Article Text

Abstract
Background We aimed to assess the uptake of minimally invasive surgery (MIS) and stereotactic body radiation therapy (SBRT) among early stage (stage IA–IIB) non-small cell lung cancer (NSCLC) cases in the USA, and the rate of conversions from MIS to open surgery.
Materials and methods Data were obtained from the US National Cancer Database, a nationwide facility-based cancer registry capturing up to 70% of incident cancer cases in the USA. We included cases diagnosed with early stage (clinical stages IA–IIB) NSCLC between 2010 and 2014. In an ecological analysis, we assessed changes in treatment by year of diagnosis. Among surgically treated cases, we assessed the uptake of MIS and whether conversion to open surgery took place. For cases that received thoracic radiotherapy, we assessed the uptake of SBRT.
Results Among 117 370 selected cases, radiotherapy use increased 3.4 percentage points between 2010 and 2014 (p<0.0001). Surgical treatments decreased 3.5 percentage points (p<0.0001). Rates of non-treatment remained stable (range: 10.0%–10.6% (p=0.4066)). Among surgically treated stage IA cases, uptake of MIS increased from 28.7% (95% CI 27.8% to 29.7%) in 2010 to 48.6% (95% CI 47.6% to 49.6%) in 2014 (p<0.0001), while conversions decreased from 17.0% (95% CI 15.6% to 18.6%) in 2010 to 9.1% (95% CI 8.3% to 10.0%) in 2014 (p<0.0001). MIS uptake among stages IB–IIB was lower and conversion rates were higher, but time trends were similar. Uptake of SBRT among stage IA receiving thoracic radiotherapy increased from 53.4% (95% CI 51.2% to 55.6%) in 2010 to 73.0% (95% CI 71.4% to 74.6%) in 2014 (p<0.0001). SBRT uptake among stage IB increased from 32.5% (95% CI 29.9% to 35.2%) in 2010 to 48.2% (95% CI 45.6% to 50.8%) in 2014 (p<0.0001).
Conclusion Between 2010 and 2014, uptake of MIS and SBRT among early stage NSCLC significantly increased, while the rate of conversions to open surgery significantly decreased. Continuing these trends may contribute to improving patient care, in particular with the expected increase in early stages due to the implementation of lung cancer screening.
- non-small cell lung cancer
- thoracic surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
We aimed to assess the uptake of minimally invasive surgery (MIS) and stereotactic body radiation therapy (SBRT) among early stage non-small cell lung cancer (NSCLC) cases in the USA, as well as the rate of conversions from MIS to open surgery.
What is the bottom line?
Between 2010 and 2014, the uptake of MIS and SBRT among patients diagnosed with early stage NSCLC increased significantly, while the rate of conversions to open surgery decreased significantly.
Why read on?
Continuing the increasing uptake of MIS and SBRT may contribute to improving patient care, in particular with the expected increase in early stage diagnoses due to international recommendations and plans for the implementation of lung cancer screening.
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide.1 2 The majority of lung cancer cases are non-small cell lung cancer (NSCLC).3 Currently, most NSCLC cases are diagnosed with metastatic disease,4 in which case curative treatment is usually not possible.5 However, the number of cases diagnosed with potentially curative early stage disease is expected to increase in upcoming years6 due to the ongoing (USA) and considered (EU and UK) implementation of lung cancer screening.7–9
While surgical resection is still standard of care for early stage NSCLC, the preferred surgical approach has shifted from thoracotomy to minimally invasive surgery (MIS). MIS includes video-assisted thoracoscopic surgery (VATS) and, more recently, robotic-assisted thoracic surgery (RATS).5 MIS is associated with less postoperative pain, shorter hospital stay, less pulmonary complications and improved quality of life compared with thoracotomy, without compromising perioperative mortality or short-term survival.10–13 Although a recent analysis suggests that the uptake of VATS among patients with lung cancer in the US Veterans Affairs is increasing,14 the generalisability of these findings to early stage NSCLC cases in the general US population remains unknown. In addition, the Veterans Affairs analysis did not include cases treated with RATS. Also, the current rate of conversions from MIS to open surgery and whether this rate has changed with the increased uptake of MIS is unclear.
Some patients with early stage NSCLC are unfit for surgery due to comorbidity or may prefer not to undergo surgery for non-medical reasons. For those patients, stereotactic body radiation therapy (SBRT) is now recommended as an alternative standard of care.5 SBRT concentrates a high dose of radiotherapy on a small target volume using only a few fractions. In patients with medically inoperable early stage NSCLC, SBRT provides local tumour control rates of up to 90% with moderate toxicity.15 16 A previous analysis suggested that the uptake of SBRT in the USA could still be lagging.17
The degree of uptake of these therapies is topical because the effectiveness of the recent recommendations and plans for lung cancer screening will depend on optimal treatment of early stage lung cancer. Therefore, we aimed to assess the uptake of MIS and SBRT among early stage NSCLC cases in the USA, as well as the rate of conversions from MIS to open surgery. We hypothesised that the uptake of MIS and SBRT in the USA increases over time. This hypothesis was tested in an ecological analysis of secular trends in the facility-based US National Cancer Database (NCDB).
