Article Text

Abstract
Introduction Self-management interventions with Written Action Plans and case management support have been shown to improve outcomes in patients with chronic obstructive pulmonary disease (COPD). Novel telehealth technologies may improve self-management interventions. The objectives of this study were to determine whether the use of an interactive phone telesystem increases Action Plan adherence, improves exacerbation recovery and reduces healthcare use in a real-life practice of a COPD clinic.
Methods Initially, 40 patients were followed by a COPD telesystem for 1 year. Detailed data from patients’ behaviours during exacerbations was recorded. The telesystem use was then extended to 256 patients from a real-life COPD clinic. Healthcare utilisation for the year before and after telesystem enrolment was then assessed through hospital administrative databases.
Results Thirty-three of the 40 patients completed the initial 1-year study. Eighty-one exacerbations were reported in the 1-year follow-up. Action Plan adherence was observed for 72% of the exacerbations and those who were adherent had a significantly faster exacerbation recovery time. The large-scale implementation of the telesystem resulted in a significant decrease in the proportion of patients with ≥1 respiratory-related emergency room (ER) visits (120 before vs 110 after enrolment, p<0.001) and with ≥1 COPD-related hospitalisations (75 before vs 65 after enrolment, p<0.001).
Discussion COPD Written Action Plan adherence was further enhanced with the use of telehealth technologies in a specialised clinic with experience in COPD self-management. Patients followed by the telesystem recovered faster from exacerbations and had a further decrease in COPD-related ER visits and hospitalisations.
Trial registration number NCT02275078.
- COPD
- self-management
- telehealth
- action plan adherence
- exacerbations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
We wanted to evaluate whether the use of telehealth technologies can further improve Written Action Plan adherence and health outcomes in patients with chronic obstructive pulmonary disease (COPD).
We found that the integration of a phone interactive telesystem into an experienced COPD clinic improved Written Action Plan adherence, leading to faster exacerbation recovery and decreased healthcare utilisation.
This study demonstrates how simple technologies can be integrated into real-life clinical practice to improve the success of COPD self-management education programmes.
Introduction
Chronic obstructive pulmonary disease (COPD) exacerbations are a major factor contributing to the burden of the disease,1 leading to an increase in hospitalisations and mortality.2–4 Conversely, prompt treatment of exacerbations improves symptom recovery and prevents hospitalisations.5 6 In order to ensure a timely and effective management of exacerbations, patients need to promptly recognise these episodes and seek the appropriate treatment.7 8 These skills are known as self-management strategies.9
In a landmark randomised clinical trial, we demonstrated that self-management strategies supported with Written Action Plans and case management can prevent up to 40% of COPD-related hospitalisations.10 These results have guided current recommendations to support the use of Written Action Plans together with case management for the prevention of severe exacerbations.11 Indeed, Action Plan adherence is associated with a faster recovery from acute exacerbations.6 Unfortunately, COPD Action Plan adherence rates have been reported to be below 50%.6 12 Adherence to COPD Action Plans can be improved with collaborative programmes with coaching of COPD nurse case managers at the cost of increased time spent supporting the patients at distance.13 This becomes more time consuming and difficult to implement in every day practice as COPD patients have more severe disease. Telehealth technologies could have a place in the real life clinical practice to support COPD collaborative self-management programmes without placing an additional burden to healthcare providers. In a randomised controlled trial, we recently demonstrated that COPD self-management education programmes with coaching by case managers and with enhanced communication through a telephone/web platform reduce acute care hospitalisation days and mortality in patients with severe COPD.14 In this study, we implemented telehealth technologies to empower patients to manage their COPD through improved self-management education and an enhanced access to case manager support. This differs from telemonitoring strategies in whose objectives are to remotely diagnose, monitor and treat patients.15
The primary objective of our study was to assess the benefits of the implementation of a phone interactive telesystem for improving self-management in terms of: (1) patients’ adherence to COPD Written Action Plans in the event of exacerbations and (2) exacerbation recovery time. Our secondary objective was to determine whether a large-scale implementation of the telesystem could further reduce healthcare utilisation in a specialised centre with experience in COPD self-management.13
Methods
Study design
We initially conducted a 1-year observational pilot study with a sample of 40 patients with COPD to assess our primary objective. We then carried out a large-scale implementation study, in which access to the phone interactive telesystem was given to the entire caseload of three nurse case managers, adding up to a total of 256 patients with COPD. All patients in the pilot study singed an informed consent prior to their enrolment. For the large-scale implementation study, patients received detailed information about the use of the telesystem from their case managers. Patients then received a letter signed by both the Director and the Head Nurse of the COPD clinic. This letter explained how patients could activate their account and contact the telesystem. Patients that accepted to be followed by the telesystem activated their accounts. Patients that refused to be followed by the telesystem informed their case managers and continued to receive regular COPD care. The studies were approved by the Research Ethics Board (REB) of the McGill University Health Centre (Clinical Trials 1 panel, approval no. 2013–978-12–053 BMD). Individual patients cannot be identified through the information presented in this analysis.
Sample size calculation
When initiating the pilot study, we estimated that a sample size of 40 patients would provide an acceptable margin of error (13%) with 95% CI to estimate an Action Plan adherence of 40%, which are the adherence rates reported in the literature. Since the proportion of adherent patients in our data was very high, the margin of error could be increased to more than 10%. We did not conduct sample size calculation for the real-life study. However, we aimed to include over 90% of the caseload of the COPD clinic to be able to detect differences in COPD related hospitalisations 1 year after telesystem use.
Subject selection
Both studies
All patients were recruited from the COPD clinic at the Montreal Chest Institute (MCI) of the McGill University Health Centre (MUHC). Eligibility: diagnosis of COPD confirmed with a postbronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC)<0.70. Exclusion criteria: (1) cognitive impairment; (2) not fluent in English or French and (3) severe comorbidities that, in the opinion of the treating physician, limited the probability of survival to <6 months.
