Article Text

Abstract
Background Neural mechanisms may play an important role in non-eosinophilic asthma (NEA). This study compared airway sensory nerve reactivity, using capsaicin challenge, in eosinophilic asthma (EA) and NEA and non-asthmatics.
Methods Thirty-eight asthmatics and 19 non-asthmatics (aged 14–21 years) underwent combined hypertonic saline challenge/sputum induction, fractional exhaled nitric oxide, atopy and spirometry tests, followed by capsaicin challenge. EA and NEA were defined using a sputum eosinophil cut-point of 2.5%. Airway hyperreactivity was defined as a ≥15% drop in FEV1 during saline challenge. Sensory nerve reactivity was defined as the lowest capsaicin concentration that evoked 5 (C5) coughs.
Results Non-eosinophilic asthmatics (n=20) had heightened capsaicin sensitivity (lower C5) compared with non-asthmatics (n=19) (geometric mean C5: 58.3 µM, 95% CI 24.1 to 141.5 vs 193.6 µM, 82.2 to 456.0; p<0.05). NEA tended to also have greater capsaicin sensitivity than EA, with the difference in capsaicin sensitivity between NEA and EA being of similar magnitude (58.3 µM, 24.1 to 141.5 vs 191.0 µM, 70.9 to 514.0) to that observed between NEA and non-asthmatics; however, this did not reach statistical significance (p=0.07). FEV1 was significantly reduced from baseline following capsaicin inhalation in both asthmatics and non-asthmatics but no differences were found between subgroups. No associations with capsaicin sensitivity and atopy, sputum eosinophils, blood eosinophils, asthma control or treatment were observed.
Conclusion NEA, but not EA, showed enhanced capsaicin sensitivity compared with non-asthmatics. Sensory nerve reactivity may therefore play an important role in the pathophysiology of NEA.
- asthma
- asthma mechanisms
- asthma epidemiology
- paediatric asthma
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Is there a difference in airway sensory nerve reactivity between asthma inflammatory phenotypes and non-asthmatics?
Using capsaicin challenge, non-eosinophilic asthmatics exhibited enhanced capsaicin sensitivity compared with non-asthmatics.
Our findings suggest that sensory nerve reactivity may play a role in pathophysiology of non-eosinophilic asthmatics and may represent a novel phenotype-specific treatable trait.
Introduction
Asthma is generally associated with TH2-mediated, allergic airway inflammation.1 However, some studies show that <50% of asthma cases are attributable to airway eosinophilia,2 and that ~50% have no overt signs of either eosinophilic or neutrophilic inflammation.3 In the absence of inflammation, the mechanisms underlying non-eosinophilic asthma (NEA) remain unclear but it is plausible that neural pathways may be involved.4 While this notion is not new,5 there is increasing contemporary literature supporting a role for neural involvement: some studies suggest that altered autonomic regulation, involving vagal tone and reduced sympathetic tone, may be important,4 while others have suggested that sensory nerve activation may play a key role in asthma pathogenesis.6 7
To date, evidence of altered airway sensory nerve reactivity in asthma, often measured using capsaicin challenge to induce cough by specifically targeting the transient receptor potential (TRP) vanilloid 1 (TRPV1) channel on sensory C-fibres, is equivocal.7 One study observed an increase in capsaicin sensitivity among adult asthmatics,8 while others found no difference between asthmatics and non-asthmatics.9 10 Studies measuring associations between capsaicin response and inflammatory biomarkers including atopy,11 12 soluble mediators,13–15 fractional exhaled nitric oxide (FeNO),12 16 sputum15 17 18 and blood12 19 eosinophil percentages have also shown mixed results. We hypothesise that these inconsistencies may be due to inflammatory asthma phenotypes expressing differential sensory nerve reactivity.
No studies have examined capsaicin responses across inflammatory asthma phenotypes assessed using induced sputum, which is considered representative of ‘actual’ airway pathophysiology.20 This study compared sensory nerve reactivity between young asthmatics and non-asthmatics and across different asthma inflammatory phenotypes, and examined associations between sensory nerve reactivity and clinical, demographic and inflammatory characteristics.
