Article Text

Abstract
Importance Use of non-invasive respiratory modalities in COVID-19 has the potential to reduce rates of intubation and mortality in severe disease however data regarding the use of high-flow nasal cannula (HFNC) in this population is limited.
Objective To interrogate clinical and laboratory features of SARS-CoV-2 infection associated with high-flow failure.
Design We conducted a retrospective cohort study to evaluate characteristics of high-flow therapy use early in the pandemic and interrogate factors associated with respiratory therapy failure.
Setting Multisite single centre hospital system within the metropolitan Detroit region.
Participants Patients from within the Detroit Medical Center (n=104, 89% African American) who received HFNC therapy during a COVID-19 admission between March and May of 2020.
Primary outcome HFNC failure is defined as death or intubation while on therapy.
Results Therapy failure occurred in 57% of the patient population, factors significantly associated with failure centred around markers of multiorgan failure including hepatic dysfunction/transaminitis (OR=6.1, 95% CI 1.9 to 19.4, p<0.01), kidney injury (OR=7.0, 95% CI 2.7 to 17.8, p<0.01) and coagulation dysfunction (OR=4.5, 95% CI 1.2 to 17.1, p=0.03). Conversely, comorbidities, admission characteristics, early oxygen requirements and evaluation just prior to HFNC therapy initiation were not significantly associated with success or failure of therapy.
Conclusions In a population disproportionately affected by COVID-19, we present key indicators of likely HFNC failure and highlight a patient population in which aggressive monitoring and intervention are warranted.
- ARDS
- COVID-19
- pneumonia
- respiratory infection
- viral infection
Data availability statement
Data are available upon reasonable request and upon approvable from our institutional IRB.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Question: What are the clinical and laboratory features of SARS-CoV-2 associated with high-flow nasal cannula (HFNC) therapy failure?
Bottom line: Few characteristics, primarily laboratory measures of multiorgan failure, were significantly associated with HFNC therapy failure in an African American urban population early in the pandemic.
Why read on: In a population disproportionately affected by COVID-19, we present key indicators of likely HFNC failure and highlight a patient population in which aggressive monitoring and intervention are warranted.
Introduction
COVID-19, a virus outbreak caused by the novel Coronavirus SARS-CoV-2, first appeared in Wuhan, China and was declared a pandemic by the WHO in March 2020.1 As of 6 December 2020, the COVID-19 pandemic has resulted in over 66 million total cases worldwide and over 1.5 million deaths in the world.2 A report from the Chinese Center for Disease Control and Prevention reported approximately 14% of COVID-19 cases were classified as severe, resulting in dyspnoea, hypoxaemia, lung infiltrates >50% within 24–48 hours, or partial pressure of arterial oxygenation/fraction of inspired oxygen (PaO2/FiO2) ratio <300.3 Patients with COVID-19 with severe features are at significant risk for acute respiratory distress syndrome (ARDS) manifesting shortly after the onset of dyspnoea. Furthermore, increasing evidence has revealed that the COVID-19 pandemic has had a disparate impact on people of colour.4 5 Millett et al found while only 20% of US counties contain a majority of black Americans, they comprise 52% of all COVID-19 diagnoses and 58% of all COVID-19 deaths across the nation.4
In patients with severe hypoxia, it may be necessary to escalate treatment to invasive mechanical ventilation (MV). However, MV is associated with various adverse events such as barotrauma, pneumonia and sepsis.6 7 In patients who do not require immediate ventilatory support, non-invasive ventilation modalities may be used rather than proceeding directly to intubation. Standard non-invasive oxygen therapies have significant limitations including limitation of oxygen supply to a maximum of 15 L/min, imprecision regarding the exact amount of FiO2 delivered, and poor tolerance of both the facemask and oxygen due to inadequate heating and humidification. High-flow nasal cannula (HFNC) is an alternative oxygen modality, that has gained considerable interest as a non-invasive method of delivering substantial oxygenation to severely hypoxic patients specifically in COVID-19.8–12 Additionally, it is often better tolerated as patients report better comfort with HFNC than with standard oxygen therapy.13–15
Over the years, HFNC has gained interest due to its effectiveness in improving oxygenation, being reported to prevent the need for intubation when compared with conventional oxygen therapy without impacting mortality.16–19 In 2017, a meta-analysis of six randomised controlled trials (RCTs) (n=1892) reported that the intubation rate with HFNC oxygen therapy was lower than the rate with conventional oxygen therapy.20 Another meta-analysis of 18 trials, which included all published trials containing superiority tests with conventional oxygen therapy or non-inferiority tests with non-invasive positive pressure ventilation (NIPPV), reported similar positive findings but found no difference in the length of intensive care unit (ICU) stays when compared with conventional oxygen therapies or NIPPV.21 In 2019, a meta-analysis of nine randomised controlled trials and 2093 participants, published by Rochwerg and colleagues, found significantly decreased risk of intubation or oxygen therapy escalation in patients with acute hypoxic respiratory failure treated with HFNC.16 However, no difference in mortality, ICU length of stay or hospital length of stay was observed.