Methods
Data
We extracted all individual-level records from the NCDB of persons diagnosed with early stage (ie, clinical stages IA, IB, IIA and IIB) NSCLC between 2010 and 2014. The NCDB, established in 1989, is a nationwide, facility-based, comprehensive clinical surveillance resource oncology data set that currently captures 70% of all newly diagnosed malignancies in the USA annually, from more than 1500 affiliated facilities. To ensure the accuracy of treatment data we excluded the following groups: non-malignant cases; cases not staged using the American Joint Commission on Cancer (AJCC) seventh edition system;18 cases with a history of multiple primary tumours of which lung cancer was not the first; cases diagnosed before the date from which the reporting facility guarantees accuracy of the data; cases that were diagnosed at the reporting facility but received therapy elsewhere; cases with more than 4 months (ie, 122 days) between diagnosis and onset of treatment; and cases for which it was unknown whether any treatment was received. These exclusion criteria are in concordance with NCDB guidelines and with a previous investigation of NCDB data conducted by our group.17
Statistical analysis
We assessed the proportion of cases that received surgery, radiotherapy and no therapy as first course treatment by clinical stage and by year of diagnosis. Among surgically treated cases, we assessed whether the planned approach was MIS (which includes VATS and RATS), and whether conversion to open surgery took place. If a patient received multiple surgeries, the NCDB records the surgical approach of the most invasive and definitive surgical treatment. In addition, we assessed the extent of resection (sublobar, lobectomy or bilobectomy, pneumonectomy, or other; see online supplementary methods for coding). Because the extent of disease may affect the technical difficulty of performing MIS, time trends in the uptake of MIS and the rate of conversions were assessed by clinical stage and by extent of resection.
