Article Text

Abstract
Background The COVID-19 pandemic has highlighted the need for alternative short-term, reliable means to aid in the treatment of patients requiring ventilatory support. Concurrent aerosol drug delivery is often prescribed to such patients. As such, this study examines one such short-term option, the disposable gas-powered transport ventilator to effectively deliver aerosol therapy. Factors such as aerosol generator type, patient breathing pattern, humidification and nebuliser position within the respiratory circuit were also examined.
Methods Aerosol drug delivery characterisation was undertaken using two different disposable transport ventilators (DTVs). Two different nebuliser types, a closed circuit vibrating mesh nebuliser (VMN) and an open circuit jet nebuliser (JN), at different locations in a respiratory circuit, proximal and distal to an endotracheal tube (ETT), with and without passive humidification, were evaluated in simulated adult and paediatric patients.
Results Placement of a nebuliser proximal to the ETT (VMN: 25.19%–34.15% and JN: 3.14%–8.92%), and the addition of a heat and moisture exchange filter (VMN: 32.37%–40.43% and JN: 5.60%–9.91%) resulted in the largest potential lung dose in the adult patient model. Irrespective of nebuliser position and humidification in the respiratory circuit, use of the VMN resulted in the largest potential lung dose (%). A similar trend was recorded in the paediatric model data, where the largest potential lung dose was recorded with both nebuliser types placed proximal to the ETT (VMN: 8.12%–10.89% and JN: 2.15%–3.82%). However, the addition of a heat and moisture exchange filter had no statistically significant effect on the potential lung dose (%) a paediatric patient would receive (p>>0.05).
Conclusions This study demonstrates that transport ventilators, such as DTVs, can be used concurrently with aerosol generators to effectively deliver aerosolised medication in both adult and paediatric patients.
- ambulatory oxygen therapy
- assisted ventilation
- nebuliser therapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Are disposable transport ventilators (DTVs) a viable option for combination aerosol therapy during adult and paediatric ventilation?
Nebuliser type, position of aerosol generator within the respiratory circuit and use of passive humidification influence drug deposition during concurrent aerosol drug delivery with DTVs. The measured lung dosages compared favourably with similar studies using critical care ventilators.
This study draws attention to DTVs as a potential option for both short-term ventilatory support and concurrent aerosol therapy in scenarios where critical care resources are limited, inappropriate or unavailable.
Introduction
Crisis events such as natural disasters, terror attacks and, more recently, a global pandemic place considerable strain on hospital systems and resources.1 2 Critical care ventilators can provide support to patients suffering from a wide range of medical conditions.3 However, a shortage of ventilators has serious implications for patient treatment and prognosis. Emergency and disposable transport ventilators (DTVs) have emerged as a potential alternative that could be used in the initial care of patients.
Mechanical ventilation (MV) is the standard respiratory care provided to critically ill patients who cannot maintain their airways or adequate oxygenation levels. DTVs are devices used in emergency or transport situations to provide positive pressure ventilation and to assist a patient in breathing.4 These devices, for example, the Vortran GO2VENT and Egemen Life Control disposable ventilator, provide controlled ventilation with a fixed fraction of inspired oxygen and have simple controls for breath rate (BR) and tidal volume (Vt). Of note, the GO2VENT is also registered for up to 30 days of short-term use with the Food and Drug Administration. Weiss et al5 compared manual and automatic resuscitators in an emergency medical situation during ventilation of intubated patients and concluded no significant difference in overall patient care between the two resuscitator types. A recent study by Afacan et al6 investigated the efficacy and safety of a DTV; based on patient vital signs and blood gas analyses, the authors found that the disposable ventilator tested was a reliable option for short-term ventilation of critically ill mechanically ventilated patients during transport. To the best of the authors’ knowledge, while a number of studies involving resuscitators are available,2 4–6 no studies have been performed in combination with aerosol therapy, and comparative aerosol delivery efficiencies remains unclear.
