Article Text

Abstract
Introduction Pleural exudative effusions without diagnosis after initial work up are a frequent problem in any respiratory division. Several ways to obtain pleural biopsy exist. Thoracoscopy is one of the most frequently used. Differential diagnosis mainly exists out of malignant pleuritis, tuberculosis, nonspecific pleuritis and rarely systemic or autoimmune disease. We performed a retrospective data analysis of our almost 10-year period experience, the first Belgian data to be published.
Methods We performed a retrospective data analysis of all patients with unexplained pleural exudates who underwent diagnostic medical thoracoscopy under general anaesthesia in our respiratory department during the period 2006–2015. We report on diagnoses made, sensitivity and specificity, safety of thoracoscopy and follow-up of patients after thoracoscopy.
Results 131 patients underwent diagnostic medical thoracoscopy during the inclusion period. 44.3% (n=58) of the patients were diagnosed with malignant pleuritis, 45.0% (n=59) with nonspecific pleuritis, 7.6% (n=10) with tuberculous pleuritis and some with other benign conditions. Complications are comparable to other data published. Six months follow-up of patients with non-specific pleuritis reveal 8.5% (n=5) of these patients to have malignant pleuritis, and another 8.5% (n=5) with infectious or other benign conditions.
Conclusion Medical thoracoscopy under general anaesthesia for diagnostic work up of pleural exudates of unknown origin generally has a high diagnostic yield. It is generally safe, certainly compared with the information it delivers. During follow-up, minority of patients with nonspecific pleuritis will prove to be malignant in origin, benign or autoimmune disease related.
- tuberculosis
- thoracic surgery
- systemic disease and lungs
- small cell lung cancer
- pleural disease
- non-small cell lung cancer
- lung cancer
- mesothelioma
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- tuberculosis
- thoracic surgery
- systemic disease and lungs
- small cell lung cancer
- pleural disease
- non-small cell lung cancer
- lung cancer
- mesothelioma
Key messages
What is already known on this topic
Thoracoscopic pleural biopsy is proposed to be the preferred way in the further workup of pleural exudates of unknown origin.
What this study adds
This study provides the first Belgian data on this subject. These national data confirm international data on diagnostic yield and safety of diagnostic thoracoscopy in pleural exudates.
How this study might affect research, practice or policy
This study consolidates the important role of thoracoscopic pleural biopsy in work up of pleural exudates of unknown origin. It also provides very useful information for everyday respiratory practice, for example, in differential diagnosis and follow-up of pleural exudates of unknown origin.
Introduction
The incidence of pleural effusions is around 320 per 100 000 per year in industrialised countries, representing approximately 1.5 million new patients in the USA.1 Initial work up (anamnesis, physical exam, ECG, chest X-ray, blood sample and thoracocentesis) can yield a diagnosis in up to 74% of patients.2 3 So approximately one in four effusions remains of unclear origin. Further diagnostic procedures usually comprises repeat thoracocentesis (which can yield an extra 27% of diagnoses4) and pleural biopsy. Pleural biopsy is most frequently performed by thoracoscopy. The main advantage of thoracoscopic biopsy is that a specimen of the most abnormal pleural surface can be examined. Second, when inspection shows suspicion of malignancy, poudrage can be performed. Diagnostic yield of thoracoscopy has been reported to be up to 93%.5
This study represents our experience during an almost 10-year period with diagnostic thoracoscopy in patients with pleural exudates without a diagnosis after initial little invasive evaluation.
Methods
Patients
All patients referred for medical diagnostic thoracoscopy in the Respiratory Division of the University Hospital Brussel from 1 January 2006 to 31 August 2015 were included. Patients with an unexplained persisting pleural exudate, deemed fit enough for thoracoscopy and in whom a change in treatment could be expected, were referred. Patients’ identification data were kept in a database. All patients in the database were analysed, no patients were excluded.
Patient and public involvement
Since this study has a retrospective design, patients nor the public were involved in the design.
