Article Text

Abstract
Introduction Accurate tuberculosis (TB) incidence and optimal surveillance strategies are pertinent to TB vaccine trial design. Infants are a targeted population for new TB vaccines, but data from India, with the highest global burden of TB cases, is limited.
Methods In a population-based prospective trial conducted between November 2006 and July 2008, BCG-vaccinated neonates in South India were enrolled and cluster-randomised to active or passive surveillance. We assessed the influence of surveillance strategy on TB incidence, case-finding rates and all-cause mortality. Predefined criteria were used to diagnose TB. All deaths were evaluated using a verbal autopsy.
Results 4382 children contributed to 8164 person-years (py) of follow-up (loss to follow-up 6.9%); 749 children were admitted for TB evaluation (active surveillance: 641; passive surveillance: 108). The TB incidence was 159.2/100 000 py and the overall case-finding rate was 3.19 per 100 py (95% CI 0.82 to 18.1). Whereas, the case-finding rate for definite TB was similar using active or passive case finding, the case-finding rate for probable TB was 1.92/100 py (95% CI 0.83 to 3.78) with active surveillance, significantly higher than 0.3/100 py (95% CI 0.01 to 1.39, p=0.02) with passive surveillance. Compared to passive surveillance, children with active surveillance had decreased risk of dying (OR 0.68, 95%CI 0.47 to 0.98) which was mostly attributable to reduction of death from pneumonia/respiratory infections (OR 0.34, 95%CI 0.14 to 0.80).
Conclusion We provide reliable estimates of TB incidence in South Indian children <2 years of age. Active surveillance increased the case-finding rates for probable TB and was associated with reduced all-cause mortality.
- tuberculosis
- respiratory infection
- clinical epidemiology
- paediatric lung disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
Accurate data on tuberculosis (TB) incidence in infants in India, a country with the highest global burden of TB cases, and information on optimal surveillance strategies is pertinent to designing TB vaccine trials.
The overall TB case-finding rate was 3.19 per 100 person-years (95% CI 0.82 to 18.1). Active surveillance increased the case-finding rates for probable TB and was associated with reduced all-cause mortality.
The results inform the monitoring of TB in a high-risk population and the planning of TB vaccine trials and other prevention strategies in Indian infants and in other high-burden TB settings.
Introduction
Accurate tuberculosis (TB) incidence estimates in children are essential in addressing the TB epidemic: (1) to guide and evaluate programmes of TB control and (2) for planning and evaluation of TB vaccine trials conducted in this age group.1 However, many countries do not require notification of TB in children given the paucibacillary nature of childhood TB, associated diagnostic challenges2 and the assumed reduced risk of transmission. These issues have resulted in a lower priority for case finding, diagnosis and treatment of paediatric TB by the WHO and by National TB Control Programs (NTCP). More recently the WHO has called for more accurate estimates of the burden of TB in children,3 including TB incidence in children aged <5 years, since young children have a high risk of developing TB following Mycobacterium tuberculosis (MTB) infection.2 Efficacious TB vaccines are urgently needed in children as the BCG vaccine has demonstrated variable efficacy in different populations in preventing MTB infection and disease progression.4 Reliable estimates of TB incidence in target populations and efficacy estimates of TB vaccine candidates depend on notification of true TB cases, which is best achieved through prospective cohort studies; globally, few studies have been conducted.5 6 Sample size estimates for vaccine trials depend on accurate surveillance and optimised case detection. This was addressed by the South African Tuberculosis Vaccine Initiative (SATVI) in a neonatal cohort study using active and passive surveillance similar to the present study.7
New TB vaccine candidates should be tested in India as a priority, given that India has the largest number of estimated incident TB cases globally (2.79 million)8 and bears 27% of the estimated burden of paediatric TB cases of the 22 high-endemic countries.9 India does not meet the global target for case detection and rates among 10 countries which account for 76% of the gap between case notification rates and estimated incidence.8 Furthermore, the models for TB incidence rates in children do not take into account specific predisposing factors in Indian children, including high burden of malnutrition,10 suggesting an overall underestimation of TB cases.