Methods
Study population
Participants (14–21 years), recruited from Wellington, New Zealand (either from a birth cohort study21 or through separate community-based recruitment), completed a respiratory questionnaire based on the International Study of Asthma and Allergies in Childhood (ISAAC) Phase II survey.22 (The ISAAC study assessed the prevalence of respiratory symptoms in nearly 2 million children and adolescents in >100 countries; the survey is available at http://isaac.auckland.ac.nz/). Asthma was defined as wheezing/whistling in the chest and/or asthma medication use in the last 12 months. Non‐asthmatics reported no asthma symptoms, no other respiratory conditions or asthma medication use.
Clinical assessments
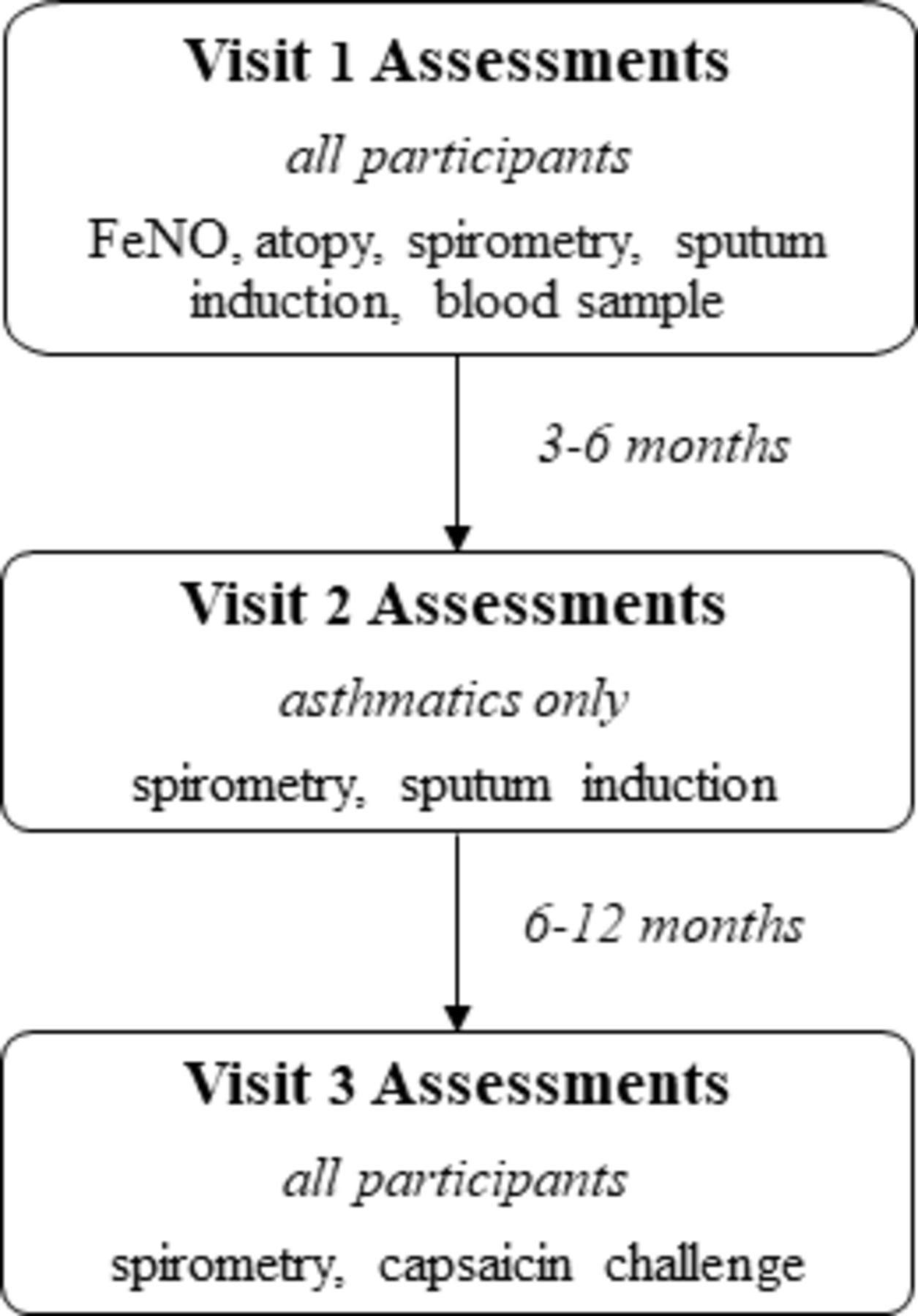
Participants took part in a maximum of three assessments (the first involving all tests described below except capsaicin challenge) (figure 1). To confirm inflammatory phenotype stability, asthmatics underwent another sputum induction 3–6 months later. Capsaicin challenge was conducted at a final assessment (second visit for non-asthmatics, third for asthmatics) for a proportion of non-smoking participants identified as either eosinophilic asthma (EA), NEA or non-asthmatics (recruitment was random within each subgroup). Capsaicin challenge was conducted 6–12 months after the final sputum induction. Asthma control was assessed using the Asthma Control Questionnaire (ACQ7).23 Participants with respiratory infection within 1 month of assessment returned when symptom-free and those with FEV1% predicted <75% were excluded. Prior to testing, asthma medication and antihistamines were withheld for ≥12 and ≥24 hours, respectively.

