Article Text

Abstract
Background Non-invasive ventilation (NIV), although effective in treating hypercapnic respiratory failure, has not demonstrated the same efficacy in treating acute hypoxaemic respiratory failure. We aimed to examine the effect of NIV use on ventilator-free days in patients with acute hypoxaemic respiratory failure admitted to the intensive care unit (ICU).
Methods We conducted a retrospective study of patients admitted to the ICU with acute hypoxaemic respiratory failure at Waikato Hospital, New Zealand, from 1 January 2009 to 31 December 2018. Patients treated with NIV as the initial oxygenation strategy were compared with controls treated with early intubation. The two groups were matched using a propensity score based on baseline characteristics. The primary outcome was the number of ventilator-free days at day 28. The secondary outcomes were ICU and hospital length of stay and in-hospital mortality.
Results Out of 175 eligible patients, 79 each out of the NIV and early intubation groups were matched using a propensity score. Early NIV was associated with significantly higher median ventilator-free days than early intubation (17 days vs 23 days, p=0.013). There was no significant difference in median ICU length of stay (112.5 hours vs 117.7 hours), hospital length of stay (14 days vs 14 days) or in-hospital mortality (31.6% vs 37.9%) between the NIV and the early intubation group.
Conclusion Compared with early intubation, NIV use was associated with more ventilator-free days in patients with hypoxaemic respiratory failure. However, this did not translate into a shorter length of stay or reduced mortality based on our single-centre experience.
- Non invasive ventilation
- ARDS
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is conflicting evidence on the use of non-invasive ventilation (NIV) in acute hypoxaemic respiratory failure.
Current guidelines make no recommendation on its use.
WHAT THIS STUDY ADDS
Compared with an early intubation strategy, NIV was associated with a higher number of ventilator-free days.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study is among the first to use this promising outcome measure that is both clinician-centred and patient-centred in the assessment of the efficacy of NIV in acute hypoxaemic respiratory failure.
It provides clinicians and researchers with further information during decision making.
Introduction
Acute hypoxaemic respiratory failure (AHRF) is a common cause of admission to the intensive care unit (ICU), with more than half of patients admitted to the ICU affected by hypoxaemia.1 Mortality rates remain high and are associated with the presence and extent of infiltrates on chest radiographs, severity of hypoxaemia and presence of acute respiratory distress syndrome (ARDS).2
Unlike in hypercapnic respiratory failure, the efficacy of use of non-invasive ventilation (NIV) in the management of AHRF is not well established. Although a meta-analysis of randomised controlled trials (RCTs) has shown that NIV use reduced the rate of endotracheal intubation and hospital mortality in AHRF,3 most included trials were small and heterogeneous. The European Respiratory Society/American Thoracic Society guideline on acute respiratory failure was unable to make a recommendation on the use of NIV in de-novo AHRF given the inconclusive evidence.4
The selection of a clinically relevant outcome for studying the impact of NIV use on AHRF is important. The mortality benefit of NIV use may be small and difficult to assess in an RCT. Intubation rate as an outcome does not consider the potential harms of delaying intubation in those who inevitably need it despite a trial of NIV. On the other hand, ventilator-free days may be relevant and meaningful to clinicians, patients and health systems. It considers both the possible benefit of NIV and intubation prevention as well as the possible harms of NIV failure.
Few studies have assessed the efficacy and safety of NIV in AHRF with specific attention on ventilator-free days. The purpose of this study is to evaluate the effect of NIV use on ventilator-free days in patients admitted to the ICU with AHRF.
Methods
We conducted a retrospective observational study comparing patients who received NIV with patients who were intubated without a trial of NIV for AHRF from 1 January 2009 to 31 December 2018 at Waikato Hospital Intensive Care Unit. This is a tertiary-level, 15-bed closed ICU staffed by specialist intensivists at all hours. The requirement for consent was waived given the retrospective observational nature of the study. Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of this study. Eligible participants were identified from the Australian and New Zealand Intensive Care Society Centre for Outcome and Resource Evaluation adult patient database and clinical coding (New Zealand Ministry of Health data set).