Telesystem pilot study (initial study)
Inclusion criteria: (1) aged ≥40 years; (2) smoking history ≥10 pack-years; (3) moderate disease as assessed by postbronchodilator spirometry FEV1<80% predicted,16 (4) one or more exacerbations requiring antibiotic or prednisone in the last year and (5) signed written consent accepting to participate in the study. Exclusion criteria: (1) home oxygen for 18–24 hours/day, chronic CO2 retention or previous mechanical ventilation (invasive or non-invasive); (3) severe comorbidities including bronchiectasis with recurrent infections and/or severe left congestive heart failure; (4) any significant medical condition other than COPD that may also result in dyspnoea (eg, unstable angina, body mass index>40). The recruitment for our pilot study was done over a 6-month period, using an existing list of patients with COPD followed at the MCI (diagnosis of COPD with previous exacerbations from the medical chart). Charts were flagged by clerical staff, while a research coordinator reviewed charts in detail for inclusion/exclusion criteria. The research coordinator contacted eligible patients by phone and invited them to attend an information session.
Telesystem large-scale implementation real life study-inclusion criteria
All patients with a diagnosis of COPD and part of the caseload of three COPD nurse case managers.
COPD self-management programme
All patients participating in both studies had received over 1 year of self-management intervention based on the Living Well with COPD programme (www.livingwellwithcopd.com).17 18 Patients also received coaching on the use of a Written Action Plan and were followed up by a specialised nurse case manager who also provided support by phone, as previously described.13 Written Action Plans included standing prescriptions for antibiotics and/or prednisone, as needed. Patients were asked to have their prescription given to the pharmacist to be used on demand. Patients were also advised to contact their case manager each time they had symptom changes compatible with an exacerbation and/or if they used their Written Action Plan.
Integration of a phone interactive telesystem
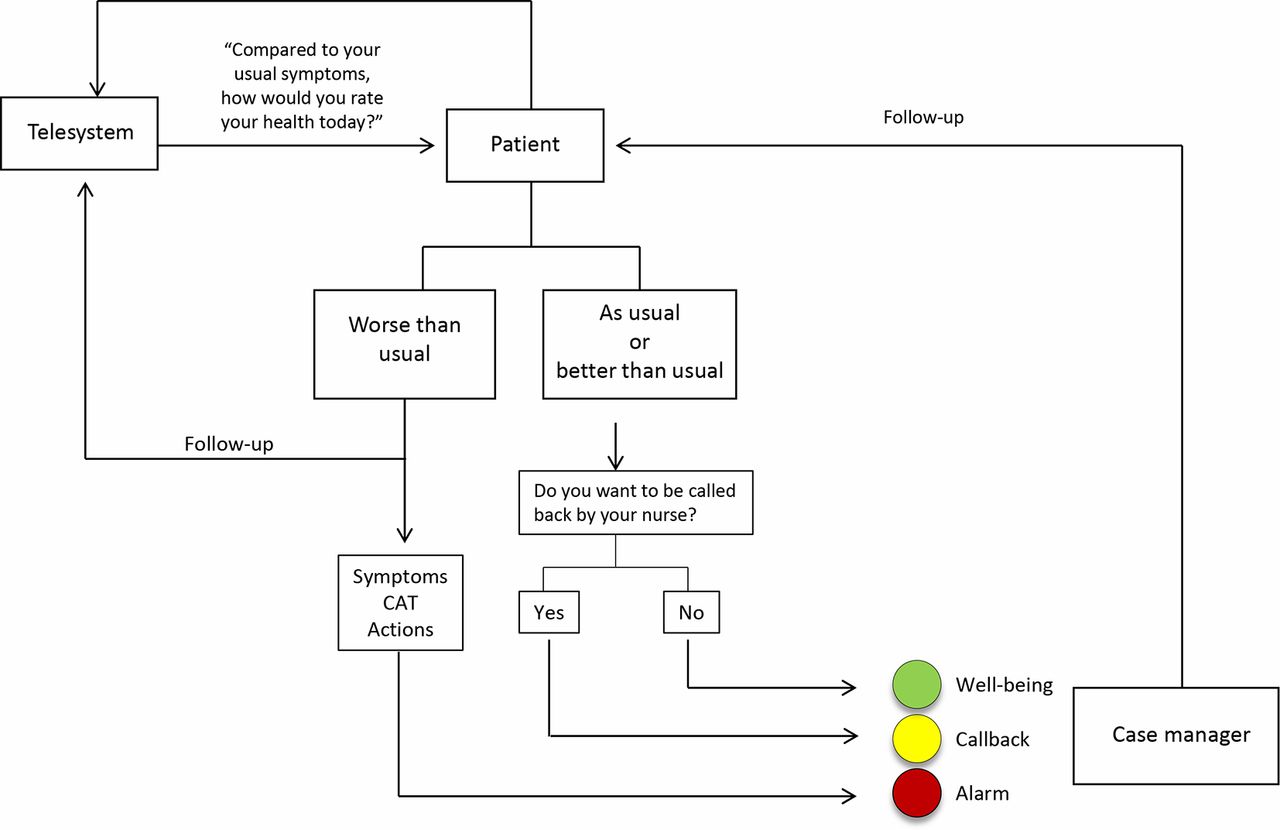
The main component of our intervention was the use of a computer-linked interactive phone telesystem (figure 1). Patients enrolled in the telesystem received a card that contained their personal identification number (PIN) and the telesystem contact information. Contact with the telesystem could be initiated by patients at all times. Additionally, the telesystem issued automated phone calls every month during the first 6 months after enrolment. Whether it was through automated calls or on direct contact by patients, the telesystem inquired on the patients’ general health status. Patients used their keyboard to submit three possible answers: (1) better than usual; (3) same as usual or (9) worse than usual. If patients reported their status as better than usual or as usual, a ‘well being’ notification was assigned. The telesystem then inquired whether patients wanted to be contacted by their case manager and if so, the telesystem issued a ‘callback’ notification. If patients’ status was reported as worse than usual, the telesystem automatically issued an ‘alarm’ notification and scheduled an automated follow-up call in 48 hours. The telesystem then used multiple choice questions to assess the following aspects: (1) patients’ symptoms including dyspnoea, sputum production, wheezing, chest tightness, cold, flu-like symptoms, fever and fatigue; (2) patients’ health-related quality of life (with the COPD Assessment Test; CAT) and (3) about COPD Action Plan use. Patients used their keyboard to submit their answers. The telesystem then notified patients that they would receive a follow-up call from their case managers and reminded them to follow their Action Plan. Finally, the telesystem reminded patients to go to the emergency room (ER) or to call 911 if they were experiencing chest pain, severe shortness of breath or if they felt their health was in immediate danger. Nurse case managers received ‘callback’ and/or ‘alarm’ notifications by email. Patients’ confidentiality was maintained since the emails only displayed patients’ study ID number. Nurse case managers accessed telesystem call information through a secured online database. This database displayed the general status of all patients enrolled in the telesystem through the use of graphs and also contained detailed information on individual patient calls. Nurse case managers used this information to plan follow-up calls. In turn, data from follow-up calls by case managers could be captured in the telesystem database by case managers. Case managers could then adapt the frequency of automated phone calls by the telesystem or add supplementary follow-up calls as needed. The case manager was the COPD nurse already following the patient in the COPD clinic.
