Article Text

Abstract
Background Acute exacerbation (AE) in idiopathic pulmonary fibrosis and other idiopathic interstitial pneumonias (IIPs) are poor prognostic events although they are usually treated with conventional therapy with corticosteroids and immunosuppressants. Previously, we demonstrated the safety and efficacy of recombinant human soluble thrombomodulin (rhTM) for AE-IIP in the SETUP trial. Here, we aimed to clarify the efficacy of rhTM for poor-prognosis cases of AE-IIP.
Methods In this study, we included 85 patients, in whom fibrin degradation product (FDP)/d-dimer was evaluated at AE, from the 100 patients in the SETUP trial. The AE-IIP patients in the rhTM arm (n=39) were diagnosed using the Japanese criteria from 2014 to 2016 and treated with intravenous rhTM for 6 days in addition to the conventional therapy. The AE-IIP patients in the control arm (n=46) were treated with the conventional therapy without rhTM between 2011 and 2013. The subjects were classified into higher and lower FDP/d-dimer groups based on the Japanese Association for Acute Medicine Disseminated Intravascular Coagulation scoring system. A multivariate Cox proportional hazard regression analysis with stepwise selection was performed to reveal the prognostic factors of AE-IIP.
Results We developed a prognostic scoring system using two significant prognostic factors, higher FDP/d-dimer at AE and prednisolone therapy before AE, with 3 and 2 points assigned for each parameter, respectively. The prognostic scores ranged from 0 to 5. Survival of AE-IIP patients with a prognostic score=0 was significantly better than that of patients with score ≥2. Survival was improved with the rhTM therapy (p<0.05) in the poor prognostic cases (score ≥2), but not in the good prognostic cases (score=0).
Conclusions Treatment with rhTM might improve survival in AE-IIP cases with poor prognoses.
Trial registration number
UMIN000014969, date: 28 August 2014.
- interstitial fibrosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Efficacy of recombinant human soluble thrombomodulin (rhTM) for acute exacerbation (AE) of idiopathic pulmonary fibrosis (IPF) (AE-IPF) was previously reported and we have also reported efficacy of rhTM on AE of idiopathic interstitial pneumonia (IIP) (AE-IIP).
rhTM improved survival of poor prognostic patients of AE-IIP.
rhTM might be recommended for poor prognostic AE-IIP patients and future studies for efficacy of rhTM on AE-IPF and AE-IIP had better be examined considering the severity of AE-IPF and AE-IIP patients.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a lung disease with unknown aetiology and a poor prognosis. Some patients with IPF experience a rapid deterioration resulting in unpredictable death;1–5 such an acute deterioration with unknown aetiology is called acute exacerbation (AE) of IPF (AE-IPF). Acute exacerbation is the most common cause of death in IPF;6 therefore early diagnosis and proper management of AE-IPF are urgently required. AE is reported to occur in idiopathic interstitial pneumonias (IIPs) other than IPF (non-IPF).7–9 In addition, prognosis of AE of unclassifiable IIPs and interstitial lung diseases (ILDs), besides IIPs, is similarly poor to that of IPF.9 10 Therefore, AE of progressive fibrosing ILDs should be examined for appropriate management,10 which can lead to a better survival rate of patients.
In the 2011 American Thoracic Society (ATS)/European Respiratory Society (ERS)/Japanese Respiratory Society (JRS)/Latin American Thoracic Association (ALAT) guidelines for the diagnosis and management of IPF,1 treatment with corticosteroids was weakly recommended for AE-IPF. For some cases of AE-IPF, immunosuppressants have also been administered, based on the results of small-scale studies.11–13 As an additional treatment, direct haemoperfusion with polymyxin B-immobilised fibre column (PMX-DHP) therapy14 was introduced to treat AE-IPF according to the findings of previous studies.15 16
The pathophysiology of AE-IPF is unknown; however, several recent studies have suggested the importance of disordered coagulation and fibrinolysis in AE-IPF.5 The survival advantage with low molecular weight heparin treatment17 supposedly validates this importance. Thrombomodulin (TM), a transmembrane glycoprotein expressed on the surface of endothelial cells, is another key regulator of coagulation.18 Thrombomodulin also inhibits inflammation by suppressing neutrophil adhesion to the endothelium, decreasing the expression of adhesion molecules and enhancing the barrier function of endothelium and degradation of high-mobility group box 1.18
Recently, recombinant human soluble TM, (rhTM; Recomodulin, Asahi Kasei Pharma Corporation, Tokyo, Japan) composed of only the extracellular domain of TM, was developed and approved for the treatment of disseminated intravascular coagulation (DIC).19 20 Its effectiveness only for AE-IPF has been reported by several studies.21–25 We recently reported the efficacy of rhTM for AE-IIP including AE-IPF in a prospective multicentre, single-arm, open-labelled trial by propensity score analysis (SETUP trial).26 Previous studies21–26 have demonstrated the efficacy of rhTM for AE-IPF or AE-IIP; however, whether rhTM can improve the survival of patients with severe AE-IPF or AE-IIP and poor prognosis remains unknown. Hence, we performed a retrospective analysis using the SETUP trial data set to answer this question. We also assessed the coagulation marker, fibrin degradation product (FDP)/d-dimer, as a predictor of survival of patients with AE-IIP.
