Article Text

Abstract
Background Non-invasive ventilation (NIV) is effective in a variety of acute respiratory illnesses in hospitalised patients. Home NIV is effective for stable patients with hypercapnia due to neuromuscular or chronic pulmonary disease. However, there are little data to guide which patients may benefit from NIV immediately following hospitalisation with hypercapnia.
Objective To evaluate outcomes of patients with daytime hypercapnia at the end of an acute hospital admission.
Design Retrospective cohort study.
Participants Entry into the cohort was by querying the hospital electronic medical system for consultations regarding NIV after discharge. Cases received NIV and controls did not. We extracted data on demographics, ICD-9 diagnoses and medications coded at admission, blood gas measurements and dates of discharge, first readmission and death.
Intervention None.
Main measurement Time from hospital discharge to mortality or readmission.
Key results We identified 585 cases and 53 controls who survived to discharge at the index admission. Cases and controls were broadly similar in age and Charlson Comorbidity Index. In the whole cohort, cases treated with home NIV were at increased risk of death compared with controls (HR 1.88 95% CI 1.17 to 3.03). In multivariate Cox regression for all-cause mortality, poor prognostic factors were increasing age (HR 1.03 per year, 95% CI 1.02 to 1.04), cardiac failure (HR 1.31, 95% CI 1.01 to 1.67) and failure to attend NIV follow-up (HR 2.33, 95% CI 1.33 to 4.10). In contrast, chronic respiratory disease was associated with improved prognosis (HR 0.77, 95% CI 0.61 to 0.97) as was sleep apnoea (HR 0.44, 95% CI 0.23 to 0.83). Cases did not have different time-to-readmission compared with controls (HR 1.42 95% CI 0.99 to 2.02).
Conclusion Transitioning to home NIV after a hypercapnic hospitalisation may be useful in younger, co-operative patients with chronic respiratory disease. For older patients or those with cardiac failure, home NIV may not be beneficial and may potentially be harmful.
- Non invasive ventilation
Data availability statement
Data are available on reasonable request. Reasonable requests for data to corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Non-invasive ventilation (NIV) is effective at preventing intubation in selected acutely hypercapnic patients and preventing hospitalisation in chronically hypercapnic chronic obstructive pulmonary disease patients.
WHAT THIS STUDY ADDS
In patients discharged after an acute hypercapnic admission to hospital, home NIV was associated with overall increased mortality, driven mostly by older patients with heart failure treated with home NIV. Patients with respiratory disease who attended follow-up had decreased mortality.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Controlled clinical trials are needed urgently to assess the risk-benefit of home NIV after an acute hypercapnic admission.
Introduction
Non-invasive ventilation (NIV) is a means of assisting a patient’s breathing by applying different levels of positive pressure to the airway without insertion of an endotracheal or laryngeal airway. NIV is effective in multiple acute medical emergencies including exacerbations of chronic obstructive pulmonary disease (COPD), pulmonary oedema, pneumonia in immunosuppressed patients and in the peri-intubation/periextubation period.1–3 Acute hypercapnia is an obvious marker of increased in-hospital mortality, but even in those surviving the acute admission, there is a high risk of readmission or mortality in the year following the index event.4 In the chronic context, home NIV is accepted therapy in patients with hypoventilation due to neuromuscular weakness and obesity hypoventilation syndrome.5 Home/domiciliary NIV is also effective in reducing mortality and readmission to hospital in hypercapnic patients with COPD.6–9 In other contexts, notably heart failure patients with or without central sleep apnoea, home NIV has either no effect on or even increases mortality.10 11
Given the increasing application of NIV both in acute and chronic settings, remarkably little is known about the clinical utility of transitioning of patients with hypercapnic respiratory failure to the community after admission—whether or not NIV should be prescribed from discharge. A recent cohort study suggested that older patients with more comorbidity were at risk of death, although the study did not evaluate the impact of home NIV on prognosis.12 The recent ERS guidelines specifically note an absence of evidence in this regard.3
The aim of this study was to observe the outcomes in a cohort of hypercapnic patients transitioned from hospital to home with NIV. We hypothesised that hypercapnic patients transitioning to home NIV would have reduced re-admission and improved survival compared with similar patients who did not receive NIV.
Materials & Methods
Setting and clinical context
Shamir Medical Center is a large district university hospital in central Israel with 850 beds. In our centre, decisions regarding commencing NIV acutely are taken by internal medicine specialists and intensivists. During discharge planning, patients with hypercapnia are referred to a pulmonologist who reviews the requirement for continued NIV. If the patient is deemed suitable based on clinical judgement, the pulmonologist recommends NIV therapy and prescribes the mask and ventilator setup to the patient’s healthcare fund physician. The device dispensed to the patient is typically chosen by the healthcare fund. Postdischarge follow-up is arranged either in the NIV clinic of the pulmonary institute or in other cases patients are followed up in the community by their health fund (eg, patients discharged to long-term care facilities).