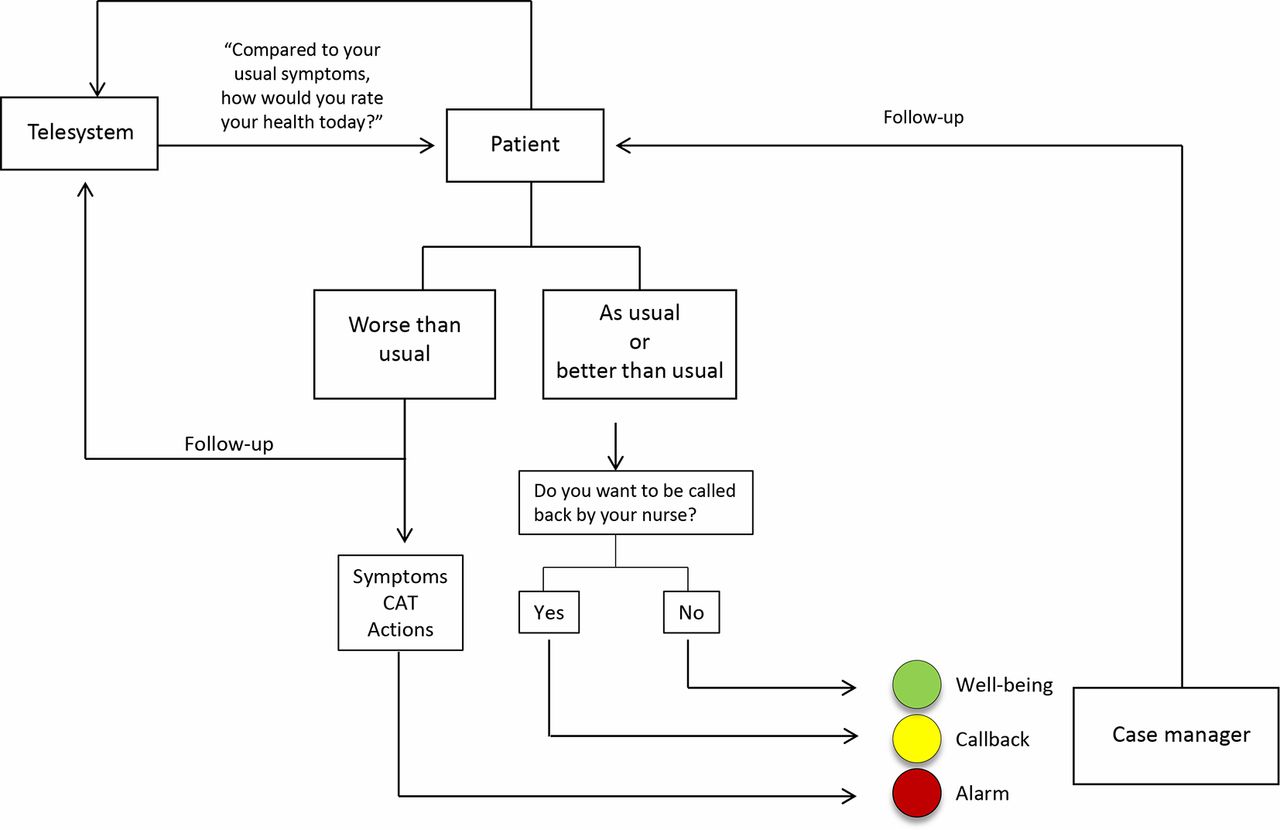
The telesystem. Patients received regular automated calls from a computer-linked telesystem. Patients could also directly contact the telesystem at any time. During the telesystem calls, patients were asked about their general health status, which could be reported as better than usual, as usual or worse than usual. Patients were also asked if they wanted to be contacted by their curse manager. Depending on patients’ answers to the automated calls, healthcare professionals received notifications indicating patient’s health status (well-being, callback or alarm). If patient’s health status was reported as worse than usual, the telesystem programmed an automated follow-up call and captured information on patients’ symptoms, quality of life (with the COPD assessment test, CAT) and patients’ actions (treatment and healthcare use). Healthcare professionals received an alarm notification email which allowed them to follow-up with patients by phone as soon as possible. COPD, chronic obstructive pulmonary disease.
The telesystem was conceived to support patients with COPD in the use of their Written Action Plans and to monitor patients’ general health at distance. Patients enrolled in the telesystem continued to receive usual care throughout the intervention and had access to the regular COPD clinic telephone line. The use of the telesystem and follow-up from nurse case managers were the same for both, patients in the initial pilot study and patients in the large-scale implementation study.
Outcomes
Pilot study
Primary outcome—COPD Action Plan adherence
COPD exacerbation, symptom-based definition: Change in ≥1 respiratory symptoms from baseline: (1) dyspnoea deterioration; (2) increased sputum and/or (3) increased sputum purulence for ≥2 consecutive days.19COPD exacerbation, event-based definition: Deterioration of respiratory symptoms requiring additional medical therapy defined as oral corticosteroids and/or antibiotics and/or acute care management.20Exacerbation start date: The first of two consecutive days of respiratory symptom worsening. Exacerbation end date: The last day with worsening symptoms. Independence of individual exacerbation events is defined as a minimum period of 7 days where symptoms are back to normal or at a new baseline. Exacerbation recovery time: Time elapsed between exacerbation start and end date. Treated recovery time: Time elapsed between medication start date and exacerbation end date. COPD Action Plan Adherence: Use of COPD Action Plan including starting exacerbation medications (rescue bronchodilator, antibiotic and/or prednisone) and/or contacting case managers within 3 days of symptom worsening.