Although HFNC is proven effective, there are conflicting recommendations regarding the use of HFNC in patients with COVID-1922 23 and many institutions are reluctant to use this modality in patients with COVID-19 due to risk of aerosolisation; although, evidence supporting the increased pathogen dispersal is sparse.24 Despite the potential usefulness, the utility of HFNC in patients with COVID-19 has only been studied sparsely,9–12 25 26 thus the availability of data of use of HFNC in hospitalised patients with COVID-19 is limited but greatly needed. As Detroit was a major outbreak centre early in the COVID-19 pandemic, experienced significant disparities and mortality, and given the use of HFNC at our institution, we investigated characteristics of the use and failure of HFNC in a primarily African American population disproportionately affected by SARS-CoV-2.
Methods
Patient and public involvement statement
No public involvement was involved in the design, or conduct, or reporting, or dissemination plans of this retrospective cohort study.
Study design
We conducted a retrospective cohort study within the Detroit Medical Center that includes the following hospital sites, Detroit Receiving Hospital, Harper-Hutzel University Hospital and Sinai-Grace Hospital.
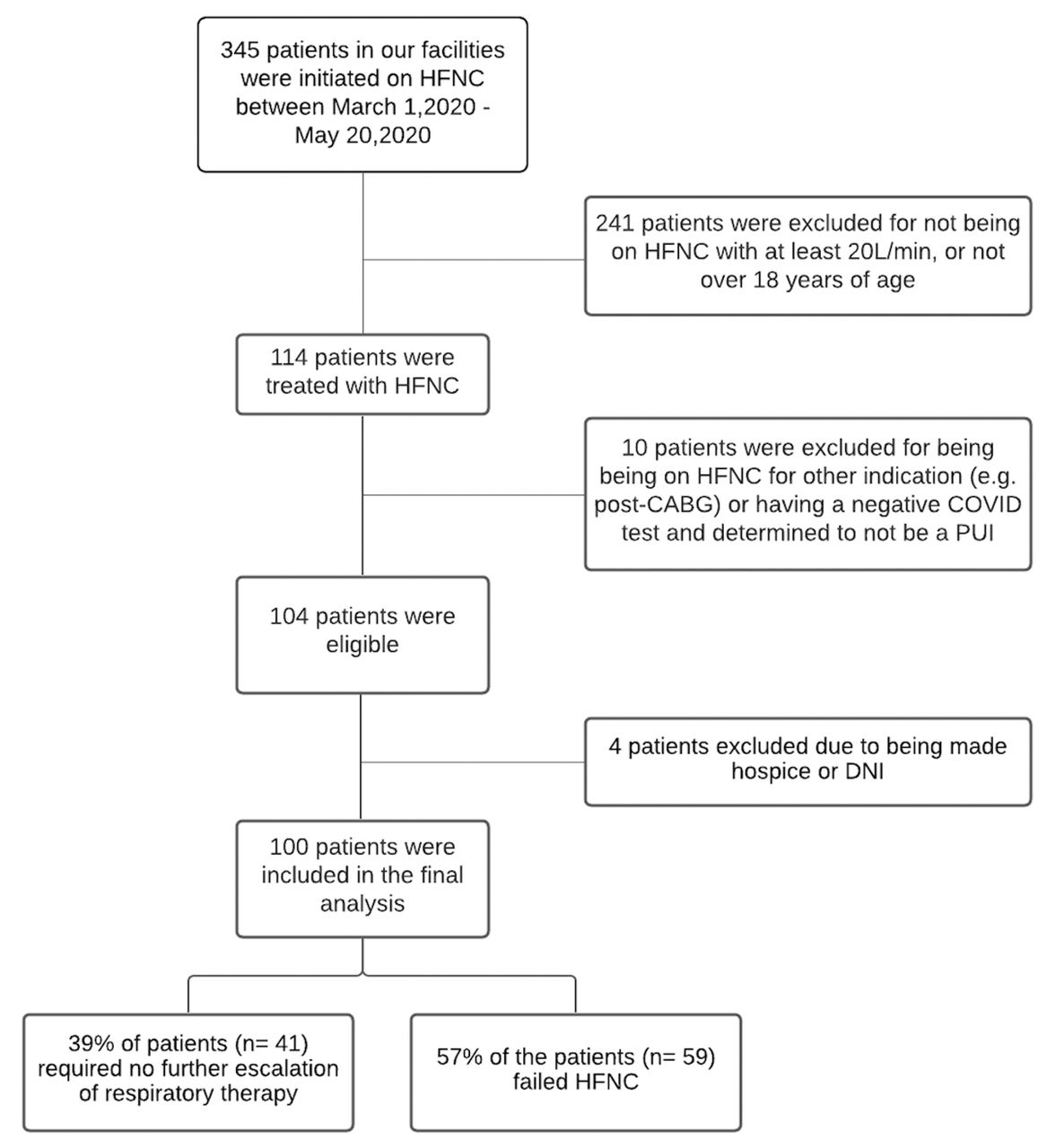
Three hundred and forty-five patients were initially identified as candidates for this study as ascertained via an institutional HFNC billing list dating between 1 March 2020 and 20 May 2020. Patients were eligible for inclusion for the study if they were (1) placed on HFNC with settings of at least 20 L/min during their hospital admission, (2) a person under investigation and/or a positive SARS-CoV-2 PCR and (3) at least 18 years of age (figure 1). Participants (n=104) were enrolled from the following Detroit Medical Center facilities, Detroit Receiving Hospital (n=40), Harper-Hutzel University Hospital (n=41) and Sinai-Grace Hospital (n=23).