Data extraction
We queried the hospital electronic medical record (EMR) system for all consults addressed to the pulmonary institute with keywords relevant to NIV between 2012 and 2017, with follow-up until November 2019. In relevant cases, we extracted dates of discharge, first readmission for any reason, death or censoring. Of note, the EMR synchronises daily with the national population registry so mortality data is always up to date. From the index admission, we extracted data on demographics, blood gas measurements, diagnoses and medications. We also recorded attendance at the NIV clinic. Patients who were admitted with pre-existing NIV were excluded. Data on compliance with NIV on a per-patient basis were not available.
Calculations and statistical analysis
A single physician reviewed each consult and categorised the outcome: irrelevant/excluded (eg, requests to assist in titration of acute NIV or pre-admission home NIV), death during index admission, NIV recommended after discharge (cases) and NIV not recommended (controls). In all cases, we calculated the Charlson score from the ICD-9 codes (International Classification of Diseases, 9th edition) coded by the admitting physician, including the total score and also binary presence of chronic pulmonary disease, cardiacfailure and dementia as defined in the Charlson score.13 Sedative medication use was defined as chronic treatment with narcotics or benzodiazepines at hospital admission.
Summary data were prepared and tabulated according to allocation to NIV decision. Differences between groups at baseline were compared with χ2/Fisher’s exact test or Wilcoxon test as appropriate. In patients who survived to discharge, a post-discharge survival analysis was performed with the date of index admission at the left-censoring date. The right-censoring dates were date-of-first-readmission and date-of-death or date-of-censoring. The primary analysis was by Kaplan-Meier plot and Cox regression with case/control status as the independent variable. Secondary endpoints were univariate Cox regression with the following independent variables: age, pCO2, bicarbonate, Charlson score, organ-specific comorbidity, obesity or known obstructive sleep apnoea and sedative medications. In order to analyse the effect of attendance at the NIV clinic on outcomes, and due to the presence of collinearity (ie, that controls would not have been invited to clinic since they did not receive NIV), we derived a composite endpoint ‘supervision’ where cases who attended clinic were deemed ‘supervised’ and those not attending ‘unsupervised’. A multivariate regression was performed with all significant factors from the univariate analysis. Finally several exploratory post hoc analyses were performed to examine specific questions arising during the analysis, as detailed below in the results. The R-statistical program (V.3.4.4) was used for all analyses, with the survival and icd packages for processing Cox regression and Charlson scores, respectively.14–16
Sample size was not calculated a priori and was based on the data available in the EMR.
Patient and public involvement
There was no specific patient and public involvement in planning or execution of the study.
Results
We screened 982 consultation files from the initial data query from the EMR. After excluding irrelevant consultations, full data on 703 potential cases were extracted (table 1). Sixty-five of these patients died during the index admission and were excluded. In the 638 patients who were discharged, 585 were defined as cases and 53 controls. In general, the patients were elderly (median age 78 years old) with fairly typical Charlson scores for general medical patients. There were no statistically significant differences between cases and controls in age (p=0.19), Charlson score (p=0.42), presence of cardiac failure (p=0.39) or pulmonary disease (p=0.66) but there were slightly more males in the controls group than cases (p<0.01) A high incidence of either cardiac failure (CHF—24%) or respiratory disease (60%) was noted, whereas dementia was infrequently coded and was therefore excluded from further analysis. Most patients who were referred for possible home NIV had chronic respiratory acidosis during their admission, with patients being prescribed home NIV having higher pCO2 (64 mm Hg cases, 59 mm Hg controls, p=0.005) but only slightly higher bicarbonate levels (p=0.04) than those who did not receive NIV. Prior to discharge, patients receiving NIV had slightly higher serum bicarbonate levels (32 mmol/L vs 30 mmol/L, p<0.002). Cases were typically prescribed NIV with a full face mask, with ventilation given in the spontaneous-timed mode with backup rate of 8–10 breaths per minute. Pressures were set after titration during the acute admission, typically in the range of 12–16 cmH2O inspiratory, and 4-6cmH2O expiratory. Oxygen was prescribed as needed to maintain SpO2 around 90%–95%.
