Article Text

Abstract
Background and objectives Pneumonia is associated with significant mortality and morbidity in older adults. We investigated changes in functional status over 6 months after pneumonia hospitalisation by frailty status.
Methods and measurements This single-centre prospective cohort study enrolled 201 patients (mean age 79.4, 37.3% women) who were hospitalised with pneumonia. A deficit-accumulation frailty index (range: 0–1; robust <0.15, pre-frail 0.15–0.24, mild-to-moderately frail 0.25–0.44, severely frail ≥0.45) was calculated on admission. Functional status, defined as self-reported ability to perform 21 activities and physical tasks independently, was measured by telephone at 1, 3 and 6 months after discharge. Group-based trajectory model was used to identify functional trajectories. We examined the probability of each trajectory based on frailty levels.
Results On admission, 51 (25.4%) were robust, 43 (21.4%) pre-frail, 40 (20.0%) mild-to-moderately frail and 67 (33.3%) severely frail patients. Four trajectories were identified: excellent (14.4%), good (25.4%), poor (28.9%) and very poor (31.3%). The trajectory was more strongly correlated with frailty level on admission than pneumonia severity. The most common trajectory was excellent trajectory (59.9%) in robust patients, good trajectory (74.4%) in pre-frail patients, poor trajectory (85.0%) in mild-to-moderately frail patients and very poor trajectory (89.6%) in severely frail patients. The risk of poor or very poor trajectory from robust to severely frail patients was 11.8%, 25.6%, 92.5% and 100%, respectively.
Conclusions Frailty was a strong determinant of lack of functional recovery over 6 months after pneumonia hospitalisation in older adults. Our results call for hospital-based and post-acute care interventions for frail patients.
- Pneumonia
- Clinical Epidemiology
Data availability statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Frailty, a vulnerable state of decrease in physiological reserve, is commonly calculated by deficit-accumulation frailty index.
WHAT THIS STUDY ADDS
In this prospective cohort study over 6 months of follow-up, we found that frailty status on admission is a strong determinant of post-hospitalisation functional status trajectory, independently of pneumonia severity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Early recognition of frailty at admission may help clinicians to develop appropriate care plans for anticipatory discharge and post-acute rehabilitation after an acute hospitalisation due to pneumonia.
Introduction
Frailty, which is a clinical state of reduced physiological reserve, has become a significant public health problem due to the rapidly ageing population worldwide.1–3 Patients with frailty are vulnerable to adverse health consequences of acute hospitalisation, including hospitalisation-associated disability.3 4 Pneumonia is one of the most common and life-threatening infectious diseases,5–9 which affects 5.6 million in the USA and 75 million in Asia-Pacific region every year.10–12 In 2015, it was responsible for 6.8 million hospitalisations and 1.1 million in-hospital deaths worldwide.13 Previous research that investigated health outcomes of pneumonia in older adults with frailty is limited to short-term ‘hard’ outcomes (eg, death and readmission). Kundi et al reported that frail older adults had a higher risk of 30-day mortality and readmission after pneumonia hospitalisation.14 In this study, frailty was measured using the administrative claims-based Hospital Frailty Risk Score, rather than a clinical frailty measure, and functional outcomes were not studied. In a prospective cohort study, we previously reported that, regardless of the pneumonia severity, the rates of death or functional decline at 30 days post-discharge increased by fivefolds for older patients with severe frailty compared with robust patients.15 In the present study, we report 6-month follow-up data to describe the epidemiology of frailty and hospitalisation-associated disability in older patients hospitalised for pneumonia. We hypothesised that frailty would be associated with clinically meaningful trajectories of functional status change after pneumonia hospitalisation.