Timeline of clinical assessments. FeNO, fractional exhaled nitric oxide.
Spirometry and FeNO
Spirometry and FeNO was measured using an Easyone spirometer (NDD Medizintechnik AG, Zurich, Switzerland) or Hypair FeNO analyser (Medisoft, Sorinnes, Belgium) as described previously.3 24
Atopy
Skin prick tests were conducted using a panel of aeroallergens as described previously: house dust mite, tree mix, grass mix, cat and dog dander, Alternaria tenuis and Penicillium mix (Stallergenes Greer, Sydney, Australia). Atopy was determined by presence of at least one weal >3 mm.3
Blood eosinophils
Blood was collected using BD-vacutainers (BD, Auckland, New Zealand) for a complete blood count. A high blood eosinophil count (blood EOS-high) was defined as ≥250 eosinophils/mm3.25
Combined hypertonic saline challenge and sputum induction
Hypertonic saline challenge/sputum induction was conducted as described previously.26 Briefly, aerosolised hypertonic saline (4.5% w/v) was produced using an ultrasonic nebuliser (DeVilbiss Ultraneb 2000, Langen, Germany) and administered orally through a mouthpiece (Hans-Rudolph, Kansas City, USA) for increasing intervals from 0.5 to 4 min, to a total of 16 min. Spirometry was conducted between intervals, and salbutamol was administered if FEV1 dropped to ≤75%-predicted. During the procedure, the number of coughs was not counted. Participants were subsequently encouraged to produce sputum in a sterile plastic container. Sputum plugs were dispersed using dithiothreitol (Sputasol, Oxoid, Basingstoke, Hampshire, England). The suspension was filtered through a 60 µm filter (Millipore, County Cork, Ireland) and total cell count and viability performed. Following centrifugation, supernatant was aspirated and stored at −80°C and the resulting cell suspension was used to prepare cytospin slides stained using a Diff-Quik fixative/stain set (Dade Behring, Deerfield, Illinois, USA). A differential cell count of 400 non-squamous cells was made using light microscopy. Samples were considered to be adequate for analysis if they had a squamous cell contamination <30% and >400 total non-squamous cells on one slide. EA was identified as ≥2.5% eosinophils at any visit and NEA as <2.5% eosinophils at both visits. Airway hyperreactivity (AHR) was defined as a ≥15% drop in FEV1 from baseline.26
Capsaicin challenge
Capsaicin challenge was conducted as described previously11 with minor modifications. Capsaicin (Sigma-Aldrich, Castle Hill, Australia) was solubilised in ethanol/Tween 80.11 Participants inhaled single breaths of aerosolised capsaicin solution in doubling concentrations (0.98–500 µM) from a jet fnebuliser (model 646, DeVilbiss, Langen, Germany) controlled by a KoKo dosimeter (nSpire Health, Louisville, Colorado, USA). One-minute intervals were maintained between different concentrations. The lowest concentration eliciting 2 (C2) and 5 (C5) coughs during a 30 s interval between each concentration was manually recorded by a nurse. The procedure was terminated if/when the C5 threshold was reached. If C2 or C5 was not reached, a value of 1000 µM was assigned for analysis. Lung function was measured before and after capsaicin challenge.