Participants
We included all patients aged 18 and above admitted to the ICU with AHRF for more than 24 hours. We excluded patients with cardiogenic pulmonary oedema, asthma or chronic obstructive pulmonary disease exacerbation (as the underlying pathophysiology of respiratory failure, and the evidence base for NIV use in these populations is different),5–7 established ceilings of treatment precluding tracheal intubation, extubation within 24 hours prior to admission, palliative care or organ donation as their treatment goal, and those who were admitted from the operating theatre already intubated.
Hypoxaemic respiratory failure was defined as an arterial oxygen partial pressure (PaO2) of less than 60 mm Hg (equivalent to 8.0 kPa) of room air and normal or low partial pressure of carbon dioxide of less than 45 mm Hg (equivalent to 6.0 kPa). Where supplemental oxygen was applied before the measurement of arterial blood gases, the definition of AHRF included the requirement for supplemental oxygen to maintain a saturation of 90% or a PaO2 to the fraction of inspired oxygen (FiO2) ratio of <300 (in mm Hg), as well as hypocapnia or normocapnia on blood gas analysis.
Data collection
Data were collected on patients’ age, sex, comorbidities, diagnosis, laboratory parameters including PaO2, PaO2 to FiO2 (PF) ratio, creatinine, platelet count and bilirubin concentration, and Glasgow Coma Scale (GCS) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores. Individual components of the Sequential Organ Failure Assessment (SOFA) score on admission, excluding the cardiovascular component, were calculated, as well as the Charlson comorbidity index. Data were retrospectively collected according to a prespecified template.
Interventions and outcomes
The intervention of interest was NIV use as the initial oxygenation strategy versus early tracheal intubation. The definition of NIV in our study includes both bilevel positive airway pressure and continuous positive airway pressure therapy. NIV was delivered via a mechanical ventilator through a dual-limb circuit with the interface of an oronasal face mask or full face mask depending on the patient’s tolerance, mask fit and air leak. Settings were instituted at the discretion of the treating clinician based on physiological and clinical assessment. Treatment with invasive mechanical ventilation was provided in accordance with international guidelines using a lung-protective ventilatory strategy. Weaning and readiness for extubation were at the discretion of the treating clinician but adhered to standard practice.
The primary outcome was the number of ventilator-free days at day 28 (VFD-28), defined as days alive and free of invasive mechanical ventilation in the 28 days following admission to ICU. Patients who died in-hospital were assigned 0 VFD-28. The secondary outcomes included in-hospital mortality, ICU length of stay, hospital length of stay, and requirement for adjunctive therapies, including prone positioning, inhaled nitric oxide, tracheostomy, renal replacement therapy or extracorporeal membrane oxygenation.
Statistical analysis
The planned sample size of 198 patients allowed 80% power to detect a difference of 4 VFD-28 with an assumed VFD-28 of 14.5 days in the intubation group.8 Given that allocation was not randomised, we performed a propensity score-matched analysis to minimise the potential confounding of treatment allocation on outcomes of interest. We used a multivariate logistic regression model to calculate the probability of being assigned to the exposure or control group. Selected variables included age, sex, ethnicity, cause of AHRF, individual components of the Charlson comorbidity index, SOFA score (excluding the cardiovascular component), APACHE II score, immunosuppressed status, PF ratio on admission, bilirubin, platelet count, creatinine and GCS score. The matching procedure was conducted on a 1:1 ratio without replacement using a nearest neighbour approach. Balance was assessed through visual inspection of matched data and t-test of difference-in-means. Using the matched cohort, baseline and outcome variables were compared using χ2 test or Fisher’s exact test as appropriate for categorical variables, Student’s t-test for normally distributed continuous variables and Wilcoxon rank-sum test for non-parametric variables. We used a p value threshold of 0.05 for statistical significance. All analyses were performed using RStudio V.1.2.1335.