Our main objective was therefore to determine the TB incidence between birth and 2 years of age in children vaccinated at birth with BCG. Furthermore, we hypothesised that TB case-finding rates and the clinical presentation of TB disease is influenced by surveillance strategy. We therefore conducted a population-based prospective trial of neonates cluster randomised to bimonthly home visits (active surveillance) or parental seeking of healthcare after education (passive surveillance) in Southern India. In the context of a large prospective trial of a vulnerable group with known high mortality, our secondary objective was to assess the impact of surveillance strategy on all-cause mortality.
Methods
Trial design
A prospective stratified cluster randomised trial with enrolment between November 2006 and July 2008. The study close-out was completed September 2010.
Trial setting
This study was conducted in Palamaner, Chittoor District, Andhra Pradesh, India, a study area covering a population of approximately 400 000 in 800 villages and 4 towns, where resident women were estimated to give birth to 4000–4500 neonates annually. The study area had 13 primary healthcare centres, 2 subdistrict level government hospitals, 4 private nursing homes/hospitals, 5 TB microscopy centres, 3 Directly Observed Treatment (DOT) centres and a private medical college hospital. A study-specific Case Verification Ward (CVW) was established at Emmaus Swiss Referral Hospital. The HIV prevalence in women attending antenatal clinics was 0.53% in 2012.11 BCG vaccination is recommended for