Power and statistical analysis
The primary aim of this study was to compare capsaicin response in asthmatics and non-asthmatics, and EA and NEA. Based on power calculations conducted prior to commencing the study, which assumed a differences in concentration of capsaicin to elicit 2 coughs of 53.6 (19.0) μmol/L in asthmatics and 116.0 µmol/L (SD 58.1) in non-asthmatics,27 we determined that 20 participants in each subgroup (non-asthmatics, EA and NEA) would be sufficient (>99% power) to detect statistically significant differences between asthma phenotypes, or between either asthma phenotype and non-asthmatics.
Analyses were performed using STATA V.11.0 (STATA Corp, College Station, Texas, USA) and GraphPad Prism 7.0 (Graphpad Software, La Jolla, California, USA). C2 and C5 values were expressed as geometric means (GM) with 95% CI, and C5 used as the primary outcome.11 Mann-Whitney U tests, unpaired t-tests or χ2 tests were used as appropriate. Linear regression was conducted using log-transformed C5. Regression coefficients were exponentiated and presented as relative differences that is, ratios (per unit increase for continuous variables and compared to the reference category for categorical variables). Ratios of >1 represent reduced capsaicin sensitivity whereas ratios of <1 represent heightened sensitivity. If significant associations were found, sensitivity analyses (excluding subgroups with or without specific characteristics) were conducted to assess robustness of findings.
Results
Population characteristics
Thirty-nine asthmatics and 21 non-asthmatics were recruited (12 asthmatics and 20 non-asthmatics from the previous birth cohort study21 and 27 asthmatics and 1 non-asthmatic through community-based recruitment). One asthmatic and two non-asthmatics were excluded due their FEV1 being ≤75% predicted, leaving 38 asthmatics and 19 non-asthmatics. Asthmatics were slightly younger but no differences in sex, ethnicity, or FeNO were observed (table 1). Prevalence of atopy, AHR and sputum eosinophil percentages were higher in asthmatics. Of the asthmatics, 18% were classified as uncontrolled, 26.3% as partly controlled and 55.4% as well-controlled. Participants recruited from the community were slightly younger than participants from the birth cohort (mean age: 18 vs 21 years), but all other baseline characteristics were comparable (data not shown).
Population characteristics
Inflammatory phenotypes
Fifty‐three per cent (n=20) of asthmatics were NEA at both visits 1 and 2, with the remaining 47% (n=18) EA. EA were more likely to be atopic, and have AHR, higher FeNO, and more poorly controlled asthma than NEA (table 1). There were no differences in nocturnal cough symptoms (table 1). Neutrophilic asthma or mixed granulocytic asthma28 were not detected, and sputum neutrophil levels were not significantly different between groups (table 1).
Capsaicin response and inflammatory phenotypes
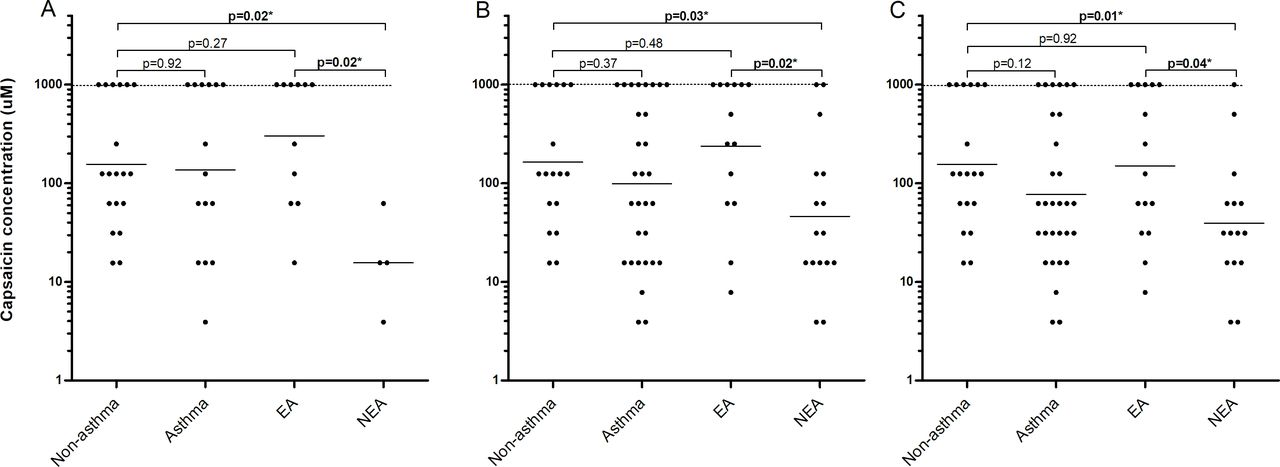