Thoracoscopy procedure
All patients underwent general anaesthesia in the operating theatre, an experienced respiratory physician performed the procedure. Patients were intubated with a single lumen endotracheal tube with jet ventilation during lung deflation. Patients were placed in lateral decubitus, and after skin sterilisation blunt dissection was used to insert the rigid thoracoscope at nipple height, at the mid to anterior axillary line. Another opening was made to insert the biopsy forceps. Pleural space was inspected as completely as possible. Biopsies were taken at the most suspicious changes of the parietal pleura, and if the pleura seemed macroscopically normal, biopsies were taken in the posterior costodiaphragmatic sinus. At least four biopsies were sent for histological analysis, direct exam (including acid fast staining) and culture (including mycobacteria). Talc poudrage was performed when malignancy was suspected, using 2 g of sterile talc. Before wound closure a chest tube was inserted, and put on suction afterwards. Daily chest X-ray was performed until tube removal.
Data collection and statistical analysis
Data collection was done in a retrospective way, based on the electronic patients files. We reviewed the files for important medical history, smoking habits, exposure to asbestos, number of diagnostic thoracocenteses or blind pleural biopsies before thoracoscopy and complications. Major complications were defined as needing intervention. Minor complications were defined as only needing supervision or prolonged treatment that was already in place.
The gold standard which we compared the diagnostic yield of thoracoscopy with was defined as follow-up of 6 months or more, or until a specific disease was diagnosed. The medical files of our hospital were consulted, and if follow-up was unavailable in our files, general practitioners were contacted by telephone, mail or email.
Length of stay was defined as the total days of hospitalisation in which the thoracoscopy took place, even if patients were admitted through emergency department.
Initial thoracoscopic diagnoses were divided as follows: malignancy, nonspecific pleuritis, mycobacterial infection, and other benign conditions. Malignant pleuritis was diagnosed when histological exam showed malignant cells in pleural biopsy. Mycobacterial infection was diagnosed when direct exam showed acid fast bacilli or culture showed mycobacteria. Benign asbestos related pleural effusion was diagnosed when pleural plaques were diagnosed without arguments for malignancy and no other diagnosis was withheld. Parapneumonic effusion or bacterial infection was diagnosed when pneumonia was present or pleural fluid or biopsy culture was positive, no other disease was diagnosed and pleural effusion regressed after treatment.
Statistical analysis was done with IBM SPSS Statistics V.23.0.0 for Mac OS. We calculated two sensitivities and specificities, ‘minimal’ and ‘maximal’. ‘Minimal’ we defined as supposing that all patients that had less than 6 months of follow-up got a new diagnosis afterwards, and maximal as if they had not . For minimal sensitivities in different diagnostic categories, we supposed they all got a diagnosis in that category (eg, malignancy, mycobacterial infection or other benign condition).
Results
Patient population
During the inclusion period, 131 patients underwent a diagnostic thoracoscopy. Patient characteristics are summarised in table 1. Mean age was 65.6+−14.1 years, 58.8% were male. 60.2% were smokers (71 out of 118 patients, not recorded in 13 patients). All patients had a blood analysis, ECG, chest X-ray. Mean number of diagnostic thoracocentesis was 1.5±0.8 per patient, and 9 patients underwent blind pleural biopsy before thoracoscopy. Ultrasound was done when in doubt if safe thoracocentesis could be performed. Chest CT was frequently done, on discretion of the attending physician.
Patient population properties
Significant medical history of the patient population is presented in table 2. In 51 patients (38.9%) malignancy was noted in the medical history, 6 patients (4.6%) had been treated for tuberculosis. None had known autoimmune or systemic disease.