Results
Patient characteristics
There were 1102 patients identified with a respiratory diagnosis code from the ICU adult patient database from 1 January 2009 to 31 December 2018 (figure 1). Of the patients, 175 met the inclusion criteria. Ninety-four patients underwent early intubation following standard therapies to deliver supplemental oxygen or high-flow nasal cannula (HFNC). Eighty-one patients were treated with NIV at first instance. Of the 81 patients, 29 avoided intubation, while the other 52 were subsequently intubated.
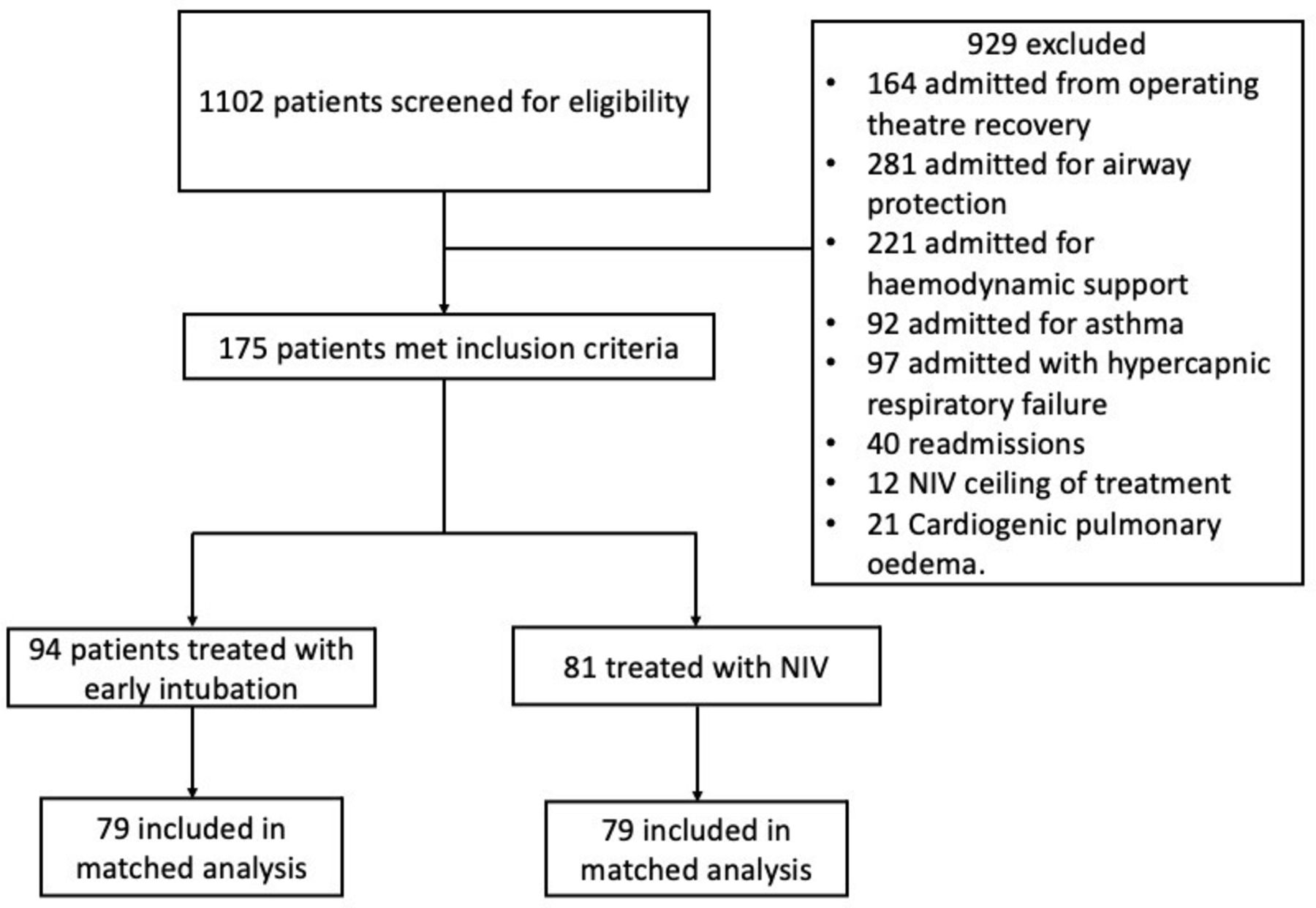
Study flow chart. NIV, non-invasive ventilation.