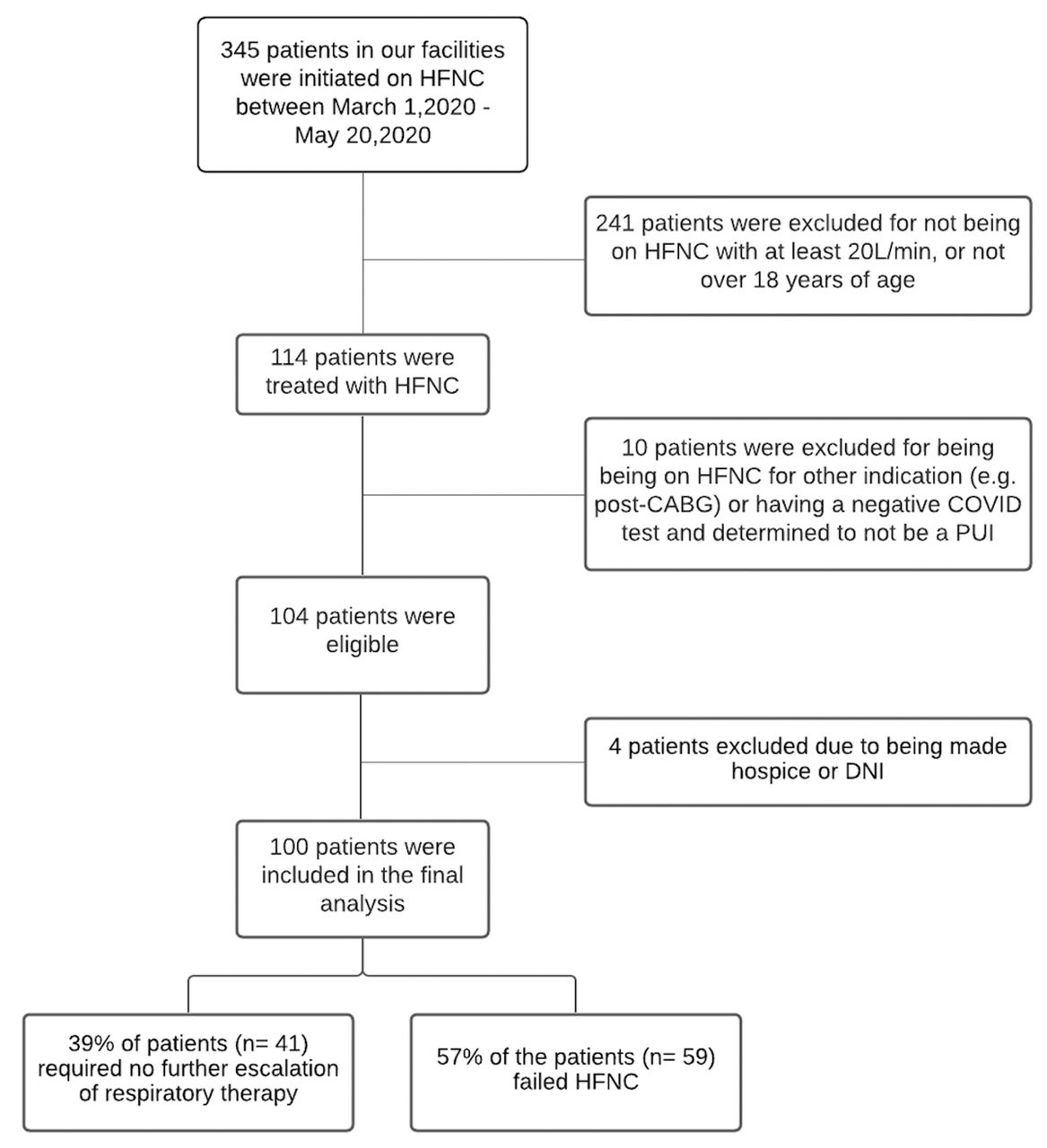
Study schema. DNI, do not intubate; HFNC, high-flow nasal cannula; PUI, person under investigation; CABG, coronary artery bypass graft.
