Article Text

Abstract
Introduction Sarcoidosis is a multisystem disease, predominantly affecting the lungs but can involve the heart, resulting in cardiac sarcoidosis (CS). Patients require MRI/Positron Emission Tomography (PET) scans for diagnosis. Echocardiography, ECG and Holter monitoring may be indicative but not diagnostic alone. Patients can present late with conduction defects, heart failure or sudden death. The CASPA (CArdiac Sarcoidosis in PApworth) study protocol aims to (1) use MRI to identify CS prevalence; (2) use speckle-tracking echocardiography, signal averaged ECG and Holter monitoring to look for diagnostic pathways; and (3) identify serum proteins which may be associated with CS.
Methods and analysis Participants with pulmonary sarcoidosis (and no known cardiac disease) from Royal Papworth Hospital will have the following: cardiac MRI with late gadolinium, two-dimensional transthoracic echocardiography with speckle tracking, signal averaged ECG and 24-hour Holter monitor. They will provide a serum sample for brain natriuretic peptide levels and proteomics by liquid chromatography coupled to high-resolution mass spectrometry. All data will be collected on OpenClinica platform and analysed approximately 6 months after final patient recruitment.
Ethics and dissemination The Camden & Kings Cross Research Ethics Committee approved the protocol (REC number: 17/LO/0667). Integrated Research Approval System (IRAS) 222 720. Dissemination of findings will be via conference presentations and submitted to peer-reviewed journals.
- sarcoidosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
This is a protocol paper for the CASPA(CArdiac Sarcoidosis in PApworth) study. Sarcoidosis is a multisystem disease characterised by non-caseating granulomas which predominantly affect the lungs in more than 90% of cases. Extrapulmonary sites include the heart, skin, liver, eyes and central nervous system.1 The aetiology is not fully understood but is likely due to an interplay between an environmental trigger and a dysregulation of the host immune system.2 3 Previous clinical studies estimate that cardiac sarcoidosis (CS) occurs in approximately 5% of cases1 but autopsy studies reported cardiac involvement in about one-fourth of cases in the USA or Europe4 and higher in Japan, suggesting up to 69% involvement.5 The incidence of CS is higher in Japanese patients with sarcoidosis, and it is the leading cause of sarcoid-attributed death (77%–85% in Japan).6 The true incidence is therefore hypothesised to be in between these figures, but this is complicated as the clinical diagnosis of CS can be challenging. The disease can be difficult to both diagnose and manage; nevertheless, a significant proportion of patients with limited pulmonary involvement have a mild course with good outcome, often not requiring corticosteroids or immunosuppression treatment.7 However, a large retrospective study of over 600 000 US hospital admissions for patients with sarcoidosis showed that a 31% had coexisting cardiac disease.8 The heart can be involved in sarcoidosis in one of three ways. First, patients with sarcoidosis are at higher risk of cardiovascular disease including heart failure and ischaemic heart disease.9 Second, they can develop pulmonary hypertension with associated right heart dysfunction. Third, they can have ‘true’ CS where granulomas directly affect the heart leading to conduction disturbance, atrial or ventricular tachyarrhythmia, heart failure or sudden death. CS is reported to be the second most common cause of sarcoid-related mortality and can affect young and otherwise relatively healthy patients.10 An early and accurate diagnosis is therefore paramount to prevent cardiac-related morbidity and mortality.
The 2014 joint consensus statement from the World Association for Sarcoidosis and Other Granulomatous disorders (WASOG), the American College of Cardiology and the American College of Chest Physicians states that there are no currently accepted international guidelines for the diagnosis of CS.11 A cardiac biopsy to reveal non-caseating granulomas is the gold standard single diagnostic method but is rarely performed due to the invasive nature of the test, associated morbidity and low diagnostic sensitivity resulting from patchy cardiac infiltration by granulomas.12 Abnormalities on non-invasive cardiac imaging modalities (MRI or Positron Emission Tomography (PET) scan), coupled with the presence of extracardiac sarcoidosis, are taken by most experts as representing a confident diagnosis of CS.11 Other modalities such as ECG and Holter ECG monitoring may be indicative of a diagnosis but cannot be diagnostic of CS by themselves due to low sensitivity and specificity.