Secondary outcome
Exacerbation recovery time.
Implementation real life study
Primary outcome: COPD-related hospital admissions.
Secondary outcome: Respiratory-related emergency room (ER) visits.
Procedures and measurements
Pilot study
Baseline characteristics, diagnosis of airflow obstruction and disease severity
Demographic characteristics and comorbidities21 were recorded in study case report forms at baseline. Airflow obstruction was defined as postbronchodilator FEV1/FVC<0.7 and disease severity was assessed with postbronchodilator per cent of predicted FEV1 values for specific age, sex and ethnicity groups.22
Action plan adherence and healthcare utilisation
Patients recorded details related to changes in their respiratory symptoms as well as medication and healthcare utilisation in a validated diary.6 23 These data were collected by research study staff every month through standardised telephone interviews. Specific dates of symptom deterioration, medication use, healthcare use and symptom resolution were captured and were used to define Action Plan adherence.
Evaluation of telesystem large scale implementation
Patients’ information on respiratory-related unscheduled healthcare use was obtained from individual electronic medical charts to capture the number and exact dates of ER visits and hospitalisations for the period covering 1 year before and 1 year after the receipt of a telesystem PIN. The collection of data for the implementation real life study covered the period of October 2013 to August 2016. Prebronchodilator spirometry values obtained within 6 months of telesystem enrolment were recorded, when available. Only data for respiratory-related health service utilisation were used in our analysis. This included the following diagnosis: COPD exacerbation, COPD with lower respiratory infection, other specified COPD, COPD unspecified, dyspnoea, pneumonia, respiratory infection and asthma.
Statistical analysis