Respiratory diseases are a leading cause of critical illness and subsequent provision of respiratory support with combination aerosol therapy is now a mainstay treatment used within the intensive care unit and emergency departments.7–9 Aerosol therapy provides high local drug concentrations with few systemic side effects. Examples of inhaled aerosol agents include bronchodilators and mucolytics which are used in the treatment of chronic obstructive pulmonary disease and asthma.9 10 A number of studies have reported on the factors that can affect aerosol drug delivery, such as choice of aerosol generator, artificial airway selection, placement within the respiratory circuit and humidification. Alhamad et al11 showed that aerosol delivery with a vibrating mesh nebuliser (VMN) and pressurised metered-dose inhaler was more efficient than with a jet nebuliser (JN) in an in vitro paediatric breathing model. The position of the aerosol generator also greatly influences aerosol drug delivery in ventilated patients. Studies by both Berlinski et al12 and Ari et al13 showed improved aerosol deposition when the aerosol generator was placed at the dry side of the humidifier compared with at the wye in both adult and paediatric settings. Finally, various reports have shown how the presence of active and passive humidification, via a heated humidifier or heat and moisture exchangers (HMEs), within the respiratory circuit can influence aerosol deposition.13 14 Ari et al14 reported lower and more consistent aerosol drug delivery with an HME than with a standard non-humidified model.
To date, there has been no study that has examined the potential of DTVs to successfully deliver aerosol for the short-term treatment of ventilator-dependent patients. The hypothesis under investigation in this piece of work is whether DTVs are a viable short-term alternative to MVs for the delivery of aerosol treatments to ventilator-dependent patients. It is well documented in MV studies that nebuliser type, position within the respiratory circuit and humidification can significantly affect the potential aerosol dose a patient receives. The potential effects, if any, of these variables on aerosol drug delivery during simulated ventilation of adult and paediatric patient models will also be examined.
Methods
The following section outlines the materials and methods used to assess the effectiveness of commercially available DTVs.
Disposable transport ventilator
The DTVs used in this study were the GO2VENT, manufactured by Vortran Medical (USA) and the Life Control disposable ventilator, produced by Egemen International-TMT Medical Products (Turkey). Neither of these ventilators have a display or gauge with the BR, Vt or inspiratory to expiratory ratio (I:E) generated. These devices have an analogue manometer which provides a reading of the Peak Inspiratory Pressure (PIP).
Respiratory circuit
The respiratory circuit used in this study is presented in figure 1. All experiments were performed with an 8.0 mm (adult) or 5.0 mm (paediatric) inner-diameter endotracheal tube (ETT) (Flexicare; Flexicare Medical, Wales, UK) connected to a capture filter (RespirGard II 303, Baxter, Ireland) and a test lung (IMT SmartLung; IMT Analytics AG, Buchs, Switzerland). The effect of passive humidification, via an heat and moisture exchange (HME) filter (Gibeck Humid Flo HME; Teleflex, North Carolina, USA), on the dose delivered to the patient was also examined. The respiratory circuit had the capability to be adapted for both adult and paediatric patient types, with the appropriate t-piece, ETT and test lung placed in situ. The total length and diameter of the adult respiratory circuit, from the exit of the DTV to the capture filter, varied from 680 to 760 mm, and from 8 to 22 mm, depending on the nebuliser type and mode of connection to the circuit. The paediatric respiratory circuit length and diameter varied from 670 to 750 mm and from 5 to 15 mm. The effect of aerosol generator location within the respiratory circuit was also examined (see figure 1). Two different positions were considered: (1) proximal (between the ETT and the end of the elbow of the respiratory circuit tubing) and (2) distal (between the HME filter and the respiratory circuit tube) to the ETT.

Schematic illustration of the test set-up. Simulated adult and paediatric ventilation assessed the lung dose (%) beyond the ETT across two nebuliser positions: (i) proximal and (ii) distal to the ETT. ETT, endotracheal tube.
Aerosol generator
Experiments were performed using a closed circuit VMN (Aerogen Solo; Aerogen, Galway, Ireland) and an open circuit JN (Cirrus Jet Nebuliser; Intersurgical, UK). The JN was operated at a driving gas flow rate of 7 L/min and run until sputter+1 min for each condition in this study. The performance characteristics of the VMN and JN, measured using laser diffraction (Spraytec; Malvern Instruments, Malvern, UK) and described previously in MacLoughlin et al,15 are presented as the average droplet size (µm), expressed as volumetric median diameter (VMD) and aerosol flow rate (mL/min). The VMN had a measured VMD of 4.26±0.08 µm and an aerosol flow rate of 0.33±0.02 mL/min; the JN had a VMD of 4.64±0.26 µm and an aerosol flow rate of 0.52±0.01 mL/min. The particle size data reported here represent the VMD of the nebulisers when operated outside of the respiratory circuit. However, when operating within a working respiratory circuit, the size of the aerosol particles that reach a patient, that is, post-ETT, can be much smaller than what is exiting the nebuliser.16 17
Aerosol dose characterisation
A 2.5 mL dose of albuterol sulfate (1 mg/mL) (GlaxoSmithKline, Dublin, Ireland) was aerosolised using both the VMN and the JN. Albuterol was chosen as it is a commonly nebulised formulation used by first responders in the emergency setting, as well as being the drug of choice in the characterisation of aerosol drug delivery systems, as specified in the international standard ISO 27427:2013. Aerosol dose was determined by quantifying the mass of drug captured on a filter proximal to the test lung. The mass of the drug was quantified by ultraviolet spectrophotometry at 276 nm and interpolation on a standard curve of albuterol concentrations. Results, indicating the dose delivered, are expressed as a percentage of the nominal dose placed in the applicable nebuliser medication cup.
