Article Text

Abstract
Background Aboriginal Australians are reported to have a high burden of chronic airway diseases. However, prescribing patterns and related outcomes of airway directed inhaled pharmacotherapy, (short-acting beta agonists (SABA), short-acting muscarinic antagonists (SAMA), long-acting β-agonists (LABA), long-acting muscarinic antagonists (LAMA) and inhaled corticosteroids (ICS)) among Aboriginal Australian patients with chronic airway disease have been sparsely reported in the past.
Methods A retrospective cohort study was conducted, using clinical, spirometry data, chest radiology, primary healthcare (PHC) presentations and hospital admission rates among Aboriginal patients identified to have been prescribed inhaled pharmacotherapy in remote and rural communities referred to the respiratory specialist service in the Top End, Northern Territory of Australia.
Results Of the 372 identified active patients, 346 (93%) had inhaled pharmacotherapy prescribed (64% female, median age 57.7 years). ICS was the most common prescription (72% of the total cohort) and was recorded to be prescribed in 76% of patients with bronchiectasis, and 80% of patients with asthma or chronic obstructive pulmonary disease (COPD). Fifty-eight percent of patients had a respiratory hospital admission and 57% had a recorded PHC presentation for a respiratory issue during the study period, with a higher rate of hospital admissions among patients prescribed ICS compared with those on SAMA/SABA or LAMA/LABA without ICS (median rate (per person per year) 0.42 vs 0.21 and 0.21 (p=0.004). Regression models demonstrated that presence of COPD or bronchiectasis alongside ICS was associated with significantly increased hospitalisation rates (1.01 admissions/person/year (95% CI 0.15 to 1.87) and 0.71 admissions/person/year (95% CI 0.23 to 1.18) against patients without COPD/bronchiectasis, respectively).
Conclusions This study demonstrates that among Aboriginal patients with chronic airway diseases, ICS is the most common inhaled pharmacotherapy prescribed. Although LAMA/LABA and concurrent ICS use may be appropriate among patients with asthma and COPD, the use of ICS may have detrimental effects among those with underlying bronchiectasis either in isolation or concurrent COPD and bronchiectasis, potentially leading to higher hospital admission rates.
- asthma
- asthma pharmacology
- Bronchiectasis
- COPD pharmacology
- imaging/CT MRI etc
- inhaler devices
- respiratory infection
- respiratory measurement
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- asthma
- asthma pharmacology
- Bronchiectasis
- COPD pharmacology
- imaging/CT MRI etc
- inhaler devices
- respiratory infection
- respiratory measurement
WHAT IS ALREADY KNOWN ON THIS TOPIC
Inhaled pharmacotherapy is often used in the management of chronic airway diseases. However, despite overwhelming evidence in the literature to suggest chronic airway diseases are highly prevalent among the adult Aboriginal Australians, the prescribing pattern/practice and appropriateness is sparsely assessed in this population.
WHAT THIS STUDY ADDS
This study demonstrated that among a referred population, the majority of Aboriginal patients with chronic airway diseases are prescribed with inhaled pharmacotherapy—inhaled corticosteroids (ICS) being the most common. Patients prescribed with ICS containing inhaled pharmacotherapy had higher recurrent hospital admissions, particularly among those with underlying chronic obstructive pulmonary disease or bronchiectasis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
ICS prescription is high, and in many cases appears inappropriate from the perspective of current guidelines, particularly concerning its use among patients with bronchiectasis. A more conservative approach should be adopted in prescription practice until prospective studies are undertaken among this population to assess safety and efficacy.
Introduction
Approximately one-third of Aboriginal Australians (Aboriginal Australian and Torres Strait Islander peoples) are diagnosed with a chronic respiratory condition, with chronic airways disease (asthma, chronic obstructive pulmonary disease (COPD) and bronchiectasis) reported to be the leading cause of morbidity and mortality in this population.1 In the Northern Territory (NT), Aboriginal Australians form 26% (approximately 60 000 people) of the overall NT population, which is the highest proportion compared with all other Australian states and territories.2 Moreover, 81% of Aboriginal people in the NT reside in remote/very remote geographic locations.2 3 Previous studies have demonstrated high rates of chronic airway diseases among NT Aboriginal people, in particular a higher burden of COPD, bronchiectasis and asthma.4 Concomitant presence of multiple respiratory conditions is also highly prevalent among NT Aboriginal people,5 specifically presence of combined COPD and bronchiectasis.6–8 Furthermore, lung function parameters are observed to be poorer among Aboriginal Australians,9–12 giving rise to considerable physical symptoms.13 In addition, hospital admission frequency/rates are reported to be much higher secondary to exacerbations of chronic airway diseases among Aboriginal Australians compared with non-Aboriginal Australians in the NT.14
Nonetheless, airway directed inhaled pharmacotherapy such as short-acting beta agonists (SABA), short-acting muscarinic antagonists (SAMA), long-acting β-agonists (LABA), long-acting muscarinic antagonists (LAMA) and inhaled corticosteroids (ICS)15 is often used/prescribed/recommended to improve symptoms, lung function parameters, reduce exacerbations and prevent hospitalisation among patients with chronic airway diseases. There are guidelines that have been established to direct appropriate prescription of inhaled pharmacotherapy, especially among patients with COPD and asthma.16 17 In the Australian context, the COPD-X Concise Guide is a widely adopted and recommended tool in the stepwise management of COPD, including use of inhaled pharmacotherapy.18–21 However, the majority of these recommendations and guidelines are drawn from studies based on non-Aboriginal/Indigenous populations and it is reasonable to speculate whether these recommendations and guidelines are applicable to Aboriginal Australians. Additionally, among patients residing in rural and remote locations, the majority of chronic medical conditions are managed at the primary healthcare (PHC) level. These services are usually provided through a remote health centre, with a nurse-based model of care supported by Aboriginal Health Practitioners and through visiting primary/medical specialists. There is often limited access to medical officers and virtually no direct access to pharmacists.22
Currently, there is sparse evidence in the literature assessing either the safety or efficacy of inhaled pharmacotherapy, or the prescribing patterns and related outcomes in the Aboriginal Australian population.23 Therefore, the aim of this retrospective study is to evaluate and to describe the clinical parameters, demographics, spirometry data, chest radiology, PHC utilisation and hospital admission frequency of Aboriginal Australians prescribed with inhaled pharmacotherapy residing in the rural and remote regions of the Top End Health Service (TEHS) region of the NT of Australia.