Capsaicin response did not differ between asthmatics and non-asthmatics (figure 2A,B) and was not associated with recruitment source (data not shown). However, NEA had significantly greater capsaicin sensitivity than non-asthmatics (GM 58.3 µM, 95% CI 24.1 to 141.5 vs 193.6 µM, 82.2 to 456.0; figure 2B). NEA tended to also have greater capsaicin sensitivity than EA, with the difference in capsaicin sensitivity between NEA and EA being of similar magnitude (58.3 µM, 24.1 to 141.5 vs 191.0 µM, 70.9 to 514.0) to that observed between NEA and non-asthmatics; however, this did not reach statistical significance (p=0.07). Using sputum eosinophil cutoffs of either 1%28 or 3%29 to define EA and NEA did not affect these findings (data not shown). Results for C2 showed no differences between groups (figure 2A). When excluding participants with elevated blood eosinophil levels (to avoid potential NEA phenotype misclassification), capsaicin sensitivity remained higher in NEA (C5 72.9 µM, 14.2 to 374.9) than non-asthmatics (170.0 µM, 71.7 to 403.0), but findings were no longer statistically significant. When subjects were stratified by atopy (online supplemental figure 1) or blood eosinophils (online supplemental figure 2) rather than EA/NEA, we found no significant differences in C2 or C5 between groups.
Supplemental material

Concentrations (μM) of capsaicin eliciting (A) 2 coughs (C2) or (B) 5 coughs (C5) in participants with and without asthma, and eosinophilic asthma (EA) and non-eosinophilic asthma (NEA). Dashed lines at 1000 µM represent values assigned to those participants who did not achieve C2 or C5 during testing. Solid line represents geometric mean. Mann-Whitney test was used. *p<0.05.
Capsaicin response and demographic/clinical characteristics
In asthmatics and non-asthmatics, no associations were found between capsaicin sensitivity and demographic parameters, asthma control, lung function, inflammatory markers, treatment or AHR (table 2). In EA, capsaicin sensitivity was significantly lower for Europeans (n=14) compared with non-Europeans (n=4; table 2). Capsaicin sensitivity was also significantly lower for those with (n=11) compared with without AHR (n=7; ratio=7.94, p<0.05). In NEA, C5 was inversely associated with FeNO (ratio=0.99 per unit increase, p<0.05) and positively associated with FEV1/FVC% predicted (ratio=1.12 per unit increase, p<0.05; table 2).
Associations between demographic and clinical characteristics and capsaicin response (C5)
Sensitivity analyses
Post hoc sensitivity analyses were conducted for characteristics independently associated with capsaicin response. Limiting analysis to asthmatics with AHR, we found that capsaicin sensitivity was significantly greater in NEA (15.6 µM, 2.6 to 95.0) than non-asthmatics (193.6 µM, 82.2 to 456.2) and EA (441.0 µM, 127.0 to 1533.0; figure 3A). Excluding non-Europeans (n=9) showed significantly increased capsaicin sensitivity in NEA (50.3 µM, 18.0 to 139.0) compared with non-asthmatics (206.0 µM, 84 to 507), and EA (320 µM, 104 to 989; figure 3B). To clarify the potential role of treatment status, we conducted further sensitivity analysis including only asthmatics who used either ICS or β-agonists (excluding n=5 NEA and n=3 EA). This also showed statistically significant (p<0.05) enhanced capsaicin sensitivity in NEA (39.4 µM, 16.9 to 91.4) compared with non-asthmatics (155.5 µM, 76.2– to 317.6) and EA (150.4 µM, 58.4 to 387.1; figure 3C). We also conducted sensitivity analysis based on lung function, FeNO (excluding NEA with elevated FeNO levels to address the issue of potential phenotype misclassification), ICS-use alone and gender (online supplemental results, online supplemental figures 3 and 4). These did not have an appreciable effect on the main findings (although in some cases results were no longer statistically significant).