Supplemental material
For cases that received radiotherapy, we assessed the radiation target (thoracic vs non-thoracic). For cases with a thoracic radiation target, we further assessed whether SBRT or another radiation modality was used. In accordance with a previous report we defined SBRT as thoracic radiotherapy with a total radiation dose of at least 45 Gray over five fractions or less.17 Because the extent of disease may affect the feasibility of SBRT, time trends in the uptake of SBRT were assessed by clinical stage.
Trends were formally tested using χ2 trend tests. Exact binomial 95% CIs were calculated for proportions. All analyses were performed using R software V.3.6.1.19 This analysis of NCDB data was deemed exempt by the Institutional Review Board at the University of Michigan.
Sensitivity analyses
If the surgical approach was unknown we assumed that MIS had not taken place. Similarly, we assumed that SBRT was not used if the radiation modality was unknown. In a sensitivity analysis, we excluded those cases with missing data on either of these variables.
A second sensitivity analysis assessed whether time trends in the uptake of MIS and SBRT differed by sex and by age.
Patient and public involvement statement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Patient characteristics
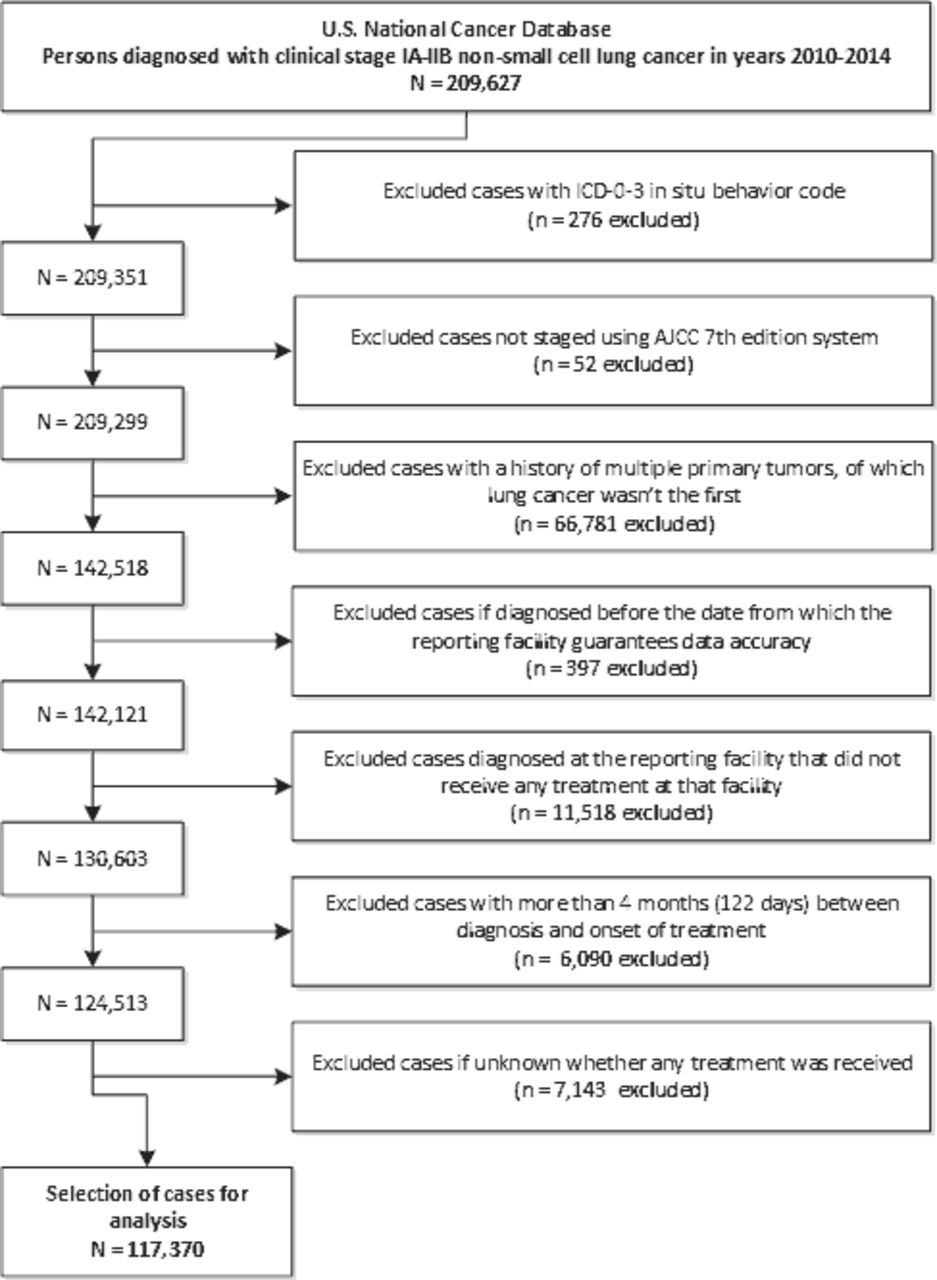
We identified records for 209 627 cases diagnosed with early stage (ie, clinical stages IA, IB, IIA and IIB) NSCLC between 2010 and 2014. After exclusions, 117 370 cases were selected for analysis (see figure 1). Among the selected cases, 55 248 (47.1%) were male. Median age at diagnosis was 70 years (IQR: 62–77 years). Clinical stage at diagnosis was IA for 61 123 cases (52.1%), IB for 26 049 cases (22.2%), IIA for 15 898 cases (13.5%) and IIB for 14 300 cases (12.2%).
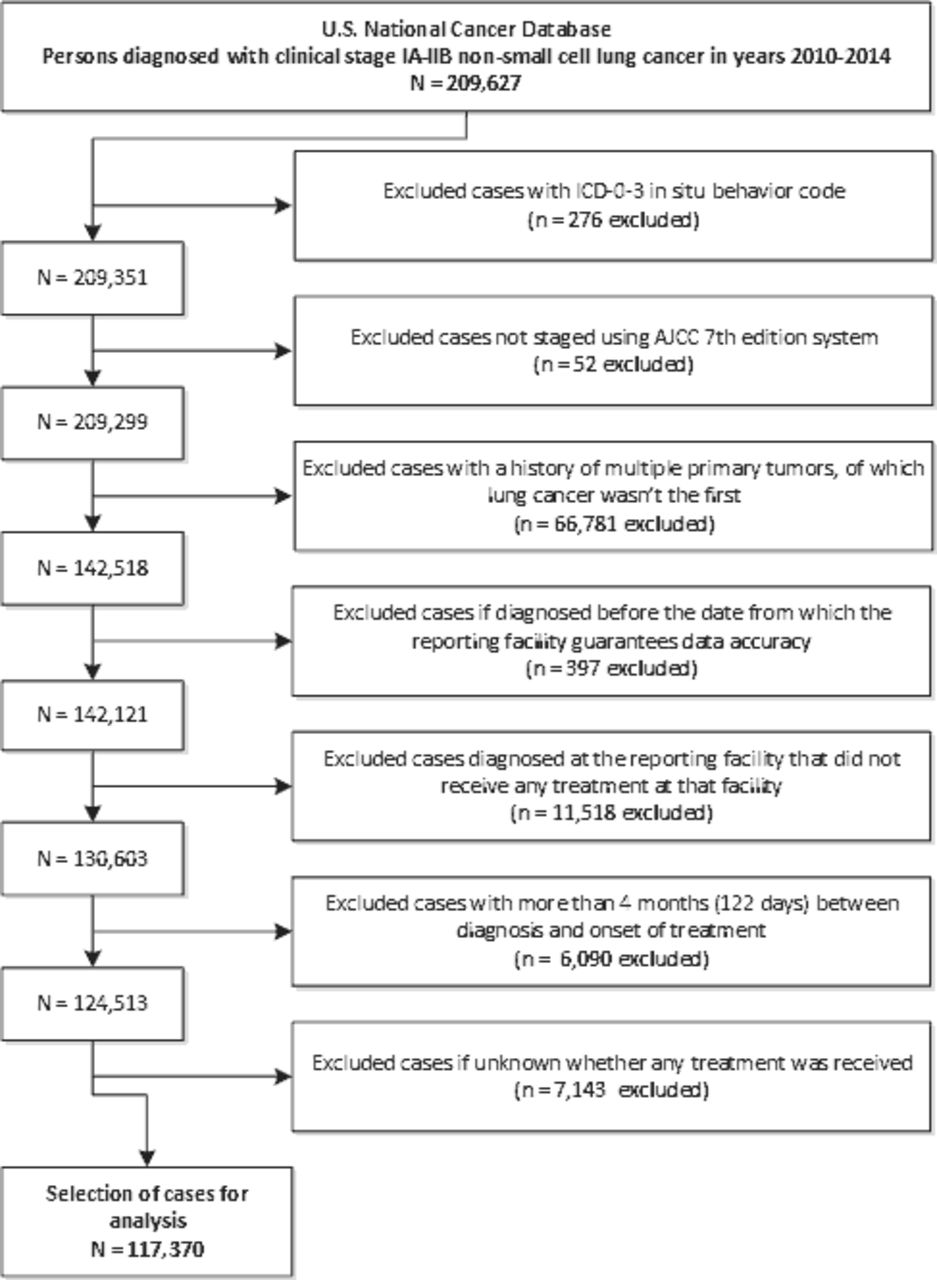
Flow chart of case selection. ICD-0-3, International Classification of Diseases for Oncology, third edition; AJCC, American Joint Committee on Cancer.
