly for smokers or those with low/high BMI. We did not, however, find a significant association between SFU and DA; this could be due to a low sample of SFUs in the DA group, although a few other studies have reported similar findings.8 ,10 Although the risks of DA are non-significant, the harmful impact of SFU on pulmonary function (as in the WS and combined effects) must not be ruled out.
Strengths and limitations
One of the strengths of this study is that it explored both the combined and individual effects of the various potential risk factors, while also investigating the regional variations in WHO regions. The study results are broadly representative of many countries where prevalence of asthma remains common, and are based on standardised methods. Results showed consistency across countries, with little attenuated adjustment for possible confounding variables and clear dose–response relationships. There are, however, a few potential limitations to this study.
First, the assessment of asthma-related outcomes and risk factors was based on self-reported responses to the WHS questions. An affirmative response to questions on WS might indicate those with COPD, although COPD would tend to occur at ages older than our specified range of 18–44 years. Studies also show self-reported asthma has a sensitivity between 60% and 65% and specificity between 65% and 70%, in comparison to peak expiratory flow testing.28 Self-reported tobacco smoking, drinking alcohol or height/weight measurements may not have been accurate due to recall or reporting bias, especially in some cultural settings, where smoking or drinking is considered to be socially prohibitive or stigmatising. However, this would tend to make our estimates more conservative. For example, the prevalence of smoking among those self-reporting WS/DA in our study was lower than that reported in other studies.29 ,30 This might reflect under-reporting of smoking by those with WS/DA.
Second, information on exposure to ambient air pollution and secondhand smoking (SHS), which are both known to be associated with increased risk/exacerbation of asthma, was not available in WHS.1 ,31 Large proportions of the populations in Asia and North and West Africa are exposed to high concentrations of ambient fine particulate matter.32 SHS may be particularly important for populations where the male smoking rate is very high while the female smoking rate is very low, such as those of Bangladesh and India. Again, this will result in underestimation of the true effect of smoking on asthma.
Implications
Given a limited number of studies on the simultaneous effect of various risk factors, our analysis covering these factors and their combined effects has important implications for asthma morbidity. The concurrent impact of these factors on WS and DA calls for greater emphasis on collaborative—rather than isolated—efforts, to reduce their exposure. Equally important is the impact on the working age population specifically, which points to another potential area of focus for future intervention strategies.
References
Footnotes
Contributors JP and PJ were involved in conception and design. JP, YIM and SM were involved in analysis and interpretation. JP, YIM, SM, MB, DA, DSM, PCG and PJ were involved in drafting the manuscript for important intellectual content.
Competing interests None declared.
Funding This study is supported by grants from the US National Institutes of Health (R01-TW05991-01 and TW07939-01), Canadian Institutes of Health Research (IEG-53506), and the Bill and Melinda Gates Foundation (57350).
Disclaimer The opinions expressed in this article are those of the authors and do not necessarily represent those of the institutions with which they are affiliated.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.