Article Text

Abstract
Introduction Patients with chronic obstructive pulmonary disease (COPD) with frequent exacerbations (ExCOPD) are commonly treated with inhaled corticosteroids (ICS) and are at risk of infections caused by potential pathogenic bacteria (PPB) including Pseudomonas aeruginosa (PsA).
Objectives To investigate the association between the use of ICS and PsA infection among ExCOPD.
Methods Case–control study with longitudinal follow-up that recruited ExCOPD after a hospitalisation due to exacerbation between 2012 and 2020. Patients with isolation of PsA (COPD-PsA) in sputum either during admission or follow-up were compared with those with other or no PPB. Clinical, functional characteristics, DDD, use of ICS and survival were evaluated. Cox regression analysis was performed to evaluate the risk factors associated to PsA infection and mortality.
Results 358 patients (78% male, mean age 73±9 years) were enrolled and followed up for a median of 4 years (IQR=3–8). 173 patients (48.3%) had at least a positive culture for PsA. COPD-PsA had more frequent exacerbations, more severe airflow limitation and higher mortality (69.4% vs 46.5%, p<0.001). There were no differences in the use of ICS between groups but the dose of ICS was significantly higher among COPD-PsA (median of 500 µg fluticasone propionate equivalents (IQR=250–1000) vs 400 µg (IQR=200–1000), p=0.007). Blood eosinophil count (BEC) was not different between ICS users and non-users. In multivariate analysis, the dose of ICS was an independent risk factor for PsA infection and mortality but not ICS use.
Conclusions ICS dose, but not its use, could be a risk factor for PsA infection in patients with severe COPD regardless of BEC.
- COPD exacerbations
- eosinophil biology
- bacterial infection
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article and the associated supplemental material; however, the datasets were not included and are available upon reasonable request. The current study is not a clinical trial.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Are inhaled corticosteroids (ICS) use a potential risk factor for Pseudomonas aeruginosa infection among frequent-exacerbator severe chronic obstructive pulmonary disease (COPD)?
The use of high-dose ICS in severe patients with COPD with frequent exacerbations is associated to Pseudomonas aeruginosa infection and poorer survival, regardless of blood eosinophil count, effect not observed with low to medium doses.
These findings should help the clinicians modify their daily practice regarding their decision on prescribing ICS for patients with severe COPD, especially regarding the dose of ICS.
Introduction
Chronic obstructive pulmonary disease with frequent exacerbations (ExCOPD) is a specific clinical phenotype that is associated with progressive decline in lung function, higher mortality and morbidity.1 2 About 50% of acute COPD exacerbations (AECOPD) are caused by potential pathogenic bacteria (PPB) infections either isolated from sputum or bronchial secretions cultures.3–5
Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis are the most commonly isolated PPB.3 4 Other Gram-negative bacteria, specifically Pseudomonas aeruginosa (PsA) and Stenotrophomonas maltophilia, are associated with more severe exacerbations and debilitated patients.6 7 PsA isolation during AECOPD hospitalisations is associated with greater degree of airway obstruction, use of systemic corticosteroids, poorer lung function, previous isolation of PsA and previous hospital admission.8–10 Further, PsA has been linked to increased airway inflammation in patients with COPD11 and mortality.12
Inhaled corticosteroids (ICS) are indicated in the treatment of ExCOPD, especially if blood eosinophil count (BEC) are higher than 300 cells/µL13 14; however, ICS therapy is associated with various adverse effects especially the risk of pneumonia15 which raises the debate about the prescription of ICS in patients with infectious exacerbations. Further, long-term use of ICS is associated with increased bacterial load in airway as well as modification of microbiome composition.16 The relationship between ICS use and the risk of PsA infection and its clinical consequences in patients with COPD are not well stablished and could modify the indication of this treatment in patients with ExCOPD caused by PsA.
Accordingly, our study aimed to: (1) investigate the association between the use of ICS and PsA infection among ExCOPD; (2) identify the risk factors associated with PsA infection among ExCOPD population and (3) study the risk factors associated with mortality among ExCOPD.