children below 1 month of age,12 and coverage is above 90% in all populations of children<2 years except within the Muslim minority (81.4%).13 Pregnant women within the study area were identified antenatally and informed about the study (n=7424).
Eligibility and surveillance for all participants
Neonates were eligible if they received routine BCG vaccine I.P. (Serum Institute of India, Pune) within 72 hours of birth (0.05 mL administered intradermally by the study team) and their families had no intention to move. All parents/caretakers were educated about TB-related symptoms and encouraged to contact a study worker or visit the CVW (transportation free of cost), if their children developed symptoms suggestive of TB or were exposed to a TB case.
Admissions and deaths at health centres within the study area and in referral hospitals in close proximity were screened weekly by the study team.
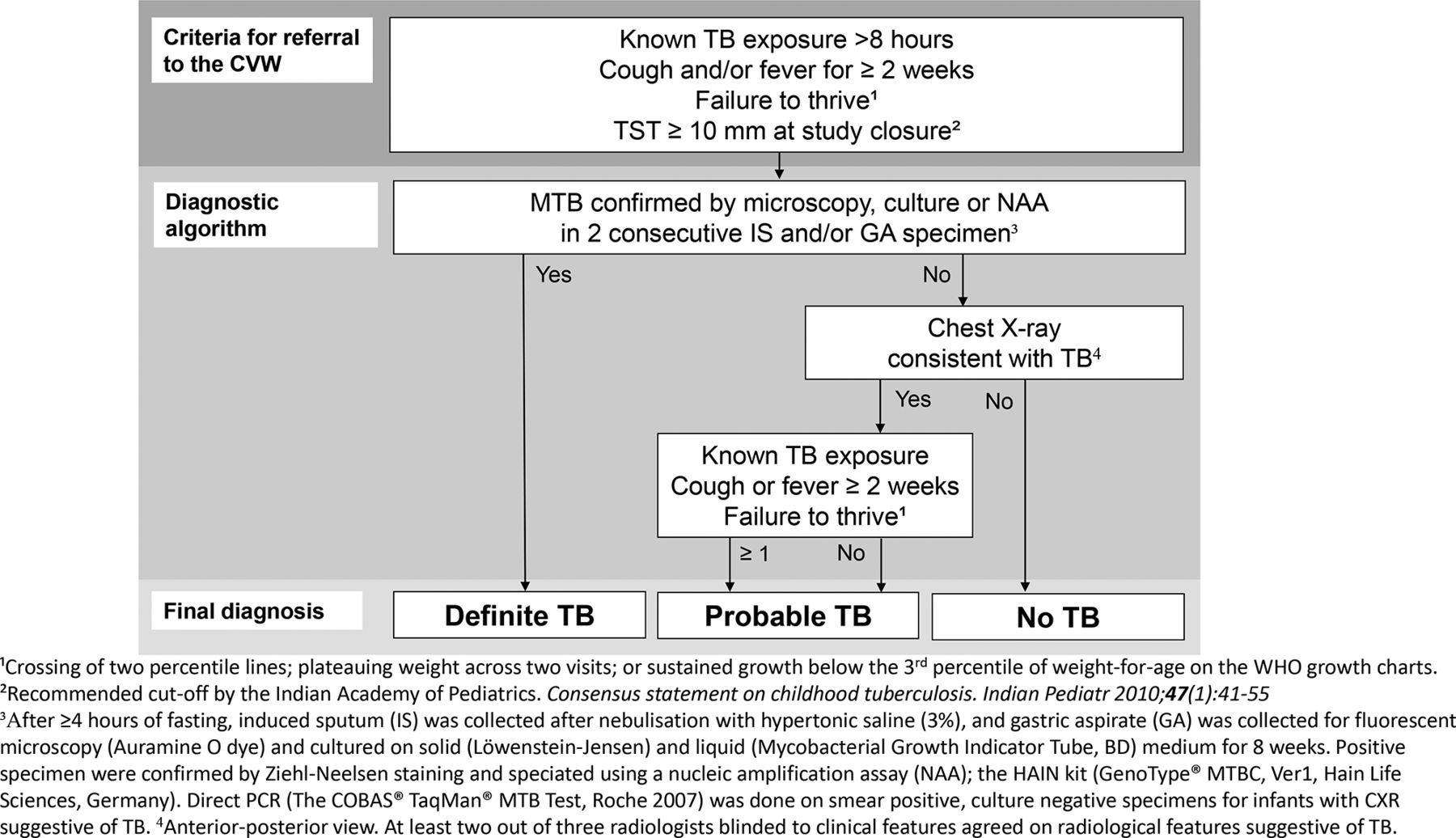
The close-out visit (day 720) included a Tuberculin Skin Test (TST) and screening for defined referral criteria (figure 1), when if present led to a full diagnostic assessment at the CVW.14 This included assessment of symptoms, clinical examination including anthropometry, chest X-ray and collection of microbiological specimens (induced sputum and gastric aspirates collected on two consecutive days) and a TST (figure 1). For children who died during the study period, a verbal autopsy (a questionnaire modified from a previous Indian study;15 online supplementary file 1) assessed probable cause of death if the parents/caretakers consented.