The baseline characteristics of the patients before and after matching are summarised in table 1. Before matching, there were statistically significant differences in APACHE II score and PF ratio between the NIV and intubation groups. Patients in the intubation group were older, although this difference was not statistically significant. Using propensity scores, 79 patients in the NIV group were matched with 79 patients in the intubation group. We observed a good balance between matched cohorts through visual assessment (online supplemental figure 1) and statistical analysis (table 1). The difference in the cause of AHRF was the only significantly different baseline characteristics between the two groups. There was a higher proportion of bacterial pneumonia in the intubation group and a higher proportion of ‘other’ causes in the NIV group. ‘Other’ causes include diffuse alveolar haemorrhage (8 patients), thoracic trauma (5 patients), interstitial lung disease (11 patients), pulmonary malignancy (7 patients) and extrapulmonary ARDS (2 patients).
Supplemental material
Baseline characteristics
Study outcomes
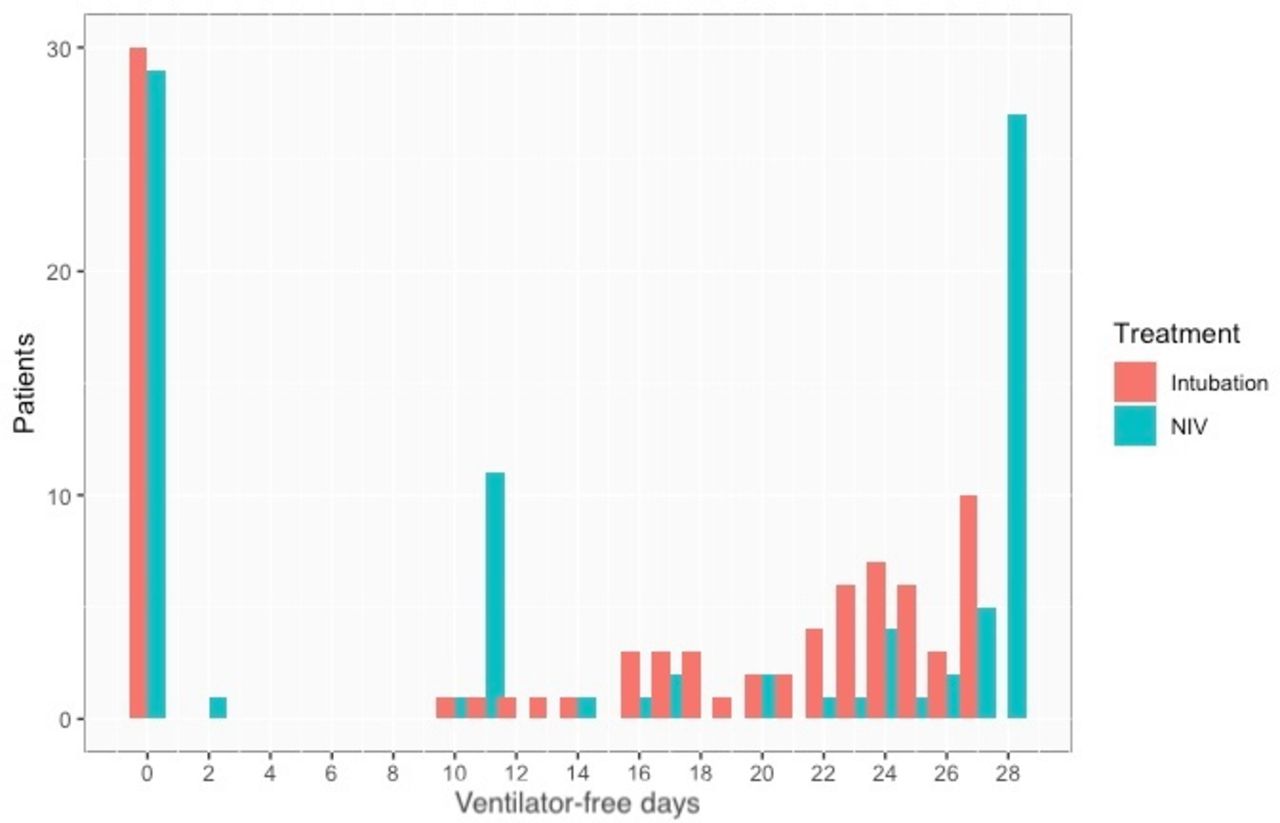
In patients with AHRF, NIV use was associated with a higher median VFD-28 compared with early intubation (23 days vs 17 days, respectively, p=0.013). However, no statistically significant difference was observed in the median ICU length of stay, median hospital length of stay, in-hospital mortality or use of adjunctive therapies (table 2). No in-hospital deaths occurred after day 28. Figure 2 shows the distribution of ventilator-free days and figure 3 shows the cumulative density proportion between the two groups.