Medical history of the patient population: malignancy, mycobacterial infection and autoimmune disease
Pleural biopsy results
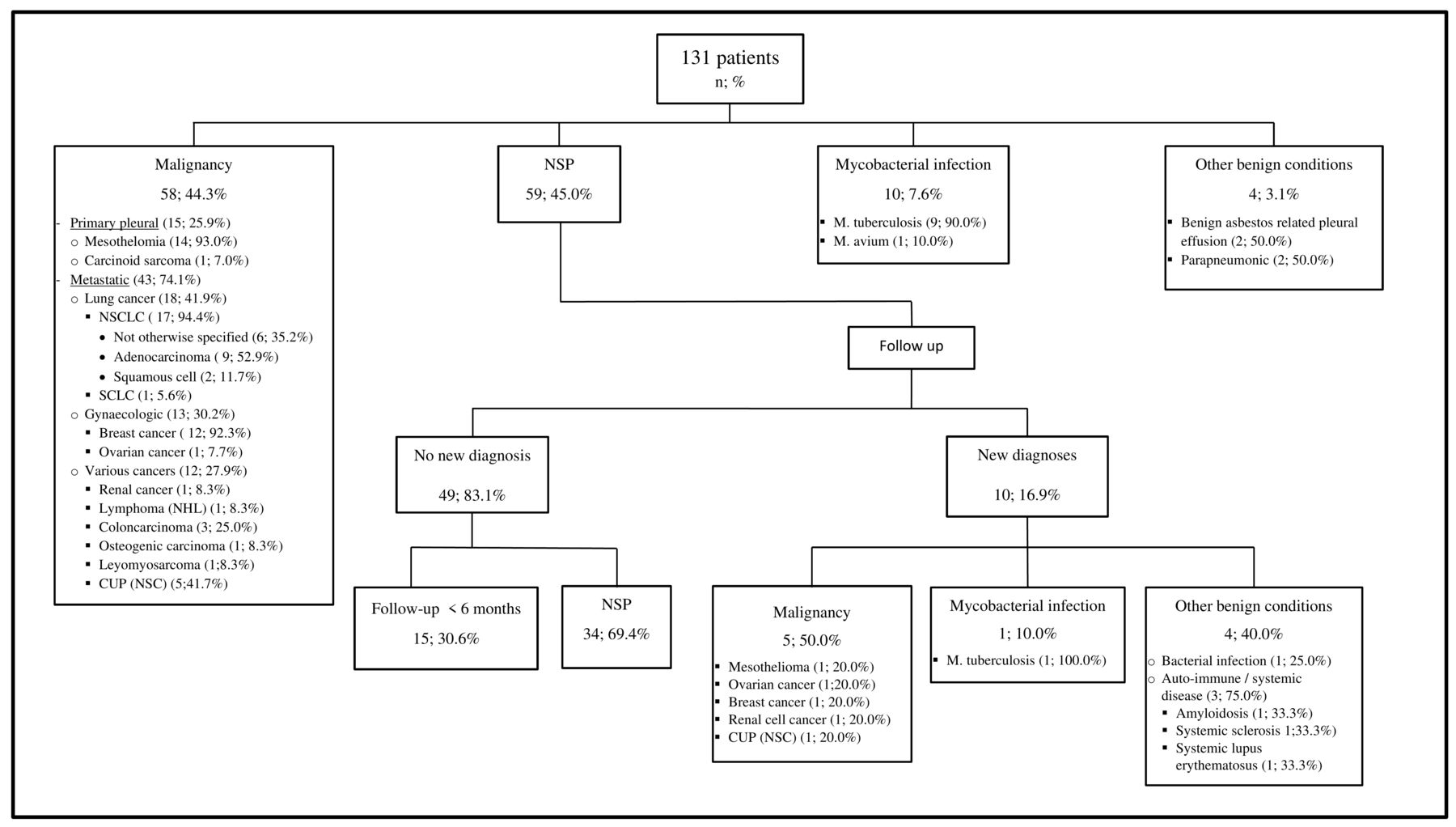
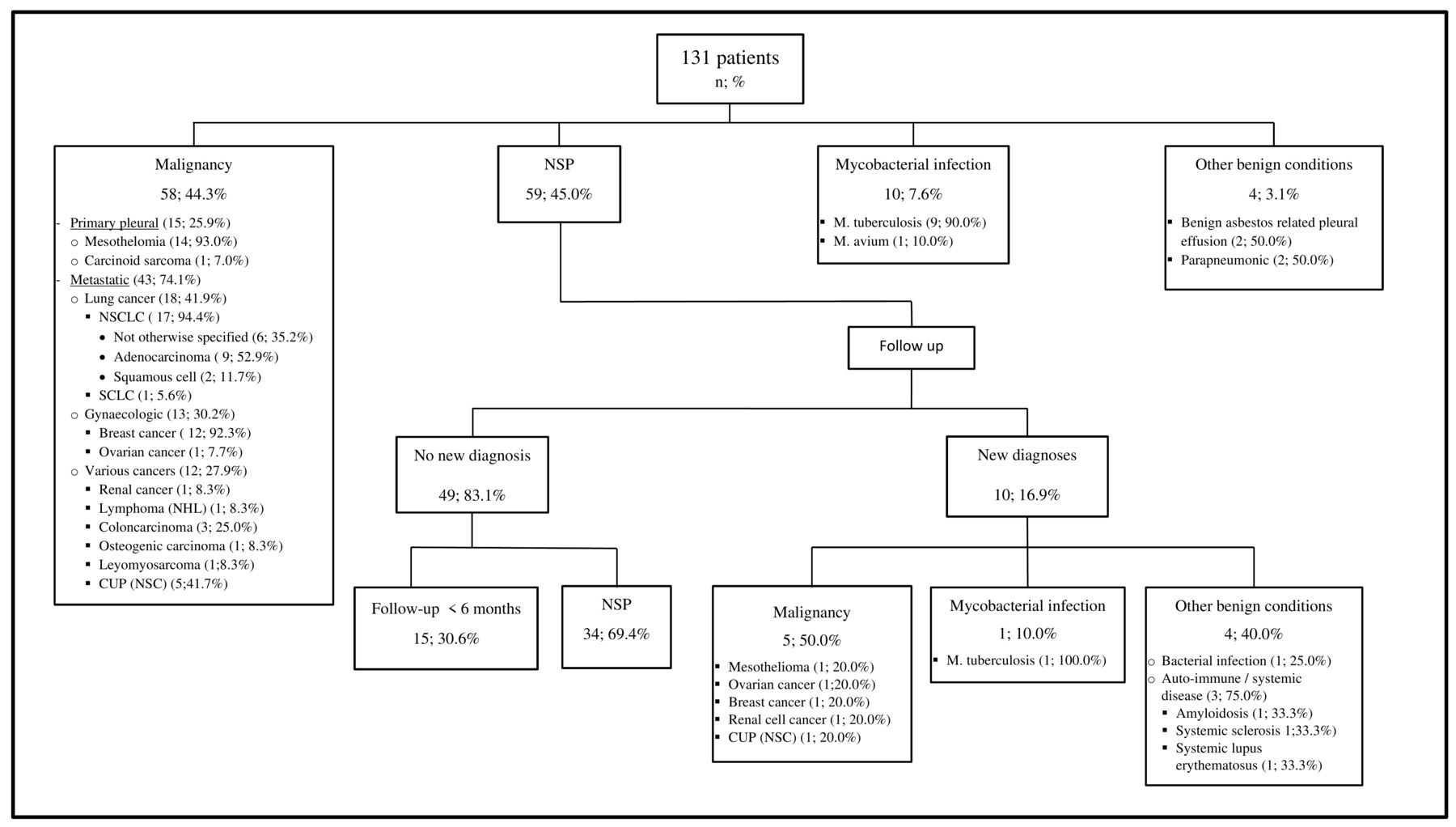
The detailed results of the thoracoscopic pleural biopsies are summarised in figure 1. For reasons of simplicity, figure 1 already contains diagnoses after follow-up as well. In 58 patients (44.3%) pleural biopsy showed malignancy. Primary pleural malignancy accounted for 25.9% of these malignancies, and 74.1% metastatic cancers. Main primary tumours were lung cancer (41.9%) and gynaecological tumours (30.2)%. The remaining 27.9% of metastatic pleural effusions are caused by various tumours. In 59 patients (45.0%) nonspecific pleuritis was diagnosed. Mycobacterial infection was diagnosed in 10 patients (7.6%) and other benign conditions were diagnosed in four cases (3.1%). These four cases existed out of benign asbestos-related pleural effusion,2 and parapneumonic effusion.2
{kind=link}
Diagnoses of thoracoscopic pleural biopsies, and after follow-up. Percentages are relative to the category above. NSCLC, non-small-cell lung cancer; SCLC, small-cell lung cancer; NHL, Non-Hodgkin Lymphoma; CUP, cancer of unknown primary; NSC, non-small-cell; NSP, nonspecific pleuritis.