Methods
Setting, study participants and ethics
This retrospective cohort study was conducted at the respiratory and sleep service based at the Royal Darwin hospital (RDH) and Darwin Respiratory and sleep health (DRSH) at the Darwin private hospital in the TEHS region of the NT of Australia. The Top End region covers approximately 35% or 4 75 338 km2 of the total area of the NT, with an estimated population of 195 000 people representing 79% of the total NT population2 24 (figure 1). The study participants were Aboriginal patients residing in remote and regional Aboriginal communities referred to the respiratory and sleep outreach service by primary health practitioners and other health practitioners.4 The respiratory and sleep service at the Top End, NT has visited an average of 20 remote Aboriginal communities approximately 2–3 times a year since 2010, as a part of the respiratory outreach service in the TEHS region (prior to COVID-19 lockdown).4 9 Patients referred to the respiratory outreach service were identified through the database maintained by the respiratory and sleep outreach team at RDH. Patients included for this study were inclusive of only those patients identified to be currently marked as ‘active patients’ as per the updated outreach records at the end of 2020, or marked as ‘active’ at time of death if deceased prior to 2020.
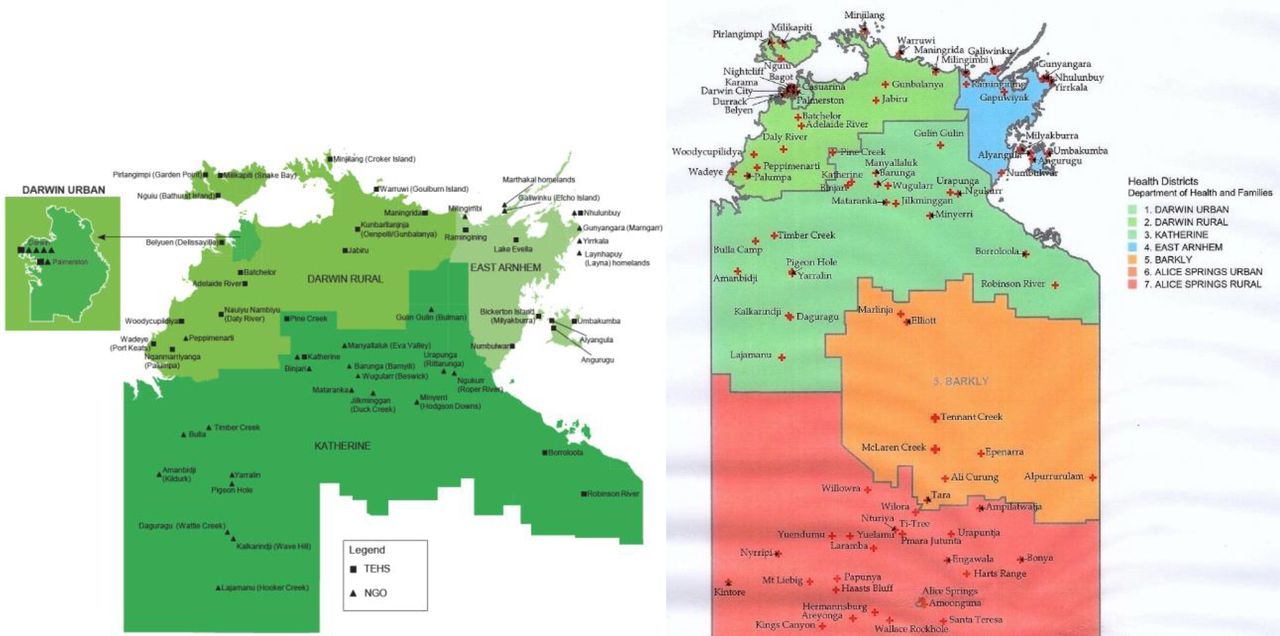
Top end health service map (TEHS), Northern Territory, Australia. Source: Department of Health—Innovation and Research—2018. Chondur R. Health Gains Planning. Department of Health and planning 2009.
The authors acknowledge the rights of Aboriginal people involved in this study, and as such conducted and reported according to strengthening and reporting of health research involving Aboriginal people.25
Patient and public involvement
As the study was retrospective in nature, patients’ participation or individual consent from the study participants was not required and the need for consent was waived by the research committee. In the public involvement perspective, Mr Izaak Thomas (Australian Aboriginal Luritja descendent) reviewed the study for its design, conduct, reporting, dissemination of our research work, in particular, the appropriateness and respect in relation to the Aboriginal context represented in this study.