Data acquisition
Variables of interest included age, sex, race, body mass-index (BMI), comorbid medical conditions, admission characteristics including laboratory data if collected within 48 hours of admission such as inflammatory markers and others, hospital course characteristics such as treatments received and measures of organ dysfunction, and outcomes data via medical record abstraction.
Admission characteristics included SpO2, administered FiO2, inflammatory laboratory markers C reactive protein (CRP), lactate dehydrogenase (LDH), ferritin, creatine phosphokinase and other laboratory markers, creatine, absolute lymphocyte count, D-dimer, troponin, leucocyte count, activated prothrombin time, prothrombin time, international normalised ratio (INR). We also collected admission radiographic findings on chest X-ray based on the radiological reading and separated into three classifications, normal, focal or multifocal.
Hospital course characteristics included blood and respiratory cultures if available during the admission, treatments received including use of anticoagulation, laboratory measure of organ dysfunction measured as the worst laboratory value for each patient throughout the admission for kidney injury (creatine), cardiac injury (troponin), measures of hepatic injury (alanine transaminase (ALT) and aspartate transaminase (AST)) and coagulopathy (INR). Definitions of laboratory measures of organ dysfunction were decided on a priori and based on elevations both above the standard laboratory reference range as well as what was deemed clinically significantly elevated. Hepatic injury/significant transaminitis was defined as either an elevation of ALT or AST ≥100 units/L. Troponemia was defined as an elevation of troponin ≥100 ng/L. Renal dysfunction was defined as an elevation of creatine of ≥2 mg/L. INR dysfunction was defined as an elevation of the INR ≥1.4.
Outcome variables were defined as follows: (1) HFNC failure: intubation or death while on HFNC therapy excluding patients placed into hospice care or made ‘do not intubate’ (DNI) while on HFNC, (2) ICU admission, (3) 60-day inpatient outcomes defined as discharged, remained inpatient, death or hospice/DNI. HFNC failure did not include transition to positive airway pressure (PAP) as PAP was not used during the time of this study due to initial concerns of aerosolisation risk early in the pandemic.27 Ventilator free days, measured at 28 days post-admission, is a composite outcome defined as the number of days a patient was intubation free after extubation and penalising patients who had an inpatient mortality event or who were not successfully extubated with a value of zero ventilator free days.28 Patients who were not intubated during their admission received 28 ventilator free days.
Statistical analysis
All statistical analyses were performed in R V.4.0.3 (10 October 2020). Patient characteristics and laboratory values were reported as medians and SD to limit the impact of outlier values. Primary outcomes analyses were performed using univariate logistic regression, reported as ORs with 95% CIs and two-sided p values, and plotted using the forestplot package in R. Multivariable effect estimates were estimated using logistic regression adjusted for relevant variables assessed at time of admission including age, gender, BMI and SpO2/FiO2 ratio. Elastic net regression was used to determine the combination of features from those with at least a modest univariate association (p<0.20) that were most informative and parsimonious in multivariable logistic regression predicting high-flow therapy failure using the glmnet package in R.
Results
One hundred and four patients were identified between March and May having been placed on HFNC for a corresponding SARS-CoV-2 diagnosis (table 1). Of these, the majority of patients were black (88.5%), male (58%) and older with a median age of 67 and SD of 15 years. Comorbidities were highly prevalent among these individuals, 48% with a history of obesity, 75% with a history of hypertension, 34% with a history of diabetes, 24% with a history of chronic kidney disease (CKD), 28% with a history of lung disease and 34% with a history of heart disease.
Study population characteristics
Eighty-three percent of patients had a laboratory confirmed SARS-CoV-2 infection, with 17% testing negative and clinically treated for COVID-19 given their high clinical suspicion and lack of an alternative diagnosis. On admission to the hospital, 28% of patients were found to be initially hypoxic with an SpO2 less than 88% whereas the median SpO2 for all patients on admission was 93% with an SD of 11% (table 1). Among these patients, acute phase reactants were significantly elevated in a majority of patients on admission: 71% of patients demonstrated CRP levels greater than 100 mg/L, 66% with LDH levels greater than 400 U/L and 73% with ferritin levels greater than 400 ng/mL. Likewise, 86% of patients demonstrated a positive D-dimer and 59% of patients demonstrated lymphopenia on admission. Radiographic studies on admission revealed multifocal pulmonary infiltrates in 82% of these patients and focal infiltrates in an additional 10% of patients.