The lack of consensus means that studies are urgently needed to accurately quantify the prevalence and severity of disease. In the current study, we propose a three-pronged investigation to improve our understanding and to optimise the diagnostic pathway of CS in patients with pulmonary sarcoidosis and no prior significant cardiac disease.
First, to use state-of-the-art MRI scanning (including water-sensitive sequences and T2 to assess for oedema and infiltration) to quantify prevalence of CS in a population of patients with newly diagnosed pulmonary sarcoidosis. This will allow us to accurately identify prevalence of cardiac involvement in our population.
Second, to identify the predictive value of 12-lead ECG, signal-averaged ECG, 24-hour ambulatory Holter monitoring, two-dimensional (2D) transthoracic echocardiography combined with speckle-tracking analysis, in identifying evidence of underlying cardiac involvement (using MRI as the gold standard) and formulate the optimal diagnostic pathway that will allow patients to be screened for cardiac involvement without the need for the ‘gold standard’ MRI which requires expertise to perform and interpret.13
Third, to perform cutting-edge proteomics and cytokine profiling on sera from our population to identify biomarkers associated with cardiac involvement. The identification of specific proteins may allow us to create simple and cost-effective blood tests to help accurately diagnose CS prior to confirmation with imaging modalities.13
Methods and analysis
Study design and patient selection
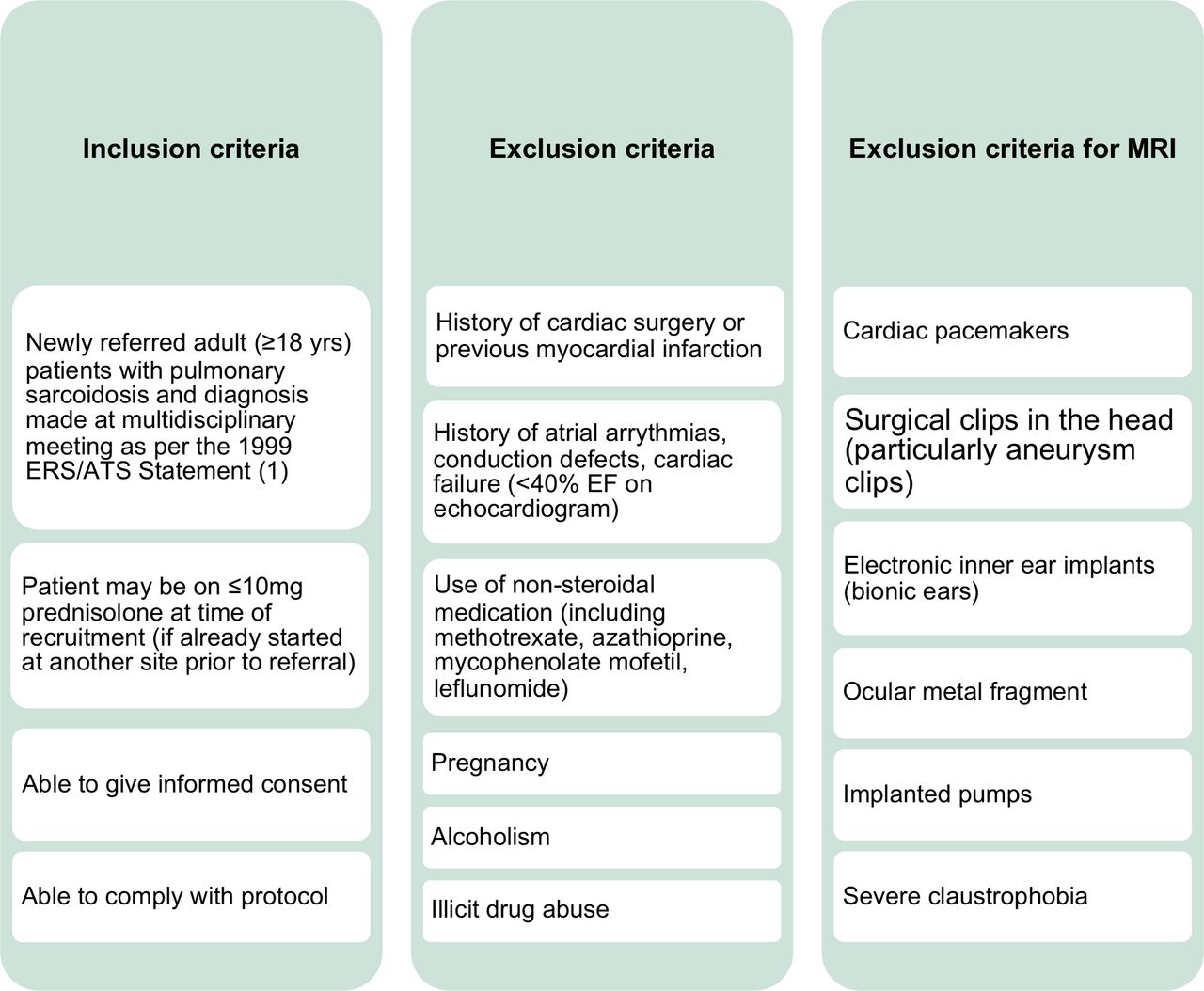
This is a prospective observational cohort study (planned to run from 2017 to 2021) for patients with pulmonary sarcoidosis with confirmed diagnosis by the Interstitial Lung Disease (ILD) MDT at Royal Papworth Hospital NHS Foundation Trust, which receives referrals from the surrounding area (East of England). Additional participant identification centres (PICs) are open at Cambridge University Hospitals and Norfolk and Norwich NHS Trust. All consecutive new