Demographic, clinical, lung function and radiology data
Patients’ demographics, self-identified Aboriginal status and usual residence location according to post code were collected through hospital electronic medical records (EMRs). Patients’ EMRs were meticulously reviewed to extract information on the physician’s clinical diagnosis/documentation for the presence of chronic respiratory diseases, restricted to COPD bronchiectasis and asthma. When available, in order to confirm the presence/pattern and severity of airway disease, results of spirometry parameters; forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC ratio, including lower limit of normal (LLN) values were collected.
Spirometry parameters were assessed for presence of restrictive impairment (prebronchodilator (BD), FVC<LLN and post-BD FEV1/FVC≥0.7), mixed impairment (post-BD FEV1/FVC<0.7 and pre-BD FVC<LLN) or airflow obstruction (AO) (post-BD FEV1/FVC<0.717 26). For the presence of significant BD response (BDR), both traditional (BDRT)16 17 27 and updated (BDRU) American thoracic society/European respiratory society criteria (BDRT, BDRU) (change of ≥12% and ≥200 mL on FVC or FEV1 pre-BD to post-BD or change ≥10%, respectively) were used.28 Severity of AO was graded as per Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.17 Information on height, weight and body mass index (BMI) was recorded while patients were undergoing spirometry testing. If patients were observed to have undergone multiple spirometry tests during this study period, the earliest test acceptable and reproducible for session quality were used to assess spirometry impairments. Radiology reports were assessed for evidence of COPD and bronchiectasis.29 30 In the case of discrepancy between the EMR and chest radiology for presence of COPD or bronchiectasis, results from chest radiology were taken in preference. In the case of patients having both CT and chest X-ray (CXR) recorded, results of CT were taken in preference to CXR. The following airway diagnosis criteria was applied:
COPD was defined when chest radiology demonstrated evidence of; emphysema, bullous disease or bronchial/bronchiolar inflammation or thickening 29 or in the absence of imaging, physicians clinical EMR documentation of COPD.
Bronchiectasis was defined when chest radiology demonstrated evidence of bronchiectasis30 or in the absence of imaging, physicians clinical EMR documentation of bronchiectasis.
Asthma or ‘potential asthma’ was defined when physicians clinical EMR documented asthma and/or spirometry demonstrated presence of significant BDRT.16
Inhaled pharmacotherapy data
All available EMRs were searched to document the details of any type or combination of airway directed inhaled pharmacotherapy prescribed, more specifically—SABA (salbutamol); SAMA (ipratropium); LABA (formaterol, indacaterol, olodaterol, salmeterol, vilanterol); LAMA (aclidinium, glycopyronium, tiotropium, umeclidinium) and ICS (beclomethasone, budesonide, fluticasone). If the patients were identified to have been prescribed multiple/change in similar class of inhaled pharmacotherapy during the study period, the most recent/last prescribed type of therapy was included in the analysis. Patients inhaled pharmacotherapy use was defined as:
SAMA/SABA with no recording of either LAMA/LABA or ICS.
LAMA/LABA with or without SAMA/SABA and without ICS.
Any use of ICS.
PHC utilisation and hospital admission data
Hospital admissions data were extracted via the electronic hospital information system using International Classification of Diseases (ICD) code specifically for chronic respiratory admissions (asthma, bronchiectasis or COPD, ICD codes J44–47). When assessable and available all respiratory related remote and rural community PHC presentations were also extracted through the hospital electronic information systems using international classification of primary care codes (PHC presentation data were not available for all patients). An end date of hospital/PHC presentation data collection was set at 1 January 2020 in order to avoid the potential influence of local COVID-19-related measures on hospital and PHC presentations, aside from patients who were deceased prior to this, in which case the end date of hospital collection was set at date of death. From this final date a retrospective 10-year window was applied, excluding all presentations outside of this window. Hospital admissions and PHC presentation data was reported in the following three manners:
A binary variable detailing if the patient ever had a hospital admission/PHC presentation during the 10-year window.
As the total number of hospital admissions/PHC presentations during the 10-year window per patient.
As the rate of hospital admissions/PHC presentations per year per person (calculated as number of presentations divided by the length of time (in years) from the patients first presentation to the collection end date (for this cohort median time between first presentation and the defined end date was 8.9 years (IQR 7.7–9.7)).
Statistical analysis
Demographic and clinical parameters including respiratory presentation rates were presented as medians (IQR), and categorical parameters presented as numbers (%). Presence of airway disease via EMRs, radiology or spirometry was compared between inhaler combinations (SAMA/SABA, LAMA/LABA or +ICS) via two-tailed χ2 test, using Fisher’s exact test in cases with cell counts <10. Differences in the proportion of patients with any respiratory presentation, PHC presentation or hospital admission between inhaler combinations were assessed via two-tailed χ2 tests. Total number of and rate of total respiratory presentations, hospital admissions and PHC presentations between inhaler combinations were tested via Kruskal-Wallis rank test. Univariate and multivariate logistic regression models were used to define the odds of having a hospital admission among patients on SAMA/SABA or LAMA/LABA compared with+ICS (used as the reference group), adjusting for age at the start of the 10-year window, sex, BMI and chronic airway diseases (asthma, bronchiectasis or COPD—in separate models) reporting results as ORs (95% CIs). Univariate and multivariate Poisson regression models were used to define hospital admission rates (number per person per year) among patients on SAMA/SABA or LAMA/LABA compared with +ICS (used as the reference group), using the same models as for the logistic regressions, reporting betas (95% CIs). A secondary subanalysis was conducted looking specifically at hospital admission rates for COPD with lower respiratory tract infection (ICD code J44.0), using the same logistic and Poisson regression models. In cases of patients missing any of the outcome or adjusting variables, they were dropped from the regression models. Alpha was set to p=0.05 throughout, and all analyses were conducted in STATA IC V.15.