Methods
Study design and participants
We screened 292 patients ≥65 years of age who were admitted to a university hospital in Korea with the suspected diagnosis of pneumonia between October 2019 and September 2020. After excluding a total of 91 patients (1) who declined to participate (n=58); (2) informed consent could not be obtained from the patient or his/her proxy (n=28); and (3) whose diagnosis changed after admission (n=5), we enrolled 201 patients. The diagnosis of pneumonia was made based on symptoms, such as fever, cough, sputum and dyspnoea, with abnormal chest radiograph results. Patients who were diagnosed with COVID-19 were transferred to hospitals designated by the government. Patient and public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Baseline assessment
Study clinicians (CMP, WK, ESL) obtained sociodemographic characteristics, medical comorbidities, functional status, cognitive function, social support, admission source (nursing home vs home), vital signs, body mass index and laboratory test results (serum albumin) on admission. Functional status was assessed using a questionnaire that asked abilities to perform the following 21 daily activities and physical tasks without another person’s help 30 days prior to admission: seven activities of daily living (ADL: feeding, dressing, grooming, ambulating, transferring, bathing and toileting), seven instrumental activities of daily living (IADL: doing housework, making telephone calls, using transportation or driving, shopping, cooking, taking medications and managing money) and seven activities in the Nagi and Rosow–Breslau scales (pulling or pushing a large object, lifting 5 kg, walking up and down a flight of stairs, walking 1 km, writing or handling small objects, reaching arms above shoulder and stooping, crouching or keeling).16 17 Cognitive function was assessed using Mini-Mental State Examination (MMSE) and AD8 (Dementia Screening Interview) questionnaire18 if the patient was unable to perform MMSE. Cognitive impairment was defined as MMSE <19 points,19 AD8 ≥3 points18 or pre-existing dementia diagnosis. We also calculated two widely used measures of pneumonia severity: CURB-65 score (Pneumonia Severity Score; range: 0–5), which includes confusion, uraemia, elevated respiratory rate, hypotension and ≥65 years of age20 and Pneumonia Severity Index (PSI) score (range: 0–395), which uses demographics, comorbidities, physical examination findings, vital signs, essential laboratory results and radiographic findings.
Measurement of frailty
The deficit-accumulation approach of frailty measurement views frailty as an age-related state of poor health that is proportional to the cumulative burden of age-related deficits.21 22 Deficits can include various attributes from a standardised clinical assessment or laboratory tests, and the degree of frailty is dependent on the total deficit burden, rather than choice of specific deficit items.23 We calculated a 50-item Frailty Index (FI) from the baseline assessment that included 25 comorbidities, polypharmacy (≥5 prescription drugs), 21 functional status items, weight loss >5 kg in the past year, body mass index <21 kg/m2 and serum albumin level <3.5 g/L. The FI (range: 0–1) is calculated as the proportion of abnormalities (eg, a patient with 20 abnormal findings has an FI of 0.40 (=20/50)). Patients were classified into robust (<0.15), pre-frail (0.15–0.24), mild-to-moderately frail (0.25–0.44) and severely frail (≥0.45) categories.24
Outcome assessment
At 1, 3 and 6 months after baseline assessment, study clinicians (CMP, WK) conducted telephone interview of patients or their caregivers to assess the ability to perform the above-listed 21 activities and physical tasks without another person’s help. The functional status composite score was created (range: 0–21), with higher values indicating better function. We also assessed in-hospital events and 6-month mortality, prolonged hospitalisation (length of stay ≥15 days) and discharged to long-term care facility. For the discharge to long-term institution events, patients who were admitted from long-term care at baseline were excluded and only those who were newly discharged to the long-term facilities were counted.
Statistical analysis
We used group-based trajectory modelling to identify clinically meaningful trajectories of functional status over 6 months after pneumonia hospitalisation.25 The functional status scores (0–21 activities) during the follow-up period were modelled using censored normal distribution, after 22 patients who died before 1-month follow-up and did not have functional status scores other than baseline score. Each trajectory was modelled with intercept only or linear, quadratic or cubic function of time since baseline assessment to find the best fitting functional form based on Bayesian Information Criterion (BIC). We considered models with 2–4 trajectories and determined the final model based on BIC and clinical interpretation of the trajectories. According to the final model, patients were assigned to a trajectory group with the maximum probability. We characterised clinical characteristics on admission and risks of death, prolonged hospitalisation, and discharge to a long-term care institution for patients with each trajectory group and compared them using Fisher’s exact test for categorical variables and analysis of variance or Kruskal-Wallis test for continuous variables. To evaluate the role of frailty assessment in predicting the recovery of hospitalisation-associated disability, we examined the proportions of different trajectories by each frailty category and estimated Spearman correlation between FI and functional status trajectory groups. We estimated OR and 95% CI of unfavourable trajectories comparing frailty categories using logistic regression that adjusted for age, sex, CURB-65 and PSI categories. As a comparison to FI, we assessed the proportions of trajectories by CURB-65 and PSI categories and estimated Spearman correlation coefficient between each pneumonia severity measure and trajectory groups. Analyses were performed with Stata, Release V.15 (StataCorp). A two-sided p value<0.05 was considered statistically significant.