Supplemental material
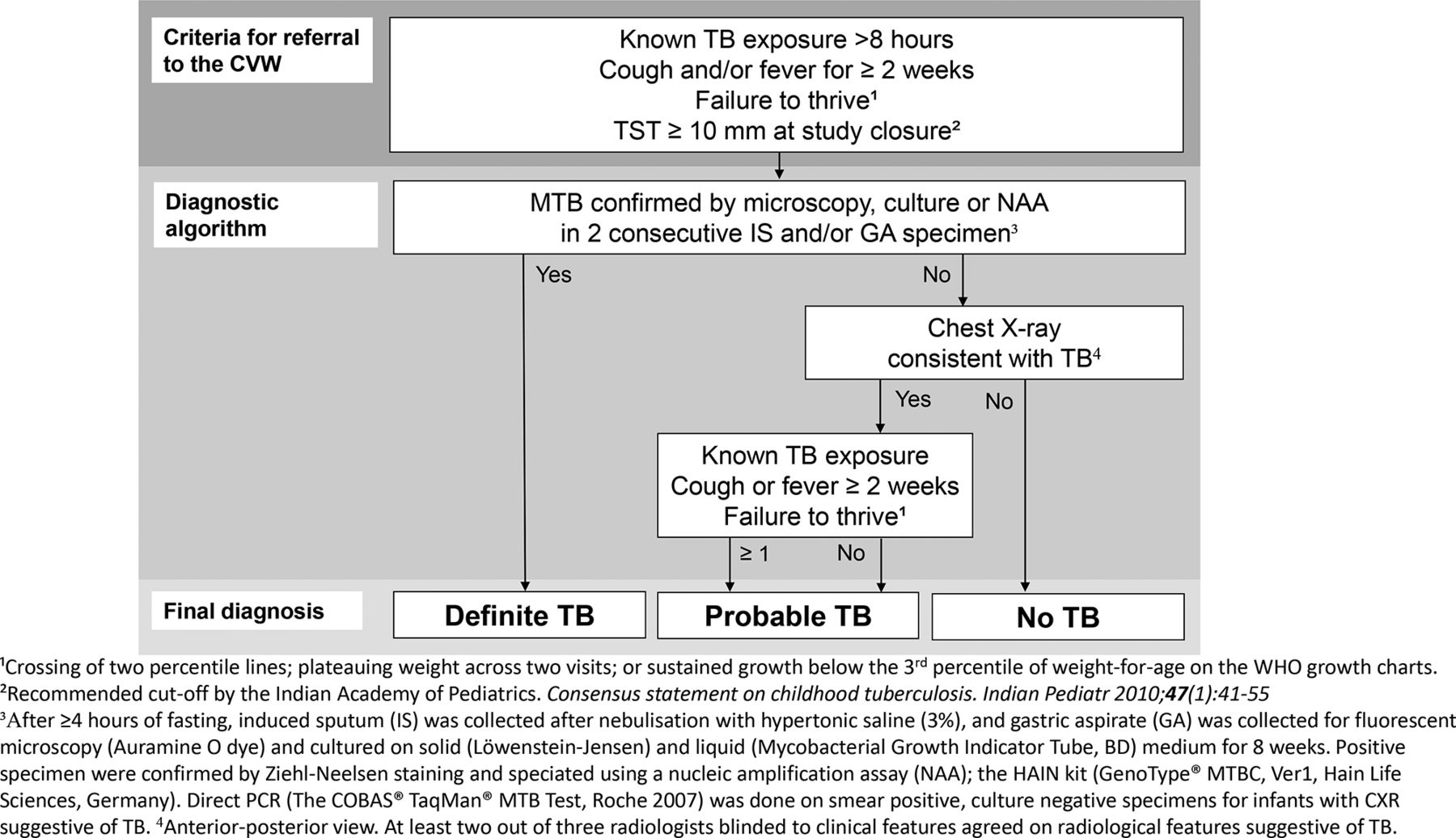
Criteria for referral to the CVW at Emmaus Swiss Hospital, Palamaner (CVW) and the diagnostic algorithm applied for the classification of definite (confirmed) and probable (unconfirmed) TB. CVW, Case Verification Ward; GA, gastric aspirate; MTB, Mycobacterium tuberculosis; NAA, nucleic amplification assay; TB, tuberculosis; TST, Tuberculin Skin Test;
Type of surveillance
Both arms included parental education about TB symptoms at inclusion. Trained study field workers16 supported each of the two surveillance arms:
Active surveillance: At a bimonthly home visit, a study field worker enquired about TB-related symptoms and recent TB exposure, recorded the weight of the child (calibrated spring balance) on a WHO gender-specific growth chart.17 If referral criteria14 were present, the field worker encouraged, repeatedly if needed, that the parent/caretaker brings the child to the CVW.
Passive surveillance: No home visits were performed.