Results
Clinical and demographic characteristics
A total of 372 active Aboriginal patients were identified through the respiratory outreach database, of whom 346 (93%) had recorded current use of inhaled pharmacotherapy. The majority of patients were female (64%), with a BMI in the normal or underweight range (58%) and a high proportion reporting a history of smoking (92%). Physician EMR documentation for the presence of chronic airway disease was observed in 97% of the study participants (COPD, bronchiectasis and asthma 92%, 32%,16%, respectively) (table 1) (figure 2). Only a minority of patients were not recorded to have any form of chronic airway disease on EMR (3%, n=12), of whom six had spirometry and four did not show any spirometric impairment.
Patients’ clinical and demographic details
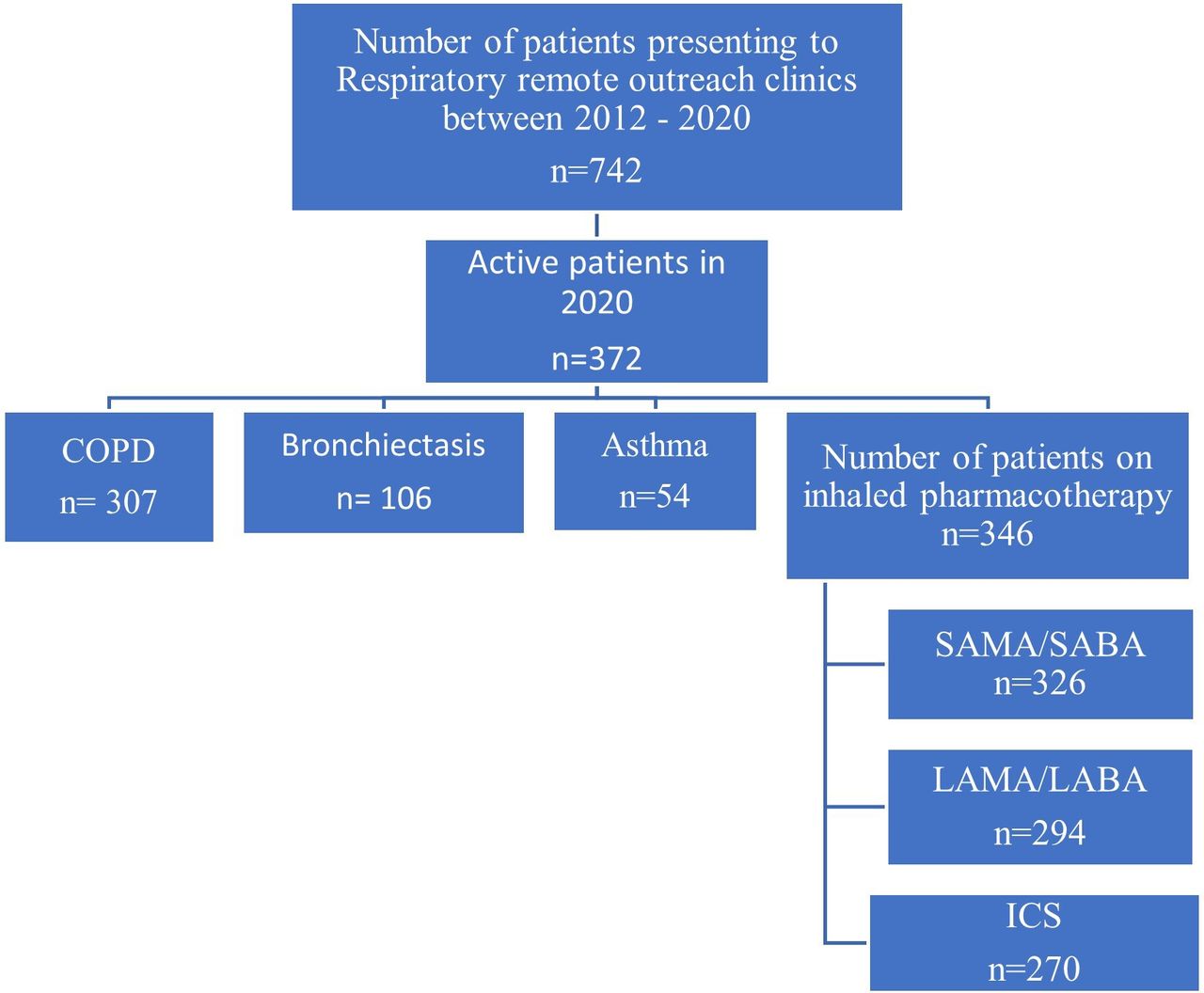
Flow diagram of patient inclusion in study. COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β-agonist; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta agonist; SAMA, short-acting muscarinic antagonist.
Inhaled pharmacotherapy prescription data
Of the 346 patients with an inhaled pharmacotherapy prescription recorded, 326/346 (94%) had SAMA/SABA recorded, and 45/346 (13%) had only either SAMA or SABA recorded, 294/346 (85%) had LAMA/LABA recorded and 31/346 (9%) had only either LAMA or LABA or a combination of LAMA/LABA+SAMA/SABA recorded, and 270/346 (78%) had ICS recorded (figure 3).