Descriptive statistics were used to report patient characteristics, exacerbation characteristics and Action Plan Adherence categories. Differences in exacerbation recovery time were compared with Mann-Whitney’s test. Differences between the proportion of patients with one or more respiratory-related ER visits or COPD-related hospitalisations before and after telesystem enrolment were compared with McNemar’s test. The absolute number of ER visits, hospitalisations and the number of days spent at the hospital before and after telesystem enrolment were compared with Mann-Whitney’s U test. Results were considered to be statistically significant if p values were ≤0.05. Data were analysed using SAS V.9.4 software.
Results
Pilot study
Patients’ characteristics
Forty patients were eligible and consented to participate in the initial study. Seven patients did not complete all follow-up visits (one lung transplant, one decease, one brain cancer and four voluntary drop-outs). The characteristics of the 33 patients that completed the study are shown in table 1. Two thirds of the patients had severe to very severe airflow obstruction, an important history of smoking. considerable symptom burden and healthcare use.
Patients’ characteristics at baseline
Exacerbation characteristics
Table 2 summarises the characteristics of the exacerbations occurring during the 12-month follow-up for the initial study. The majority of patients presented two or more exacerbations during the year of initial evaluation. Sixty-eight of these exacerbations also fit the definition for event-based exacerbations, whose characteristics are presented in online supplementary table 1.
Supplemental material
Exacerbation characteristics
Patient actions during COPD exacerbations
Several actions alone or in combination were undertaken by patients during acute exacerbations. Table 3 presents the specific first action/s (within and beyond 3 days) as well as all the actions that patients undertook within the first 3 days of symptom worsening. The most common behaviour, both as a first action and as an action within 3 days of exacerbation onset, was initiating Action Plan medication. This was followed by contact with the case manager, which was done alone or in combination with other actions.