Results
Functional status trajectories after hospitalisation with pneumonia
The final group-based trajectory model included four trajectories of functional status change over 6 months after pneumonia hospitalisation: excellent, 28 (13.9%); good, 52 (25.9%); poor, 58 (28.9%); and very poor, 63 (31.3%) (figure 1). Patients who followed the excellent trajectory had a mean baseline functional score of 21 (SD: 0) and remained fully independent throughout 6 months. Patients in the good trajectory group also had a mean baseline functional score of 18.2 (1.9) with a minimal decline. Patients in the poor trajectory group had a mean baseline functional score of 11.8 (5.1) and experienced a substantial 50% decline (approximately six activities) at 1 month and remained impaired throughout 6 months. Patients in the very poor trajectory group started with a very low baseline functional score of 1.4 (2.4) with a minimal decline. Except for the excellent trajectory group, none of the trajectories returned to the baseline functional status. The 6-month mortality rates for four trajectory groups were 10.3%, 5.9%, 33.5% and 46.1%, respectively.
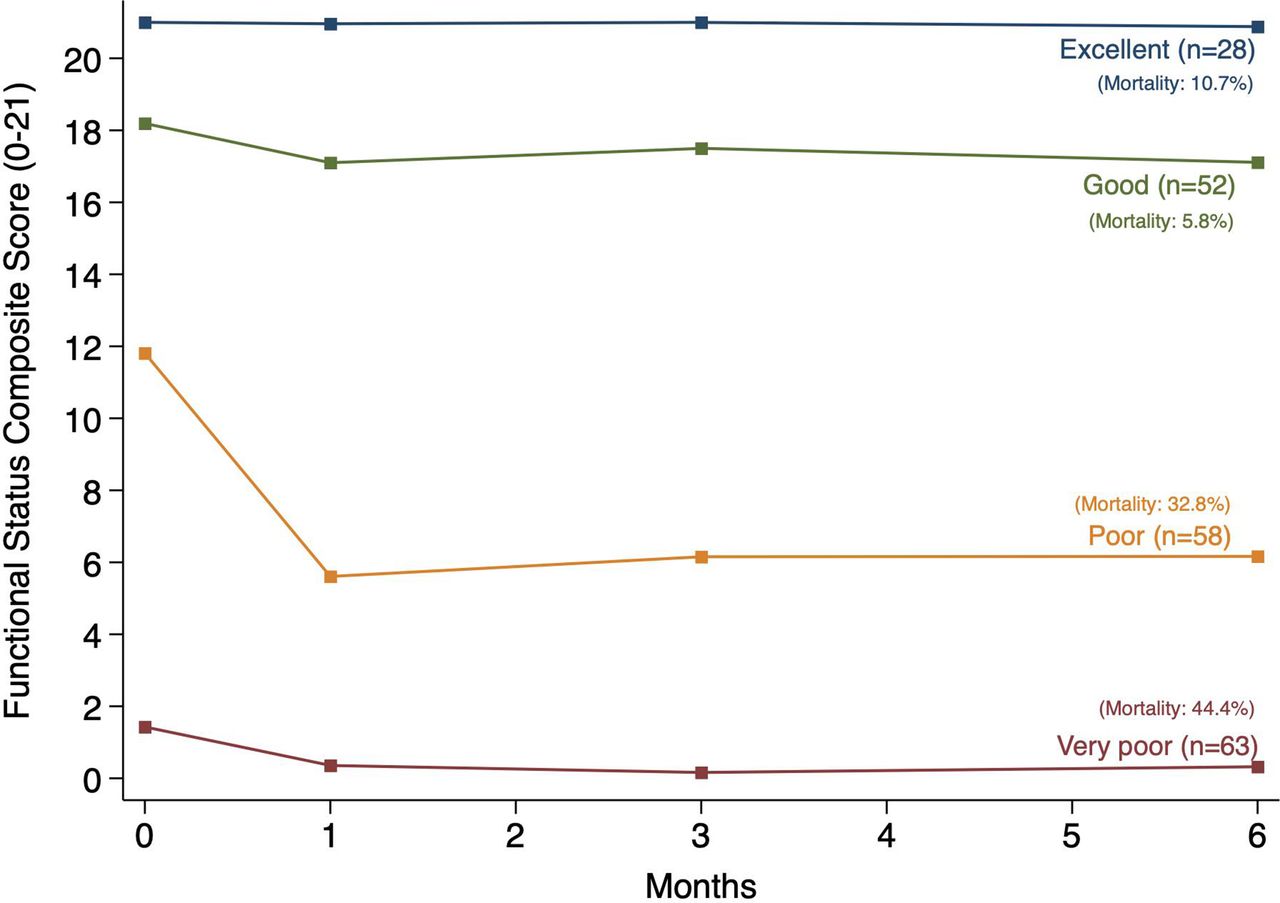
Functional status recovery trajectories in hospitalised older adults with pneumonia. The functional status composite score is ability to perform 21 activities of daily living, instrumental activities of daily living and physical tasks without another person’s help. The score range 0–21 with higher values indicating better function. Four trajectories were identified using a group-based trajectory model based on functional status at baseline and during the 6-month follow-up: excellent, (n=28; mortality,10.7%); good, (n=52; mortality, 5.8%), poor (n=58; mortality, 32.8%) and very poor (n=63; mortality, 44.4%).