Statistical methods
Results are expressed as the mean±SD aerosol/lung dose (percentage). Paired t-tests were conducted to establish if the aerosol dose varied significantly across different nebuliser types at different positions within the respiratory circuit. P values of<0.05 were considered statistically significant. The experiments were repeated five times independently (n=5) for each test scenario.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
In order to ensure that the DTVs could effectively deliver the required ventilation rates to the adult and paediatric patient models, a CITRIX H4 breath analyser (Intermedical AG, Buchs, Switzerland) was used to confirm the breathing patterns. Standard adult (Vt=500 mL, BR=15 beats/min and I:E=1.0:1.0) and paediatric (Vt=300 mL, BR=30 beats/min and I:E=1.0:2.0) breathing patterns were generated. For the adult patient model the following breathing patterns were generated: GO2VENT; BR: 16±2 beats/min, Vt: 495±25 mL, I:E: 1.0:1.15±0.05, Life Control mix; BR: 13.5±0.5 beats/min, Vt: 505±15 mL, I:E: 1.0:1.25±0.05 and in the paediatric model: GO2VENT; BR: 31±1 beats/min, Vt: 270±40 mL, I:E: 1.0:1.6±0.3, Life Control mix; BR: 26.5±0.5 beats/min, Vt: 250±10 mL, I:E: 1.0:1.45±0.5.