Materials and methods
Subjects
We performed a retrospective analysis of subjects from the SETUP trial,26 a recent prospective study. The inclusion and exclusion criteria of patients in the SETUP trial were as previously described.26 Briefly, AE-IIP patients diagnosed according to the modified JRS diagnostic criteria26 and provided written informed consent were prospectively enrolled and treated with rhTM and conventional therapy from 2014 to 2016. AE-IIP patients treated with conventional therapy without rhTM from 2011 to 2013 were retrospectively registered consecutively. AE-IIP patients with severe non-pulmonary diseases, life-threatening bleeding, a clinically significant infection, actual or possible pregnancy, a history of hypersensitivity to rhTM, cerebrovascular disorders within the past year and surgery within the past month were excluded. All patients were centrally assessed and some were excluded from the data set used for analysis. AE-IIP patients prospectively treated with rhTM and conventional therapy (rhTM arm, n=39) and retrospectively registered AE-IIP patients treated without rhTM before enrolment in the rhTM arm (control arm, n=61) were included in the SETUP trial to evaluate the efficacy and safety of rhTM.26 To evaluate the importance of a coagulation marker, 15 AE-IIP patients, in whom the FDP/d-dimer was not evaluated, were excluded from the study (online supplementary figure 1).
Supplemental material
This study was registered with the University Hospital Medical Information Network Center.
Methods
Diagnosis of underlying IIPs and AE-IIPs
The diagnosis of underlying IPF was based on criteria from the ATS/ERS/JRS/ALAT guidelines for the diagnosis and management of IPF.1 The diagnosis of IIP was based on the ATS/ERS/JRS statement,27 and IIP that could not be diagnosed as IPF was classified as non-IPF. Non-IPF IIP cases did not undergo surgical lung biopsy and all non-IPF cases were diagnosed to have unclassifiable IIPs and did not include pathologically diagnosed non-specific interstitial pneumonia, desquamative interstitial pneumonia or clinically diagnosed organising pneumonia.
AE-IIPs were diagnosed based on the following modified JRS diagnostic criteria for AE-IPF.28 (1) Within 1 month, the following three conditions should be satisfied: (i) progressively worsening dyspnoea; (ii) new ground-glass opacities evident in high-resolution CT (HRCT) scans superimposed over background reticular opacity, traction bronchiectasis, traction bronchiolectasis or honeycombing and (iii) a reduction in resting partial pressure of oxygen in arterial blood (PaO2) of more than 10 mm Hg compared with previous measurements. (2) Apparent causes of acutely impaired respiratory functions, such as infection, pneumothorax, cancer, pulmonary embolism and congestive cardiac failure should be excluded. However, AE triggered by infection5 cannot be excluded entirely, and possibly included in this study, because bronchoalveolar lavage could not be performed in all cases to exclude infection.
Administration of rhTM
Administration of rhTM, at 380 U/kg/day for 6 days, as approved for DIC treatment,20 was commenced on the day of AE-IIP diagnosis in the hospital.
Conventional treatment for AE-IIPs
Conventional treatments for AE-IIP were started according to the decision of each institute in hospital. Briefly, AE-IIPs in both the rhTM and control arms were treated with prednisolone with/without an immunosuppressant after the intravenous administration of high-dose methylprednisolone for three successive days. Tapering of prednisolone dose was usually started in the hospital; however, prednisolone administration was continued in the outpatient department in the same hospital and was not stopped until Day 91. PMX-DHP therapy15 16 was performed using the PMX-DHP column, Toraymyxin (Toray Medical, Tokyo, Japan), which was attached for 4 to 6 hours at a flow rate of 80 mL/min and was repeated once within 48 hours. Nafamostat mesilate (Torii Pharma, Tokyo, Japan) was used to reduce intracatheter coagulation. Anticoagulants and antiplatelet drugs were used to treat comorbidities. Invasive positive pressure ventilation, non-invasive positive pressure ventilation or nasal high flow was introduced to maintain oxygenation in some cases with severe respiratory failure.