Methods
Study design and ethics
Case–control study that recruited patients with confirmed diagnosis of COPD based on Global Initiative for Chronic Obstructive Lung Diseases (GOLD) criteria with a history of frequent exacerbations after a hospitalisation due to AECOPD.13 The study was conducted in a tertiary teaching hospital between 2012 and 2020. All patients were regularly followed up after discharged in ordinary outpatient respiratory clinics or through an integrated care programme for ExCOPD running in the same hospital10 for a maximum of 8 years. All the patients signed a written informed consent.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, conduct, reporting or dissemination plans of our research.
Population
All patients who had a diagnosis of COPD according to GOLD criteria13 after a hospitalisation for AECOPD with a history of 2 or more exacerbations per year, able to produce a sputum sample either during admission or follow-up, and living in the area of influence of the hospital were included in the study. Patients with COPD with growing of PsA in at least one sputum culture taken either during admission or follow-up (either being as single isolated microorganism or mixed with other PPB) were considered cases (COPD-PsA group). Patients with cultures resulting in other PPB different to PsA or growing of usual respiratory flora were considered controls (COPD-non-PsA group). Further, patients during the follow-up who had invalid sputum sample or unable to produce sputum with no previous sputum sample positive for PsA were considered as COPD-non-PsA. Patients with COPD with non-respiratory comorbidity including deteriorative cognitive function or psychiatric illness that affected their mental capacity and substantially affected the prognosis of the disease were excluded from the study.
Procedures
All patients underwent clinical evaluation, pulmonary function testing, chest X-ray and chest CT to rule out bronchiectasis when suspected (>98% underwent CT scan during hospitalisation or on follow-up). Detailed drug history—namely long-acting ß2 agonist, long-acting antimuscarinic bronchodilators, and inhaled ICS including the type of ICS and its dose modification over the study duration—was taken. All the doses of ICS were calculated as fluticasone propionate equivalents where 100–250 µg daily dose was considered as low dose, 400–500 µg as medium dose and ≥1000 µg as high dose.17 All acute exacerbations as defined by GOLD guidelines13 and requiring hospital contact (as outpatients or requiring an emergency visit or new hospitalisation) were recorded. AECOPD was treated according GOLD guidelines.13 The patients were followed up after discharge from the hospital initially after 2 weeks and later every 3 to 6 months as scheduled visits.
Sputum culture
A sputum sample was taken for microbiological evaluation during hospitalisation for AECOPD for every patient admitted, on follow-up if the patient had either previous positive culture for PPB or at presentation with symptoms of AECOPD. Respiratory samples were collected in sterile containers within 24 hours of admission during hospitalisation and on follow-up while presenting to the hospital outpatient respiratory clinics. Samples were transferred within 2 hours to the microbiological laboratory for Gram staining and bacterial culture. Sputum samples were tested for viability of culture according to Murray-Washington criteria.18 In case of non-viable sample, another sputum sample was recollected. Patients who were unable to give valid sputum sample during hospitalisation, bronchoscopy was performed and bronchial aspirate was collected. A sputum bacterial load ≥106 or bronchial aspirate bronchial load ≥104 colony forming units/mL was considered as significant. The identified microorganisms were classified as PsA and other PPB including Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, methicillin-susceptible or methicillin-resistant Staphylococcus aureus and other Gram negative-bacilli. Other micro-organisms such as Streptococcus viridans, Staphylococcus epidermidis or Candida spp were considered non-PPB.
Variables and outcomes
ExCOPD and mortality were recorded for every patient during follow-up. The higher value of blood eosinophils was recorded. New episodes of PsA infection, PPB infection or pneumonia during hospitalisation and follow-up were also recorded. Further, the use of ICS and its dose were also recorded during follow-up of patients for further analysis.
Statistical analysis
Quantitative data were presented as mean±SD or median and IQR according to its normal distribution, while qualitative data were presented as number and percentage (%). Unpaired Student’s t-test, Mann-Whitney U test and χ2 tests were used as appropriate. Spearman correlation coefficient was used to study the collinearity between BEC, ICS and PsA infection. Bivariate and multivariate Cox regression analysis were used to evaluate the hazard factors associated with PsA infection as well as mortality. Cox regression analysis was considered based on the fact of the change of ICS use and dose—as a covariate—over the follow-up duration of the study. A multivariate model was built on the basis of the prescreening univariable significance and the clinical relevance of covariates in the initial comparisons according to the presence or absence of PsA infection. The covariates were introduced in the model manually where multiple multivariate models were evaluated. The multivariate model with the best overall goodness-of-fit was chosen. HR and 95% CI were shown. In all Cox regression models, fluticasone propionate equivalents ICS doses were considered for both groups of patients. Kaplan-Meier survival analysis was plotted in order to identify the survival probability among ICS users during follow-up. A two-tailed p≤0.05 was considered statistically significant. SPSS package (V.22.0, IBM) was used for all analyses.