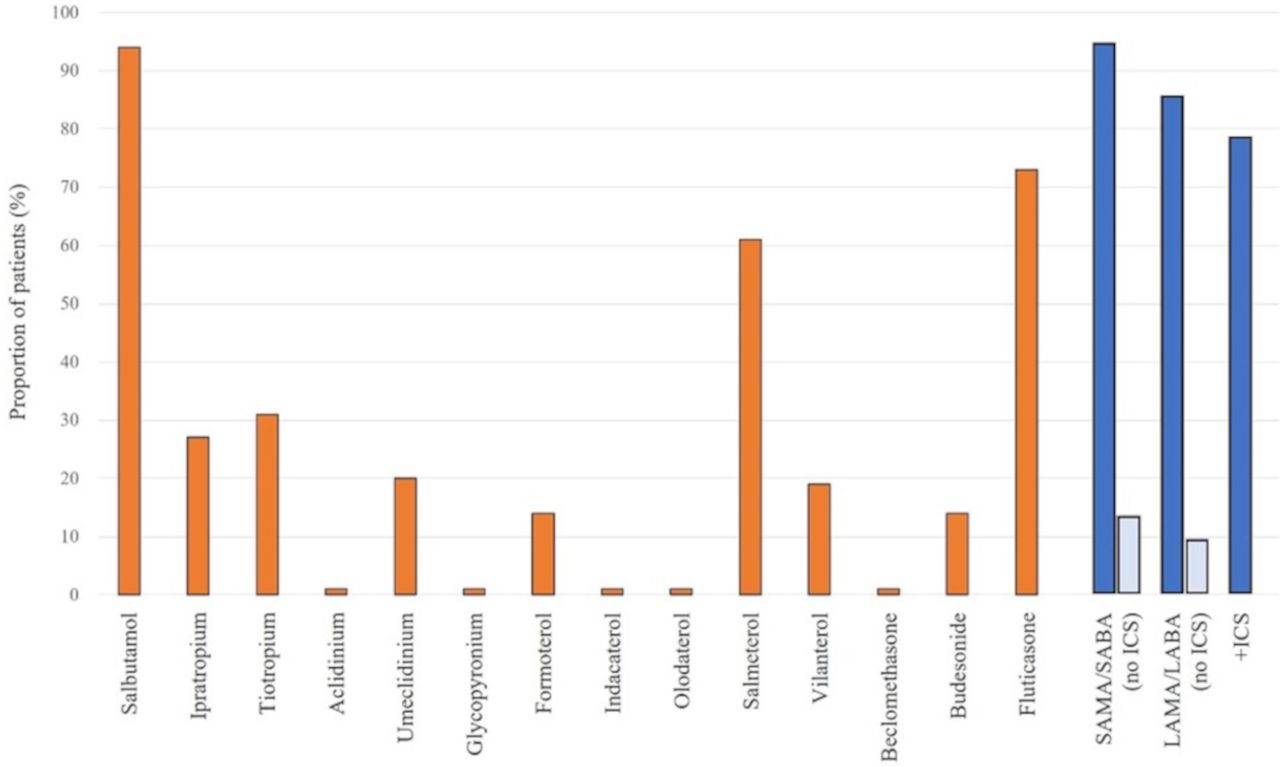
Proportion of patients with individual pharmacotherapy prescriptions, and those grouped by SAMA/SABA, LAMA/LABA or+ICS. ICS, inhaled corticosteroid; LABA, long-acting β-agonist; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta agonist; SAMA, short-acting muscarinic antagonist.
Inhaled pharmacotherapy use as per EMR and chest radiology
COPD was the most common respiratory comorbidity recorded for each of SAMA/SABA, LAMA/LABA and +ICS patients (71% (32/45), 90% (28/31) and 92% (247/270) respectively, Fisher’s exact test p=0.001) (table 2). The majority of patients prescribed LAMA/LABA alone had only COPD listed in their EMRs (71%, 22/31) compared with SAMA/SABA or+ICS patients (51 (23/45) and 50% (136/270), respectively). A greater proportion of+ICS patients, however, had COPD and bronchiectasis listed compared with SAMA/SABA or LAMA/LABA patients (28% (76/270) vs 13% (6/45) and 16% (5/31), respectively).
Inhaler prescriptions by comorbidity as recorded on electronic medical records, or as identified on radiology
Radiology reports were available for 335 patients to determine radiological evidence of airway diseases. COPD was the most common, recorded in 142/335 (42%), with 90/335 (27%) showing bronchiectasis and 46/335 (14%) recording concurrent COPD and bronchiectasis (table 1). Of the 44 patients with isolated bronchiectasis on radiology, the majority (75%, 33/44) had a recorded prescription of+ICS, while among patients with isolated bronchiectasis on EMR (n=12), half (50%, 6/12) had recorded use of+ICS (table 2). This proportion rose to 87% among patients with bronchiectasis plus COPD via EMR (76/87), 50% in plus asthma via EMR (1/2) and 100% in patients with all three present via EMR (5/5). Among patients with radiologically defined bronchiectasis plus COPD the proportion was 78% (36/46). Of the 96 patients with radiologically defined isolated COPD, the majority (85%, 82/96) recorded use of+ICS, as did the majority (75%, 136/181) of those with isolated COPD on EMR.