Diagnoses after follow-up of 6 months or more
In the 59 patients with nonspecific pleuritis, follow-up showed a new diagnosis in 10 of them (16.9%). Of these new diagnoses five effusions were malignant in origin (50.0% of new diagnoses, 8.5% of 59 patients with initial diagnosis of nonspecific pleuritis). Mesothelioma was diagnosed by repeat thoracoscopy, metastatic ovarian and renal cell cancer by repeat thoracocentesis fluid cytology, cancer of unknown primary by CT-guided pleural biopsy, and metastatic breast carcinoma on autopsy. One new diagnosis was due to infection with m. tuberculosis (thus 10.0% of the new diagnoses, 1.7% of patients with initial diagnosis of nonspecific pleuritis) and four effusions were due to other benign disease (40.0% of the new diagnoses, 6.8% of patients with initial diagnosis of nonspecific pleuritis). These diagnoses existed of one due to bacterial infection, three due to autoimmune or systemic disease. In the remaining 49 patients without a new diagnosis, follow-up was less then 6 months in 15 patients. In one of these patients, the effusion regressed, in five it persisted. In the other nine patients, no information was available. In the other 34 cases with follow-up of more than 6 months (mean 46±32 months), the effusion regressed in 22 patients, in 8 it persisted, in 4 patients no information was available.
Statistical analysis
Sensitivities and specificities
General and specific sensitivities and specificities, negative and positive predictive values are shown in table 3.
General and specific sensitivities, positive and negative predictive values
General sensitivity for any diagnosis was minimally 80.9%, and 92.4%, maximally. Specificity was 100.0% for all diagnoses. Sensitivity for diagnosing malignancy was between 74.4%, and 92.1%, for mycobacterial infection between 38.5% and 90.9%, 0% for autoimmune or systemic disease, and between 17.4% and 50.0% for other benign conditions. Positive predictive value was 100.0%, negative predictive value range was 57.6%–83.1%.
Safety
Median length of hospital stay was 4 days (IQR 3–14 days). Complication data are presented in table 4. Major complications were seen in six patients (4.6%), existing of trapped lung and (wound or pleural) infection and need for decortication (two), empyema with acute kidney injury and single need of dialysis (one), hospital-acquired pneumonia which needed transfer to ICU (one), deep venous thrombosis of the right arm (one) and repeat pneumothorax (one). Minor complications were seen in two patients (1.5%), existing out of important subcutaneous emphysema (one) and transient haemoptysis (one).
Safety data
Mortality perioperatively was 0.0%, postoperative five patients died (or 3.8%). Mean age of deceased patients was 78 years old, with a mean stay of 19 days before thoracoscopy (general bad condition needing hospitalisation). Deaths were at postoperative day 2, 3, 5, 19 and 23. Causes of death were aspiration or hospital-acquired pneumonia and respiratory insufficiency not otherwise specified.
Discussion
Pleural effusion of unknown origin remains a frequent problem, with important implications. Thoracoscopy is frequently necessary, as well for diagnostic or therapeutic reasons.
These data represent our experience of medical thoracoscopy in a period of almost 10 years, the first Belgian data to be published to my knowledge. The amount of patients is comparable to other studies.6–8
Out of 49 patients with nonspecific pleuritis 15 had less than 6 months of follow-up, and thus, we calculated a maximal and minimal sensitivity, as was done before in another study.9 Due to the little number of some diagnoses these parameters sometimes have a wide range, which makes it impractical for daily use. However, we think the sensitivity will be closer to the highest percentage, since we do not expect all patients with incomplete follow-up to have gotten a rare or missed diagnosis.
Thoracoscopy was performed under general anaesthesia, so in this discussion we tried as much as possible to compare to other studies in which thoracoscopy was performed under general anaesthesia.