Results
Patient characteristics
The current study enrolled 358 patients with COPD after discharge for an AECOPD and followed-up for a median of 4 years (IQR=3–8). 173 patients (48.3%) had at least one sputum with growing of PsA. Table 1 shows the baseline and clinical characteristics of the studied COPD population classified according to presence (COPD-PsA) or absence of PsA infection (COPD-non-PsA).
Baseline characteristics of the COPD population classified according to PsA infection during the study duration (2012–2020)
Male constituted the majority of COPD-PsA and COPD-non-PsA groups (86.7% and 69.7%, respectively, p<0.001; table 1). There was no statistically significant difference regarding age, smoking history, associated comorbidities, modified medical research council (mMRC) dyspnoea scale, history of AECOPD or pneumonia (p>0.05, table 1); however, more frequent exacerbations and lower forced expiratory volume in 1 s (FEV1%) predicted were detected among COPD-PsA group (p<0.001 and 0.036 respectively, table 1). The majority of COPD-PsA group were GOLD III and IV (46.8% and 28.1% respectively, p=0.008; table 1). Bronchiectasis was more frequently associated with PsA infection (26% vs 11.4%, p=0.001; table 1). COPD-PsA group had more frequently detected PPB compared with COPD-non-PsA group (4.49±4.66 vs 0.66±1.02, respectively, p<0.001; table 1). Inhaled antibiotics, either colistin or tobramycin, were more frequently prescribed among COPD-PsA group (p<0.01, data not shown). Systemic corticosteroids courses administrated during AECOPD were significantly more frequent among those with PsA infection rather than non-PsA group (7.68±7.14 vs 5.39±5.50, p=0.001, table 1). Further, mortality was higher among COPD-PsA throughout the 8 years of follow-up (69.4% vs 46.5%, p<0.001; table 1).
Inhaled corticosteroids
The use of ICS was not different between patients in the COPD-PsA group when compared with COPD-non-PsA (87.9% vs 82.7%, p=0.170, table 1). The daily dose of ICS was significantly higher among COPD-PsA group when compared with COPD-non-PsA infection (median of 500 (IQR=250–1000) vs 400 (IQR=200–1000) µg /day fluticasone propionate equivalents respectively, p=0.007, table 1). Fluticasone propionate was the most frequently used ICS, followed by budesonide (p=0.003, table 1). On follow-up, there was a statistically significant reduction of the daily ICS dose used in both groups when compared with the doses at the time of enrolment to the study (median of 400 (IQR=100–1000) vs 500 (IQR=200–1000) µg/day fluticasone propionate equivalents, p<0.0001, online supplemental figure S1).