Evaluation of AE-IIPs
AE-IIPs were evaluated before and at the onset of AE. Briefly, the severity of IIP (stages I-IV, mildest to most severe) in a stable state was evaluated according to the JRS criteria. This was done using PaO2 at rest and arterial oxygen saturation of pulse oximetry (SpO2) in room air during a 6 min walk test:28 stage 1, PaO2 at rest ≥80 mm Hg; stage 2, PaO2 at rest ≥70 mm Hg and <80 mm Hg; stage 3, PaO2 at rest ≥60 mm Hg and <70 mm Hg and stage 4, PaO2 at rest <60 mm Hg. Patients with stage 2 or 3 were re-classified into stage 3 or 4, respectively, if SpO2 during the 6 min walk test was less than 90%. The severity of most of the subjects was evaluated within 6 months before the onset of AE-IIP. Shortness of breath before AE was evaluated according to a modified Medical Research Council (mMRC) score.29 DIC was diagnosed based on the Japanese Association for Acute Medicine DIC scoring system,30 at AE-IIPs diagnosis. FDP/d-dimer was also evaluated based on the DIC scoring system: score 0, FDP <10 mg/L; score 1, 10 mg/L≤ FDP <25 mg/L; score 3, FDP >25 mg/L. Survival of AE-IIP patients in control arm with the FDP scores of 1 and 3 was similar and significantly worse than that of patients with FDP score 0 (log-rank test, p<0.001 and p=0.039, respectively) (online supplementary figure 2). Hence, FDP was classified into higher (≥10 mg/L) and lower (<10 mg/dL). According to the criteria of Akira et al31 after an independent classification by a pulmonary radiologist (MA) and a pulmonary physician (TA), the HRCT pattern at the diagnosis of AE-IIPs was classified into one of the following three patterns: peripheral, multifocal and diffuse. HRCT patterns were then classified as a diffuse or non-diffuse pattern. Oxygenation at AE was evaluated using the PaO2/fraction of inspired oxygen (FiO2) ratio, and severely disturbed oxygenation cases were defined to have a PaO2/FiO2 ratio of ≤200.32 Serum levels of Krebs von den Lungen-6 (KL-6) were measured using a commercial ELISA kit (Eisai, Tokyo, Japan). The cut-off level of KL-6 was 500 U/mL.33
Supplemental material
Safety and causes of death
The subjects in the rhTM arm were the same as those in the SETUP trial. Information about safety and causes of death of the 100 subjects of the SETUP trial, reviewed by a safety committee, has already been reported.26 Safety and causes of death were compared between cases of poor and good prognostic stages in rhTM arm.
Statistical analysis
All analyses were based on the intention-to-treat principle. Continuous and categorical data are presented as medians (range) and values (percentages), and they were compared between the rhTM and control arms using the Wilcoxon rank-sum and Fisher's exact tests, respectively. Ninety-day survival was estimated using the Kaplan-Meier method and compared using a log-rank test.
A multivariate Cox proportional hazard regression analysis with stepwise selection was performed automatically using statistical software according to its algorithm to predict the survival of patients with AE-IIP in the control arm. A scoring system for prognostication was developed. Points for each parameter were determined according to the β coefficients of the multivariate Cox proportional hazard regression analyses. The ratio of β coefficients of each parameter was converted to a ratio of suitable integral values. We defined the integral values as points of each parameter. Total points were defined as prognostic scores for each case. The cut-off values for the prognostic scores for 90-day survival were determined using receiver operation characteristics (ROC) curve analysis. AE-IIP cases with high/low prognostic scores were defined as poor/good prognostic cases. The survival of AE-IIPs patients with high/low points for each parameter and with high/low overall prognostic scores was compared using a log-rank test.
All reported p values are two-sided, and the results with p<0.05 were considered statistically significant. Statistical analyses were performed using SPSS, V.24 (IBM, Armonk, New York, USA).
Results
Patient demographics
Among the 85 patients with AE-IIP, there were 34 patients with of IPF and 51 patients with non-IPF. The survival of AE-IPF patients was similar to that of AE-non-IPF patients (p=0.691, log-rank test). There were no significant differences in clinical parameters, treatment for IIP itself at the stable state before AE diagnosis, or parameters at AE diagnosis between the rhTM and control arms (table 1). The management of AE-IIPs was similar in both arms (table 2). The frequency of immunosuppressant use for AE-IPF (6 out of 34 cases) was similar to that for AE-non-IPF (15 out of 51 cases) (p=0.306, Fisher’s exact test). Patient survival in the rhTM arm tended to be better (figure 1)(p=0.062, log-rank test).