Patient actions during COPD exacerbations
Time-to-treatment during COPD exacerbations
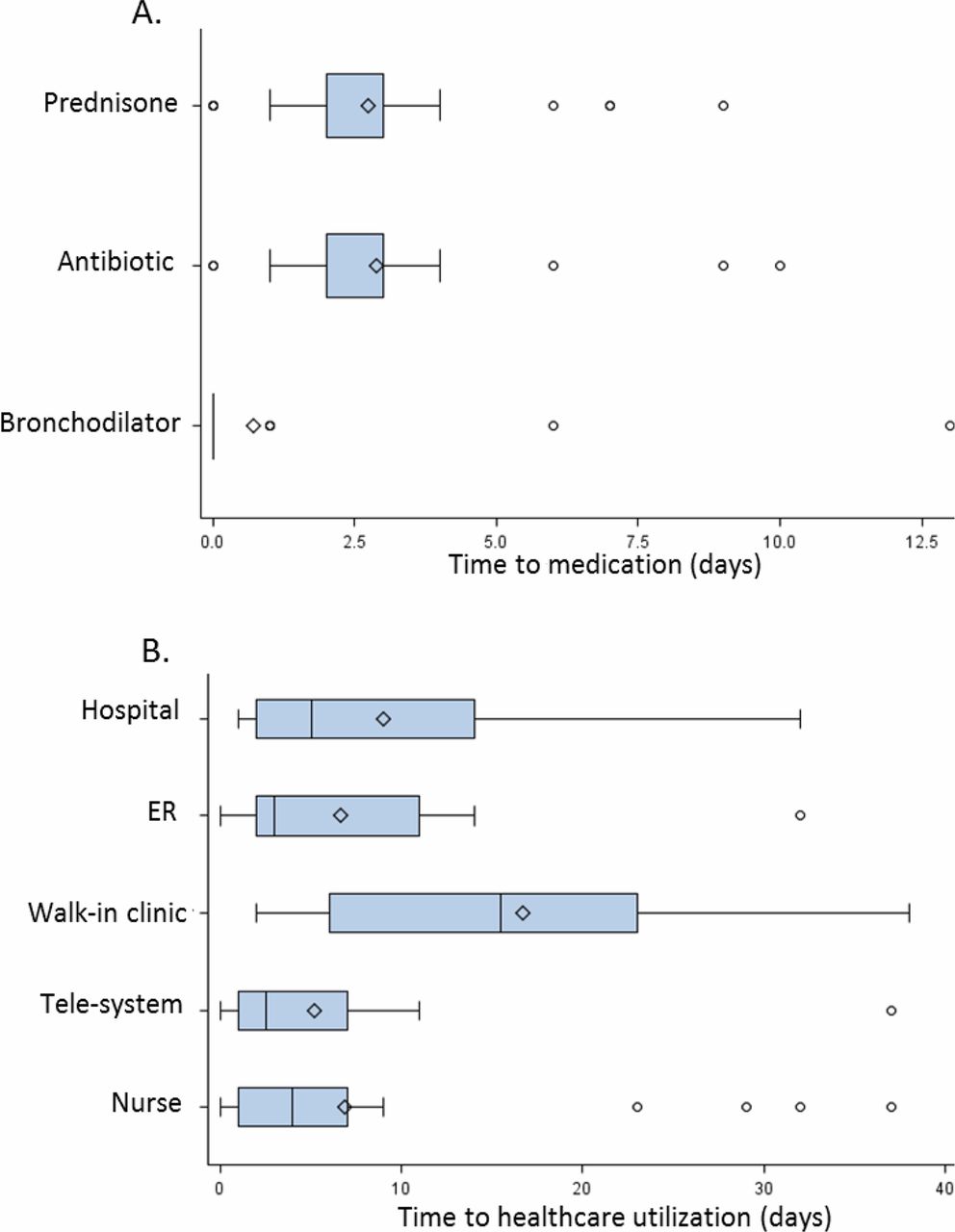
The times to each action during COPD exacerbations, including time to medication and time to healthcare utilisation, are presented in figure 2. On average, patients initiated prednisone, antibiotic and rescue bronchodilator within 3 days of exacerbation onset (figure 2A). The time to contact with healthcare providers was variable, with an average delay of approximately 6 days to contact the telesystem, nurse case manager (direct contact) and ER and delays greater than 6 days to being admitted to the hospital or going to the walk-in clinic (figure 2B).

Time-to-treatment during COPD exacerbations. (A) Time to medication use (days). (B) Time to healthcare utilisation (days). Box plots from left to right: circles to the left box plots, outliers; left whisker, lowest observation; left box border, lower quartile (25th percentile); vertical line dividing the box, median; diamonds within the box, mean; right box border, upper quartile (75th percentile); right whisker, highest observation; circles to the right of box plots, outliers.
COPD Action Plan adherence and exacerbation recovery
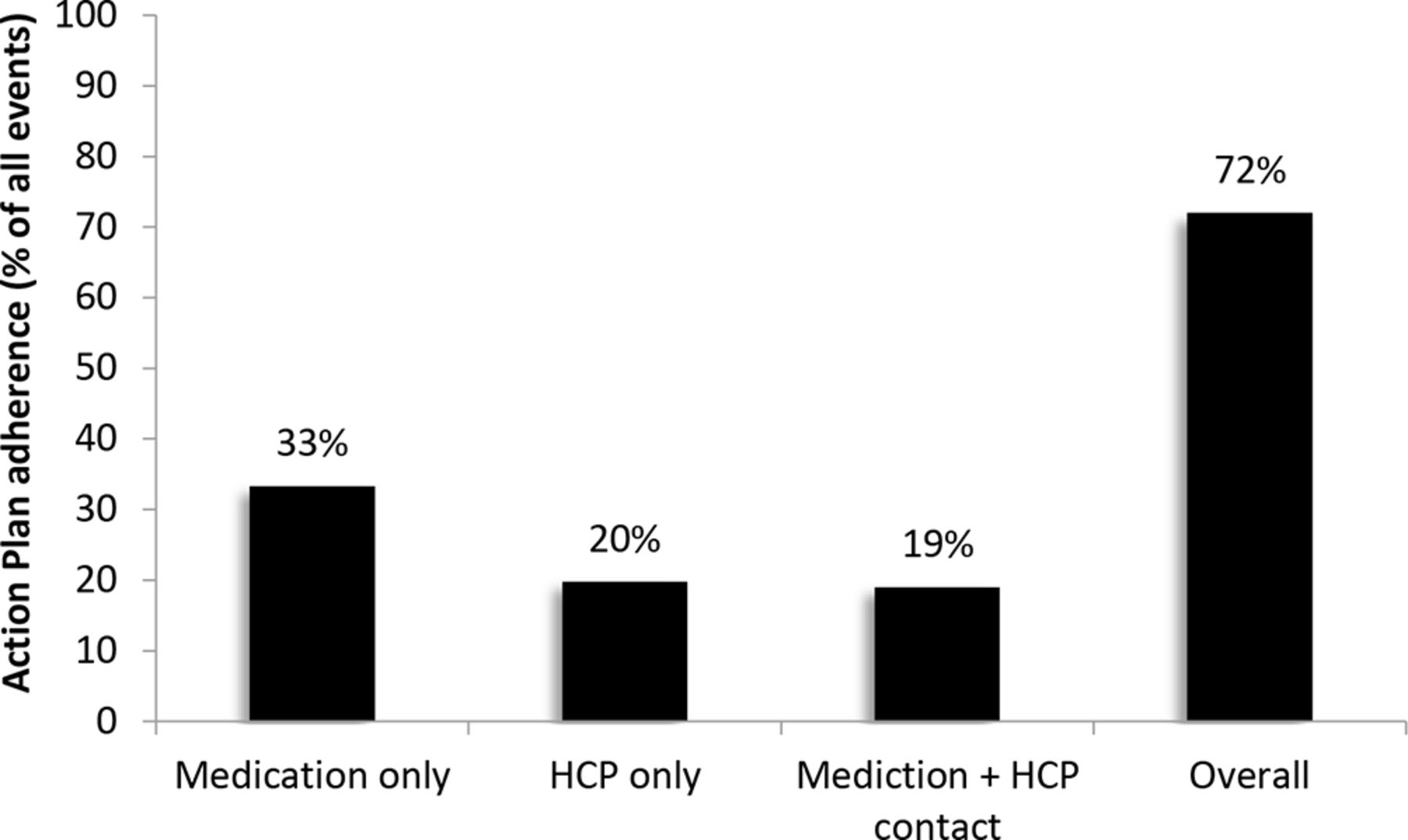
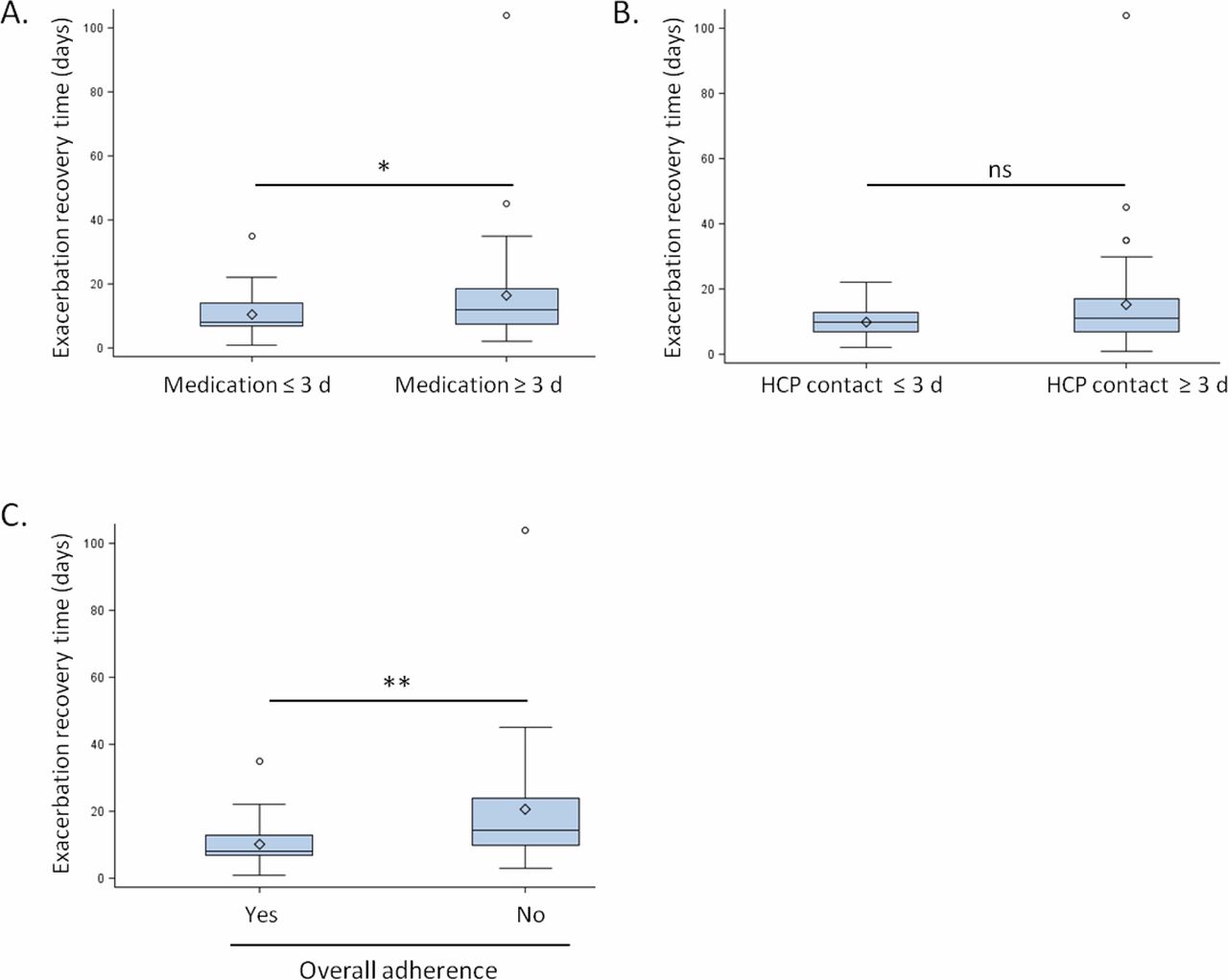
Overall, Action Plan adherence was observed in 72% of the reported exacerbations (figure 3). This included exacerbations in which patients either took their Action Plan medication and/or contacted a healthcare professional within 72 hours of symptom worsening. Recovery time was significantly reduced for exacerbations in which patients adhered to their Action Plan medication and for overall adherent patients (figure 4A and C). Recovery time did not change significantly for the events in which patients contacted healthcare professionals within 3 days of symptom worsening (figure 4B).