Supplemental material

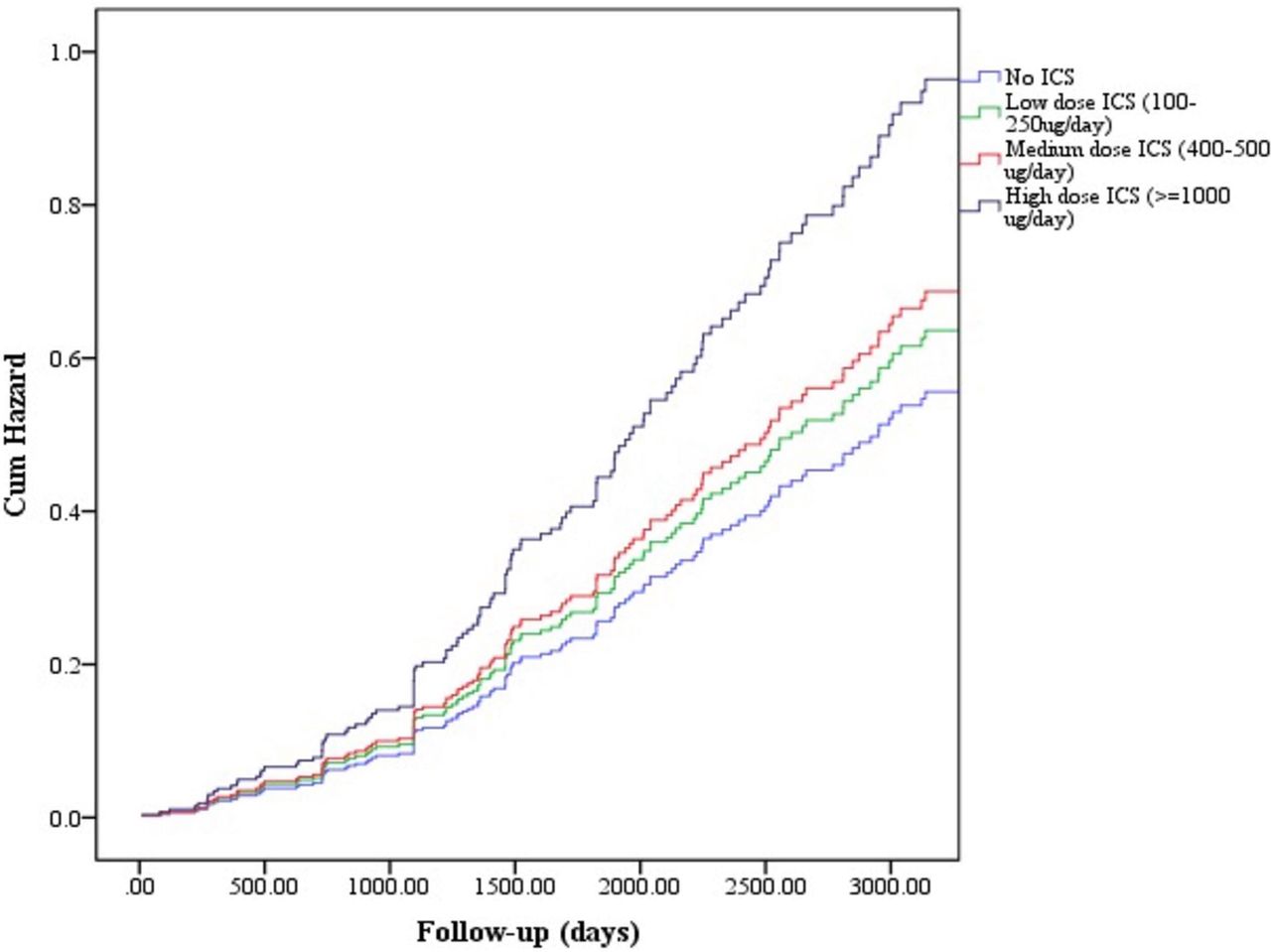
Hazard function analysis of dose of ICS and its relation to acquiring PsA infection. ICS, inhaled corticosteroids; PsA, Pseudomonas aeruginosa.
We found no statistically significant difference between COPD-PsA and COPD-non-PsA groups regarding the incidence of pneumonia (p=0.118, table 1). Further, there was no association between the use of ICS and pneumonia (p=0.858, data not shown). Moreover, BEC was not different between ICS users and non-users (270.8±318.4 vs 252.5±263.5, p=0.692).
Correlations
PsA infection positively correlated with BEC (r=0.381, p≤0.001, (online supplemental table S2) as well as ICS dose (r=0.107, p=0.042, (online supplemental table S2); but there was no correlation between PsA infection and ICS use (r= −0.008, p=0.884 online supplemental table S2). Further, there was neither correlation between BEC and ICS dose nor BEC and ICS use (p>0.05, (online supplemental table S2).
Regression and survival analysis
In the bivariate cox regression analysis, neither ICS use nor the type of ICS nor the use of systemic corticosteroids during AECOPD (>3 courses throughout follow-up duration) were independent risk factors associated to PsA infection among patients with COPD (p>0.05; online supplemental table S1); however, the dose of ICS was a statistically significant independent risk factor for PsA infection (OR 1.15, 95% CI 1.04 to 1.28, p=0.009; online supplemental table S1). Similarly, ICS use was not a risk factor for development of pneumonia (HR 1.28, 95% CI 0.83 to 1.98, p=0.270); while the dose of ICS was a significant weak risk factor for development of pneumonia (HR 1.12, 95% CI 1.0 to 1.25, p=0.043).