Patient demographics
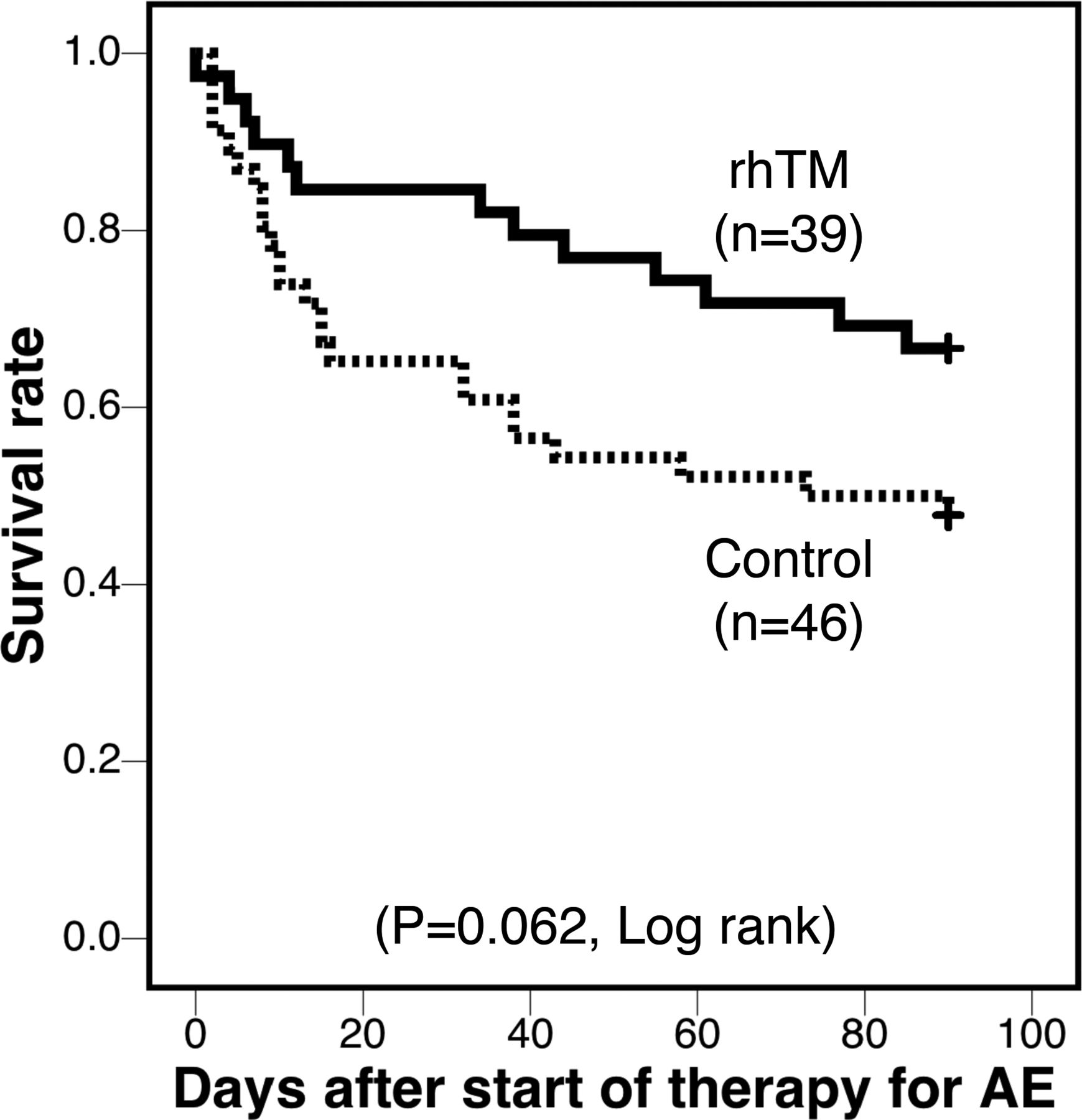
Survival curves after the start of therapy for AE were assessed by the Kaplan-Meier method. The rhTM arm (sold line, n=39) showed a tendency towards improved 90-day survival compared with the control arm (dotted line, n=46; p=0.062, log-rank test). The 90-day survival rate was 66.7% (26/39) for the rhTM arm and 47.8% (22/46) for the control arm. Except in the case of death, all patients underwent follow-up until Day 91. AE, acute exacerbation; rhTM, recombinant human soluble thrombomodulin.
Therapy for AE-IIPs and management of respiratory failure
The frequency or median (range) is presented for each parameter.
The frequency or median of each parameter was compared between the two groups using the Wilcoxon rank-sum test or Fisher’s exact test, respectively.
Duration from the last evaluation of disease severity to AE was >180 days in nine patients of the control arm and six patients of the rhTM arm (p=0.78)
The maximum follow-up periods were 90 days for both groups. Follow-up periods for all alive patients were 90 days.
Higher FDP is 10 mg/L≤FDP, and lower FDP is <10 mg/L as described in the methodology.
Prognostic factors of AE-IIPs in control arm determined using the univariate COX proportional hazard regression analysis
The univariate Cox analysis revealed that prednisolone therapy before AE, higher FDP/d-dimer and PaO2/FiO2 ratio of ≤200 at AE diagnosis were significant prognostic factors suggesting a poor prognosis (table 3).
Univariate Cox proportional hazards regression analysis for the survival of AE-IIP patients after the onset of acute exacerbation in the control arm
Stepwise selection of parameters for prognostic scoring of the control arm
To predict the survival of AE-IIP patients in the control arm, the multivariate Cox proportional hazard regression analysis with stepwise selection was performed. Prednisolone before AE and FDP/d-dimer at AE diagnosis were significant poor prognostic factors (table 4A). rhTM therapy was a significant predictor of better survival of AE-IIP patients after adjustment with the two prognostic factors using the Cox proportional hazard regression analysis (HR; 2.700, 95% CI; 1.398 to 5.215, p=0.003) (data not shown).
Prognosis scoring model to predict the survival of AE-IIP patients in the control arm
Association between selected parameters and other parameters in the control arm
Prednisolone before AE was associated with mMRC, disease severity of IIP and long-term oxygen therapy (LTOT) before AE. This suggested that there was respiratory dysfunction in IIP patients before AE (table 5). FDP/D-dimer was associated with the PaO2/FiO2 ratio at AE diagnosis of AE, suggesting AE-IIP disease severity (table 5).