patients with sarcoidosis discussed at MDT or seen in clinic who meet the eligibility criteria (figure 1) will be approached and invited to take part in the study.

Inclusion and exclusion criteria for the CASPA (CArdiac Sarcoidosis in PApworth) study. EF, Ejection Fraction.
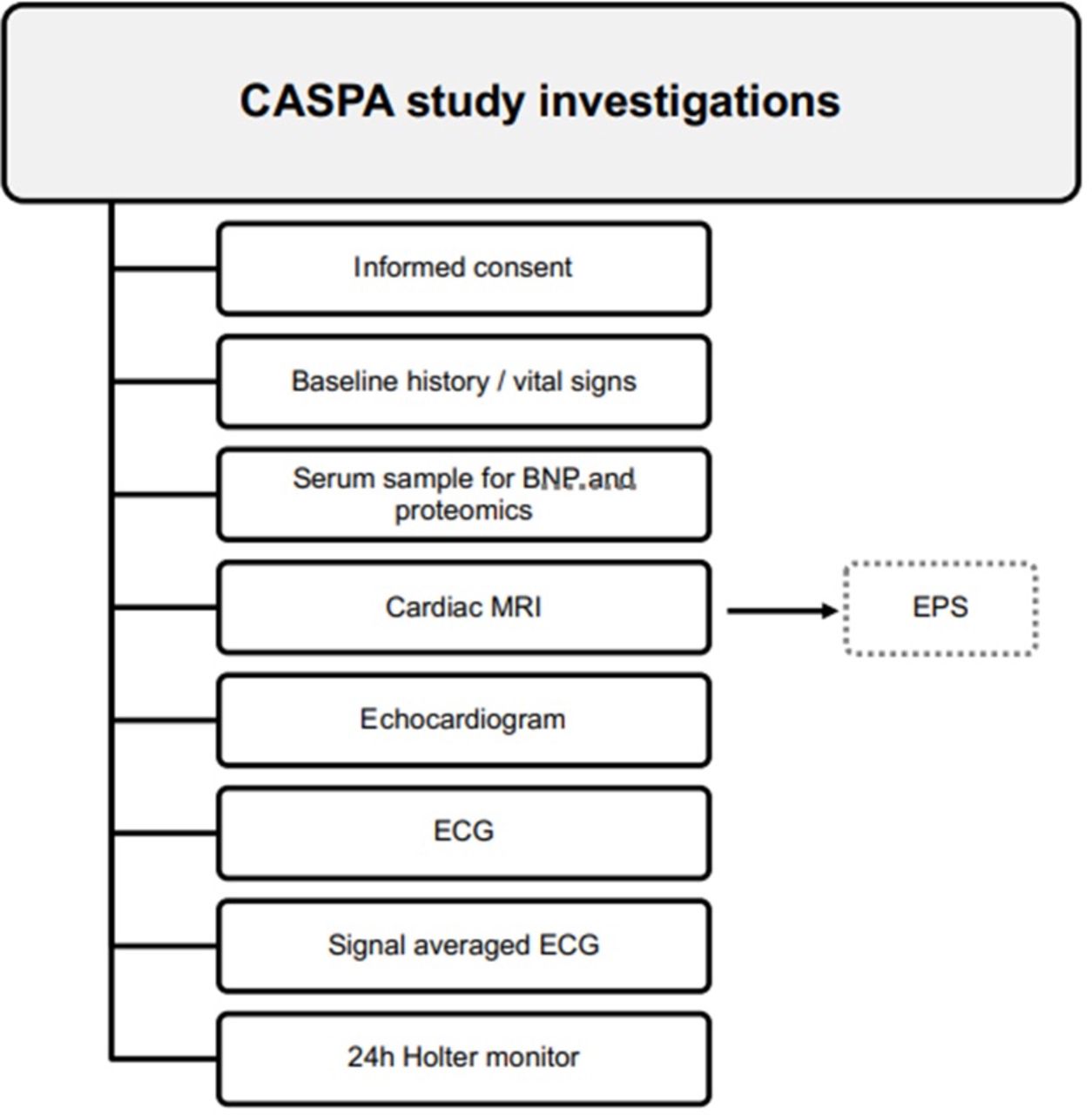
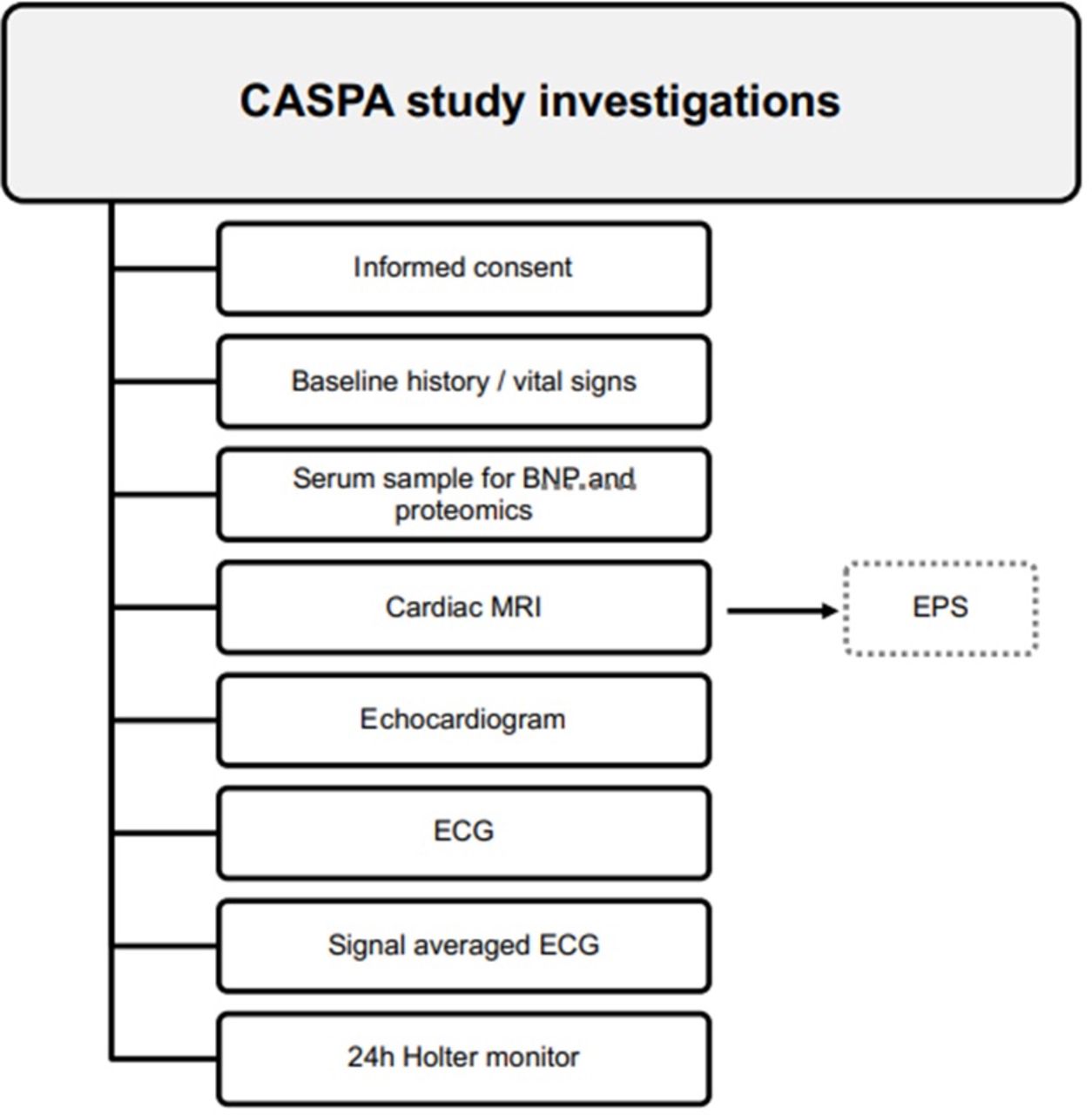
The study will assess for any cardiac disease (including and specifically CS) in participants with pulmonary sarcoidosis (and no significant cardiac disease). Study investigations will be conducted in one visit (figure 2). No therapeutic intervention will be carried out in the study. Any participant with confirmed CS diagnosis (based on MRI findings) will be offered further investigations (including electrophysiology studies where indicated) and treatment as deemed necessary by a consultant cardiologist and consultant electrophysiologist with a specialist interest in the management of CS. This group will then be offered ongoing clinical follow-up within the ILD service.