Randomisation
Stratified cluster randomisation was chosen in order to avoid migration from passive to active surveillance while ensuring a balance between different levels of development of villages and population sizes. A total of eight strata were defined according to the level of development of villages and population size: (1) rural-high small, (2) rural-high medium, (3) rural-high large, (4) rural-low small, (5) rural-low medium, (6) rural-low large, (7) urban-medium and (8) urban-large. Each stratum had its own randomisation list. Within each stratum clusters were defined as population units consisting of villages or subsections of towns (based on Census of India divisions). A total of 592 clusters were used (see online supplementary file 2). Within each stratum, clusters were manually picked (‘out-of-a-hat’) and alternately allocated to active and passive surveillance by two field supervisors according to the corresponding randomisation list.
Outcomes
Based on a predefined diagnostic algorithm (figure 1), the children were classified as having definite TB, probable TB or no TB using a diagnostic algorithm,14 similar to that of the neonatal study conducted by SATVI.7 Definite and probable TB cases constituted the primary outcome ‘all TB cases’. All children given a diagnosis of definite or probable TB were referred to the RNTCP for treatment. MTB infection as judged by TST was performed in admitted children and per protocol on the close-out visit as described and judged positive if ≥10 mm as recommended by Indian guidelines.18
Sample size
No formal sample size calculation was performed for the outcomes definite/probable TB and MTB infection, due to the lack of reliable data on TB incidence in both adults and children in the district in 2006 when the study was initiated. Preliminary results from a similar study in South Africa showed a risk of definite TB in neonates of 2.3%.7 The overall reported TB incidence in South Africa was ~3.5 times the incidence in India,19 translating into >25 expected TB cases in the present target cohort of 4000–4500 neonates.
Parents/caretakers gave written consent for their children to be enrolled.16 Additional consent was obtained for the diagnostic procedures undertaken.
Data management and statistical analysis
Data were entered on case report forms (CRFs) and checked for completeness and double-entered into a customised data management software (using the Microsoft SQL server (MS-SQL 2000) and ASP.Net as the programming tool). Any data mismatch was resolved against the original CRF. A final 10% quality check was performed prior to import into Microsoft Excel and SPSS (V.23) for analysis.
Baseline characteristics of birth and socioeconomic status (SES), data on TB exposure, TST and attrition rate were summarised as counts and percentages. Variables recording housing material and cooking fuel were dichotomised (bricks vs others; electricity or gas vs others, respectively). Intervention groups were compared in the entire cohort by means of Pearson χ² tests.
Differences between surveillance arms in clinical characteristics at the CVW, admission and referral criteria, study drop-outs (all reasons), causes of death and prevalence of MTB infection, were analysed using logistic mixed-effects regression models including adjustments for cluster-specific random effects and fixed effects of age (only at the time of the CVW visit), gender, religion and father’s education (as assessed by literacy) and fuel. Results were reported as OR with corresponding 95% CI. Mean follow-up times were compared using a similar linear mixed model.
The TB case-finding rates were calculated using Poisson regression and person-years (py) of follow-up. Py were calculated from the date of birth until the date of TB diagnosis, death, close-out visit or withdrawal, whichever event came first. For participants lost to follow-up, py were calculated as midway between the last contact date and date of the next expected visit. Sensitivity analyses under various assumptions about length of follow-up and TB status were also performed.
Results
Birth and socioeconomic characteristics in the study cohort
Of the eligible neonates, 4 872 had parents available for consent query within 15 days of birth. Non-availability for consent was largely due to the practice of women travelling to their mother’s homes to deliver. The 4382 participants, who enrolled, corresponded to a response rate of ~90%. Of these 2215 neonates were cluster randomised to active and 2167 neonates to passive 2-year surveillance (figure 2) and 2276 (51.9%) were boys. Cluster randomisation succeeded in similar distributions of most baseline characteristics between the surveillance groups. However, the passive surveillance group contained more Hindus (p<0.001), lower paternal literacy (p=0.002) and higher use of wood/agricultural residues for fuel (p<0.001) (table 1).