Patient demographics in the control arm for prednisolone-treated patients at the stable state and FDP/d-dimer at the AE diagnosis
The frequency or median (range) is presented for each parameter.
The frequency or median of each parameter was compared between the two groups by Wilcoxon rank-sum test or Fisher’s exact test, respectively.
Higher FDP is 10 mg/L≤FDP and lower FDP is <10 mg/L as described in the methodology.
Effect of rhTM on the survival of AE-IIP patients with a better and worse prognosis, as evaluated using a single parameter
The survival of AE-IIP patients treated with/without rhTM was compared in patients with a better and worse prognosis. The AE-IIP patients treated with prednisolone before AE (n=32) showed significantly worse survival than those without prednisolone before AE (n=53)(p=0.008, log-rank test, data not shown). The survival of AE-IIP patients with lower FDP/d-dimer levels (n=60) was better than those with higher FDP/d-dimer levels (n=25)(p<0.001, log-rank test, data not shown). rhTM did not significantly improve the survival of AE-IIP patients with a higher FDP/d-dimer at AE diagnosis (p=0.084, log-rank test; online supplementary figure 3a) nor those treated with prednisolone before AE (p=0.074, log-rank test; online supplementary figure 3c). rhTM did not significantly improve the survival of AE-IIP patients with lower FDP/d-dimer at AE diagnosis (p=0.267, log-rank test; online supplementary figure 3b) nor those treated without prednisolone before AE (p=0.288, log-rank test; online supplementary figure 3d).