General treatment patterns
Table 1 presents general treatment patterns by clinical stage at diagnosis and by year of diagnosis. Overall, the percentage of early stage NSCLC cases receiving surgery decreased with advancing stage at diagnosis, from 72.2% (95% CI 71.9% to 72.6%) among stage IA to 48.3% (95% CI 47.5% to 49.1%) among stage IIB (−23.9 percentage points; p<0.0001). Conversely, the percentage receiving radiotherapy increased with advancing stage (from 22.4% (95% CI 22.1% to 22.7%) among stage IA to 44.6% (95% CI 43.8% to 45.4%) among stage IIB (+22.2 percentage points; p<0.0001)). Also, the percentage of cases receiving no treatment increased from 7.6% (95% CI 7.4% to 7.9%) among stage IA to 15.5% (95% CI 15.0% to 16.1%) among stage IIB (+7.9 percentage points; p<0.0001).
Treatment patterns among early stage non-small cell lung cancer cases by clinical stage at diagnosis and by year of diagnosis
Between 2010 and 2014, the number of early stage NSCLC cases that received surgery decreased by 3.5 percentage points (p<0.0001), from 67.9% (95% CI 67.3% to 68.5%) in 2010 to 64.4% (95% CI 63.8% to 65.0%) in 2014. The number of cases that received radiotherapy increased by 3.4 percentage points (p<0.0001), from 25.6% (95% CI 25.0% to 26.2%) in 2010 to 29.0% (95% CI 28.4% to 29.5%) in 2014. The percentage of cases that did not receive any treatment varied between 10.0% (95% CI 9.7% to 10.4%) and 10.6% (95% CI 10.2% to 11.0%) across years 2010–2014, with no particular time trend (p=0.4066).
Online supplementary table 1 shows the extent of resection among surgically treated cases by clinical stage and year of diagnosis. Overall, 18.1% (95% CI 17.8% to 18.4%) received a sublobar resection, 77.0% (95% CI 76.7% to 77.3%) received a lobectomy or a bilobectomy, and 3.7% (95% CI 3.6% to 3.8%) received a pneumonectomy. Only minor changes in the distribution of surgical extent occurred over time. However, the percentage receiving sublobar resection decreased from 24.3% (95% CI 23.9% to 24.7%) among stage IA to 9.4% (95% CI 8.8% to 10.2%) among stage IB (−14.9 percentage points; p<0.0001). Conversely, the percentage receiving pneumonectomy increased with advancing stage, from 0.8% (95% CI 0.7% to 0.9%) among stage IA to 13.2% (95% CI 12.4% to 14.0%) among stage IIB (+12.4%; p<0.0001).
Uptake of MIS and rate of conversions
Figure 2A shows the trend in uptake of MIS by clinical stage among those treated surgically between 2010 and 2014. Among surgically treated stage IA cases (n=44 160), the uptake of MIS increased by 19.9 percentage points, from 28.7% (95% CI 27.8% to 29.7%) in 2010 to 48.6% (95% CI 47.6% to 49.6%) in 2014. Although the percentage receiving MIS in 2010 was lower for stages IB–IIB than for stage IA (22.9% (95% CI 21.5% to 24.3%) among stage IB, 20.0% (95% CI 18.2% to 21.8%) among stage IIA, 15.7% (95% CI 13.8% to 17.8%) among stage IIB), the increase over time was similar (+18.5,+15.1 and +16.8 percentage points, respectively). Whereas the uptake of MIS increased over time, the rate of conversions to open surgery among these cases decreased. For stage IA, the rate of conversions decreased by 7.9 percentage points, from 17.0% (95% CI 15.6% to 18.6%) in 2010 to 9.1% (95% CI 8.3% to 10.0%) in 2014 (figure 2B). The rate of conversions was higher for stages IB–IIB compared with stage IA in 2010, but the decreases over time were similar (range across stages: −7.0 to −10.6 percentage points). All stage-specific trends in the uptake of MIS and the rate of conversions to open surgery were statistically significant (p<0.0001).