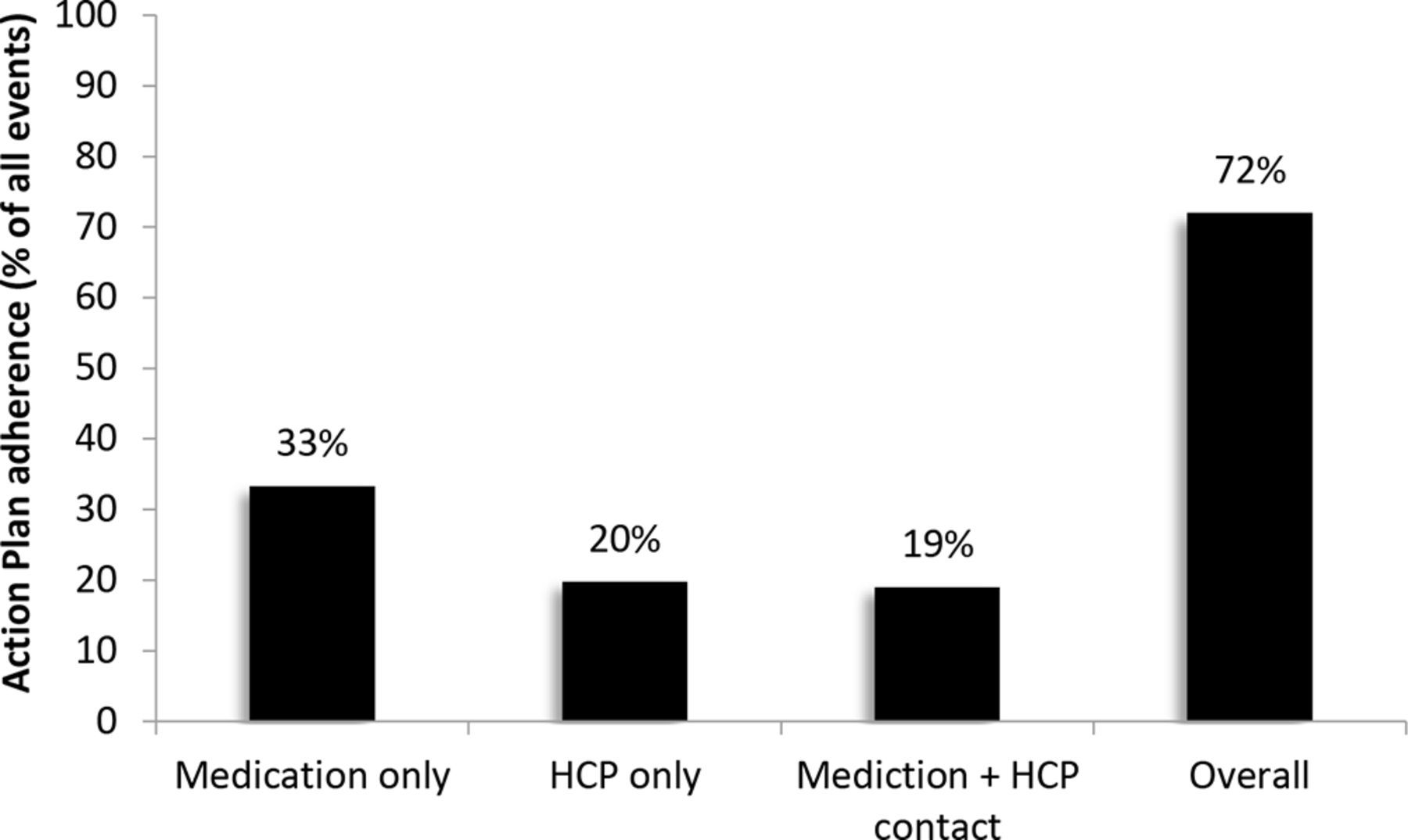
COPD Action Plan adherence. Proportion of exacerbations in which patients took their Action Plan medication, contacted their HCP and did both, take their Action Plan medication and contact their HCP. Overall adherence was considered for exacerbations in which patients either took their medication or contacted their HCP within 72 hours of exacerbation onset. COPD, chronic obstructive pulmonary disease; HCP, healthcare professional.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exacerbation recovery time by Action Plan adherence category. Time to recover from a COPD exacerbation in days for the following categories: (A) patients taking their COPD Action Plan medication within 72 hours of exacerbation onset; (B) patients contacting a HCP within 72 hours of exacerbation onset and (C) patients that either took their Action Plan medication or contacted their HCP within 72 hours of exacerbation onset. Box plots from top to bottom: circles above box plot, outliers; top whisker, highest observation; top box border, upper quartile (75th percentile); diamond inside box plot, mean; horizontal line dividing the box, median; bottom box border, lower quartile (25th percentile); bottom whisker, lowest observation. Results were compared with Mann-Whitney’s test; *p<0.05 and **p<0.001. COPD, chronic obstructive pulmonary disease; HCP, healthcare professional.
Telesystem large-scale real-life implementation
The use of the telesystem was extended to the caseload of the COPD clinic for a total of 256 patients (117 male/139 female, aged 70±9 years, prebronchodilator FEV1 0.42±0.2% of predicted). Overall, these characteristics are very similar to those of patients that completed the initial pilot study. Table 4 presents the unscheduled healthcare use 12 months before and 12 months after implementing the telesystem. Following the addition of the telesystem in patients who already had self-management intervention with the support of a case manager nurse, we observed a significant decrease in the number of patients with ≥1 respiratory-related ER visits and COPD-related hospitalisations. Although non-significant, we also observed a trend towards a decrease in the absolute number of respiratory-related ER visits, COPD-related hospitalisations and days hospitalised for a COPD-related diagnosis (table 4).
Health resource utilisation before and after telesystem enrolment
Discussion
With these studies, we have demonstrated that COPD self-management strategies already implemented in an experienced COPD clinic can be further strengthened through the use of communication technologies. In our initial pilot study, we have shown that the integration of a COPD phone interactive telesystem, in a centre experienced in collaborative COPD self-management can result in further increased adherence rates to Written Action Plans in patients having COPD exacerbations.6 13 In line with previous observations, patients that adhered to their Written Action Plan experienced faster exacerbation recovery times.6 Then, when the telesystem was implemented to the entire caseload of a COPD clinic, we demonstrated a statistically significant reduction in the proportion of patients experiencing respiratory-related ER visits and COPD-related hospitalisations.
Adequate behaviours are a major determinant of outcomes during COPD exacerbations. Patient recognition of exacerbation onset and prompt treatment improve recovery and reduce hospitalisations.5 The timely management of exacerbations can be ensured through the use of COPD Written Action Plans in conjunction with case manager support.24 We have previously demonstrated that adherence to Written Action Plans accelerates exacerbation recovery.6 However, in a previous study we only observed Action Plan adherence rates of 40%.6 This has been confirmed by other studies in patients with COPD.25 In a more recent study conducted by our group in the same clinical setting of a COPD clinic, we observed that Action Plan adherence rates can be increased from 40% to 60% through the implementation of a more intense follow-up.13 In the present study, we observed that COPD Action Plan adherence rates can be further increased from 60% to 72%, which are the highest adherence rates reported in the literature so far. This increase in Action Plan adherence is relevant since adherent patients recover faster. More importantly, we were able to demonstrate that this implementation on a large-scale COPD has the potential to further reduce hospitalisations from exacerbations.