Moreover, the daily dose of ICS, not its use, was a significant risk factor associated to PsA infection in multivariate Cox regression analysis (HR 1.26, 95% CI 1.01 to 1.57, p=0.040, table 2) after correction for age, mMRC dyspnoea scale, the degree of airway obstruction based on GOLD classification and the use of systemic corticosteroids during AECOPD with cumulative hazard of 90% of acquiring PsA infection in case of high ICS dose (figure 1) on follow-up.
Multivariate Cox regression analysis of predictors of acquiring PSA infection
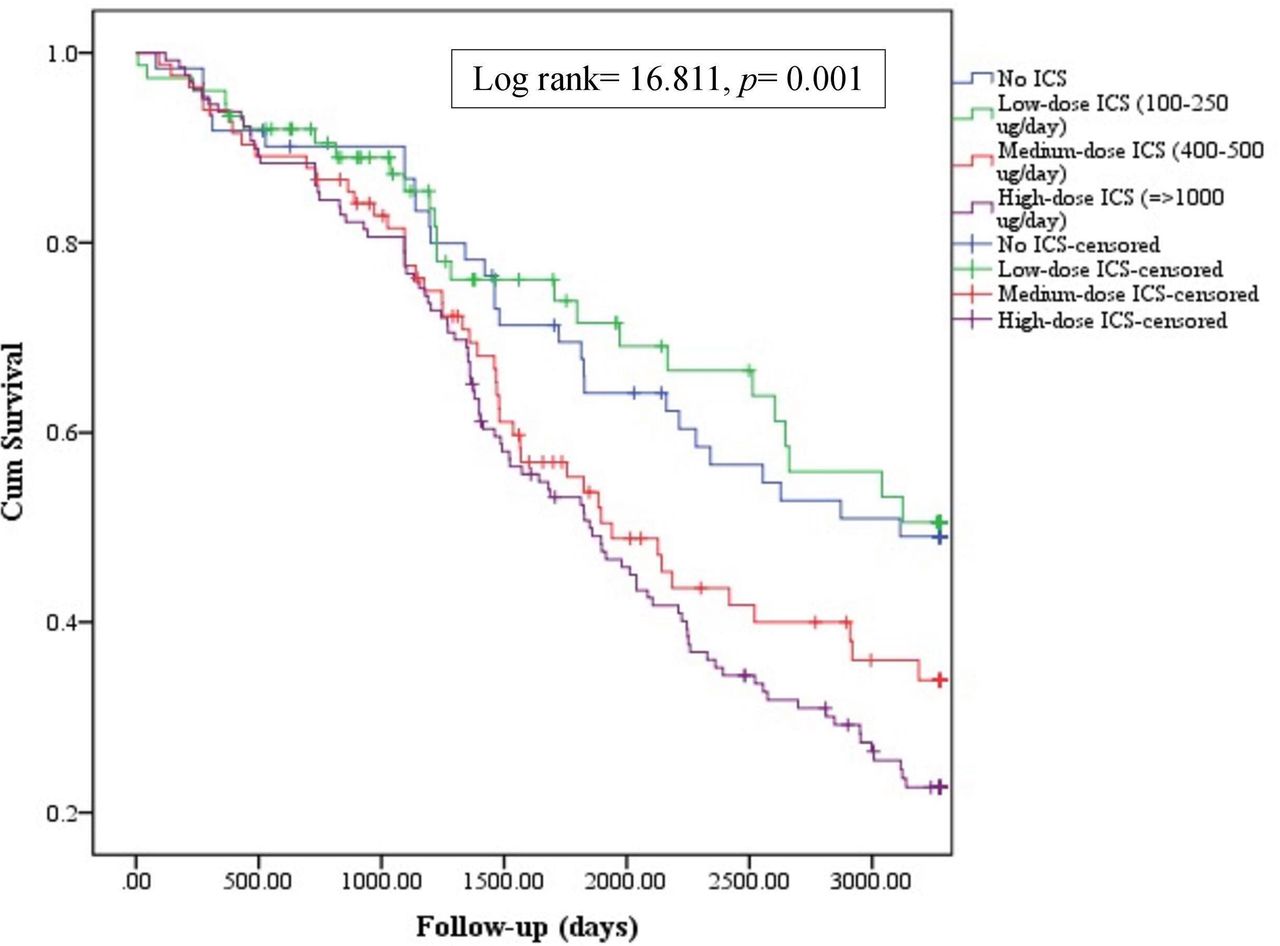
Patients with COPD using higher daily ICS dose, but not the use of ICS, were also at 1.33 hazard of mortality in multivariate cox regression analysis (95% CI 1.07 to 1.65, p=0.01, table 3) after being adjusted for age, mMRC dyspnoea scale and FEV1% predicted as a measure of airway obstruction severity. The use of ICS had a protective trend against mortality; however, it does not reach a statistical significance (HR=0.55, p=0.172, table 3). Both PsA infection and higher mMRC dyspnoea scale were additional hazard factors of mortality (p<0.05). Further, BEC ≥300 cells/uL was a protective factor against mortality (HR 0.71, 95% CI 0.52 to 0.99, p=0.04). Kaplan-Meier survival analysis showed that the high dose of ICS was associated with significant worse survival of 25% vs 50% compared with low-to-medium ICS dose users (p=0.001, figure 2).