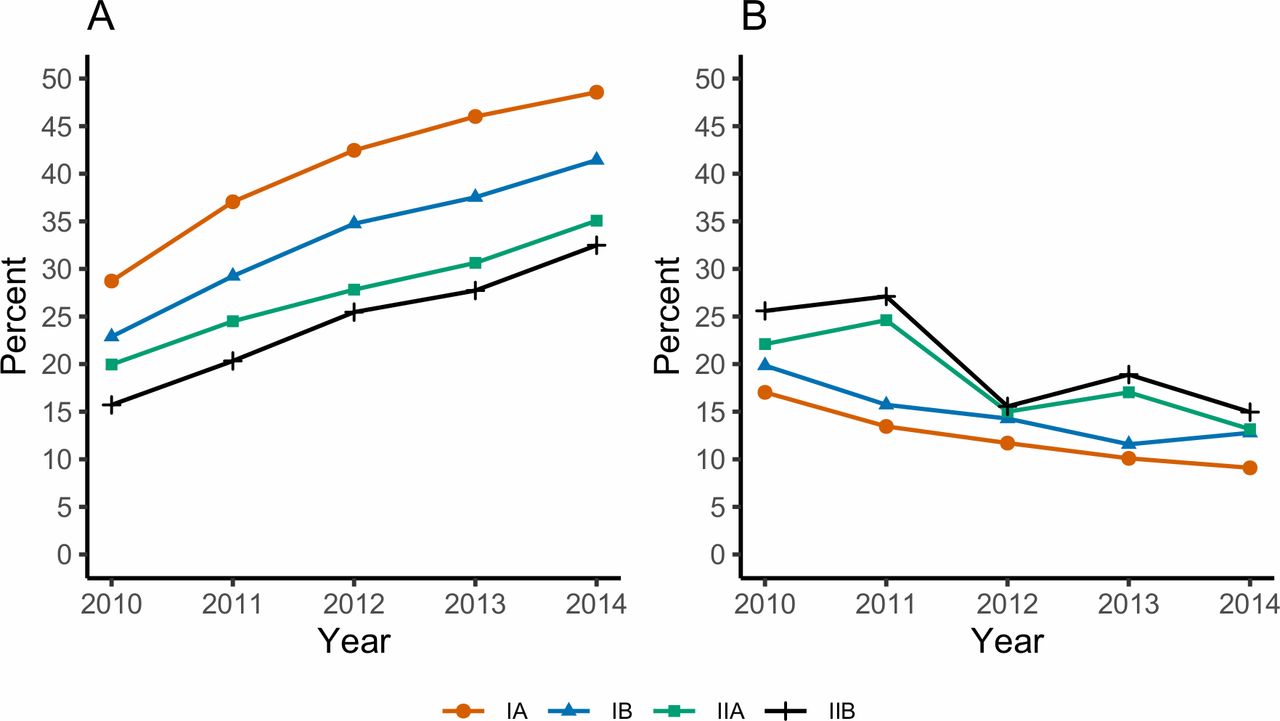
Uptake of minimally invasive surgery among early stage non-small cell lung cancer cases between 2010 and 2014 by clinical stage at diagnosis. (A) The percentage of lung cancer surgeries that were started as minimally invasive surgery between 2010 and 2014 by clinical stage at diagnosis. (B) The percentage of lung cancer surgeries which started as minimally invasive surgery that were converted to open surgery between 2010 and 2014, by clinical stage at diagnosis.
Time trends in the uptake of MIS and the rate of conversions to open surgery by extent of resection are shown in figure 3. In 2010, the uptake of MIS was highest among those receiving a sublobar resection (33.6% (95% CI 31.8% to 35.4%)), followed by lobectomy or bilobectomy (23.6% (95% CI 22.8% to 24.4%)) and pneumonectomy (11.2% (95% CI 8.8% to 14.0%)). Between 2010 and 2014, uptake of MIS increased for all extents of resection (for sublobar resection:+20.8 percentage points (p<0.0001); for lobectomyor bilobectomy: +19.0 percentage points (p<0.0001); for pneumonectomy: +8.9percentage-points (p=0.0002)). In 2010, rates of conversions were highest for those receiving pneumonectomy (36.8% (95% CI 25.4% to 49.3%)), followed by those receiving lobectomy or bilobectomy (20.9% (95% CI 19.4% to 22.5%)), and finally those who received a sublobar resection (11.8% (95% CI 9.7% to 14.1%)). The rate of conversions decreased over time for sublobar resections (−5.4 percentage points; p<0.0001) and for lobectomy or bilobectomy (−9.4 percentage points; p<0.0001), but not for pneumonectomy (p=0.5813).

Uptake of minimally invasive surgery among early stage non-small cell lung cancer cases between 2010 and 2014 by extent of resection. (A) The percentage of lung cancer surgeries that were started as minimally invasive surgery between 2010 and 2014 by extent of resection. (B) The percentage of lung cancer surgeries which started as minimally invasive surgery that were converted to open surgery between 2010 and 2014, by extent of resection. Overall, only 1.3% of surgically treated cases received surgery of ‘other’ extent. Therefore, time trends were not assessed for this category.