Sensitivity analysis
General sensitivity
General sensitivity in our data was between 80.9% and 92.4%. This is comparable to the sensitivity of 93% in the recent meta-analysis of Wei et al, however, for local anaesthesia thoracoscopy.7 Sensitivities for video assisted thoracoscopy under general anaesthesia are, however, in the same range or a little higher (ranging from 82.3% to 95.2%).8 10–12
Negative predictive value range is 57.6%–83.1% for any diagnosis, which is comparable to 76% of McDonald et al8 but probably a bit lower than 85%–90% in Menzies et al.9 (95% CI 84% to 96% and 78% to 92%, depending on possible diagnoses in patients lost to follow-up).
Specific sensitivities
Sensitivity for malignant pleuritis was high (92.0%), but a little lower than in other studies (94.0%–95.0%).12 13 Sensitivity for mesothelioma in our study was a lot higher than in the meta-analysis of Wei et al (93.3% vs 42.0%), for unclear reasons (eg, percentage of mesothelioma was even less than in Valsecchi et al6, which study was however not included in the meta-analysis of Wei et al). It is however comparable to 90.9% in Ferrer et al.13
The malignancies diagnosed during follow-up were one mesothelioma, two gynaecological cancers, one primary renal cell cancer and one cancer of unknown primary tumour. So, in our study, there seems to be no specific primary cancer type that is missed frequently, in contradiction with the data of several other studies, in which frequently malignant mesothelioma or metastatic pulmonary carcinoma were diagnosed.9 14–16
Sensitivity was 90.9% for tuberculous pleuritis, and not 100% as in another study1 due to one missed case, which was diagnosed with a thoracoscopic lung biopsy. In a Turkish study, even after all patient got a closed pleural biopsy first, also 1 case of tuberculosis was missed on thoracoscopic pleural biopsy.17
Sensitivity for other benign conditions was very low, as has also been described elsewhere.1 9 12 18 19 This concerns most frequently patients with benign asbestos-related pleural effusion, and autoimmune disease such as systemic lupus erythematosus and rheumatoid arthritis. This is probably due to aspecific histological findings in these diseases, due to not well understood pathophysiology.20 Some diagnostic clues of these rare diseases are described by Boutin et al and by Anevlavis et al.18 20
Diagnoses made on pleural biopsy
The 44.3% of patients with malignant pleuritis is in the range of other studies (60.0%, 54.0%, 44.2%, 36.6%).8 9 12 17 Of course this also depends on previous diagnostic work up before thoracoscopy (eg, imaging, number of thoracentesis, closed pleural biopsy), but also on your patient population, and if the data were collected in TB-endemic countries.21 We have a higher percentage of nonspecific pleuritis compared with these other studies, and lower percentage of other benign conditions. We however have no empyema, haemothorax nor heart failure, which is prevalent in some other studies.9 12 Neither do we have (clinical) probable diagnoses, but only certain diagnoses, and we categorised all these uncertain diagnoses as nonspecific pleuritis.
Follow-up of non-specific pleuritis
In our study, in 59 patients with nonspecific pleuritis 5 (8.5%) were diagnosed with malignant pleuritis afterwards. This is practically the same as in a previous study of our department with a mean follow-up of 32.9 months, which showed 5 patients (8.3%) of malignancies diagnosed afterwards,16 2 of them being mesothelioma.
This is also comparable to two other studies, in which both 5% of malignancy was diagnosed during follow-up,14 15 however, in other studies up to 25% of malignancy was found,22 23 in the latter after a mean period of 6 months. In another study in a tertiary referral hospital with high incidence of mesothelioma 12% showed to have malignant pleural effusion, all of them mesothelioma related, and mean follow-up until diagnosis was 9.8 (±4.6) months.24 In another study in which 86 patients were followed up for approximately 5 years, 3.5% patients showed to have malignancy within the first year of follow-up, all of them mesothelioma.25 Janssen et al found 14.9% malignant pleuritis, diagnosed after a mean follow-up of 8.7 months, almost 1 in three being mesothelioma.
The high percentage of mesothelioma is again contradictory to our data, in which we found multiple types of metastatic cancers, and no majority of mesothelioma.