Supplemental material
Prognostic scoring and survival of AE-IIP patients
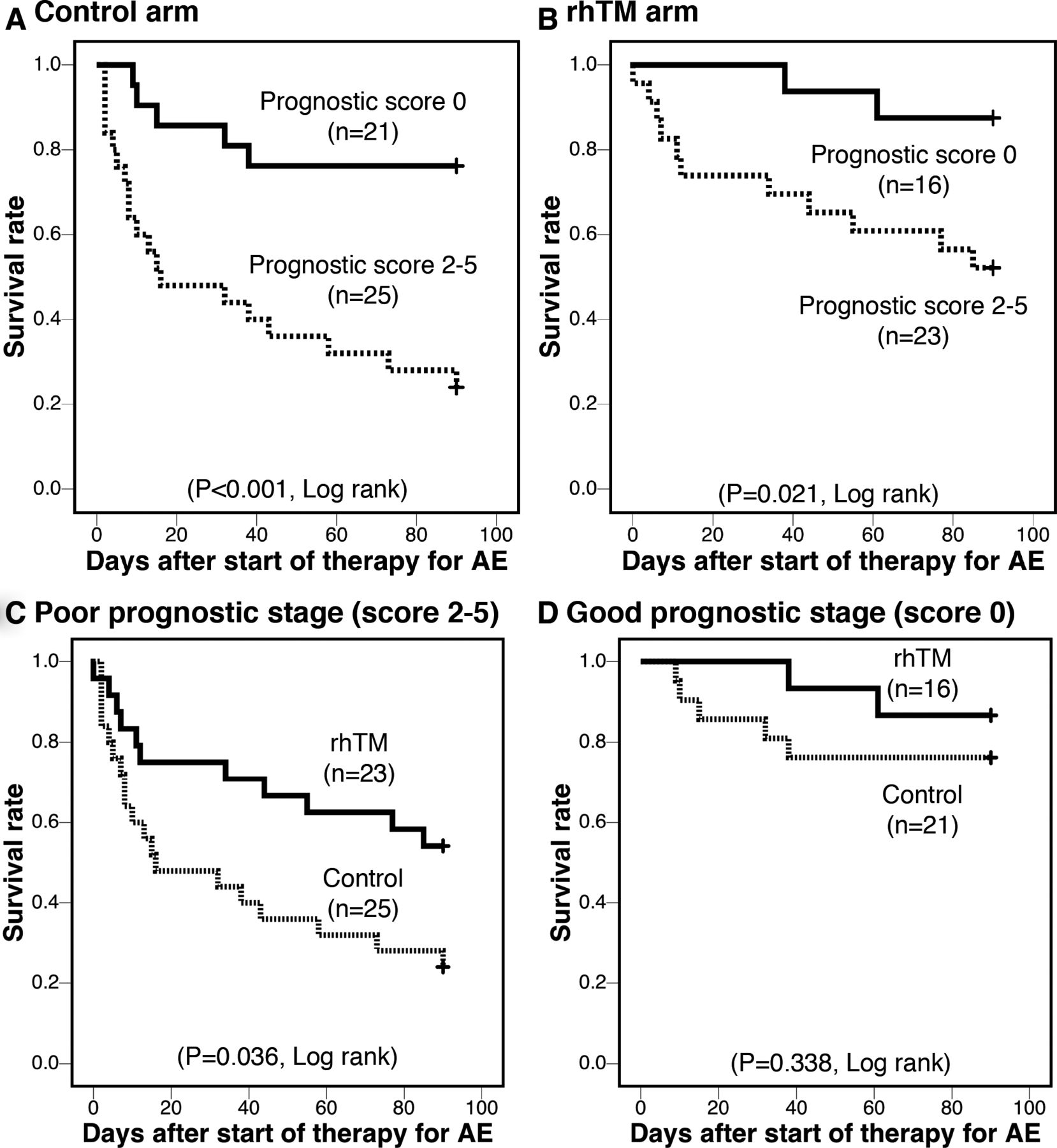
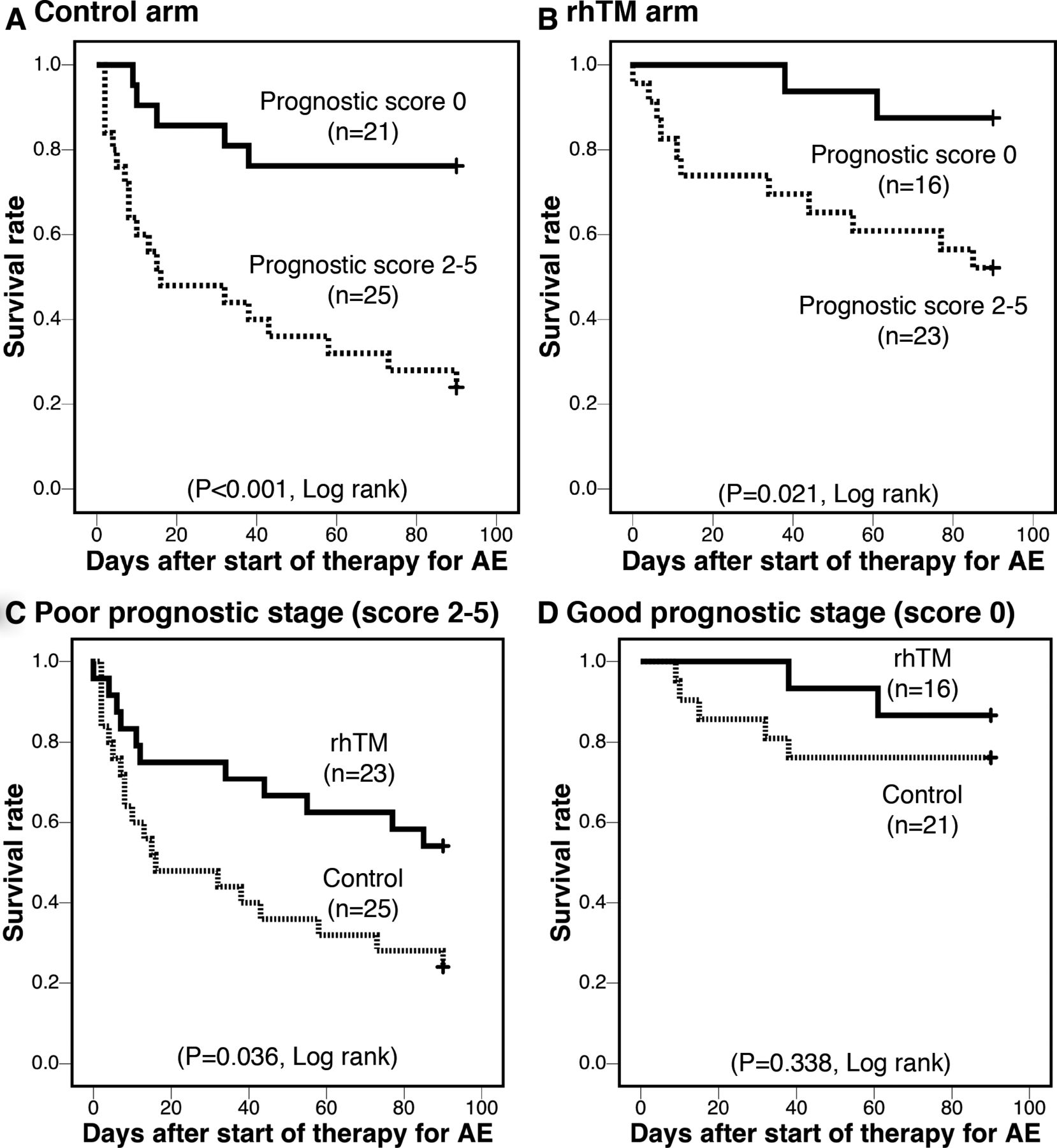
Prognostic scoring was performed as shown in table 4B. The prognostic score was composed of FDP/d-dimer at AE diagnosis and prednisolone therapy before AE, which were significant survival predictors, based on the multivariate Cox proportional hazard regression analysis (table 4A) and according to the ß coefficients of these two parameters (table 4A). The parameters were determined to contribute 3 points and 2 points, respectively (table 4B). The prognostic scores of the control arm were as follows: 0 (n=21), 2 (n=11), 3 (n=8) and 5 (n=6). The 90-day survival rates were 76.2%, 36.3%, 25% and 0%, respectively.The ROC analysis revealed that a cut-off prognostic score of 2 enabled prediction of the 90-day survival of AE-IIP patients in the control arm. The survival of AE-IIP patients in the control arm with a prognostic score of 0 (n=21, good prognosis stage, 90-day survival: 76.2%) was better than those with a prognostic score of 2, 3 or 5 (n=25, poor prognosis stage, 90-day survival: 24.0%) (p<0.001, log-rank test; figure 2A). The survival of AE-IIP patients in the rhTM arm with a good prognostic stage was also better than those with a poor prognostic stage (p=0.021, log-rank test; figure 2B).