{kind=link}
{kind=link}
CASPA (CArdiac Sarcoidosis in PApworth) study investigations. All patients will have the tests shown in a single study visit. A blood sample will additionally be taken for serum brain natriuretic peptide (BNP) analysis and subsequently stored as serum for proteomics. Any patients identified as having cardiac sarcoidosis (CS) on MRI will be offered a clinical review with an electrophysiologist with a view for an Electrophysiology (EP) study.
Study objectives
The primary objective is to assess the prevalence of CS in patients with a new diagnosis of pulmonary sarcoidosis using cardiac MRI as the gold standard investigation for the detection of cardiac sarcoidosis. The secondary objectives are (1) to determine the optimal diagnostic pathway of investigation to identify confirmed cardiac involvement on cardiac MRI using 12-lead ECG, signal-averaged ECG, 24-hour ambulatory Holter monitoring, and 2D transthoracic and speckle-tracking echocardiography; and (2) to determine the ability of novel serum biomarkers to identify confirmed cardiac involvement on cardiac MRI.
Study investigations
Cardiac MRI
Cardiac MRI scans will be performed with a 1.5 T Siemens Avanto or Aera MRI scanner (Siemens Healthcare, Erlangen, Germany) using a dedicated eight-channel phased-array cardiac coil under ECG gating and breath-holding in line with standard recommendations. To evaluate the anatomy of the left and right ventricles cine images with steady-state free precession will be obtained from short axis and long axis (slice thickness 8 mm, interslice gap 0 mm). Black blood T2-weighted images will be acquired to assess for oedema and infiltration in the short-axis orientation before administration of contrast media. Late gadolinium imaging will assess presence and anatomical distribution of late myocardial scar. Ten minutes after the administration of a gadolinium-based contrast medium (0.2 mmol/kg, Gadobutrol, Bayer AG, Leverkusen, Germany), contiguous short-axis slices from the base to the apex of the left ventricle will be acquired using a breath-holding ECG-gated sequence as well as standard long axis sequences. Single shot phase sensitive inversion-recovery LGE images will also be acquired.
Cardiac MRI (CMR) images will be randomised by expert radiologists. Left and right ventricular volume and ejection fraction will be measured offline using standardised postprocessing recommendations using commercially available software (CVI42; Circle Cardiovascular Imaging, Calgary, Alberta, Canada) and the presence of localised wall thinning and regional wall motion abnormalities determined. Extent and distribution of LGE will be determined by visual assessment with segmental analysis of anatomical distribution and pattern of late gadolinium enhancement as epicardial, intramyocardial or subendocardial. An abnormal CMR will be defined as the presence of Left Ventricular (LV) or Right Ventricular (RV) regional wall motion abnormalities, localised hypertrophy or wall thinning of the RV or LV, LV systolic dysfunction (as defined by an Left Ventricular Ejection Fraciton (LVEF) <50%) or the presence of LGE in a non-vascular distribution.