The data presented in the following section reflect the overall effectiveness of DTVs in delivering aerosol to a particular patient model rather than a tête-à-tête evaluation of the individual devices. As such, the data reported in this section are the range in lung dosages (%) delivered to the different simulated patient models. The results do, however, offer an evaluation as to the most effective form of aerosol generator and respiratory circuit arrangement that can be used to most effectively treat either an adult or a paediatric patient.
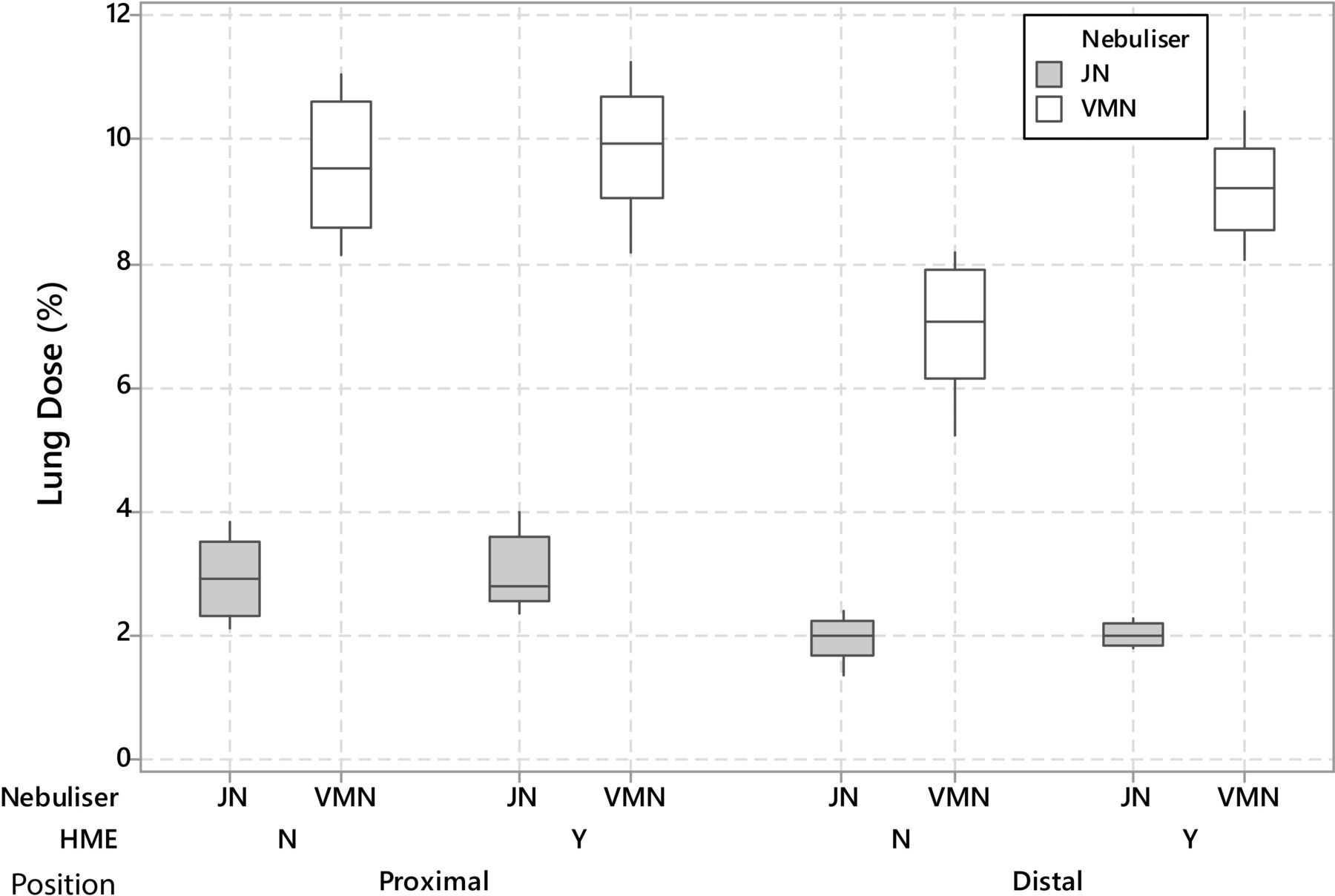
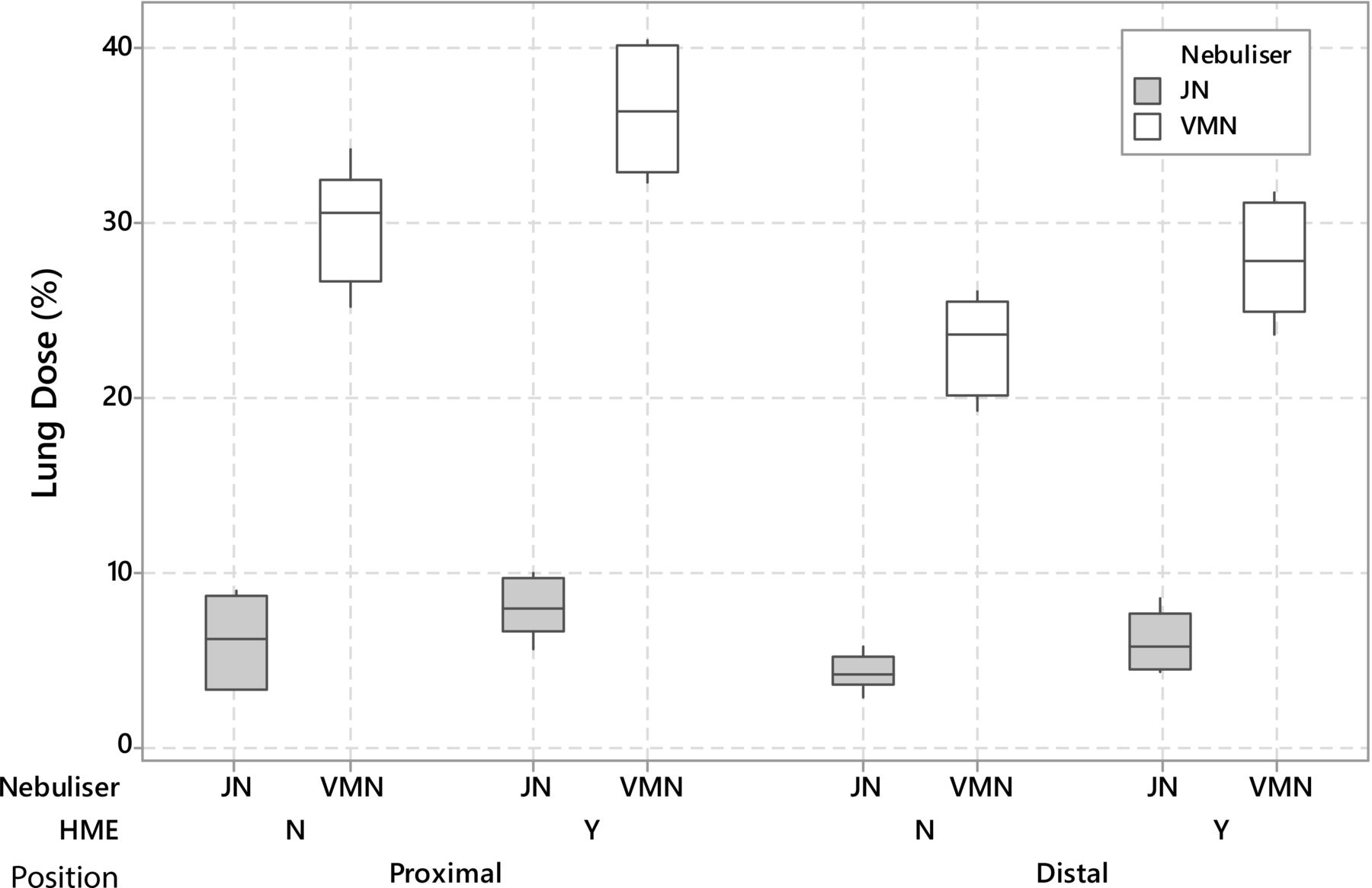
Figure 2 is a box plot comparing the performance of the two different nebulisers, at two different locations within the respiratory circuit, with and without passive humidification for a simulated, intubated, adult patient. For both nebuliser types, nebuliser position and passive humidification had a significant effect on the potential dose (%) an adult patient would receive, p<<0.05 see online supplemental table 2. The largest lung doses (%) were measured when the nebulisers, both VMN and JN, were positioned proximal to the ETT (VMN: 25.19%–34.15% and JN: 3.14%–8.92%) and when an HME was