Uptake of SBRT
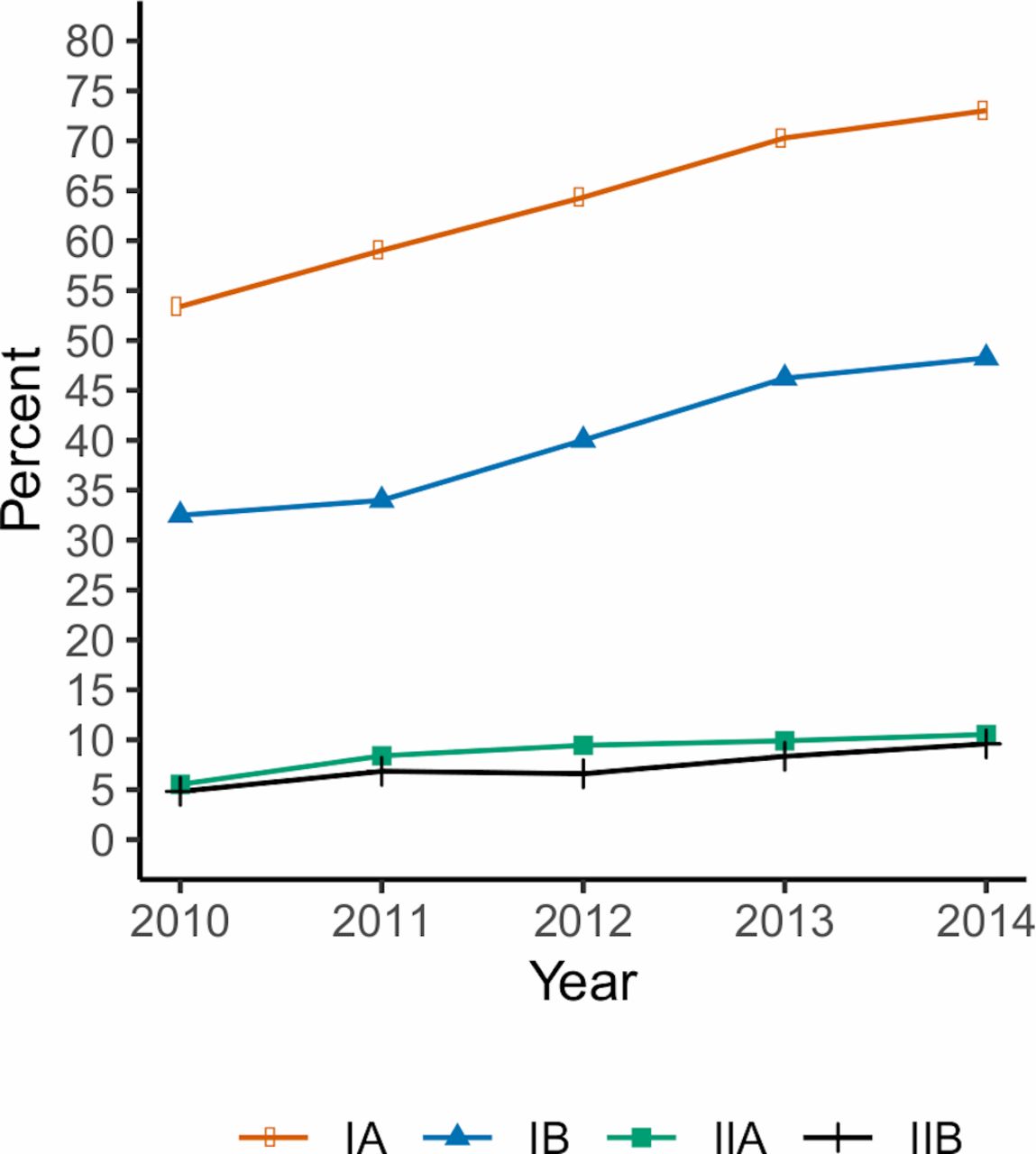
Among early stage NSCLC cases treated with radiotherapy, 95.5% (95% CI 95.3% to 95.7%) received thoracic radiotherapy. Figure 4 shows the uptake of SBRT among these cases by clinical stage. Among the 13 252 stage IA NSCLC cases that received thoracic radiotherapy, the use of SBRT increased from 53.4% (95% CI 51.2% to 55.6%) in 2010 to 73.0% (95% CI 71.4% to 74.6%) in 2014 (+19.6 percentage points). The uptake of SBRT among the 6729 stage IB NSCLC cases that received thoracic radiotherapy increased by 15.7 percentage points, from 32.5% (95% CI 29.9% to 35.2%) in 2010 to 48.2% (95% CI 45.6% to 50.8%) in 2014. However, during the same period the percentage receiving SBRT remained low among the 4962 stage IIA cases and the 6005 stage IIB cases that received thoracic radiotherapy. The uptake of SBRT among stage IIA was 5.5% (95% CI 4.2% to 7.2%) in 2010 and 10.5% (95% CI 8.7% to 12.6%) in 2014 (+5.0 percentage points). Among stage IIB, the uptake of SBRT was 4.8% (95% CI 3.7% to 6.2%) in 2010 and 9.6% (95% CI 8.0% to 11.4%) in 2014 (+4.8 percentage points). All stage-specific time trends in the uptake of SBRT were statistically significant (p<0.0001).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Uptake of stereotactic body radiation therapy among early stage non-small cell lung cancer cases treated with thoracic radiotherapy between 2010 and 2014 by clinical stage at diagnosis.
Sensitivity analyses
Data on the surgical approach or radiation modality were missing for 5089 cases. After excluding those cases, the uptake of MIS and SBRT were higher, although stage-specific time trends remained similar (see online supplementary figures 1 and 2). For example, among 42 773 surgically treated stage IA cases, the uptake of MIS increased by 20.6 percentage points, from 29.2% (95% CI 28.2% to 30.2%) in 2010 to 49.8% (95% CI 48.8% to 50.8%) in 2014 (p<0.0001). The rate of conversions to open surgery among stage IA cases decreased from 17.1% (95% CI 15.6% to 18.6%) in 2010 to 9.1% (95% CI 8.3% to 10.0%) in 2014 (−8.0 percentage points; p<0.0001). Among 12 241 stage IA cases that received thoracic radiotherapy, the uptake of SBRT increased from 59.0% (95% CI 56.7% to 61.2%) in 2010 to 77.8% (95% CI 76.3% to 79.3%) in 2014 (+18.8 percentage points; p<0.0001).