{kind=link}
{kind=link}
Ninety-day survival of AE-IIP patients with a prognostic score of 0 (good prognostic stage, solid lines) and prognostic scores of 2 to 5 (poor prognostic stage, dotted lines) was compared using the Kaplan-Meier method ((A) control arm and (B) rhTM arm). The survival of AE-IIP patients with a good prognostic stage was better than that of patients with poor prognostic stage in both control arm (A) (p<0.001, log-rank test) and rhTM arm (B) (p=0.021, log-rank test). Survival of the AE-IIP patients with the poor prognostic stage (prognostic score 2 to 5) in rhTM arm (solid line, n=23) was better than that of patients in the control arm (dotted line, n=25) (log-rank test, p=0.036) (C). However, the survival of the AE-IIP patients with the good prognostic stage in the rhTM arm (solid line, n=16) was similar to that of patients in the control arm (dotted line, n=21) (log-rank test, p=0.338) (D). AE,acute exacerbation; rhTM, recombinant human soluble thrombomodulin; IIP,idiopathic interstitial pneumonia.
Effect of rhTM on the survival of poor prognostic AE-IIP patients evaluated using the prognostic score
rhTM therapy significantly improved the survival of AE-IIP patients with the poor prognostic stage (p=0.036, log-rank test; figure 2C); however, the survival of AE-IIP patients evaluated to have a good prognosis according to the prognostic score was not significantly improved by rhTMtherapy (p=0.338, log-rank test; figure 2D).
Safety and causes of death in rhTM arm
Bleeding was observed only in the rhTM arm (n=2) and both patients were in the poor prognostic stage; however, its frequency was statistically similar in the poor and good prognostic stages (online supplementary table 1, p=0.503, Fisher’s exact test). The frequency of all adverse events in the poor prognostic stage (five events/23 patients) was not significantly different from that in good prognostic stage (two events/16 patients) (online supplementary table 1, p=0.678, Fisher’s exact test). Causes of death in the rhTM arm included infection (n=1), unspecified vascular event (n=1, dissection of aorta was suspected) and AE (n=11). The autopsy was not performed in any of the dead patients (online supplementary table 1).
Supplemental material
Discussion
In the present study, we showed that the conventional therapy with rhTM improved the survival of AE-IIP patients with a poor prognosis, as predicted by the scoring system developed based on prednisolone therapy before AE and FDP/d-dimer at AE onset. To the best of our knowledge, this is the first study to show the possibility that rhTM improves outcomes in poor-prognostic patients with AE-IIP. Besides, the multivariate Cox proportional hazard regression analysis revealed that rhTM improved the survival of AE-IIPs patients, in whom FDP/d-dimer was evaluated, although the univariate analysis did not show a significant improvement. The results of this study are consistent with those of the SETUP trial,26 although statistical methods employed in the two studies were different.
Kataoka et al22 and Sakamoto et al21 reported a survival advantage with rhTM treatment. However, the efficacy of rhTM for poor prognostic AE-IIP patients has not been evaluated. In the SETUP trial,26 we clarified the efficacy of rhTM for AE-IIPs using the propensity score analysis with various possible parameters that may reflect prognosis. With this method, we could not classify all the cases into two groups. Thus, we developed the prognostic score using the factors selected by the multivariate Cox proportional hazard regression analysis.
Prednisolone administration before AE is a significant predictor of AE34 and it may be associated with a poor prognosis after AE. Here, we showed it to be a useful predictor of poor prognosis. It is hypothesised that infection, one of the most important triggering factors of AE in IPF, occurs more often in prednisolone-treated patients. Bacterial ribosomal RNA copy numbers in the broncheoalveolar lavage fluid were elevated in AE-IPF cases at the onset of AE compared with stable IPF patients.35 An increase in the microbiome has been reported to be associated with disease progression in IPF,36 and it may lead to a rapid progression after the occurrence of AE. However,the frequency of steroid-treated cases was similar in stable IPF and AE-IPF groups in the former study35 and only several steroid-treated IPF cases were included in the latter study.36 These studies cannot directly reveal a pathophysiological link between steroids and AE, although infection might cause AE in IPF patients. In our study, prednisolone administered before AE was associated with LTOT, the disease severity of IIP and mMRC before AE, suggesting the severity of IIP before the onset of AE. Hence, disease severity at a stable state, rather than prednisolone administered before AE might be associated with the occurrence of AE. However, the PANTHER study,37 which was conducted to evaluate triple therapy, comprising prednisolone, azathioprine and N-acetylcysteine, clarified the adverse effects of immunosuppressive therapy on IPF and poor prognostic significance of prednisolone before AE onset on AE-IPF cannot be neglected. Prednisolone before AE was not associated with underlying IIPs, IPF or non-IPF in patients in the control and rhTM arms (online supplementary table 2). Hence, we suppose prednisolone before AE did not reflect pathophysiological difference of AE-IPF and AE-non-IPF IIP.