Throughout the hospital course, patients often developed extra-pulmonary organ dysfunction (table 2). Most common among these was kidney dysfunction, with 80% of patients with no history of CKD developing a rise in creatine of greater than 1.1 mg/dL and 65% of the study population developing kidney injury defined as a creatine greater than 2.0 mg/dL. Additional measures of organ dysfunction include hepatic injury (transaminitis >100) in 28% of patients, cardiac injury (troponin >100) in 31% of patients and coagulation dysfunction (INR >2) in 11% of patients. When looking at secondary infections, a proportion of patients also went on to develop bacteraemia during their admission with 13.5% of patients developing positive blood cultures after excluding those with likely skin contamination. For respiratory cultures, approximately 25% of patients were found to have positive growth and notable among these were Pseudomonas (7/26) and Staphylococcus (3/26) species.
Hospital course
As these patients were admitted between March and May 2020, a majority of patients were placed on hydroxychloroquine (78.8%) and/or steroids (73.1%) during their COVID-19 admission. Use of anticoagulants among these patients varied with 43% receiving prophylaxis dosing, 45% receiving therapeutic dosing and 12% receiving no anticoagulation therapy. From an outcomes perspective, the median hospital stay was 16 days with a wide SD of 15.6 days. Initiation of HFNC among patients with SARS-CoV-2 occurred in the setting of the emergency department, general medical floor or ICU. Of those requiring HFNC therapy, 76% of patients were admitted to the ICU with a median length of stay of 9 days. Additionally, 58% required eventual intubation with a median duration of 8 days. At 60 days, only 37% were discharged from the hospital whereas 53% suffered an inpatient mortality event with an additional 8% being placed on hospice.
Prior to HFNC initiation, patients were on average hospitalised for 4 days. Approximately half of all patients received an arterial blood gas (ABG) prior to initiation, with the median demonstrating a mild respiratory alkalosis with hypoxia (online supplemental table 1). Additionally, we computed a modified sequential organ failure score (mSOFA) 24 hours prior to high flow therapy with patients demonstrating a median score of 5 and SD of 2, thus placing most patients within the lowest predicted mortality risk score category (0–7).29 On HFNC initiation, most patients were already admitted to the ICU and started with an FiO2 ranging between 85% and 100% and flow rate of 30–40 L/min with a median duration of therapy of 2 days. Seventy-six per cent of the cohort was ultimately admitted to the ICU.