The uptake of MIS and SBRT increased over time for both sexes and all age groups (see online supplementary figures 3–6). In addition, the rate of conversions to open surgery decreased over time for both sexes and all age groups. The uptake of VATS and SBRT were slightly higher among women than among men, whereas the rate of conversions was slightly lower. For example, the uptake of VATS among men in 2010 was 23.5% (95% CI 22.5% to 24.5%), compared with 26.6% among women (95% CI 25.7% to 27.6%). The uptake of SBRT was notably higher for more advanced ages (see online supplementary figure 6). For example, the uptake of SBRT in 2010 was 5.3% (95% CI 2.1% to 10.5%) among those younger than 50 years, compared with 38.8% (95% CI 36.2% to 41.5%) among those older than 80 years.
Discussion
General treatment patterns
Patterns of care indicate that most early stage NSCLC cases receive surgery and/or radiotherapy. However, whereas the percentage receiving radiotherapy increased with advancing stage, the percentage receiving surgery decreased with advancing stage. This likely reflects the increasing difficulty of performing more extensive surgical resections, even among those with stage IA–IIB disease.
Uptake of MIS and rate of conversions
The use of MIS among surgically treated cases increased over time, up to 48.6% among stage IA cases in 2014. This increasing uptake of MIS was robust across the different conducted sensitivity analyses. Our findings are similar to those in a recent study, in which 44.5% of wedge resections and lobectomies among patients with non-metastatic lung cancer in Veterans Affairs hospitals between 2012 and 2015 were conducted using VATS.14 The European Thoracic Surgery Database, which collects data from 170 hospitals across 22 European countries, reported that the uptake of VATS lobectomies increased from 5.4% in 2007–2011 to 29.3% in 2012–2015.20 Thus, it appears that the uptake of MIS in Europe is also increasing, although its uptake may lag compared with the USA.20 In the UK, the uptake of MIS is similar to the USA; increasing from 53.4% in 2016 to 55.8% in 2017.21 Rates of conversions were similar in the UK (10.6% of lobectomy and bilobectomy procedures in 2017), compared with our US-based study (11.5% of lobectomy and bilobectomy procedures in 2014).21 The increasing use of MIS may particularly benefit patients with a reduced lung function or cardiopulmonary reserve, in whom this approach has been shown to reduce rates of pulmonary morbidity compared with open surgery.22
While we confirm that the uptake of MIS is increasing, we add that the rate of conversions to open surgery decreased during the same period. This may reflect increasing experience of thoracic surgeons.23 Whereas the uptake of MIS decreased with advancing stage, the rate of conversions increased with advancing stage. This finding may be partly explained by the decreasing use of sublobar resections and the increasing use of pneumonectomy with advancing stage. Indeed, the uptake of MIS was lower for more extensive resections (eg, pneumonectomy < (bi)lobectomy < sublobar resection). These observations may reflect the technical difficulty of performing more extensive resections by MIS.
In the USA, annual lung cancer screening has been recommended for high-risk individuals.7 It has been estimated that the full-scale implementation of lung cancer screening in the USA will shift the percentage of stage I diagnoses in the general population (which includes individuals that are not eligible for screening) from 22.2% to 30.6%.6 This will increase demand for lung cancer surgery in the USA by up to 37.0%.6 If screening is to be effective, these cases should receive optimal treatment by MIS resection in a high-volume hospital.24 25 Therefore, we expect that the uptake of MIS in the USA will continue to increase in coming years. In Europe, lung cancer screening has not yet been implemented. Nevertheless, several European countries have expressed the intention to start planning for the implementation of lung cancer screening.8 Therefore, we expect that the uptake of MIS lung resections will continue to increase in Europe as well.
Uptake of SBRT
Among patients with stage IA–IB NSCLC, the uptake of SBRT increased substantially between 2010 and 2014. This finding was robust to the different sensitivity analyses. The increasing uptake of SBRT may particularly benefit patients with lung cancer with comorbidities, which can increase the risks related to surgery. In the Netherlands, Palma and colleagues demonstrated that an increased use of SBRT among patients with stage I NSCLC led to fewer untreated elderly patients.26 In our US-based study, the overall percentage of early stage patients that received radiotherapy (both SBRT and conventional radiotherapy) also increased (by 3.4 percentage points). However, we did not find a corresponding reduction in the rate of non-treatment. Instead, we found that the percentage of early stage cases that received surgery decreased by 3.5 percentage points. This suggests a possible shift from operable patients towards medically inoperable patients (eg, due to comorbidities), which should be further investigated in future studies. The constant non-treatment rate of approximately 10% suggests possibilities for a further increase in the use of radiotherapy, and in particular SBRT, among early stage cases that would otherwise not receive any treatment.
Currently, SBRT is only recommended for medically inoperable early stage NSCLC cases. However, some studies have suggested that SBRT may be feasible in medically operable patients,27 which could increase the future uptake of SBRT. Because lung cancer screening is only recommended for patients fit to undergo curative lung surgery,7 it’s continued implementation may not directly increase the future use of SBRT. However, in practice it may be difficult to assess fitness for surgery prior to screening. Therefore, the increase in early stage cases due to screening may still lead to a further increase in the use of SBRT. Consequently, it is likely that the uptake of SBRT will continue to increase.