Inhaled pharmacotherapy use as per pulmonary function test results
The majority of patients (n=283/346, 82%) had spirometry recorded, though 44/283 (16%) did not have post-BD spirometry to assess for AO or BDR, and an additional 12 (total 56/283) were missing percent predicted and percentage change values. However, among the 239 who had both pre-BD and post-BD spirometry values available, there was no significant difference in pre to post values for FEV1/FVC (0.634 (95% CI 0.615 to 0.653) vs 0.636 (95% CI 0.617 to 0.655), p=0.569), therefore pre-BD FEV1/FVC was used for AO in these 44 patients. AOs were common, noted in two-thirds of patients (65%, 183/283), though these often occurred alongside an FVC below the LLN resulting in a mixed impairment (58%, 165/283) (table 3). Only 3% (8/283) of the cohort did not show any evidence of spirometric impairment. A greater proportion of patients with mixed impairment were prescribed with+ICS (85%, 140/165) compared with those with a restrictive impairment (78%, 69/89). A greater proportion of patients with a SAMA/SABA prescription showed no significant impairments on spirometry compared with LAMA/LABA or+ICS (14% (4/29) vs 0 (0/27) and 2% (4/227), respectively (Fisher’s exact p=0.014). A greater proportion of patients with+ICS who showed airway obstruction were at GOLD stages III or IV (88%, 128/146), compared with patients with SAMA/SABA (77%, 10/13) or LAMA/LABA (60%, 9/15). Presence of BDR ‘potential asthma’ was observed in 55 patients (23%, 55/227) on spirometry, with the majority of these patients (80%, 44/55) observed to have a+ICS prescription.
Inhaler prescriptions by spirometry result
Inhaled pharmacotherapy prescription with bronchiectasis
A further analysis was undertaken to understand the pattern of inhaler prescription for the 142 patients with a diagnosis of bronchiectasis (either in EMR or via radiology) (table 4). Among patients with a diagnosis of bronchiectasis, 76% (108/142) had a prescription for +ICS. Breaking it down further, to exclude patients with other potential comorbidities, 29/142 (20%) did not have any evidence of AO, asthma or COPD on radiology. Of these 29 patients, 21 (72%) recorded+ICS prescription. Of the five patients with no evidence of asthma, AO, or COPD via any of spirometry, radiology or recorded in patients’ EMRs, all had a prescription for+ICS. The rate of+ICS prescription among patients with bronchiectasis was comparable to patients with evidence of asthma (78/97) or COPD (249/313) (80% each).
Inhaler use according to underlying airway disease (bronchiectasis)
Inhaled pharmacotherapy prescription relationship to hospital admissions and PHC presentations
Healthcare presentations due to respiratory conditions were common, with 83% (288/346) of patients recording at least one presentation (either PHC or hospital). Hospital admissions were recorded in 58% (201/346) (table 5). Respiratory hospital admissions were significantly more common among patients using +ICS, with 62% (167/270) having at least one hospital admission compared with 52% (16/31) of LAMA/LABA and 40% (18/45) of SAMA/SABA (p=0.017). The total number of presentations was additionally significantly greater among the +ICS group with a median 3 hospital admissions per patient compared with 2 for SAMA/SABA and LAMA/LABA. Furthermore, the median rate of presentations (/person/year) among patients who presented at least once was twice as high among the+ICS group compared with the SAMA/SABA or LAMA/LABA groups (p=0.004). The total number of patients deceased in the ICS group was higher compared with SAMA/SABA or LAMA/LABA groups (n=22/270 (8%) vs n=2/45 (4%) and n=4/31 (13%), respectively). However, with low numbers (<5) in the SAMA/SABA or LAMA/LABA group compared with ICS group, the statistical power is low.
Presentations to PHC or hospital admissions secondary to exacerbation of airway disease or lower respiratory tract infections
Regression analyses for respiratory healthcare presentations/utilisation
In logistic regression models, the odds of having a hospital admission (any of ICD J44-J47) were significantly reduced among patients who were prescribed only SAMA/SABA compared with+ICS, with no significant difference between LAMA/LABA and+ICS (table 6). However, the rate of hospital admissions was significantly reduced among patients on LAMA/LABA compared with+ICS in all adjusted models. In the respiratory disease adjusted models (models A, B and C (models as detailed under table 6)), there was a difference in the effect of the presence of each disease. Presence of asthma did not significantly change the hospitalisation rate (−0.34 (95% CI −0.8 to 0.12)), while presence of bronchiectasis (0.71 (95% CI 0.23 to 1.18)) or presence of COPD (1.01 (95% CI 0.15 to 1.88)) were associated with significantly increased hospitalisation rates. When the model was refined to only COPD admissions with a lower respiratory tract infection (ICD-J44.0), the results remained the same, with patients on+ICS recording a significantly greater rate of hospital admissions than those on LAMA/LABA without ICS. Figure 4 illustrates the inhaled pharmacotherapy prescribing patterns as per clinical, spirometry, radiology, including hospital and PHC presentations.
Logistic and Poisson regression models exploring the effect of inhaler prescription on odds of healthcare presentation and rate of presentations, using patients on +ICS as baseline

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical factors and outcomes of patients by inhaler prescription. AO, airflow obstruction; BDR, bronchodilator response; Br, bronchiectasis; COPD, chronic obstructive pulmonary disease; +ICS, plus inhaled corticosteroids; MI, mixed impairment; PHC, primary healthcare; RI, restrictive impairment; LABA, long-acting β-agonists; LAMA, long-acting muscarinic antagonists; LRTI, lower respiratory tract infection; SABA, short-acting bronchodilators; SAMA, short-acting muscarinic antagonists.