2D transthoracic echocardiography
Standard 2D echocardiographic data will be obtained from the study performed on the same day as the CMR. All studies will be performed on a Philips IE33 or EPIC System (Philips Medical Systems, The Netherlands) with an S5 transducer. Chamber quantification and function, and the presence of valvular heart disease will be assessed according to the published American Society of Echocardiography guidelines.14 2D data sets for speckle-tracking analysis include three short-axis views (basal, midventricular, apical) and three apical longitudinal views (4-chamber, 2-chamber and 3-chamber). Adjustments in sector depth and angle will be made to yield a temporal resolution of 80–100 frames per second. A minimum of 40 frames per cycle is required for offline analysis (with a range of 40–82 frames per cycle achieved). The speckle-tracking programme, VVI V.3.0.0 (Siemens Healthcare, Mountain View, California, USA) will be applied to the echocardiographic images from archived studies, allowing endocardial, myocardial and epicardial strain parameter assessment. Longitudinal strain will be measured from the apical 4-chamber, apical 2-chamber and apical 3-chamber views on echocardiography. Circumferential strain will be measured in three short-axis views (basal level at the mitral valve, midventricular level at the papillary muscles and the apical level at the true LV apex). All echocardiographic images will be analysed in a random order by a single reader. An abnormal echocardiogram will be defined as the presence of LV or RV regional wall motion abnormalities, localised hypertrophy or thinning of the LV or RV myocardium, or LV systolic dysfunction as represented by an LVEF <50% (assessed by Biplane Simpsons method from 2D data).
12-lead ECG and ambulatory Holter monitoring
Standard resting 12-lead ECG will be performed on all study participants as per current clinical practice. They will undergo a 24-hour period of ambulatory ECG monitoring as per standard clinical practice and the monitor will be removed by the participant at home after the 24-hour period and posted back (with a prepaid envelope) to the study site.
Signal-averaged ECG (SAECG)
Resting SAECG will be performed concurrent with the 12-lead ECG to record low-amplitude electrical activity in the myocardium by averaging a large number of high-resolution QRS complex recordings. The following criteria will be used to determine the presence of late potentials: (1) filtered QRS duration ≥114 ms, (2) RMS‐40<20 μV, and (3) LAS‐40>38 ms. Late potentials are generally considered present, when at least two of three conventional or modified criteria are satisfied.
Clinical data collection
Clinical observations for routine outpatient clinics and medical history will be recorded at the study visit, including respiratory (breathlessness and presence of cough) and cardiac symptoms (palpitations and dizziness). Additionally, we will document any steroid medications (oral or inhaled) and the latest results for relevant routine clinical assessments including chest radiographs, high-resolution CT, pulmonary function tests and 6-minute walk test.
Proteomic analysis
Serum proteins will be quantitated using label-free quantitative mass spectrometry. Each serum sample will be processed by liquid chromatography coupled to high-resolution mass spectrometry to generate an intensity value for approximately 600 serum proteins. These data will be stratified by cardiac involvement in sarcoidosis to determine potential serum biomarkers associated with CS (based on MRI diagnosis of CS) for hypothesis-generating research. Any novel biomarkers will also be correlated with serum B-type natriuretic peptide levels which are taken at time of patient study visit.
Sample size calculations and statistical analysis
A sample size calculation of 104 participants is based on the expected 30% prevalence of CS in our patient cohort, assuming 0.95 specificity and sensitivity of the cardiac MRI (as the proposed gold standard test for the purpose of this proposal) and 0.064 precision of the 90% CI. With regard to our secondary objectives, we will use signal averaged ECG (SAECG), 24-hour ambulatory Holter monitoring and speckle-tracking echocardiogram as surrogate variables for MRI. All of them are binary variables (0=no heart problem, 1=heart problem). Binary logistic regression will associate MRI outcome (yes/no) with each of the three alternatives, independently, in conjunction with additional confounders such as age, sex and ethnicity. Hence, the three models will be identical, but for ECG, 24-hour tape or echo, only one will appear in each model. The area under receiver operating characteristic curve will be calculated for the overall discrimination assessment of the model and model comparisons. In addition, pseudo R-squared15 will also be reported and alternatively used for model comparisons as well.