The uptake of SBRT was modest but present among stages IIA and IIB. This is most likely due to concerns about either lymph node involvement, tumour size or size of the irradiated field. SBRT is indeed most appropriate for tumours smaller than 5 cm (which encompasses stage I–IIA). Nevertheless, SBRT may also be used for larger isolated tumours (T1–3, N0, M0).5 28
Strengths and limitations
The most important strength of this current analysis is the use of the NCDB data set, which captures treatment data on 70% of incident cancer cases in the USA. Although this database is facility-based, an earlier report found no major differences in the distributions of sex, age, race or ethnicity, health insurance status, histology, and stage between lung cancer cases in the NCDB and the population-based Surveillance, Epidemiology, and End Results data set.17 Therefore, in contrast to previous reports, the findings of our study are likely representative for the general US population.14
A possible limitation of our study is the lack of clinical information in the NCDB, such as performance status. Therefore, we could not determine whether cases were medically operable or not. Future research is necessary to determine whether cases that do not receive any treatment may have been medically eligible for surgery or SBRT.
A second possible limitation of using cancer registry data is that coding practices may change over time. However, the AJCC seventh edition staging manual was almost exclusively used during the study time period, which limits changes in study eligibility over time. In addition, no changes occurred in the coding of any of the outcome variables (eg, surgical approach, surgical extent or radiation modality).
A third limitation is that we did not assess whether the increasing use of MIS and SBRT affected patient outcomes. The NCDB does not include patient-reported outcomes, such as quality of life. In addition, we feel that a prospective randomised trial is the best method to provide an unbiased comparison of oncological outcomes across treatment modalities. Recently, the prospective VIdeo-assisted thoracoscopic lobectomy vs conventional Open LobEcTomy for lung cancer Trial confirmed that that VATS lobectomy is associated with significantly lower in-hospital complications and a shorter length of stay than open lobectomy, without compromising oncological outcomes.29 Another recent prospective randomised controlled trial, which included inoperable stage I NSCLC cases, showed that SBRT provides superior tumour control compared with standard radiotherapy, without increasing toxicity.30 These studies indicate that the increasing uptake of MIS and SBRT in the USA will likely provide clinical benefit to patients with early stage NSCLC.
Conclusions
In conclusion, patterns of care show that surgeons in the USA have been increasingly using MIS to treat early stage NSCLC while the rate of conversions decreased. SBRT is also increasingly used. The increasing uptake of MIS and SBRT may particularly benefit patients with lung cancer at higher operative risk. Nevertheless, the increasing use of radiotherapy does not seem to coincide with a reduction in the percentage of cases that do not receive any treatment. Therefore, there may be room for an additional increase in the use of radiotherapy, and in particular SBRT, among cases that would otherwise receive no treatment. Continuing the increasing trends in uptake of MIS and SBRT may contribute to improving overall patient care, in particular with the expected increase in early stage lung cancer due to the implementation of lung cancer screening.
References
Footnotes
Presented at Some of the results presented in this manuscript were presented at the 19th World Conference on Lung Cancer (Toronto, 25 September 2018).
Contributors EFB, KtH, DAA and HJdK contributed to the conception and design of the work; EFB performed data analysis; EFB, KtH, DAA and HJdK contributed to interpretation of the data; EFB drafted the manuscript; KtH, DAA and HJdK critically revised the manuscript for important intellectual content; EFB, KtH, DAA and HJdK approve of the final version for publication and agree to be accountable for all aspects of the work.
Funding This work was funded by Grant 1U01CA199284-01 from the National Cancer Institute at the National Institutes of Health as part of the Cancer Intervention and Surveillance Modelling Network (CISNET).
Disclaimer The National Cancer Institute had no involvement in the study design, analysis and interpretation of data, in the writing of the report, or in the decision to submit the article for publication.
Competing interests HJdK, KtH and EFB are members of the Cancer Intervention and Surveillance Modeling Network (CISNET) Lung working group (grant 1U01CA199284-01 from the National Cancer Institute). HJdK is the principal investigator of the Dutch-Belgian Lung Cancer Screening Trial (Nederlands-Leuvens Longkanker Screenings onderzoek; the NELSON Trial). KtH and EFB are researchers affiliated with the NELSON Trial. HJdK and KtH received a grant from the University of Zurich to assess the cost-effectiveness of CT lung cancer screening in Switzerland. HJdK and KtH were involved in the Cancer Care Ontario Health Technology Assessment Study for CT Lung Cancer Screening in Canada. KtH is involved in the Selection of Eligible People for Lung Cancer Screening using Electronic Primary Care DaTa (SELECT) Study. KtH was an invited speaker at the 17th, 19th and 20th World Conferences on Lung Cancer, as well as the 5th Russian Society of Clinical Oncology conference, for which travel expenses were paid (in part). DAA serves on the International Association for the Study of Lung Cancer (IASLC) Smoking Cessation and Tobacco Control Committee, and the American College of Chest Physicians Lung Cancer Guidelines Executive Committee.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This analysis of NCDB data was deemed exempt by the Institutional Review Board at the University of Michigan.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. An application for the National Cancer Database data may be completed at https://www.facs.org/quality-programs/cancer/ncdb/puf.
Author note Please see the following abstract: Blom EF, Ten Haaf K, Arenberg D, De Koning HJ. MA18.06 Patterns of Lung Cancer Care in the United States: Developments and Disparities (Abstract). J Thorac Oncol 2018; 13: S420.