{kind=link}
{kind=link}
{kind=link}
Concentration (μM) of capsaicin eliciting 5 (C5) coughs in participants with AHR (A), Europeans only (B), and in participants using inhaled corticosteroids (ICS) or β-agonist medication (C). Dashed lines at 1000 µM represent values assigned to those participants who did not achieve C2 or C5 during testing. Solid line represents geometric mean. Mann-Whitney test was used. *p<0.05. AHR, airway hyperreactivity; EA, eosinophilic asthma; NEA, non-eosinophilic asthma.
Capsaicin challenge and spirometry
FEV1%-predicted and FVC%-predicted were significantly reduced following capsaicin challenge in asthmatics and non-asthmatics. However, this was not different between subgroups, including EA and NEA (table 3).
Changes in lung function following capsaicin challenge
Discussion
This study found enhanced airway sensory nerve reactivity in NEA compared with non-asthmatics, while no difference between EA and non-asthmatics was found, suggesting that sensory nerve reactivity may play a role in the pathophysiology of NEA but not EA. No associations between capsaicin sensitivity and atopy, sputum eosinophils, blood eosinophils, asthma control or treatment were observed. However, AHR was associated with reduced capsaicin sensitivity in EA, while FENO was associated with increased capsaicin sensitivity in NEA.
Although our findings are consistent with some previous reports showing no difference in capsaicin response between asthmatics and non-asthmatics,9 10 other studies found a heightened capsaicin response in asthma.8 12 These inconsistencies may be due to demographic and methodical differences, or alternatively, as suggested here, airway sensory nerve reactivity may be specific to inflammatory phenotypes, with differences masked for comparisons with general asthma.
To our knowledge, a direct relationship between sensory nerve reactivity and NEA has not previously been shown. However, recent studies have suggested an association with non-atopic asthma,7 which, like NEA, may be driven by non-TH2 mechanisms.2 For example, one study reported that capsaicin-induced cough was more pronounced in non-atopic asthmatics compared with atopic asthmatics or non-asthmatics.12 Another study suggested that heightened capsaicin sensitivity is associated with poor asthma control/severity in non-atopic asthmatics.19 However, data are equivocal and a study in non-asthmatics found no association with atopy,11 suggesting that atopy does not reliably predict capsaicin response. In agreement, we observed no differences between non-atopic and atopic asthmatics, or between atopic or non-atopic individuals in general. However, our study was not powered to examine capsaicin response in non-atopics, who made up a small proportion (16%) of asthmatics, as is typical in New Zealand.3
Few studies have assessed associations between airway inflammation and sensory nerve reactivity; these yielded inconsistent results, possibly due to asthmatic airway inflammation heterogeneity. Three studies showed no association between capsaicin response and sputum eosinophilia15 17 18; however, in these studies capsaicin response was assessed in allergic asthmatics or following allergen challenge, which likely excluded individuals with TH2-low inflammation and/or NEA. Other studies used FeNO12 16 or blood eosinophils12 19 as indicators of TH2-mediated airway inflammation, and again, results varied.16 30 In the present study, we used multiple TH2-indicators; both systemic (atopy, blood eosinophils) and airway-specific (FeNO, sputum eosinophils), but an increased capsaicin response was observed only in NEA. Capsaicin sensitivity was also associated with FeNO in NEA, but this association (a 1 ppb FeNO increase was associated with 1% greater capsaicin sensitivity) was small, and unlikely to be of clinical significance. The reasons for the mixed findings between studies are unclear, but it is possible that, while elevated FeNO and blood eosinophils are markers of TH2 inflammation, they may not be specific enough to accurately identify airway inflammatory patterns, and in particular, NEA (in our study 75% of NEA were atopic). This is supported by previous data showing that blood eosinophils and FeNO levels do not accurately predict sputum eosinophil percentages.20
The causes of enhanced sensory nerve reactivity in NEA are unknown. However, viruses and irritants, identified as potential triggers of asthma,7 and NEA in particular,2 may play a role. These may result in sensory nerve TRPV1 channel activation or increased expression, leading to increased cough response, even in the absence of other pathophysiology, such AHR (as observed in the EA group in this study), or inflammation.7 Similar hyperresponsive capsaicin-sensitive phenotypic changes have been reported in vasomotor rhinitis, despite no evidence of nasal mucosal inflammation.31 Alternatively, increased capsaicin response may be due to alterations in the afferent pathways or neuronal networks upstream of initial TRPV1 activation.7
Although we found no statistically significant associations with characteristics previously associated with capsaicin sensitivity such as age,15 gender,12 asthma control19 or treatment,8 we observed an association with ethnicity in EA. There are few studies examining associations between either sensory nerve reactivity or inflammatory phenotypes and ethnicity, and of the former, no association has been found.32 As our finding was based on very small numbers, it may be due to chance.