Discussion
To the best of the authors’ knowledge, this is the first study that used clinical, spirometry and radiology data to comprehensively assess the prescribing pattern of inhaled pharmacotherapy and its related outcomes in an Aboriginal Australian population with chronic airway disease. This study highlights several key findings:
Almost 93% of remote residing Aboriginal patients with chronic respiratory conditions who were referred to the respiratory and sleep outreach service were noted to have been prescribed with one form or another airway directed inhaled pharmacotherapy.
ICS containing inhaled pharmacotherapy was by far the most frequently prescribed inhaled pharmacotherapy.
COPD was the most common condition recorded among study patients prescribed with inhaled pharmacotherapy, with the majority being prescribed LAMA or LABA either alone or in conjunction with ICS.
Irrespective of what impairment was observed on spirometry, ICS containing inhaled pharmacotherapy prescription is the most common.
ICS was observed to be prescribed in up to 76% of patients with bronchiectasis.
Patients with a prescription of ICS showed almost double the hospital admission rate, especially with COPD or bronchiectasis compared with asthma.
ICS prescription was also significantly associated with increased hospital admission rates secondary to lower respiratory tract infections.
Despite overwhelming evidence in the literature to indicate that chronic airway diseases are highly prevalent among Aboriginal/Indigenous people, not only among Aboriginal Australians,4–8 but also among other Indigenous people globally,31–36 there is little evidence in the literature examining the efficacy, safety or prescribing patterns and related outcomes of inhaled pharmacotherapy. Hence, the current study addresses this gap in knowledge and could be viewed as an invaluable addition to the literature.
In this study, we observed that COPD was the most common condition among patients being prescribed inhaled pharmacotherapy. This is not surprising though, as it reflects the high prevalence of COPD in the remote residing NT Aboriginal population, as well as the high smoking rates (>90%) noted in the current and previous studies.4–6 While there is evidence to suggest either LAMA or LABA in combination or in isolation are beneficial in the management of patients with COPD,37–39 the use of ICS in the management of patients with COPD is controversial and continues to be debated.40–42 In our study, the majority of patients diagnosed with COPD were observed to be prescribed with LAMA/LABA containing inhaled pharmacotherapy, in line with the beneficial outcomes noted in previous reports.37–39 However, a significant proportion of patients with COPD were also noted to be prescribed with ICS.
Among patients presenting with chronic airway diseases, spirometry alongside other clinical parameters, including exacerbation frequency are often used in clinical decision making, including when considering inhaled pharmacotherapy in day-to-day clinical practice.17 18 In the absence of spirometry reference norms among adult Indigenous people,43 there are substantial challenges in the accurate diagnosis and classification of the severity of airway disease,44 45 in order to guide inhaled pharmacotherapy appropriately. Health practitioners caring for Indigenous/Aboriginal people undoubtably rely on and adopt evidence established in non-Aboriginal/Indigenous ethnic populations that may or may not be appropriate for Indigenous/Aboriginal people. A previous study from our centre found that among Aboriginal patients with COPD, irrespective of which severity classification is used (GOLD, COPD-X or Global lung function initiative-2012), the majority of patients will likely be classified as having either severe or very severe disease.46 Hence why, with spirometry demonstrating a high proportion of patients classified to have severe COPD, and in line with current recommended guidelines,20 we observed a significant proportion of patients with COPD having an ICS prescription. However, a recent study has demonstrated that there could be excessive decline in lung function parameters, in particular for FEV1 values, associated with ICS use among Aboriginal Australians with chronic airway diseases.47 Hence, caution has to be exercised while considering ICS containing pharmacotherapy among an Aboriginal Australian population with a high prevalence of concomitant airway disease.
Use of inhaled pharmacotherapy may be appropriate among patients with asthma or selected patients with COPD,16–21 yet among those with bronchiectasis, consensus guidelines are far more individualised and depend on the frequency of exacerbations, prior medication response and comorbidity of asthma and/or COPD.48–51 As ICS reduces the local (pulmonary) immune response, there is potential for deleterious effect of ICS use among patients with bronchiectasis, as the disease is typically underlined by long term bacterial colonisation, perpetuating a vicious cycle of recurrent infective exacerbations and further airway inflammation, alongside a decline in lung function, which may be exacerbated by long term use of ICS.47 52 In our study, we noted a significant proportion of patients with underlying bronchiectasis had ICS prescribed—even in the absence of evidence of comorbid lung conditions—and moreover, patients prescribed with ICS had higher rates of hospital presentations. Hence, it may be reasonable to presume the overlap of bronchiectasis and ICS prescription could be at least partially driving the higher hospital admission rates seen among our patients. Contrary to international guidelines recommending against the use of ICS among patients with bronchiectasis unless there are clear clinical justification,53 ICS containing pharmacotherapy continues to be prescribed frequently/liberally even among the non-Aboriginal Australian population,54 with data suggesting unprecedently 6.3% of Australians have a current ICS prescription,55 potentially inappropriately in certain circumstances. Furthermore, more recent studies have raised serious concerns in relation to ICS use and its association with risk of pneumonia among patients with airway diseases, more specifically with fluticasone containing inhaled pharmacotherapy.56–59 The results of our study potentially add to this body of evidence, with the high rate of hospitalisations among patients with a prescription of ICS, and fluticasone was by far the single most prescribed ICS among our study participants.