Supplemental material
Primary outcome
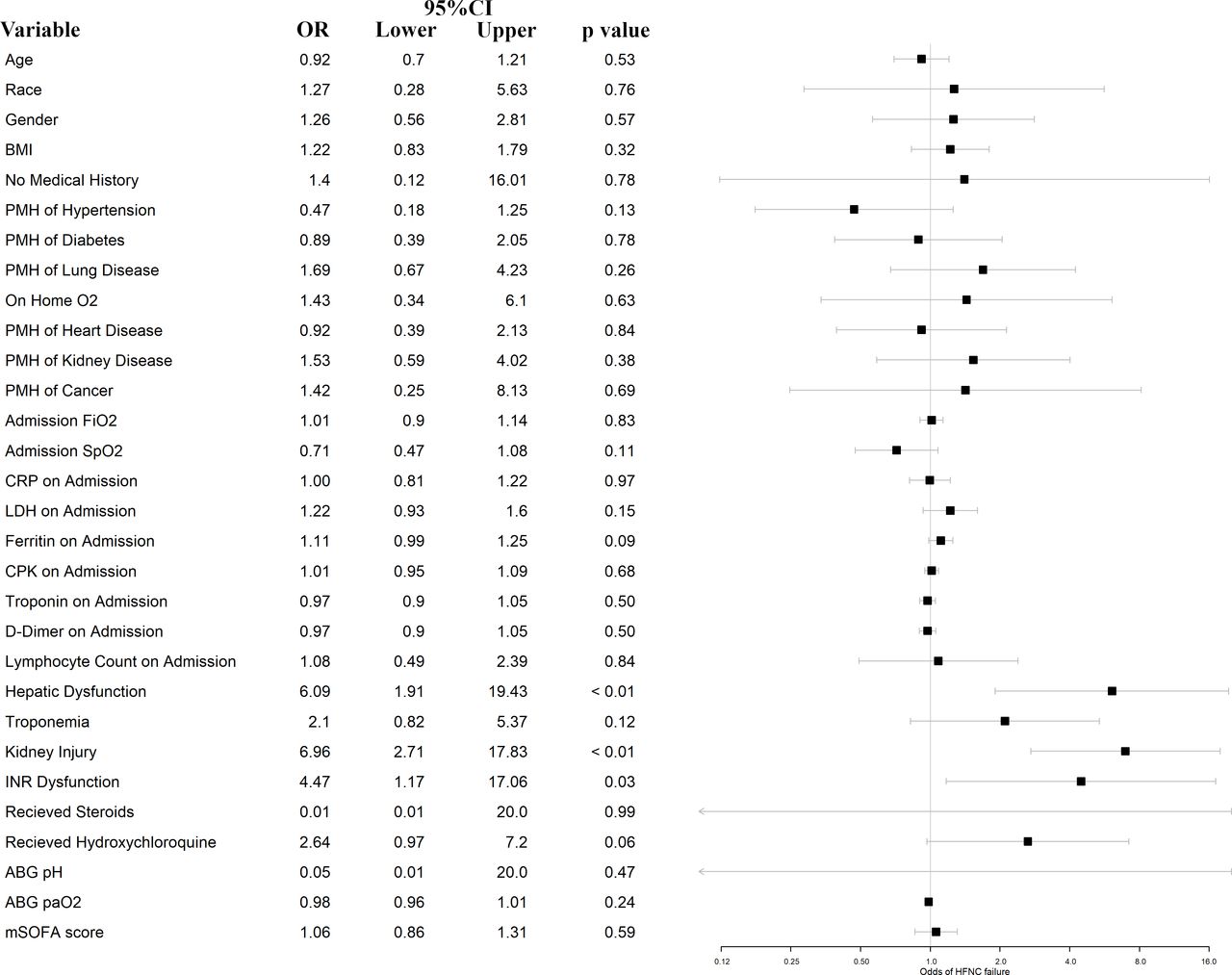
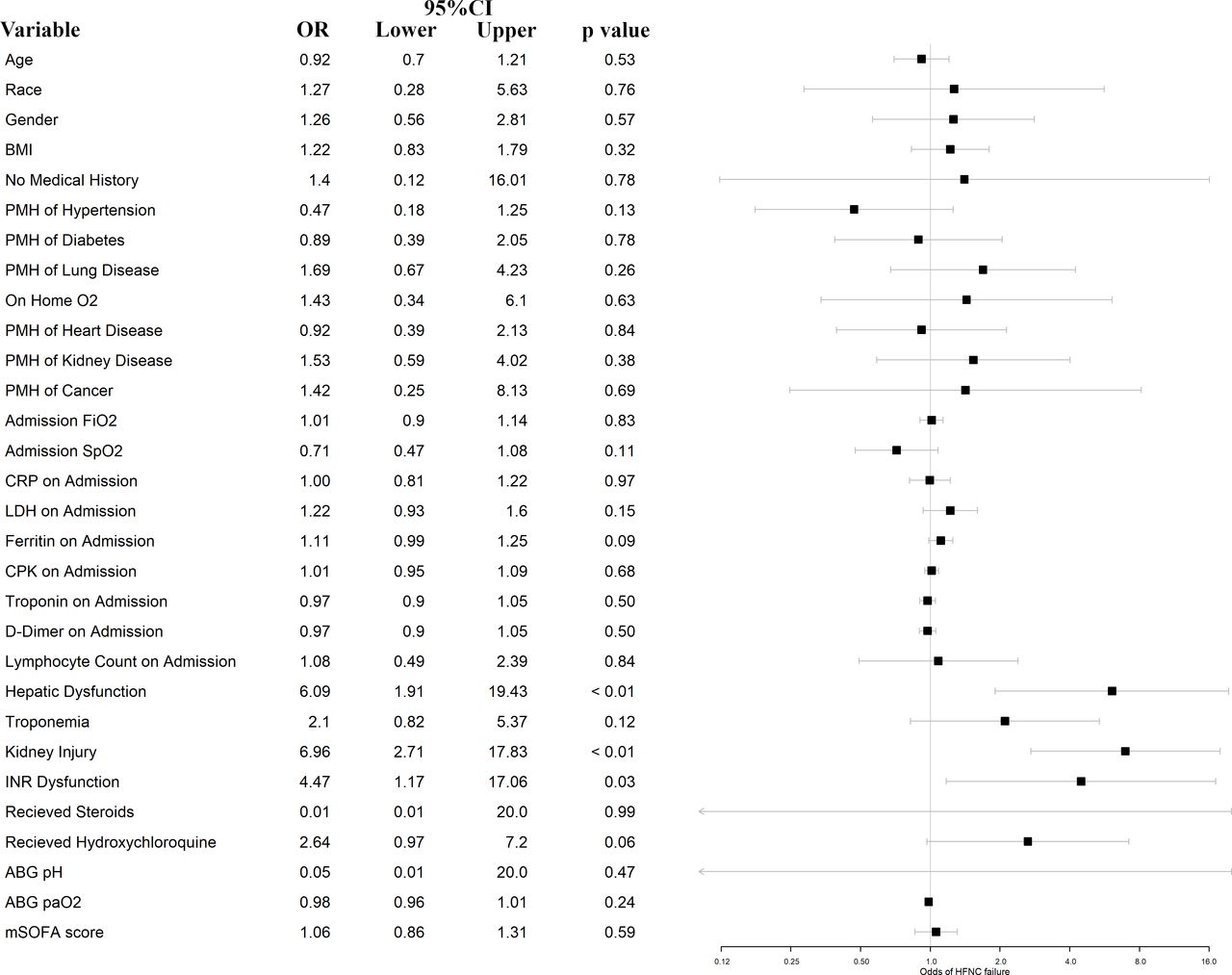
To understand patient and disease factors associated with HFNC outcomes we evaluated for association with HFNC failure defined as an event resulting in intubation or mortality while on HFNC (figure 2, table 3). Failure occurred in 57% of the patient population with 39% requiring no further escalation of respiratory therapy and 4% being made hospice or DNI while on therapy and thus excluded from further analyses. Neither demographics nor medical history were significantly associated with HFNC failure. On admission evaluation, only ferritin demonstrated a modest association with HFNC failure with an approximately 11% increased odds of failure for every increase in 100 ng/mL above 300 ng/mL (95% CI 0.98 to 1.25, p=0.09). Oxygen requirements at admission were also not associated with HFNC failure during the hospital course. However, measures of organ dysfunction, occurring during the admission, were strongly associated with HFNC failure; transaminitis was associated with a sixfold increase in failure rate (95% CI 1.9 to 19.4, p<0.01), kidney injury was associated with a sevenfold increase in failure rate (95% CI 2.7 to 17.8, p<0.01) and coagulation dysfunction was associated with a 4½-fold increase in failure rate (95% CI 1.2 to 17.1, p=0.03) and these associations persisted in the setting of covariable adjustment (online supplemental table 2). Additionally, patients receiving hydroxychloroquine trended towards a 2½-fold increase in failure rate with a modest statistical association (95% CI 0.96 to 7.20, p=0.06). Conversely, measures of arterial pH and PaO2 as well as mSOFA scoring immediately prior to HFNC initiation were not significantly associated with HFNC failure. Among patients who experienced HFNC failure, mortality was significantly elevated with an associated sevenfold increase in death (95% CI 2.8 to 18.2, p<0.01). HFNC failure was associated with an average reduction of 16 ventilator free days when assessed at 28 days (95% CI 11.6 to 20.2, p<0.01). To identify the subset of clinical and laboratory features that in combination best predicted