We chose a 6-month period of follow-up, which, comparing to other studies, might have been short and it is possible we missed some malignancies. This decision was made because of the retrospective nature of our study, and for a longer period of follow-up ranges of sensitivities would have been even bigger (more loss to follow-up). However, our percentage of malignancy is almost exactly the same as in Venekamp et al, in which the follow-up was almost 33 months, and certainly comparable to some of the studies mentioned above. Most malignancies are diagnosed within 1 year after thoracoscopy, and rarely later. Number needed to detect one malignancy during the first year after thoracoscopy was calculated as 18, and afterwards 250.15 17 25
In our data persisting pleural effusion was seen in 26.5% (another 9 patients loss to follow-up), and in 22 of 34 patients with follow-up of more than 6 months the effusion regressed, (mean time of 7 months). In two other studies, persistence or reappearance ranged from 12.5% to 16.7%.14 16
Safety
Median length of stay was 4 days, which is 1 day longer than the study of McDonald et al.8 However, in their study, patients admitted more then 2 days before thoracoscopy were excluded from analysis of length of stay, which was not the case in our data set. Since the IQR is from 3 tot 14 days, the rather long median length of stay seems to have been caused by a minority of patients with unusual long length of stay.
Mortality in our study was 3.8%, with a mean age 78 years, and all of these patients were admitted urgently before diagnosis of pleural effusion. According to the standards of the British Thoracic Society and the Society of Cardiothoracic Surgeons in Great Britain and Ireland (BTS/SCTS) mortality should be less than 1.6%. As two of five deceased patients died on postoperative day 19 and 23, one could argue if this due to thoracoscopy, and it seems mortality in our study was not only due to the thoracoscopic procedure, but also due to underlying disease and general weak condition.10 In Harris et al, mortality was 6% during hospitalisation.12
Major complication rate in our study was 4.6%, which is higher than the standards of BTS/SCTS (<2%).10 However, in other studies, major complication rates ranged from 1.9% to 15.0%.5 8 12 26 Definition of major and minor complications is not always clearly stated and can be different between studies. Also, it is not always noted if (and which proportion of) patients are hospitalised electively or urgently because of symptoms. The latter could indicate a worse general condition. These two reasons make it difficult to compare complication rates.
Minor complication rate was 1.5%, which is a lot less than reported in the studies of Colt and Harris et al (5.7% and 8.0%, respectively).5 12
Strengths and limitations
Our data collection was performed retrospectively from a single tertiary centre. Given the retrospective nature, we relied on data in the patients’ files, with the inherent limitations. Follow-up was 6 months, after which we possibly missed some diagnoses. We also have some patients lost to follow-up, generating statistical uncertainty. The number of patients included is not very big, but certainly comparable to other studies. We have no probable diagnoses, only certain diagnoses, which makes our data more robust than some other studies.
Generalisability
This is a single-centre study, performed by an experienced respiratory physician during a period of almost 10 years. Although this certainly limits generalisability, given the data are comparable to studies in multiple other countries, we think these results should be rather generalisable in the same setting and region.
Conclusion
Pleural effusion without diagnosis after initial evaluation is a frequent problem in a respiratory division, for which thoracoscopic pleural biopsy is regularly necessary. Our data, which are the first Belgian data published, represent our experience with medical thoracoscopy. These data are comparable to other studies, as well in diagnostic yield, in diagnoses made, and safety data. Medical thoracoscopy has a high diagnostic yield, and is generally safe, certainly compared with the diagnostic and therapeutic importance. If malignant pleuritis is diagnosed after a diagnosis of nonspecific pleuritis, usually it is within 1 year, rarely within 2 years. Follow-up after diagnosis of nonspecific pleuritis should preferably be 2 years.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethics Committee UZ Brussel Reference ID: 2015/385.
Acknowledgments
We would like to thank Prof. Dr. Vincken W, head of the Respiratory Division of UZ Brussel at the time of the study, for supervising this study.
References
Footnotes
Contributors TDK performed all the thoracoscopic procedures, and kept the patients’ identification data in a database. He provided and cared for study patients. EPD assisted TDK for part of the thoracoscopic procedures, and afterwards collected all the data, when necessary contacted the general practitioners, did the statistical analyses and wrote the article. He also cared for the study patients. EPD is the corresponding and submitting author, and guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.