In order to better understand how our intervention modified patient behaviours, we conducted a qualitative evaluation that consisted of 27 semistructured interviews and questionnaires to evaluate patient’s perception of the telesystem as a tool to support COPD self-management, as well as perceived benefits, barriers, facilitating factors and any suggestions. Although the details of this qualitative evaluation will not be presented in this manuscript, our analysis showed that most patients considered that the calls made by the telesystem helped patients increase their disease awareness and improve their symptom control. Additionally, patients felt reassured to have a support tool to manage their disease. Therefore, it is likely that increased awareness and increased confidence played a key role in increasing Action Plan adherence.
Recently, there has been a growing interest in the use of information and communication technology to improve outcomes in chronic diseases. However, remote monitoring of signs and symptoms and respiratory physiology alone have failed to show benefit on early intervention and reduction on health service use. Trials with remote patient monitoring platforms such as PROMETE II and CHROMED had both negative results.26 27 It has therefore been suggested that we should use telemedicine to enhance best practice, as an adjunct to self-management approaches assisting proper healthcare coaching.28 Patient engagement, also known as patient activation, is necessary for these behavioural changes to occur.29 Previous studies have reported increased feelings of security and reassurance with the use of telemonitoring technologies in COPD.30 31 In the present study, we have demonstrated that more simple technologies can increase patients’ level of confidence to manage their disease. Our approach differs from existing telemonitoring systems in that patient participation and activation were essential in our model of care. Patients were taught to recognise their baseline symptoms and kept a symptom diary in which they recorded the specific dates of any worsening of dyspnoea, cough, sputum quantity, sputum colour and other general symptoms including fatigue, fever and symptoms of a cold or influenza. Patients were given written Action Plans with information on the measures to take if they experienced any worsening of their symptoms. Regardless, patients were encouraged to contact their case manager if they experience any symptom worsening. Although the telesystem captured information on patients’ symptoms and patients’ actions, the primary objective of the telesystem was not to monitor patient status but to encourage them to adhere to their Action Plans and to facilitate communication with their case managers. In this regard, our telehealth technology was used as a facilitator of collaboration between patients and case managers.
The main strength of our study is that it represents benefits related to the implementation of a phone interactive telesystem in the ‘real-life’ setting of a specialised COPD clinic with experience in COPD self-management.13 Although done at a small scale, our initial study included several detailed measurements such as exact dates of symptom aggravation, medication use, healthcare utilisation and symptom recovery. The use of validated diaries and the frequency of exacerbation questionnaires helped minimise recall bias.23 These detailed measurements allowed us to assess the impact of the telesystem on Written Action Plan adherence and on patients’ actions during exacerbations. Through the use of electronic health records, we were able to assess the impact of the COPD telesystem on healthcare for the whole population of patients with severe COPD followed in a COPD clinic and not only for a selected group who agree to participate in the study.
The main limitation of our study is related to its design, this is an observational study and not a randomised controlled trial. We cannot completely attribute the improvement in COPD self-management skills to the telesystem. Furthermore, the skills and expertise of the three nurse case managers could have positively influenced our results. Despite this limitation, our data strongly suggest that patient activation together with strategies to ensure rapid communication with healthcare professionals could be contributing to increased Action Plan adherence rates and to improved outcomes. Moreover, patients were their own control from a historical perspective. Since patients were not recruited in random order, there is potential for selection bias. However, this was mitigated by our large-scale implementation study, in which we analysed the healthcare utilisation for COPD-related exacerbations for which we analysed an entire cohort comprising over 90% of the caseload of the COPD clinic. Finally, we acknowledge that the monthly calls from the research team might have influenced self-management behaviours, since patients are aware of being observed and might therefore be more engaged in adhering to their treatment (Hawthorne effect). However, we consider that monthly phone calls supported with information from validated symptom diaries are the best means to capture both symptom and event-based exacerbations. Monthly calls are required to ensure the accuracy and quality of the data related to exacerbation onset, duration and specific dates of medication and healthcare use. Moreover, research staff calls are necessary to avoid recall bias.
In conclusion, our study has demonstrated that COPD Action Plan adherence can be improved with the use of a phone interactive telesystem when combined with self-management strategies with the coaching of a case manager. Based on our experience at the MCI, we have been able to improve collaborative self-management in patients with high disease burden by enhancing communication between patients and case managers.13 Although this is not the same cohort of patients than the one included in our previous studies, patients included in our study had been followed using the same high-quality standards of care. Indeed, we have shown that Action Plan adherence rates are higher in our experienced centre; however, the highest adherence rates we have reported in patients using written Action Plans, followed by a case manager and having received COPD self-management training are 60%.13 One main implication of our study is that communication technologies can be integrated into COPD self-management programmes in experienced secondary and tertiary care centres. Both patients with COPD and case managers could benefit from large scale implementation of similar technologies. Additionally, our results could constitute the basis for the design of trials to assess whether telemedicine and telehealth in COPD can have real a return on investments.
Acknowledgments
The COPD interactive phone telesystem was developed and provided by TelASK Technologies (Ottawa, ON, Canada). We would like to thank all the patients participating in the study.
References
Footnotes
Presented at Information in this article was presented as an abstract in the following meetings: (1) 2017 American Thoracic Society International Conference, May 2017, Washington DC, USA; (2) 12es Journées Francophones Alvéole, March 2018, Nantes, France; (3) Canadian Respiratory Conference 2018, April 2018, Vancouver, BC, Canada; (4) European Respiratory Society International Congress 2018, September 2018, Paris, France.
Contributors JB and RF had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. JB, MS and RF contributed substantially to the study design. JB, RF, MS, DB, ID, IO, AJ, RA and MP contributed to the study implementation. MP, RF and MAR substantially contributed to data collection. RF contributed to data analysis and interpretation. JB and RF contributed to the writing of the manuscript.
Funding Funding for this project was provided by GlaxoSmithKline as an Investigator-Initiated project (ClinicalTrials.gov identifier:NCT02275078).
Competing interests JB reports grants from CIHR, Canadian Respiratory Research Network (CRRN), grants and personal fees from GLAXOSMITHKLINE, GRIFOLS, grants from AEROCRINE, grants and personal fees from BOEHRINGER INGELHEIM, ASTRAZENECA, NOVARTIS, grants from the Foundation of the MUHC, personal fees from NOVARTIS, all outside the lifespan of the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.