Study oversight and data analysis plan
A multidisciplinary steering committee has been formed which will include study investigators, research nurses, sponsor and funder representatives, study statistician and data manager, plus a patient and public representative. It will convene at 6 monthly intervals. All data including clinical records, informed consent forms and patient information sheets will be stored at Royal Papworth NHS Trust as per standard data protection guidelines. Data will be collected either at the time of visit or subsequently by clinical notes analysis and will be entered into a study-specific electronic case report form built on the enterprise edition of the clinical data management system, OpenClinica. All data will be analysed at the end of the data collection period (approximately 6 months after the final patient has been recruited). The local standard operating procedure (SOP) for archiving of research studies will be followed (Reference RPH:SOP011).
Patient and public involvement
The original research question and the need for improved testing for CS were discussed with patients with pulmonary sarcoidosis from both the Royal Papworth Hospital and patients who were members of the charity Sarcoidosis UK (at the time called SILA). After these initial discussions, patients had no further input into the study design. Individual participants will have access to their own study results and all participants will be given access to final publications.
Ethics and dissemination
The London – Camden & Kings Cross Research Ethics Committee has approved the study protocol (REC number: 17/LO/0667). Integrated Research Approval System (IRAS) 222 720. Dissemination of findings will be via presentations at clinical academic conferences and submitted to peer-reviewed scientific journals.
Discussion
The prevalence of CS (especially in patients with no overt cardiac signs or symptoms) in the UK is unknown. Worldwide, there is variation between studies and countries. For this reason, the primary objective of this study is to identify the number of patients who have MRI evidence of CS within a group of 104 patients with pulmonary sarcoidosis. Clinical data have suggested that only 5% of all patients with sarcoidosis have clinically apparent CS1 but autopsy studies from the USA and Japan have suggested that this figure may be higher, between 16% and 69%.5 6 16–19 In one small study of patients with sarcoidosis who died suddenly, autopsy revealed granulomas present in the left ventricle in all 17 patients.20 As such, CS may lead to conduction disturbances including and up to complete heart block, atrial or ventricular tachyarrhythmias, congestive heart failure or sudden death. Rarer findings which have been reported include valve defects and pericardial effusions.21 22 The consequences of this may be catastrophic for patients with mild pulmonary involvement, and as such, an accurate understanding of CS prevalence is important.
The diagnosis of CS relies on imaging as features from the history and examination of a suspected patient are unreliable. A history of palpitations may be elicited but this could also be due to systemic activity in sarcoidosis or side effects of medications including corticosteroids.23 Patients may complain of breathlessness out of context with lung disease but again this may be difficult to quantify and distinguish from pulmonary sarcoidosis alone.24 25 On examination, patients may have signs of cardiac failure and a number of experts have suggested clinical review pathways which incorporate symptoms and signs into a diagnostic pathway10 but these are always taken together with appropriate imaging and cannot diagnose CS alone.
The current gold standard for diagnosis of CS (aside from a cardiac biopsy) is a compatible image suggesting CS on MRI or PET scan taken together with a secure extracardiac (most often pulmonary) diagnosis of sarcoidosis.11 MRI uses gadolinium as a contrast agent and delayed enhancement of this has a sensitivity up to 100% for diagnosis of CS with a lower specificity of approximately 80%.26 Recent use of T2 mapping to detect changes in water distribution (relating to areas of oedema) may increase accuracy and allow for serial MRI measurements to monitor the extent of CS.27 Fluorodeoxyglucose-positron emission tomography (FDG-PET) scans have similar levels of accuracy for diagnosis of CS.28 However, both MRI and PET scans are expensive to perform and interpret (often with a level of subjective analysis) and depend on specific cardiac or radiological expertise. These scanners may not be available in all hospitals and even if they are, they may be prioritised for other diseases, for example, cardiac conditions (MRI) or cancers (PET). MRI requires the use of gadolinium contrast which has the potential to cause contract reaction in a minority of patients29 and PET scans have a radiation exposure. FDG-PET scanning also requires either a specific high-fat, low-carbohydrate diet, a period of fasting or a heparin infusion prior to scanning to increase the accuracy of the imaged metabolic update in the areas of cardiac sarcoidosis.30 31 For these reasons, it is important to find alternative reliable tests which may be more accessible and interpreted.