Distribution of birth and socioeconomic characteristics at enrolment in the intervention arms

{kind=link}
{kind=link}
Flowchart for enrolment in the Neonatal Cohort Study. CVW, Case Verification Ward.
Study attrition
Of the enrolled children, 90.4% completed the 2-year follow-up, corresponding to a study attrition rate of 9.6% (table 2). Mean follow-up time was 22 months (SD 4.25), but influenced by surveillance strategy when adjusted for SES factors (mean 22.2 (active) vs 21.8 (passive), estimate −0.39, SE 0.13, 95% CI −0.65 to −0.14).
Study attrition in total and within each surveillance arm
Characteristics of children evaluated for TB during the study period
Referral and admission was seven times more likely under active compared with passive surveillance (ORreferral 7.38, 95% CI 6.21 to 8.77; ORadmission 7.9, 95% CI 6.37 to 9.79). The major difference in referral and admission rates between the active vs passive surveillance arms was accounted for by those children referred with failure to thrive (FTT) (33.5% of those referred were not admitted); children with FTT in the passive surveillance arm were less likely to be brought to the CVW by their parents/caretakers. Otherwise, the referral criteria were evenly distributed within the surveillance arms.
Children in the passive surveillance arm were evaluated at an older age than children in the active surveillance arm (mean age 20.3 vs 13.3 months, estimate 7.31, 95% CI 6.20 to 8.42), were four times more likely to have FTT and less likely to have known TB exposure, abnormal chest X-ray and TST ≥10 mm (online supplementary file 3).
TB incidence and case-finding rates in the surveillance groups
TB was confirmed in four children and probable TB was diagnosed in nine children. The distributions of TB cases for the surveillance arms are given in table 3. Based on 8164 py (active: 4166 py, passive: 3998 py), the estimated overall TB incidence was 159.2 per 100 000 (95% CI 92.5 to 274.1). The overall case-finding rate was 3.19 per 100 py (95% CI 0.82 to 18.1, p=0.06). Whereas the case-finding rate for definite TB was similar between surveillance groups, the case-finding rate for probable TB was significantly higher with active surveillance (1.92/100 vs 0.3/100 py, p=0.02).
Rates of TB case-finding and all-cause deaths by randomisation group*
The four sensitivity analyses gave very similar results, with case-finding rates ranging from 0.73 to 3.27 py (none of the p<0.05; online supplementary file 4).
Prevalence of MTB infection in the cohort at study closure
In the 3961 children completing the study, the prevalence of MTB infection as judged by a TST ≥10 mm18 was 2.9% in the entire cohort and comparable between the surveillance arms, despite TB exposure more frequently being reported in the active surveillance arm (3.8% vs 1.4%, OR 3.02, 95% CI 1.95 to 4.67).
Mortality
Out of 120 children who died, the causes of death were evaluated by verbal autopsy in 110 children. Neonatal deaths (within 27 days of birth) and postnatal deaths (≥28 days from birth) constituted 23.3% and 76.7% of deaths, respectively. Children with active surveillance had reduced risk of dying and were less frequently lost to follow-up (table 2).
Furthermore, the death-rate was reduced in active surveillance and this was mostly attributable to reduction of death from pneumonia/respiratory infections (OR 0.34, 95% CI 0.14 to 0.80; online supplementary file 5) . Notably, only one of the children who died had known TB exposure. This child was evaluated at the CVW at the age of 5 months because of respiratory symptoms (TST 4 mm, CXR normal, neg IS/GA specimen), 17 months before death.
Discussion
To design and implement adequately powered trials of novel TB vaccine candidates, local, accurate estimates of TB incidence are required. The present study is the first to estimate the TB incidence among a general Indian population <3 years of age and to evaluate the impact of active versus passive TB case finding using prospective community-based cohort methods. Based on 8164 py, the cumulative overall TB incidence (definite and probable cases pooled) was 159.2 per 100 000 py. Active surveillance increased the detection of probable TB cases and reduced all-cause mortality, specifically deaths attributable to respiratory infections.