Study outcomes
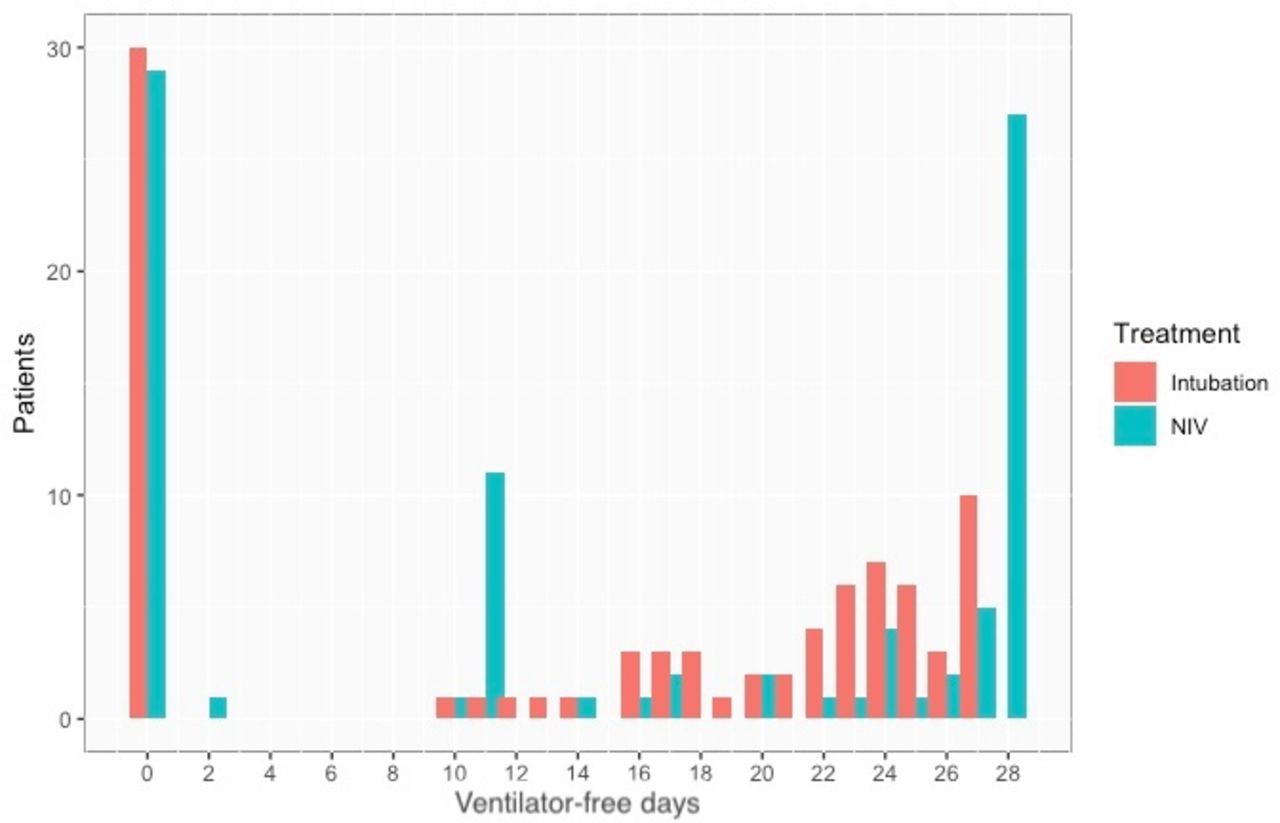
Distribution bar plot shows the distribution of ventilator–free days among all the patients in both NIV (blue) and early intubation (red) groups. NIV, non-invasive ventilation.