high-flow therapy failure, elastic net logistic regression was used on features with an at least modest association with the primary outcome (p<0.20). Five features remained after regularisation of high-flow therapy failure predictors, laboratory measures of kidney (OR=7.1, 95% CI 2.3 to 21.7), hepatic (OR=4.5, 95% CI 1.2 to 17.5) and coagulation (OR=2.1, 95% CI 0.44 to 10.0) dysfunction as well as a medical history of hypertension (OR=0.26, 95% CI 0.07 to 0.94) and treatment with hydroxychloroquine (OR=4.0, 95% CI 1.12 to 14.2) in this sample.
{kind=link}
{kind=link}
Associations with high-flow therapy failure. PMH, past medical history; ABG, arterial blood gas; BMI, body mass index; CPK, creatine phosphokinase; CRP, C reactive protein; LDH, lactate dehydrogenase; INR, international normalised ratio; mSOFA, modified sequential organ failure score.
Comparison of characteristics by the primary outcome
Discussion
The COVID-19 pandemic has led to an unprecedented healthcare crisis. Patients presenting with moderate and severe SARS-CoV-2 pneumonia universally require oxygen administration, ranging from nasal cannula to MV; complicated by a widely varied disease presentation ranging from mild respiratory symptoms to cytokine storm with multisystem involvement, septic shock and severe respiratory failure.30
Presented here is to our knowledge the largest detailed investigation of the use of high flow nasal cannula in the SARS-CoV-2 pandemic in a primary African-American urban population. This sample is comprised patients admitted early during March–30 May 2020 in Detroit, USA, a first wave outbreak epicentre severely affected by COVID-19 resulting in 26 409 cases and 2947 deaths in metropolitan Detroit during this period. A considerable number of these cases occurred in minority populations (estimated to be greater than 40%), leading to a state-wide initiative, the Michigan Coronavirus Task Force on Racial Disparities, to address these disparities.31 Our study reflects these observations, as our study-eligible patient population contained a considerable proportion of African American patients (88.5%) who experienced a significantly higher burden of comorbidities that is, 76.9% with above normal BMI (overweight: 28.8%, obesity: 48.1%), followed by with hypertension (75%), diabetes (33.7%), heart disease (33.7%), lung disease (27.9%), CKD (24%) and oncological disease (6.7%), as well as elevated inpatient mortality (52.8%).