Supplemental material
Serum FDP/d-dimer21 at AE diagnosis has been shown to be elevated. Yamazaki et al38 reported the prognostic significance of FDP/d-dimer in patients with AE of IPF and non-IPF IIP. Our study also revealed that FDP/d-dimer is a significant prognostic factor in AE-IIP patients treated without rhTM. Sakamoto and Kataoka reported the efficacy of rhTM for AE-IPF, similarly to the findings of our study; however, FDP/d-dimer was not a significant prognostic factor for all AE-IPF treated with/without rhTM.21 22 This result does not negate the prognostic significance of serum FDP/d-dimer. Sakamoto reported that rhTM decreased FDP/d-dimer at 14 days after AE treatment in AE-IPF patients, although the conventional therapy did not reduce it without rhTM.21 If rhTM improved the survival of AE-IPF patients by reducing blood FDP/d-dimer levels, AE-IPF patients with higher FDP/d-dimer at AE diagnosis might survive longer after rhTM therapy, and FDP/d-dimer might no longer be a significant prognostic factor.
A validated severity grading system for AE-IPF and AE-IIP is not present. Kishaba et al also created a grading system for the severity of AE-IIPs using the following factors: KL-6, LDH, PaO2/FiO2 ratio, the extent of ground-glass opacity and consolidation on HRCT.39 All parameters included in this scheme were evaluated at the time of AE diagnosis and the system was not validated in other cohorts in their study. AE-IIPs patients treated with rhTM with a good prognostic stage (score 0) survived significantly longer than those with a poor prognostic stage (score 2 to 5) (p=0.021, log-rank test; figure 2b). Hence, our prognostic scoring system developed using data of the control arm was also useful for the rhTM arm, validating our prognostic scoring system. Besides, as mentioned earlier, parameters before AE suggesting disease severity at the stable state are also important predictors that should be included in the prognostic scoring system.
Our study permitted the usage of anticoagulants and antiplatelet drugs for the treatment of comorbidities. Adverse events of bleeding did not increase even with the use of these drugs, because the two patients complicated with bleeding in the rhTM arm did not take anticoagulants or antiplatelet drugs. Treatment with these two drugs was not a significant prognostic factor of AE-IIPs (table 3). Hence, efficacy of rhTM on AE-IIPs might have been caused by not only inhibition of micro-coagulation, but also anti-inflammatory and anti-apoptotic effects.18
This study had some limitations. First, this analysis was performed retrospectively using data obtained from a limited number of patients from a non-randomised trial. Second, patient characteristics and management of AE-IIPs between the control and rhTM arms might have been different due to the difference in enrolment periods between the two arms although there was no difference as shown in tables 1 and 2. Third, the prognostic score that we used in this study cannot be used in subsequent studies. In our investigation, 14 of the 34 patients with AE-IPF were treated with prednisolone before the diagnosis of AE; however, corticosteroids were not recommended by the treatment guidelines for IPF.1 In the future, AE-IPF patients might be treated with corticosteroids before AE onset less frequently than those in our study and we might not be able to use our prognostication system in the future. Thus, the system should be modified using a parameter corresponding to the disease severity of IIPs before the onset of AE, instead of prednisolone therapy, for future studies of AE-IIPs.
Conclusions
We conclude that treatment with rhTM might improve survival in AE-IIP patients with poor prognoses.
References
Footnotes
Contributors TA contributed to study conception and design, radiological findings, data analysis and interpretation and manuscript preparation and review. HK, YO, SM, HM, IG, SY, CS and KT contributed to study conception and design, data acquisition, data analysis and interpretation and manuscript review. MM contributed to study conception and design, data analysis and interpretation and manuscript review. MA contributed to the radiological findings, and manuscript preparation and review. YI, the corresponding author, contributed to study conception and design, data analysis and interpretation and manuscript preparation and review. All authors approved the final version of the manuscript.
Funding This study was partially supported by a grant from the National Hospital Organization (H28-NHO (Kokyu)-2) awarded to TA and YI, and AMED: DLD/14526278 and PAP/14526182 awarded to YI and YI and TA, respectively.
Competing interests YI is an advisor of Boehringer Ingelheim, Shionogi Co Ltd and Asahi Kasei. TA received lecture fees from Boehringer Ingelheim and Shionogi Co Ltd for the activities outside the submitted works.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was approved by the Institutional Review Board of the Kinki-Chuo Chest Medical Center (KCCMC; approval number: 447, February 24, 2014), as well as the review boards of the other institutions. Written informed consent was obtained from all participants in the rhTM arm.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. The data that support the findings of this study have not been made available because this study was approved in 2014 and data sharing was not included in the design of this study.