The likelihood of being referred and admitted was almost 7–8 times higher in children in the active compared with the passive surveillance arms. We expected that active surveillance with bimonthly home visits would result in the identification of more children meeting the defined referral criteria by regular weighing and by reducing the threshold for referral. Nevertheless, we were surprised that the effect observed in our study was more pronounced than in the SATVI study.7 This might be explained by a generally lower educational level (primary school or lower) in Indian mothers in this study (59%) compared with South African mothers in the SATVI study (26%)7 or other factors. Similar to Moyo et al,7 we found a higher case-finding rate of probable TB cases in the active compared with the passive surveillance arms likely resulting from active surveillance facilitating earlier diagnosis of TB and even diagnosis of early or incipient disease.2 20 21 More definite TB cases could then be expected to develop in the context of passive surveillance and notified at study closure. Despite examination for TB in all children at study closure, this was not observed. Notably, the prevalence of MTB infection was similar in the active and passive surveillance arms, rendering a bias from lower SES in the passive surveillance arm on TB incidence estimates unlikely. Although we cannot verify whether the uneven distribution of probable cases represents a combination of overdiagnosis within the active and underdiagnosis within the passive surveillance arms, we think it unlikely that we have overestimated the incidence of total TB cases. The diagnostic algorithm for probable TB in the study relied on the approach used by SATVI.5 7 More stringent criteria for case definition of microbiologically unconfirmed cases have been suggested in more recent studies6 and introduced in consensus guidelines.22 We acknowledge that reduced pretest probability for TB in our Indian cohort compared with South African cohorts is likely to have affected the accuracy of the diagnostic algorithm. Furthermore, there is the possibility that some children diagnosed with probable TB had symptoms of initial MTB infection which would have eventually resolved spontaneously.2 23 Notably, we previously found significant differences in the expression of transcriptional biomarkers between children from the present cohort diagnosed with either clinical TB, MTB infection and controls,24 which strengthens the appropriateness of the diagnostic algorithm applied. Even though there might be misclassification of cases in the present study, probable TB cases are expected to constitute about 70% of TB cases in young children2 which corresponds precisely to the proportion in the current study. It is also worth noting that the diagnostic procedures and algorithm focused on pulmonary TB implying a risk of underdiagnosing extrapulmonary TB which was reported in 8.2% of HIV-uninfected South African children aged <3 years. Of interest, two studies conducted in the context of vaccine trials found the cumulative incidence of TB in BCG-vaccinated children<2 years was approximately 3%.5 6 In a more recent prospective study covering a population of 13 764 children<3 years in Southern Mozambique, presumptive TB cases (13.2% HIV positive) were identified by passive and/or active case-finding. The incidence for definite TB was 135 per 100 000 py.23 An interesting similarity between our Indian cohort and the Mozambican study was the burden of malnutrition, but in general, it appears that the epidemiological situation in most African countries is not directly comparable to India. Clearly, the HIV epidemic has influenced TB incidence even in HIV-uninfected children by left-skewing the TB epidemiological age curve in areas of high HIV prevalence.2 In our Indian cohort, however, the impact of HIV infection is presumably very low.11 In this context, the incidence of definite TB in our Indian cohort of 49 per 100 000 population could be considered to be higher than expected.
An important finding in this study is the reduced all-cause mortality in children with active compared with passive surveillance. This was true both when assessing mortality with case-rates per 100 py (no adjustments made) and with ORs adjusted for relevant SES variables. Previous studies support an impact of outreach health programmes on infant health.25 Multiple interventions judged effective in reducing infant mortality26 were provided by our study team, regardless of surveillance. These included an increased number of healthcare workers (HCW) in the study area who visited women before and after delivery encouraging an institutional delivery and attendance to the recommended antenatal visits and immunisation programmes for their infants. But as the HCW were instructed to continue to deliver these health messages throughout the study, it is likely that mothers/caretakers of children within the active surveillance arm received these messages to a greater extent. Interestingly, when stratifying the cause of mortality, only the risk of dying attributable to pneumonia/respiratory infections were significantly reduced with active surveillance. This is likely explained by the focus on TB and respiratory symptoms.