We demonstrate the characteristics and outcomes of high-flow therapy for COVID-19 early in the SARS-CoV-2 pandemic in a primarily underserved urban population. Within our sample of patients, 39% were treated with HFNC successfully and required no additional respiratory therapy escalation. These data and others support HFNC utilisation to optimise healthcare resources and potentially limit intubation in severe COVID-19 cases. A smaller study in Madrid, Spain reported similar HFNC success rates (47.5% vs 39.4%) with a mortality rate of 22.5%.12 Relative to the Detroit sample, patients studied were younger, experienced less comorbidities and presented with low CURB-65 scores indicating less severe disease. With respect to monitoring of HFNC in respiratory distress syndrome, studies have shown changes in respiratory rate and PaO2/FiO2 as indicators of imminent failure.32 Other studies have suggested using the ROX index as a marker of HFNC failure risk in patients with ARDS.33 In our facility, intubation was guided by clinical reasoning and deteriorating respiratory status of the patient and varies from clinician to clinician.
Patients also did not receive interval ABG sampling to monitor response to HFNC therapy secondary to resource and personnel shortages. Unfortunately, resource and personnel shortages were at the highest during this period of the pandemic in the Detroit medical system and healthcare provider contact with confirmed SARS-CoV-2 was limited when possible. Other such studies have similar limitations.25
In our cohort, we observed a mortality rate of 53% similar to that reported in other studies with mortality estimates ranging from 52% to 61%.34 35 These data and others,36 37 suggest HFNC use reduces intubation and subsequent MV. While these external data suggest a minimal impact on mortality, in our sample we observed a strong association of reduced mortality in individuals with COVID-19 when treated with high-flow therapy for those not requiring MV. Additional prospective studies with matched controls are necessary to determine whether this effect remains true. Mortality remains high among severe COVID-19 respiratory disease likely secondary to the complexity of the infection and development of atypical ARDS38 compounded by a higher than expected proportion of patients with hypercoagulability and multisystem involvement (hepatic, renal and cardiac injury) than reported in typical ARDS.39 40
Interestingly, our study demonstrates that COVID-19 related multi-organ dysfunction such as hepatic dysfunction (OR 6.09, 95% CI 1.9 to 19.4, p=<0.01), renal dysfunction (OR 6.96, 95% CI 2.7 to 17.8, p=<0.01) and INR dysfunction (OR 4.47, 95% CI 1.2 to 17.1, p=<0.03) are associated with increased risk of HFNC failure (figure 2). The presence and degree of the multisystem involvement could prove to be a useful tool to identify patients at high risk of HFNC therapy failure and thus subsequent need for MV. Additionally, there has been concern of elevated mortality in patients receiving delayed intubation during the use of HFNC and therefore, it is imperative to rapidly identify high-risk patients for monitoring and intervention.41 Further investigations should be pursued to evaluate these markers of HFNC therapy failure in additional SARS-CoV-2 populations and such studies should include an appropriate matched control group who did not receive HFNC to evaluate whether HFNC therapy differentially impacts mortality and whether markers of HFNC failure are useful prognosticators in COVID-19.
Limitations
Our study has several limitations. As this study is a single centre, retrospective cohort study that included fewer patients and no matched control group assessment of high-flow therapy association temporality and impact on intubation rate in COVID-19 was limited. Therefore, a prospective randomised controlled with larger cohorts and multi-centre analysis is needed to confirm our results. Additionally, our facility did not employ criteria such as the ROX index to aid in the identification of HFNC therapy failure and guide intubation usage.42 Furthermore, these patients were receiving the recommended treatment during the first wave of COVID-19 which consisted of hydroxychloroquine and steroids. As a result, this impacts the study’s generalisability as the recommended treatments continue to evolve as we continue to learn more about COVID-19.
Data availability statement
Data are available upon reasonable request and upon approvable from our institutional IRB.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by both the Detroit Medical Center and Wayne State University Institutional Review Board (IRB Protocol #20-04-2179). A waiver of consent was granted as this study was a retrospective study with minimal risk and had no patient contact.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PLN, HO and DW contributed equally.
Contributors PLN conceptualised the study. PLN, HO, DW, SK, ASharma, GD, GS, ASoubani had substantial contributions to the acquisition, analysis, or interpretation of data for the work; PLN, HO, DW, SK, ASharma, GD, GS, ASoubani drafted the work or revised it critically for important intellectual content; PLN, HO, DW, SK, ASharma, GD, GS, ASoubani had final approval of the version to be published; PLN, HO, DW, SK, ASharma, GS, ASoubani had agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.