Baseline characteristics associated with functional status trajectories
Compared with those who had excellent or good trajectories, patients with poor or very poor trajectories were older (mean (SD) age: excellent, 74.4 (6.6) vs very poor, 80.4 (7.7)), had greater frailty (median (25th percentile, 75th percentile) FI: excellent, 0.07 (0.04, 0.11) vs very poor, 0.54 (0.50, 0.58)) and more severe pneumonia by CURB-65 score (median (25th percentile, 75th percentile): excellent, 2 (1, 2) vs very poor, 3 (1, 4)) and PSI score (median (25th percentile, 75th percentile): excellent, 105 (83, 113) vs very poor, 143.5 (121, 171)) (table 1). They also had higher prevalence of stroke history (excellent, 2 (7.1%) vs very poor, 29 (46.0%)), ADL disability (excellent, 0 (0%) vs very poor, 62 (98.4%)), IADL disability (excellent, 0 (0%) vs very poor, 63 (100%)) and nursing home resident status (excellent, 0 (0%) vs very poor, 33 (52.4%)).
Baseline characteristics by functional status trajectory after pneumonia hospitalisation
In-hospital events and 6-month functional status trajectories
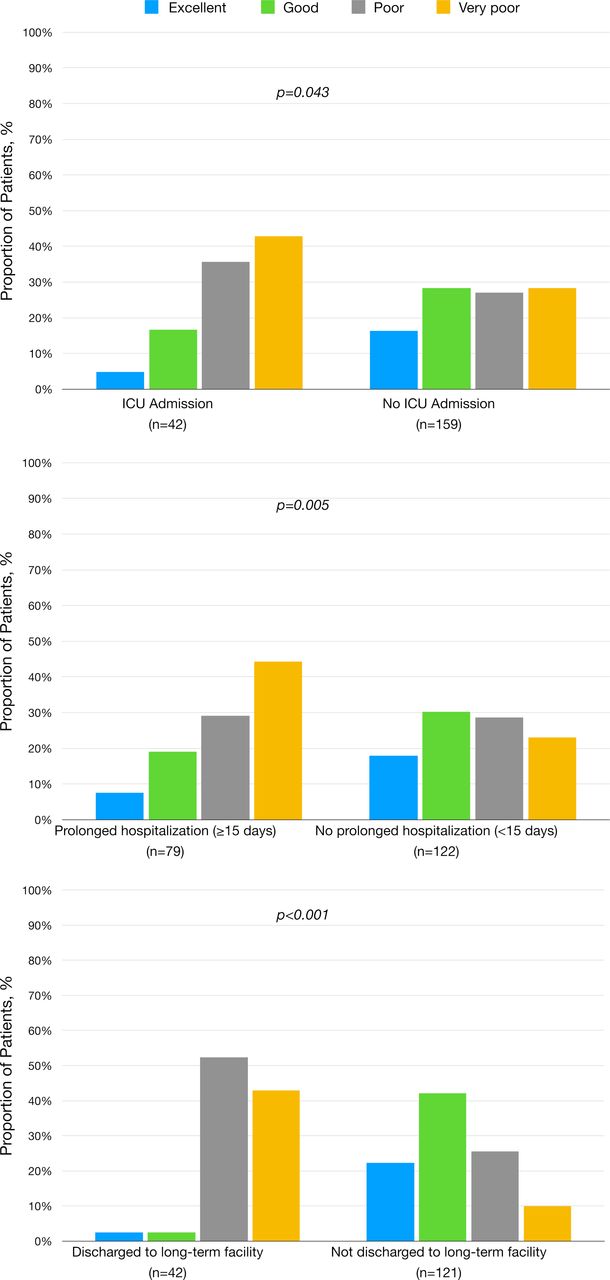
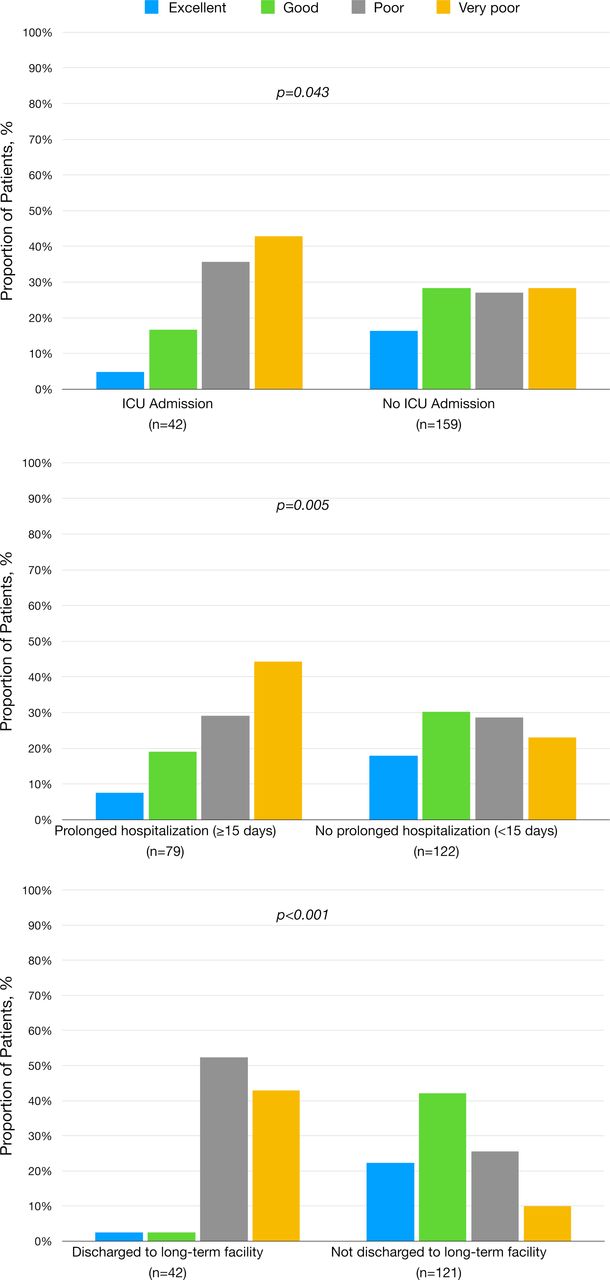
To observe in-hospital events occurred in patients by each trajectory group, the frequency and the proportion of different in-hospital events are presented in figure 2. For intensive care unit (ICU) admission, the most common trajectory was very poor trajectory (18, (28.6%)), followed by poor (15, (25.9%)), good (7, (13.5%)) and excellent (2, (7.1%)) trajectories. Prolonged hospitalisation (length of stay >15 days) showed the pattern similar to ICU admission, with the most common trajectories being very poor trajectory (35, (55.6%)), followed by poor (23, (39.7%)), good (15, (28.9%)) and excellent (6, (21.4%)) trajectories. Unlike ICU admission and prolonged hospitalisation, older patients who discharged to a long-term care facility were mostly from poor trajectory (22, (41.5%)), followed by very poor (18, (60.0%)), good (1, (1.9%)) and excellent (1, (3.6%)) trajectories. Although there were less frequent patients in very poor trajectory group compared with the poor trajectory group, the proportion was higher. This may be because there were 33 out of 38 patients from long-term care facilities pre-admission who were in the very poor trajectory group and excluded from the analysis.