The strengths of the present study are the large number of neonates enrolled in a community-based study, its standardised procedures for referral and diagnosis,5 7 balance between the two surveillance arms with regard to similar TB exposure and infection rates and low attrition. Assessment of active and passive surveillance also allowed for evaluation of the effect of follow-up strategy on the detection of TB cases. Lower SES, present in the families/households of children in the passive surveillance arm, is a well-established risk factor for TB disease27 and mortality26 but by adjusting for differentially distributed variables (eg, religion, parental education and fuel for cooking) in the two surveillance arms, except for in the case-rate calculations, we reduce the risk of residual confounding. Use of cluster randomisation is a limitation, as it may not achieve similar distributions of variables in the two arms as easily as for individual randomisation; if possible, future studies should use more, smaller clusters. Lack of data on outcome of patients with TB due to referral to the RNTCP for treatment is also a limitation as we cannot ascertain whether children classified as probable TB truly had symptoms of initial MTB infection or other respiratory infections, which would have resolved spontaneously,23 or with antibiotic treatment.22 Based on this, we suggest that children put on treatment for assumed TB or other (respiratory) disease be followed up in future studies aiming to more firmly estimate TB incidence in young children.
In conclusion, we have established the TB incidence in an important target population for new TB vaccines: children<3 years in a typical rural district in Southern India in a community-based prospective cohort study of neonates. Active surveillance with regular home visits seems to be most appropriate in order to detect probable TB cases, which represent the most common presentation of TB in young children. Active surveillance was also associated with the benefit of reduced all-cause mortality in a vulnerable population, mostly due to respiratory infections, one of the main child killers globally.28
Acknowledgments
Larry Geiter, Sean Bennett, Lew Barker, and Robert Walker, previously at Aeras, and John Kenneth previously at St. Johns’ Research Institute, Bangalore, India. Study physicians, field and lab workers in the Palamaner Study Field Site and at St. Johns’ Research Institute, India.
References
Footnotes
Collaborators TB Trials Study Group: TMD, HMSG, ACH, A Jacob, F Jahnsen, G D’Souza, A V Kurpad, EL, B Lindtjorn, R Macaden, MV.
Contributors Implementation and coordination of the study: MV, NJ. Data analyses: SJ, SS, CR, MV. Figures: SJ, SS. Wrote the manuscript: SJ, MV, CR, HMSG. Approved and contributed to the manuscript: SS, NJ, ACH, VC, EL, TMD.
Funding This work was supported by the Research Council of Norway (grants 179342 and 192534); the University of Bergen (Norway); Aeras (USA) and St. John’s Research Institute (India). Aeras and St.John’s Research Institute (SJRI) were responsible for the in-site preparation and training of study staff, study design. SJRI was responsible for conduct of the study and data collection with contributions from Aeras, the Research Council of Norway (RCN) and the University of Bergen (UoB). SJRI was responsible for laboratory and data analysis with contributions from UoB. Interim analysis was undertaken by Aeras. SJRI and UoB wrote the final report and decided to submit the paper for publication. Aeras provided input to the final report.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval The Institutional Ethical Review Board of the St. John’s National Academy of Health Sciences, Bangalore, an independent Ethics Committee contracted by Aeras, USA, and the Ministry of Health Screening Committee, Government of India (No. 5/8/9/60/2006-ECD-I dt. 10.11.2006).
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement This study utilised data that was part of a larger investigation. The closed-out data has been shared between collaborators in accordance with a prior agreement. The study team can make available, on requests linked to specific questions, and with the agreement of all collaborating institutions and regulatory authorities, data on specified variables that were part of the present study analysis.