included in the respiratory circuit (VMN: 32.37%–40.43% and JN: 5.60%–9.91%). Irrespective of position and humidification in the respiratory circuit, use of the VMN resulted in the largest lung dose (%). A similar trend was recorded in the paediatric model data (see figure 3 and online supplemental table 2), where the largest lung doses (%) were measured when either nebuliser was positioned proximal to the ETT (VMN: 8.12%–10.89% and JN: 2.15%–3.82%) and the HMEF (VMN: 8.18%–11.02% and JN: 2.34%–4.00%) was incorporated into the respiratory circuit. However, the addition of an HMEF had no statistically significant effect on the potential lung dose (%) when either nebuliser was placed proximal to the ETT, that is, the position that resulted in the largest lung dose (%), p>>0.05.
Supplemental material
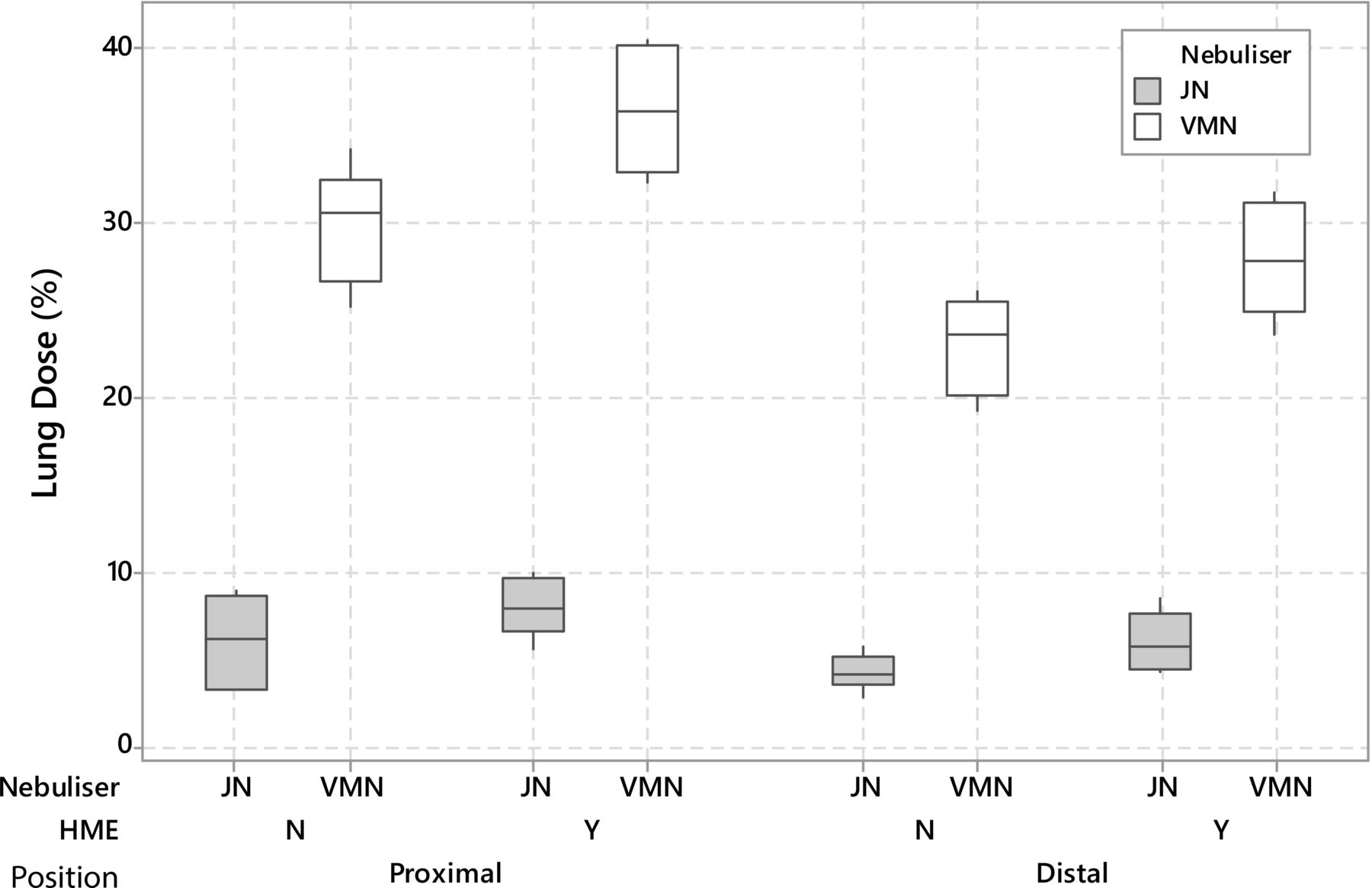
Box plot presentation of the variations in lung dose (%) with changes in nebuliser, passive humidification and nebuliser position within the respiratory circuit for a simulated intubated adult patient. The plots display the minimum, first quartile, median, third quartile and maximum lung dosages (%) measured. HME, heat and moisture exchanger; JN, jet nebuliser; VMN, vibrating mesh nebuliser.
{kind=link}
{kind=link}
{kind=link}
Box plot presentation of the variations in lung dose (%) with changes in nebuliser, passive humidification and nebuliser position within the respiratory circuit for a simulated intubated paediatric patient. The plots display the minimum, first quartile, median, third quartile and maximum lung dosages (%) measured. HME, heat and moisture exchanger; JN, jet nebuliser; VMN, vibrating mesh nebuliser.
Hence, in an adult patient, ventilated with a DTV, the nebuliser type, location in the circuit and respiratory circuit setup to maximise the lung dose (%) is as follows: a VMN, positioned proximal to the ETT and with an HMEF between the DTV and the respiratory circuit tubing. While in a paediatric patient, ventilated with a DTV, a VMN, positioned proximal to the ETT, with or without an HMEF results in the largest lung dose (%).
Discussion
This study was designed to assess the potential of DTVs to successfully deliver aerosol to simulated, intubated, adult and paediatric patient models. Similar to MV studies, the delivery of aerosol was found to be significantly influenced by the type of aerosol generator, position in the respiratory circuit and the presence of passive humidification.