{kind=link}
{kind=link}
In-hospital events and 6-month functional trajectories. In-hospital events versus event-free were compared for each trajectory group: ICU admission versus no ICU admission, prolonged hospitalisation (length of stay ≥15 days) versus no prolonged hospitalisation (length of stay ≥15 days), and discharged to long-term care facility versus not discharged to long-term facility. The proportions of patients from each trajectory group are presented in different colours of bar graphs. Excellent trajectory group (blue, n=28); good trajectory group (green, n=52); poor trajectory group (grey, n=58); and very poor trajectory (yellow, n=63). The proportions of patients in long-term care institutionalisation excluded 38 patients from long-term care facilities pre-admission: excellent trajectory group (blue, n=28); good trajectory group (green, n=52); poor trajectory group (grey, n=53); and very poor trajectory (yellow, n=30). ICU, intensive care unit.
Frailty, pneumonia severity and functional status trajectories
Functional status trajectory was strongly dependent on frailty status on admission (Spearman correlation coefficient with functional status trajectory categories: 0.90; p<0.01) (table 2). Among robust patients, the most common trajectory was excellent trajectory (54.9%), followed by good trajectory (33.3%) and poor trajectory (11.8%). Almost three quarters of pre-frail patients followed good trajectory (74.4%) and the remainder followed poor trajectory. The majority of mild-to-moderately frail patients and severely frail patients followed poor trajectory (85.0%) and very poor trajectory (89.6%), respectively. The probability that a patient would follow unfavourable trajectories (poor or very poor) increased from 11.8% in robust patients, 25.6% in pre-frail patients, 92.5% in mild-to-moderately frail patients, to 100% in severely frail patients.
Frailty Index, pneumonia severity and functional status trajectory after pneumonia hospitalisation
Pneumonia severity measures were modestly correlated with functional status trajectories (Spearman correlation coefficient with functional status trajectory categories: 0.45; p<0.01, for CURB-65; 0.39; p<0.01, for PSI) (table 2). As a result, neither CURB-65 nor PSI on admission uniquely distinguish functional status trajectories.
Discussion
Little is known about the severity and duration of hospitalisation-associated disability after acute infectious disease in older adults. Our study found that 60.2% of hospitalised older patients with pneumonia experienced unfavourable—poor (substantial decline from baseline) and very poor (persistently low)—trajectories and that the probability of following the unfavourable trajectory increased exponentially from 11.8% in robust patients, 25.6% in pre-frail patients, 92.5% in mild-to-moderately frail patients, to 100% in severely frail patients. Although older adults with frailty had more severe pneumonia, the association of frailty with unfavourable trajectory was independent of pneumonia severity. These results highlight the high incidence and lasting duration of hospitalisation-associated disability in older adults with pneumonia.
Previous studies have shown that hospitalisation-associated disability in older adults was associated with change in functional status prior to hospitalisation,26 frailty and cognitive decline at hospital admission.27–31 Acute illness or injuries such as a fall that results in a hospitalisation increases the risk of new or worsening disability.30 32 Gill et al found that in older adults, pre-hospitalisation disability and frailty are associated with an increased risk of functional decline and decreased ability to recover post-hospitalisation.30 32 Results of our study confirm findings of previous studies while adding to the literature knowledge that is specific for hospitalisation due to pneumonia, a common cause of hospitalisation in older adults. Similar to the functional trajectories found by Gill et al after hospitalisation due to falls,32 we found various functional trajectories older adults experience 6 months after hospitalisation due to pneumonia. Functional trajectories 6 months after admission due to acute respiratory failure were reported in recent studies,33 34 however, the patient population was not specific to older adults and baseline clinical characterisation of patients were not present.
In our study, we used frailty as a clinical measure to characterise the baseline health status of patients. The FI takes into consideration various health domains that are routinely assessed in an evaluation of older patients, such as medical history, cognitive status and Katz or Barthel ADL index. The average administration time in our study was 15–20 min without cognitive assessment and 30 min with cognitive assessment (which was not feasible in 60% of the patients). The FI allows gradation of frailty severity (as opposed to just the presence or absence of frailty) and a more holistic and complete assessment for comprehensive care planning. Cognitive impairment is important to capture as it has been shown to be associated with worse disability after a hospitalisation in older adults.27 Our findings suggest the utility of FI to assist in anticipatory discharge planning after an acute hospitalisation due to pneumonia.