The current study also found that ICS prescription, regardless of underlying respiratory condition, was associated with significantly higher overall hospital admission rates and more specifically with higher COPD with lower respiratory tract infection admission rates (ICD-J44.0), in particular in the presence of bronchiectasis. Due to the retrospective study design, we cannot ascertain if ICS prescription contributed to excessive hospital admission rates or if the excessive hospital admission rates triggered ICS prescriptions, and nor could the exact point of initiation of therapy compared with hospital or PHC presentations be determined accurately. Nonetheless, healthcare utilisation for respiratory disorders is generally observed to be higher for Indigenous people globally, especially in high-income countries such as Australia, New Zealand and Canada.14 60–62 It is unclear at this stage if the high healthcare utilisation rates observed are related to the adoption of therapeutic interventions established among non-Aboriginal/Indigenous populations, or if it is related to a higher prevalence of chronic and more severe respiratory disease burden.
Nevertheless, in the Australian context, it appears that inhaled pharmacotherapy is liberally and extensively used to treat chronic airway diseases among Aboriginal Australians, despite the lack of clear evidence or guidelines. Several previous studies have reported on the use of airway directed inhaled pharmacotherapy in other ethnic populations, indeed highlighting rather inappropriate prescribing patterns on several fronts, more particularly in the excessive use of ICS among patients with airway disease, including at the PHC level.63–66 This trend appears to be true for the current study, as we noted that inhaled pharmacotherapy prescribing patterns did not clearly align with spirometry results, particularly among patients demonstrating restrictive or mixed impairments. This is despite the Australian rural guidelines manual (CARPA) recommending to consider ICS only if the spirometry demonstrates BDR among patients with bronchiectasis.51 It is imperative to acknowledge that there are substantial differences in the way in which respiratory diseases manifests in Aboriginal people in comparison to non-Aboriginal Australian counterparts.67–77 In this vein, recent studies have recommended to take a personalised and tailored approach, by adopting clinical, spirometry and radiology in the accurate diagnosis, alongside advocating cautious use of inhaled pharmacotherapy in the management of chronic respiratory conditions among Aboriginal people.47 78 Moreover, following locally developed prescribing guidelines that have been specifically developed for patients residing in remote and rural communities is vital,51 in order to reduce treatment emergent morbidity and mortality.42 59 Currently, there is limited access to comprehensive medication review services for Aboriginal people79 and in remote communities.80 Studies have shown that the involvement of Aboriginal Health Workers and Consultant pharmacists can have a positive impact on appropriate prescribing patterns.81 82 These types of services could be established and evaluated in this setting.
Limitations
The authors acknowledge that this study has several limitations. The participants included in this study were drawn from referred patients to a specialist respiratory service in the TEHS region of the NT, hence, the outcomes represented in this study cannot be generalised, neither to other Aboriginal Australians residing in the NT nor to those living in other Australian states or territory or Indigenous people globally. The reason we observed a high proportion of patients being on inhaled pharmacotherapy is likely related to this. Moreover, medication adherence data were not available to be assessed, which would have had an impact on hospital and PHC presentations. Furthermore, spirometry, radiology and pharmacotherapy prescriptions did not all occur at the same time point, but rather were spread through the study window, and indeed some patients may have swapped between therapies and dosages in this time period, including during exacerbations, thus curtailing the potential for this study to truly assess any time course effect. In addition, medical services provision for patients residing in remote communities can be variable and transient, swapping between primary/visiting general practitioners/visiting specialist health work force, hence, choice and treatment initiation or ceasing are often dependent on the individual medical practitioner’s discretion. On a similar note, we did not collect data on length of hospital admission or care provided during hospital admissions, which may have affected propensity for future visits, nor the exacerbation history of the patient which limits our ability to define the appropriateness of+ICS prescription. In other underserved populations medication sharing is commonly reported, however, whether this is the case in the current population and study sample is not known. We also did not include or compare the prescribing practice between Aboriginal and non-Aboriginal patients in this study, in order not to introduce bias. As such, previous studies have demonstrated significant difference in the way chronic respiratory diseases manifests Aboriginal patients compared with non-Aboriginal Australians. Nevertheless, this is the first study to assess the prescription and associations of inhaled pharmacotherapy in a predominantly adult Aboriginal Australian population, highlighting opportunities for prospective further research to exploring avenues in the better management of chronic respiratory conditions.
Conclusion
This study has demonstrated that airway directed inhaled pharmacotherapy was observed to be substantially used in the management of chronic airway diseases among Aboriginal patients being referred to the respiratory service in the NT. ICS containing inhaled pharmacotherapy appears to be prescribed extensively, rather inappropriately in certain respiratory conditions, which may be detrimental for overall outcomes. Strategies are required for advocating appropriate inhaled pharmacotherapy prescribing practice among Aboriginal people with chronic airway diseases.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Human Research Ethics governance/committee of the NT, TEHS and Menzies School of Health Research (Reference: HREC 2020-3840).
Acknowledgments
We sincerely thank Mrs Raelene L Messenger, respiratory clinical nurse consultant respiratory form RDH and Ms Ara Joy Perez form DRSH/DPH in contributing towards this study. We also extend our sincere appreciation to our Aboriginal health workers and primary care physicians in co-ordinating respiratory care for Aboriginal people residing in the TEHS region of the NT of Australia. We also thank the division of medicine and the research committee members at RDH for supporting funding for this study.
References
Footnotes
Contributors All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. SH is the guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study received internal funding/support from the Division of Medicine, Royal Darwin Hospital, Darwin, Australia.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.