{kind=link}
{kind=link}
{kind=link}
Cumulative density proportion plot shows the cumulative proportion of patients over increasing ventilator-free days. The difference in the height of the two curves at any point represents the difference in the cumulative probability of having a value for days without invasive ventilation of less than or equal to that point on the x-axis. NIV, non-invasive ventilation.
Subgroup analysis
Of the 51 patients who failed initial treatment with NIV requiring subsequent intubation (NIV failure group), 25 died in hospital, giving an in-hospital mortality rate of 49%. Subgroup analysis was undertaken to see if NIV failure results in lower VFD-28. The median VFD-28 in the NIV failure group was numerically lower (0 days vs 17 days); however, this difference was not statistically significant (p=0.09894).
Univariate analysis performed between NIV success and NIV failure patients showed higher APACHE II score, higher creatinine and higher proportion of viral pneumonia in the NIV failure group (online supplemental table 1). These, however, were not significant on multiple regression analyses.
Discussion
This propensity-matched cohort study showed that NIV used as the initial oxygenation strategy was associated with higher ventilator-free days than an early intubation strategy. This, however, did not translate into a difference in in-hospital mortality, ICU length of stay or hospital length of stay. Of note, patients who failed NIV treatment and were subsequently intubated had a high mortality rate and thus fewer VFD-28 compared with the early intubation cohort. This finding was not statistically significant, likely due to the small sample sizes.
To date, RCTs have shown inconsistent results on the effect of NIV on mortality in patients with AHRF.9 10 Although a previous meta-analysis of RCTs demonstrated a mortality benefit, the results were inconclusive as there was significant heterogeneity between studies.3 There is a concern that NIV use in AHRF could improve gas exchange, but mask clinical deterioration and increase adverse events following treatment failure.11 12 When NIV is interrupted, there could be a quick loss of positive effects on alveolar recruitment and reduction in work of breathing.13 We tried to account for this concern by using the composite endpoint of VFD-28, which aims to balance the benefits of success (avoiding intubation and survival) with the risks of failure (prolonged mechanical ventilation or death).
In our study, we had a high rate of NIV failure, with 65% of patients in the NIV group requiring subsequent intubation. This finding is comparable with some studies,14 15 but higher than the recent Large Observational Study to Undertand the Global Impact of Severe Acute Respiratory Failure (LUNGSAFE) subanalysis of NIV use in ARDS.16 Those who failed NIV also had a high mortality rate, a finding consistent with the current literature highlighting the safety concerns with NIV use for this indication.17
Compared with those who avoided intubation, those who failed NIV had significantly higher APACHE II scores and serum creatinine and higher proportion of bacterial pneumonia diagnosis. A study of similar size assessing the risk factors for NIV failure in haematopoietic stem cell transplantation patients with ARDS showed elevated creatinine as a risk factor for NIV failure.18 Our study is also consistent with other previous studies showing community-acquired pneumonia, illness severity and extrapulmonary organ dysfunction to be associated with NIV failure.19
Interestingly, other poor prognostic indicators identified in previous studies, such as PF ratio and age, were not significantly different between the NIV success and failure groups in our study.19 20 This could be due to the small sample size of our study and reflect a type II error. The proportion of patients with viral pneumonia was similar in the NIV success and failure groups. This is of interest to the current COVID-19 pandemic. RCTs are underway to assess non-invasive oxygenation strategies in COVID-19 pneumonitis, with some early promising results.21 22
Compared with the LUNGSAFE cohort,16 we had a higher in-hospital mortality rate in the early intubation patients. This could be due to the differences in inclusion criteria; our study excluded admissions directly from the operating theatre, which would include patients undergoing elective surgical procedures generally associated with a lower in-hospital mortality rate. The mortality rate in the NIV groups, however, was similar in both studies. Much like the LUNGSAFE substudy, we found no difference in in-hospital mortality between the early intubation group and NIV group after propensity score matching.