Consistent with other studies,8 19 baseline lung function was not associated with capsaicin response. However, following capsaicin challenge, FEV1%-predicted and FVC%-predicted were slightly decreased across all groups with no differences between subgroups. This is in agreement with previous studies showing that capsaicin does not cause clinically significant bronchoconstriction in asthmatics.12 Our results suggest that while capsaicin produces an increased tussive response in NEA, it is not associated with clinically significant AHR in this (or any other) group.
The observation that increased sensory nerve reactivity is associated with NEA may have significant implications. As reported previously, NEA makes up >50% of asthma3 and is less responsive to ICS,33 the mainstay drug in asthma management. There is therefore a substantial and unmet need in the therapeutic management of this group. If sensory nerve reactivity plays a role in the pathology underlying NEA and is therefore a potential treatable trait,34 then accurately identifying individuals with increased airway sensory reactivity, and developing specific therapeutic approaches targeting this, will be important. Of particular interest, recent reports suggest that anticholinergics (which are effective in some but not all asthma)35 may markedly reduce airway reactivity to a variety of stimuli including capsaicin.4 Tiotropium bromide reduces both cough and cough-reflex sensitivity in asthma refractory to ICS/LABA.36 Alternatively, P2X3 antagonists (which have shown promise in the treatment of refractory chronic cough) may be of benefit.37 However, it is currently unclear whether these will be effective in NEA, which was not associated with nocturnal cough symptoms in this study. It is also possible that capsaicin treatment itself may be beneficial in sensory nerve hyperreactivity in NEA, as has been shown in vasomotor rhinitis.38 Finally, in addition to results being relevant to treatment, our findings suggest that capsaicin challenge, in conjunction with other methods such as sputum induction, AHR, FeNO and atopy testing, may be a useful tool to differentiate between asthma phenotypes, and provide important clues regarding causal (non-allergenic) exposures.
This study has limitations. First, the number of participants, particularly when stratified by phenotype, was relatively small. Although power calculations, based on limited observations from other studies, suggested sufficient power (see Methods), differences observed in our study were somewhat smaller than we had assumed and power to detect differences between groups was therefore reduced. This may explain why there was a significant difference between NEA and non-asthmatics, and a similar difference between NEA and EA that did not reach statistical significance, involving slightly smaller numbers. In addition to reduced power, this study involved multiple comparisons, which may have contributed to some chance findings. However, for our main aim (to assess whether capsaicin responses are different across asthma inflammatory phenotypes, and non-asthmatics) and focusing on the primary outcome (C5), we found 7 (43.8%) statistically significant (p<0.05) findings across 16 comparisons (figures 2B and 3C), which is considerably more than expected based on chance alone (0.8; 5%). Therefore, based on the fact that results were highly consistent across multiple sensitivity analyses, we believe that these results are unlikely a chance finding. For table 2, which summarises the results of our secondary aim (to examine associations between sensory nerve activity and clinical, demographic, and inflammatory characteristics in asthmatics) we had fewer statistically significant findings (4 out of 54 (7.4%) compared with 2.7 (5%) expected for comparisons in asthmatics). Therefore, those associations are more likely explained by chance and should therefore be interpreted with a degree of caution.