{kind=link}
{kind=link}
Kaplan-Meier survival analysis according to the dose of ICS among the patients with COPD throughout the study (2012–2020) (log rank=16.811, p=0.001). COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids.
Multivariate Cox regression analysis of predictors of mortality among COPD population
Discussion
Severe ExCOPD are frequently infected by PsA at some point in the natural course of their disease. ExCOPD are commonly treated with ICS and we have shown that the presence of PsA in sputum is a marker of severity and mortality. In an attempt to demonstrate an association between PsA and ICS use, we show here that higher dose of ICS was an independent risk factor for PsA infection but not the use of them. Moreover, patients with continued use of high daily dose of ICS had worse survival compared with low-to-medium ICS dose. Meanwhile, the use of ICS was not associated with poorer survival, and in fact, it seemed to be a protective factor against mortality in multivariate analysis.
Previous studies
Almagro et al found that 16% of their AECOPD admissions were caused by PsA infection and that PsA infection was significantly related to posthospitalisation mortality up to 3 years.19 Similarly, Eklöf et al found that PsA was a strong independent risk factor for all causes of death during AECOPD admissions and a cause of subsequent hospitalisation on 2 years of follow-up of their patients with COPD.12 Further, Jacobs et al found that those outpatient COPD with PsA isolation had lower FEV1% predicted and were at higher risk of mortality compared with negative PsA group.20 Ni et al in their meta-analysis found that the coexistence of COPD and bronchiectasis was associated with higher rate of PsA infection.21 Martínez-García et al found that severe exacerbations and severe airway obstruction were risk factors for first PsA isolation among COPD cohort; while persistent PsA infection was related to the presence of bronchiectasis and severe persistent exacerbation as well as associated with increased mortality.22 Our results agree with these studies as our COPD population with PsA had more severe airway obstruction, more frequent exacerbations, higher mortality and higher frequency of associated bronchiectasis. We found also that PsA infection was a risk factor of mortality in multivariate analysis which could be an important factor explaining the higher mortality among our COPD-PsA population. Further, we found that low lung function as expressed by FEV1% predicted was a risk factor for acquiring PsA infection which is in accordance with Martínez-García et al.22
Interpretation of the results
Frequent antibiotic and oral corticosteroid courses used commonly in the management of AECOPD13 could cause a microbiota modification that leads to isolation of PsA.20 ICS is recommended in the management of ExCOPD,13 but some controversies are present about the prescription of ICS in stable COPD since ICS use has been linked to increased risk of pneumonia in previous studies.15 23
Interestingly, in the current analysis, we found that neither ICS use nor ICS type nor the use of systemic corticosteroids during AECOPD was a risk factor associated to PsA infection. Conversely, the use of ICS showed a protective trend against mortality in our studied ExCOPD population. Additionally, ICS use was not associated with increased risk of pneumonia; however, high dose of ICS was a weak risk factor for development of pneumonia (HR=1.12). In line with our results, Garcia-Vidal et al found that there is no relation between the use of ICS and PsA infection in their COPD cohort.8 However, ICS use was linked to increased risk of pneumonia in previous studies15 23 especially the use of fluticasone propionate compared with budesonide.24 25 Martinez-Garcia et al found that ICS increased the risk of pneumonia among patients with COPD with low BEC (<100/uL) and it was associated with chronic bronchial infection.26 We found that there was no association between the use of ICS and BEC in our severe COPD population; however, BEC ≥300 cells/uL was protective against mortality. Yang and Yang found that increased blood eosinophils is associated with decreased mortality in severe AECOPD.27