To our knowledge, this is the first study to use ventilator-free days as the primary outcome measure in assessing the efficacy of NIV. This endpoint takes into account the mortality and duration of mechanical ventilation, which are important patient-centred outcomes.23 Although previous studies showed a detectable difference in mortality for interventions with patients with PF ratio <150,16 24 25 sample sizes in these studies were larger. In addition, studies have shown the mortality rate for ICU patients in Australia and New Zealand to be lower than the rest of the world, causing concern for not detecting a difference in mortality.26 For these reasons, we believed VFD-28 to be an outcome measure that provides greater statistical power to detect a clinically important treatment effect in the design of this study. The use of propensity score matching allows us to match more patients than traditional matching methods based on each individual covariate, increasing the precision of our findings.27 The lack of effect of NIV use on in-hospital mortality is consistent with previous studies showing a small if not negligible difference.4 28 We also excluded patients with treatment limitations that prohibit invasive mechanical ventilation, making these data comparable with previous studies.
Limitations of the study include its retrospective and non-randomised design. We attempted to minimise bias by applying strict inclusion criteria consistent with the existing literature and by using propensity score matching to control for confounding variables. Despite the use of propensity matching, there remained differences in the cause of AHRF between the two groups, which confound and reduce the sensitivity of our findings. The small sample size and the large number of patients excluded also make these results difficult to generalise. We could not accurately capture other possible confounders, such as HFNC, NIV settings, rates of reintubation or successful extubation after reintubation, as this information was not routinely collected in the databases we used.15 29 HFNC has been used to treat AHRF at our centre for approximately a decade. Hence, most patients included are likely to have had a trial of HFNC before being considered for either NIV or tracheal intubation in ICU.
The low VFD-28 in the NIV failure group is primarily due to the fact nearly half of these patients (49%) died rather than due to prolonged mechanical ventilation. This high mortality rate is likely due to these patients being sicker and having more extrapulmonary organ dysfunction. As highlighted by our study and others, these differences underscore the importance of patient selection in selecting NIV as the initial oxygenation strategy. We could not truly compare this group with an early intubation strategy as the NIV failure group are selected based on an outcome occurring after treatment allocation.
This study contributes additional evidence that NIV use in AHRF in ICUs could improve outcomes other than intubation rate or mortality alone. This study also demonstrates that the use of VFD-28 as an endpoint in trials assessing non-invasive oxygenation strategies may be desirable, especially when the prior likelihood of a mortality benefit is small.
In conclusion, this single-centre, propensity-matched analysis showed the use of NIV as the initial oxygenation strategy in AHRF is associated with higher VFD-28 compared with early tracheal intubation. Although NIV as the initial oxygenation strategy did not translate into a difference in in-hospital mortality, our results suggest that it can be considered a safe alternative to early intubation in carefully selected, closely monitored patients with AHRF.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the New Zealand Health and Disability Ethics Committee (19/CEN/199). This study was retrospective and approved by the human ethics committee and deemed of low risk and hence informed consent was waived.
Acknowledgments
We would like to acknowledge the assistance of Veronique Gibbons with reviewing the study protocol and registering the study, as well as Dianne Takiari for obtaining data from ANZICS-CORE. We would also like to acknowledge the Waikato Hospital Respiratory Research Unit for providing the open access fee for this publication.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DJ and RAM conceptualised the study. DJ and SMF developed the data collection template and collected the data. DJ and CLC analysed and interpreted the data. DJ and CLC wrote the initial draft of the manuscript, with editing and revision by RAM and SMF. RAM and CLC provided supervision. CLC and DJ administered the study. DJ as the guarantor of this study accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.