Echocardiogram has previously been shown in some studies to be abnormal in up to 70% of patients with CS, the most common finding being left ventricular dysfunction.23 Other findings may include septal or wall dyskinesia6 with valve disease related to sarcoidosis less common.32 However, another one more recent study showed that echocardiography added to cardiac history and ECG did not change sensitivity of the initial screening strategy (68.8% vs 72.9%). Despite a high positive predictive value (83.9%), echocardiography had a low sensitivity (27.1%).13 The additional use of speckle-tracking echocardiography to measure of global longitudinal strain (GLS) is thought to significantly increase the sensitivity of CS diagnosis using echocardiogram alone with a reduction of GLS having a sensitivity and specificity of >90% in one study.33 However, this requires additional analysis and interpretation and is not available in every hospital echocardiography department.
The use of a standard 12-lead ECG is part of the initial screening of all patients with sarcoidosis but is thought to be normal in up to 50% of all patients with CS.25 When they are abnormal, the most common findings are conduction disturbances and arrhythmias.34 The additional use of a signal averaged ECG (which works to average many QRS complexes to reduce noise interference and thus may reveal subtle abnormalities) has been shown to be of additional benefit with a QRS duration <100 ms conferring up to 100% specificity in one study.35 Holter monitoring alone may be highly predictive of CS abnormalities of supraventricular tachycardia, ventricular ectopic beats and AV block indicating cardiac involvement in sarcoidosis.36 Holter monitoring is a relatively inexpensive test that can be performed in the outpatient setting with patients being asked to return the monitor after the test period is complete.
There are no widely accepted blood-based markers for evaluation of cardiac disease in sarcoidosis. Levels of pro-BNP (pro-brain natriuretic peptide) has been investigated with one study of 150 patients showing association with CS with an area under the curve of 0.913.37 However, pro-BNP is not specific for CS and is elevated in a number of cardiac diseases.38 High sensitivity cardiac troponin T (hscTnT) has been investigated and shown to correlate with serum ACE levels and may be useful in diagnosing CS.39 hscTnT has also been shown in some patients to normalise with treatment of CS using corticosteroids.40 However, serum ACE alone is unhelpful in both diagnosis and monitoring of CS activity.
Proteins associated with CS could pave the way towards simple and cheap blood tests to assist with diagnosis but this technique has not yet been used in CS. In respect to proteomics in pulmonary sarcoidosis, Surface-enhanced laser desorption/ionization (SELDI) has been shown to identify serum proteins specific to radiographic stage of sarcoidosis,41 and serum and bronchoalveolar cytokine profiles have been shown to differentiate between pulmonary forms of sarcoidosis and tuberculosis.42
Conclusions
The majority of patients with CS will initially present to respiratory teams and it is therefore important that the true prevalence of the condition is quantified, and that improved screening and diagnostic methods are developed. CS may present with a number of complications, including sudden death, in patients with pulmonary sarcoidosis who are unaware of having cardiac involvement. Additionally, patients with sarcoidosis are at higher risk of ischaemic heart disease, cardiac failure and pulmonary hypertension. The findings from the CASPA study will first identify the prevalence of CS in a population of patients with pulmonary sarcoidosis with no overt cardiac disease. Second, it will use ECG, signal-averaged ECG, speckle-tracking echocardiogram and 24-hour ambulatory Holter monitoring reports in all 104 study patients to look for combinations of these tests to be best used as a surrogate diagnosis for CS, using the MRI findings as the gold standard. Finally, a proteomic analysis will be performed on serum from all patients to look for serum biomarkers which may correlate with CS. We anticipate that these results will add information to the literature of heart disease in sarcoidosis.
Acknowledgments
The study is being conducted in collaboration with the Papworth Trials Unit Collaboration (PTUC) whose staff support the design, conduct and analysis including data management (TD, Data Manager), clinical trial management (VS), quality assurance (Dr Sarah Fielding, QA lead) and statistics (Y-DC). We would additionally like to thank Andy Bush for his guidance and support, as well as Sathya Partheeban for creating with the study name.
References
Footnotes
Contributors MT, LW, SA, KT and VS conceived the study, obtained funding, wrote the study protocol, obtained ethical approvals for the study and coordinated the deployment of analytical methods for analysis. JCQ-C took the lead in writing the manuscript with support from MT and LW. Planning and recruitment were carried out by JCQ-C, MT and KD. YC, a senior statistician, constructed a statistics and data analysis plan in conjunction with TD, MT, LW, JCQ-C. All authors contributed to the study design and study protocol.
Funding Funding for this study was awarded after a peer-reviewed grant application process by the British Lung Foundation (Sarcoidosis UK SILA grant total amount £112 816).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.