Second, asthmatics were generally well-controlled and identified using an epidemiological definition and not on the basis of objective tests (such as bronchodilator reversibility and/or AHR). Therefore, some misclassification may have occurred, particularly for NEA, in which asthma symptoms are often present in the absence of objective measures (such as AHR).39 However, we consider that any bias introduced as result will be minimal as this approach, used in previous studies,40–42 generally compares well with clinical diagnoses,40 and has been shown to be better than some objective measures.41 Indeed, there are several issues with objective testing for confirmation of asthma diagnosis in a community based setting, particularly given the inherently variable nature of asthma, and that most asthmatics are not treatment naïve (>60% in the current study were using ICS at the time of assessment). This (among other reasons) has led to recommendations that asthma be considered on the basis of symptoms rather than pathophysiology.43 In this study, of the 38 participants who we defined as asthmatics, 34 had their asthma diagnosed by a doctor (as indicated from the questionnaire); of the four subjects that were identified as asthmatic with no doctor diagnosis of asthma, three had used inhaled ICS in the past 14 days. Therefore, only one subject was defined based on respiratory symptoms alone. Excluding this person from the analyses did not materially change the results, although p values increased marginally (data not shown). Also, the main study findings were similar when applying a more stringent definition of asthma, that is, restricting analysis to only asthmatics who used ICS or β-agonists, or with AHR; suggesting that associations observed are robust and unlikely to be due to asthma misclassification.
Third, due to the cross-sectional nature of the study, capsaicin challenge was not repeated and reproducibility of capsaicin response in inflammatory phenotypes remains unstudied. However, a high degree of reproducibility of capsaicin response has been documented previously.44 Fourth, there is a possibility that at least some of the NEA cases may be EA in which ICS suppressed airway eosinophilia.33 However, post hoc analysis, excluding the four NEA participants who used ICS in the last 14 days, did not have an appreciable effect (although results were no longer statistically significant). Fifth, information regarding cough symptoms and medication use was collected on the basis of participant self-report using the ISAAC questionnaire. As such, data regarding ICS dose or asthma treatment step were unavailable, and although we have data regarding nocturnal cough symptoms, no information on daytime cough frequency was collected. We were therefore unable to determine if capsaicin response was associated with daytime or overall cough frequency. Finally, it has been suggested that that a non-linear fix-modelling procedure may be more appropriate than fixed C2/C5 endpoints.12 However, in this study, capsaicin challenge was terminated on reaching C5 (to avoid further participant discomfort). Hence, non-linear fix-modelling was not feasible.
In conclusion, our study shows that sensory nerve reactivity may play an important role in the pathophysiology of mild-to-moderate NEA in young adults. Although it is not yet clear if this is relevant in older groups or more severe asthma, we suggest that sensory nerve reactivity may represent a novel therapeutic target in NEA, a group in which current asthma medications have previously been shown to be less effective.33
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Informed consent was obtained from participants/parents, and the study was approved by the Northern B Health and Disability Ethics Committee (15/NTB/2).
Acknowledgments
We are grateful to the study participants, Elizabeth Harding, Angela Thurston, Christoph Martens, Stephanie Hobbs and Mary Tohill, for conducting the clinical assessments, Prachee Gokhale and Jeroen Burmanje for their involvement with sample processing, and Soo Cheng for her involvement in data analysis. We would also like to thank colleagues at the Centre for Translational Physiology, Otago University, Wellington, for allowing us to use their facility for the clinical assessments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JD and CB contributed to the initial conception and design of the study. JD, CB, JC, RB, SH, PG, PP, Y-CT, TS and NP contributed to the final design of the study and the acquisition of research funding. HA, CB, JD, JC, RB, PP, Y-CT and TS contributed to data collection. All authors contributed to analysis and interpretation of the data. HA, CB and JD produced the first draft of the paper. All authors participated in preparing the final manuscript.
Funding The Centre for Public Health Research is funded by a Programme Grant from the Health Research Council (HRC) of New Zealand, and this research was funded by an HRC Project Grant.
Competing interests RB reports research funding from Health Research Council of New Zealand, AstraZeneca, GlaxoSmithKline and Genentech; and personal fees from AstraZeneca, Theravance, GlaxoSmithKline, Cipla and Avillion, outside the submitted work. PG reports research grants and personal fees from AstraZeneca, GlaxoSmithKline, Novartis outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.