Commonly used pneumonia severity measures, CURB-65 and PSI, were developed to predict 30-day mortality.35 These measures do not take baseline functional status into consideration. Functional status and recovery are important outcomes to many older patients who survive acute hospitalisation for pneumonia. Chen et al showed that PSI was associated with delayed discharge and functional decline in older patients with pneumonia.36 In our study, CURB-65 and PSI were scattered across all trajectory groups and did not reliably predict long-term functional status as compared with FI. These results suggest that FI should be used in conjunction with pneumonia severity scores to provide appropriate hospital and post-acute care in hospitalised older patients with pneumonia. In addition to long-term functional status, the four trajectory groups also correlated with in-hospital outcomes. Worse trajectory groups had higher rates of ICU admission, prolonged hospitalisation and long-term care institutionalisation. Though patients in the excellent and good trajectory group composed 20.6% of ICU admissions and 50.4% of prolonged hospitalisation, they only made up 5.5% of the patients who went to long-term care institutions. This suggests that though patients in the excellent and good trajectory group may have arduous hospitalisations, they may be able to recover and be discharged home rather than to a long-term care centre. By being able to predict the trajectory of patients using the FI, this could have important clinical implications in terms of deciding management of older patients with pneumonia. Since ending up in long-term care institutions is an important decision-making factor for patients, the ability to predict who could avoid this outcome based on FI could guide aggressivity of pneumonia management.
Our study suggests a possible window of opportunity to implement rehabilitation programmes to prevent the loss of functional status, especially for those who are pre-frail or mild-to-moderately frail on admission. Of the four functional status trajectories, the poor trajectory group experienced a substantial decline in functional status within the first month of the admission and persistent disability afterwards (figure 1). A majority of patients in this group were pre-frail (11 of 58 patients) or mild-to-moderately frail (34 of 58 patients). Whereas previous studies have looked at the effect of implementing rehabilitation programmes for ICU, chronic obstructive pulmonary disease and emergency department patients,37–39 no studies examined interventions for older patients based on frailty levels immediately following an acute hospitalisation. Based on our findings, interventions targeting pre-frail or mild-to-moderately frail older patients may achieve a larger reduction in hospitalisation-associated disability.
Our study has several strengths and limitations. Major strengths of our study include a prospective cohort design to assess functional recovery in an acute care setting over an extensive 6-month period with high rates of successful follow-up. Additionally, the present study enrolled 201 patients with a fairly even distribution of baseline frailty. However, the study has a few limitations that merit consideration. First, functional status was defined by self-reported telephone interviews, rather than through clinician-based observation. Second, our results may have limited generalisability and external validity given that the present study employed a single centre prospective cohort, which was comprised entirely of an older Korean population. It is possible that functional recovery in older results may differ in a more diverse patient population; hence, we recommend that clinicians weigh geographic and situational differences specific to their healthcare infrastructure in their interpretation of our results. Additionally, our cohort was restricted to older adults who were hospitalised due to pneumonia, and therefore, our results could be limited to the applications of a single disease, notwithstanding the fact that pneumonia is associated with significant mortality and morbidity in many older adults.5 40 Finally, a small minority of older adults, such as patients with cancer included in the robust frailty group, may experience temporal variations in post-baseline frailty, and hence, in turn, could interfere with the predictive ability of our trajectory scores.
In conclusion, our study showed that 6 of every 10 older patients who were hospitalised for pneumonia had substantial loss or persistent severe impairment in functional status. Frailty status on admission was a strong determinant of post-hospitalisation functional status trajectory, independently of pneumonia severity. These results can be useful to develop interventions and prioritise resources to prevent hospitalisation-associated disability in hospitalised older patients with pneumonia.
Data availability statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Korea University Anam Hospital, IRB number K2019-1789-010. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Presented at This work was presented in part at the American Geriatrics Society (AGS) 2020 Annual Scientific Meeting. The manuscript is not under consideration by another journal.
Contributors Study design and concept: CMP, DHK. Acquisition, analysis and interpretation of data: CMP, WK, HCR, ESL, JHK, DHK. Drafting of the manuscript: CMP, RD, JJL, SMS, DHK. Critical revision of the manuscript for important intellectual content: CMP, WK, ESL, JHK, DHK. Statistical analysis: CMP, DHK. Administrative, technical or material support: CMP, WK, DHK. Study supervision: WK, DHK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.