In addition, we found that high dose ICS is a strong independent risk factor for acquiring PsA infection even after adjustment to use of systemic corticosteroids as well as for mortality. This could be explained on the basis that ICS use, especially in high doses, is associated with change of local airway defence mechanisms including T-cells, alveolar macrophages and various signalling cytokines.16 28–30 Garcha et al found that airway bacterial load in stable COPD is related to higher dose of ICS use.30 Similarly, Contoli et al found that 1 year of high-dose fluticasone propionate use among stable COPD was associated with significant increase of sputum total bacterial load specially referred to Streptococcus pneumoniae and Haemophilus influenzae.16 Further, Håkansson et al found in bronchiectasis patients that PsA isolation was more frequent among those using ICS and that higher ICS dose was associated with mortality.31
Clinical implications
Our data could reinforce the concept that, by itself, the use of ICS in ExCOPD are of benefit regardless the infectious aetiology based on the improvement of their survival.
In addition, our data discourage the use of high doses of ICS in ExCOPD, since it was directly linked to increased risk of PsA infection and mortality. Current guidelines recommend the use of the lowest effective ICS dose32 33 and to consider the benefit–risk balance before initiating an ICS prescription. Previous reviews showed a relatively flat dose-response curve for ICS-clinical response and a steep dose-response for ICS-side effects.34 35 Both the Informing the Pathway of COPD Treatment (IMPACT) study36 and TRIBUTE study37 used low-medium doses of ICS and found that there was a significant reduction of moderate-to-severe AECOPD with no increased risk of pneumonia after 52 weeks of therapy. Interestingly, in line with our data, a recent study by Eklöf et al found that ICS was a risk factor for acquiring PsA infection as a dose-dependent risk compared with those not using ICS in severe COPD Danish cohort.38
Limitations
The current study has some limitations. First, we did not study the underlying mechanisms of increasing mortality among COPD-PsA population using ICS. However, increased airway inflammation caused by PsA and its high virulence in terms of biofilm formation and resistance of airway-mediated clearance mechanism could be possible mechanisms among ExCOPD patients.39–41 Second, an overlap between the airway colonisation and new airway infection could be present as we did not analyse separately those with chronic bronchial infection. However, lower airways bacterial colonisation is associated with frequent AECOPD and could modulate the characteristics of the exacerbation.42 Lastly, we used only ordinary microbiological culture rather than quantitative PCR for bacterial detection in the current study. Microbiological detection in the airways using molecular techniques could be more accurate and discriminatory30; however, it is costly and not available in all centres. To our knowledge, this is the first case–control study with longitudinal follow-up that demonstrates that not ICS use, but ICS dose is associated to PsA infection in frequent exacerbator COPD patients.
Conclusions
ICS dose could be an important risk factor for PsA infection in ExCOPD but not its use. Further, high ICS dose is an independent risk factor for mortality. Moreover, PsA infection is another important risk factor for mortality among those patients. However, further studies are still required to evaluate the relationship between ICS and PsA infection in patients ith COPD.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article and the associated supplemental material; however, the datasets were not included and are available upon reasonable request. The current study is not a clinical trial.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethical committee of Islas Baleares Ref IB 3537 /17.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HS and NT-P: acquisition of data, analysis and interpretation of the data, statistical analysis, drafting the manuscript; JV and LR-C: recruitment of the patients, acquisition of data, interpretation of the data, drafting the manuscript; AI, CL-C, CJ, PF-R and AO: sputum analysis and microbiological evaluation, data analysis, interpretation of the data, critical revision of the manuscript; BGC: conception and design of the research, analysis and interpretation of the data, supervision of the work, drafting the manuscript, critical revision of the manuscript for important intellectual content.
Funding The project was partly funded by a non-restricted grant from Menarini. HS is funded by full scholarship ID 2019/2020 from the Ministry of Higher Education of the Arab Republic of Egypt.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.