The effects of aerosol generator selection on delivery efficiency have been documented in a number of publications for both adult and paediatric patients12 13 18 19 in MV studies. However, to the best of the authors’ knowledge, this is the first study to make use of a DTV to deliver aerosol. Similar to the aforementioned referenced studies, the VMN consistently outperformed the JN, for both adult, 1.4–4.6-fold higher lung dose (%),13 20 and paediatric patient models of higher lung dose (%) of 1.2–3.5-fold18 19 patient models. The data presented in this study are in line with those studies, where use of a VMN resulted in a lung dose of 2.5–5.0-fold (%) than the JN in the simulated adult patient. While in the simulated paediatric patient, use of the VMN resulted in a larger lung dose (%) of 3.0–4.5-fold. The reasons for the superior performance of the VMN over the JN have been documented previously in a number of other publications21–23 and as such do not need to be restated.
The maximum aerosol delivery was achieved when the nebuliser, VMN or JN, was positioned proximal to the ETT for either patient type (p<<0.05; see online supplemental tables 1 and 2). This result is contrary to the findings reported in numerous traditional MV studies, where the largest lung and tracheal doses (%) received by the patient occurred when the nebuliser was positioned distal to the ETT, that is, proximal to the ventilator.12 13 18 24 In the current study, when the nebuliser was placed distal to the ETT, proximal to the DTV (see figure 1), the generated aerosol must pass through a 90° turn prior to the ETT. As such, there is considerable aerosol loss and deposition at this point in the respiratory circuit, particularly when the JN is used in the circuit due to the additional air flow from the compressor required to drive the nebuliser. When positioned proximal to the ETT (see figure 1), the aerosol generators deliver aerosol directly into the ETT, therefore minimising areas within the respiratory circuit for aerosol to deposit prior to reaching a potential patient. It is proposed that the much simpler respiratory circuit arrangement used with a DTV is the reason for this contrary finding.
The potential benefits of passive humidification on the delivered lung dose (%) were also examined. An HME filter was placed in the respiratory circuit proximal to the DTV (see figure 1). HMEs are often incorporated into respiratory circuits to ensure adequate humidification as the upper airway is bypassed during intubation. Ari et al14 compared the aerosol deposition in simulated, intubated, ventilated adult patients with and without an HMEF. The authors found that the HMEF had no effect on aerosol dose (%) in the setup, which incorporated exhaled humidity. However, in the setup without exhaled humidity, the addition of an HMEF resulted in a lower delivered dose (%) than the control case (no HMEF). The present study was conducted without exhaled humidity and the HMEF was positioned proximal to the DTV, which was upstream of the nebuliser in both respiratory circuit arrangements (see figure 1). During inspiration, the circuit becomes charged with aerosol. DTV respiratory circuits are a single limb circuit and the exhalatory breath passes back through the circuit to the release port on the DTV. It is proposed that, due to its position in the respiratory circuit, the HMEF acts as a resistance to the return flow of aerosol; as such, a greater quantity of aerosol remains within the circuit to be delivered. In the paediatric patient model, it is postulated that this phenomenon does not occur due to the significant aerosol losses that occur in the smaller ETT, paediatric ETT: 5.0 mm ID 20 cm length, adult ETT: 8.0 MM ID 30 cm length, p>>0.05 when comparing lung dose (%) with and without an HMEF at the same nebuliser position in the circuit (see online supplemental table 2).
Study limitations
The intention of this study was to perform an in vitro investigation of the ability of DTVs to deliver aerosol effectively and efficiently. Limitations of the study design include the following: only a single breath type for both patient types was used and only a single JN type was used. Neither patient model incorporated exhaled humidity; additional research is required to determine the effects on dose delivery (%).
Conclusions
The findings reported in this paper show that DTVs are a viable short-term alternative to mechanical ventilators to deliver concurrent aerosol drug therapy to both adult and paediatric patients. Nebuliser type, position within the respiratory circuit and passive humidification, via an HMEF, were found to significantly affect the potential delivered dose (%) in both adult and paediatric patient models. During simulated ventilation of an adult patient, placement of a VMN proximal to the ETT, with an HMEF in the respiratory circuit, provided the highest lung dose (%). Similarly, in a paediatric patient, the VMN placed proximally to the ETT provided the highest lung dose (%); however, the addition of an HMEF to the circuit made no statistically significant difference to the result. The findings reported herein should inform caregivers on appropriate or improved device selection and consequently may have a significant effect on clinical outcomes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RMacL, MJ and MMGE conceived of and designed the study. MMGE and AOS conducted experiments, collated the data, performed some analyses and wrote the manuscript. MMGE performed the statistical analysis. All authors amended the manuscript and approved the final version.
Funding The study was funded by Aerogen Limited.
Competing interests All authors are employees of Aerogen Limited.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.