Baseline characteristics of the cohort
Survival analysis
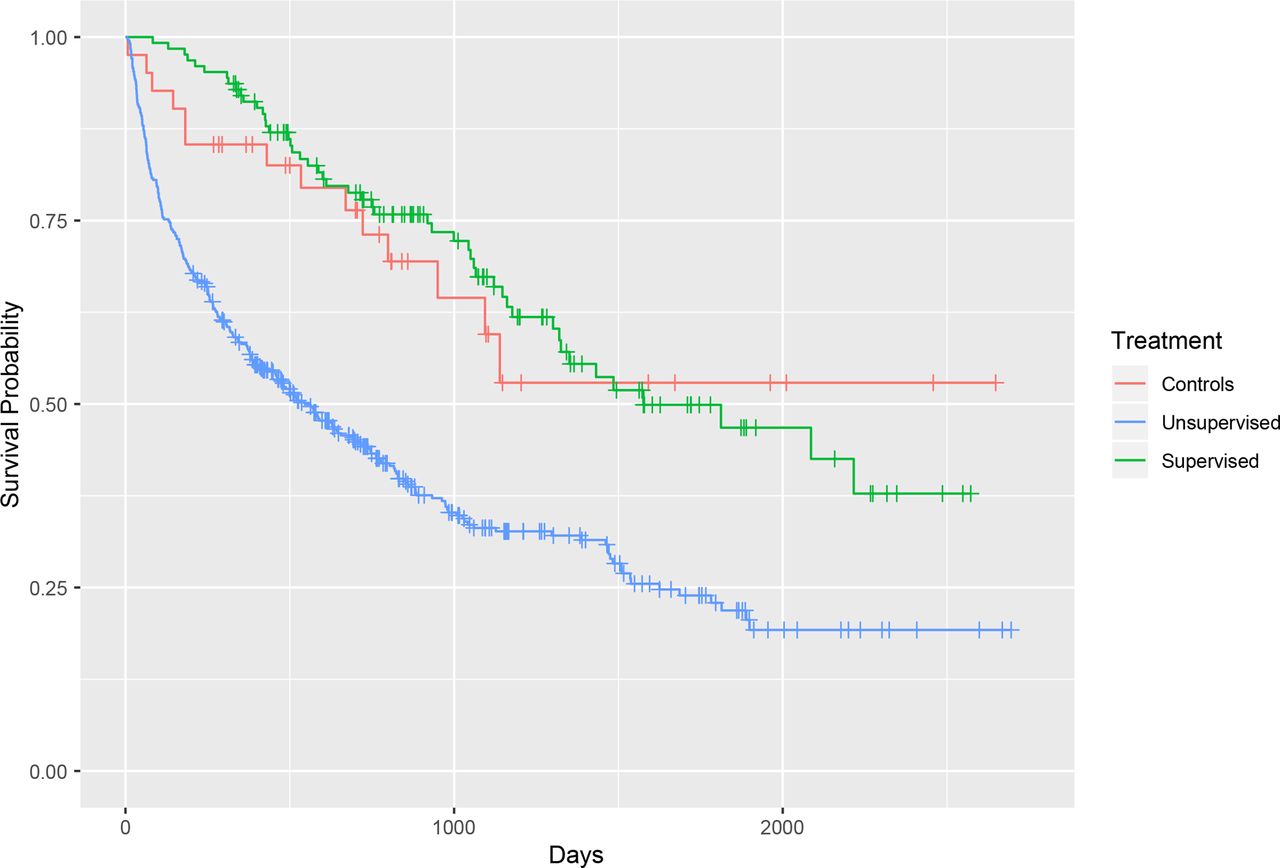
In the cohort, median survival was 824 days (95% CI 698 to 982 days) and 359 patients died (56%). Cases survived median 763 days (95% CI 639 to 933), whereas controls 1850 days (95% CI 950 to 2693). Discharge with home NIV was associated with an increased risk of mortality compared with controls (HR 1.88, 95% CI 1.17 to 3.03) (figure 1, table 2). After considering only patients discharged on NIV who did not attend NIV clinic (ie, unsupervised), the risk of death was higher (HR 2.54, 95% CI 1.48 to 4.33) whereas those who did attend NIV clinic (ie, supervised) did not have increased risk of death (HR 0.96, 95% CI 0.52 to 1.74) (figure 2). Other risk factors for increased mortality in univariate analysis were increasing age, presence of cardiac failure and use of any sedative medication (table 2). Of note, presence of chronic pulmonary disease was associated with lower risk of death (HR 0.70, 95% CI 0.57 to 0.87), as was obstructive sleep apnoea (HR 0.41, 95% CI 0.23 to 0.73).

Kaplan-Meier curve of overall survival, with stratification by NIV status (cases vs controls). Overall, prescription of NIV was associated with worse prognosis (univariate HR 1.88, 95% CI 1.17 to 3.03). NIV, non-invasive ventilation.
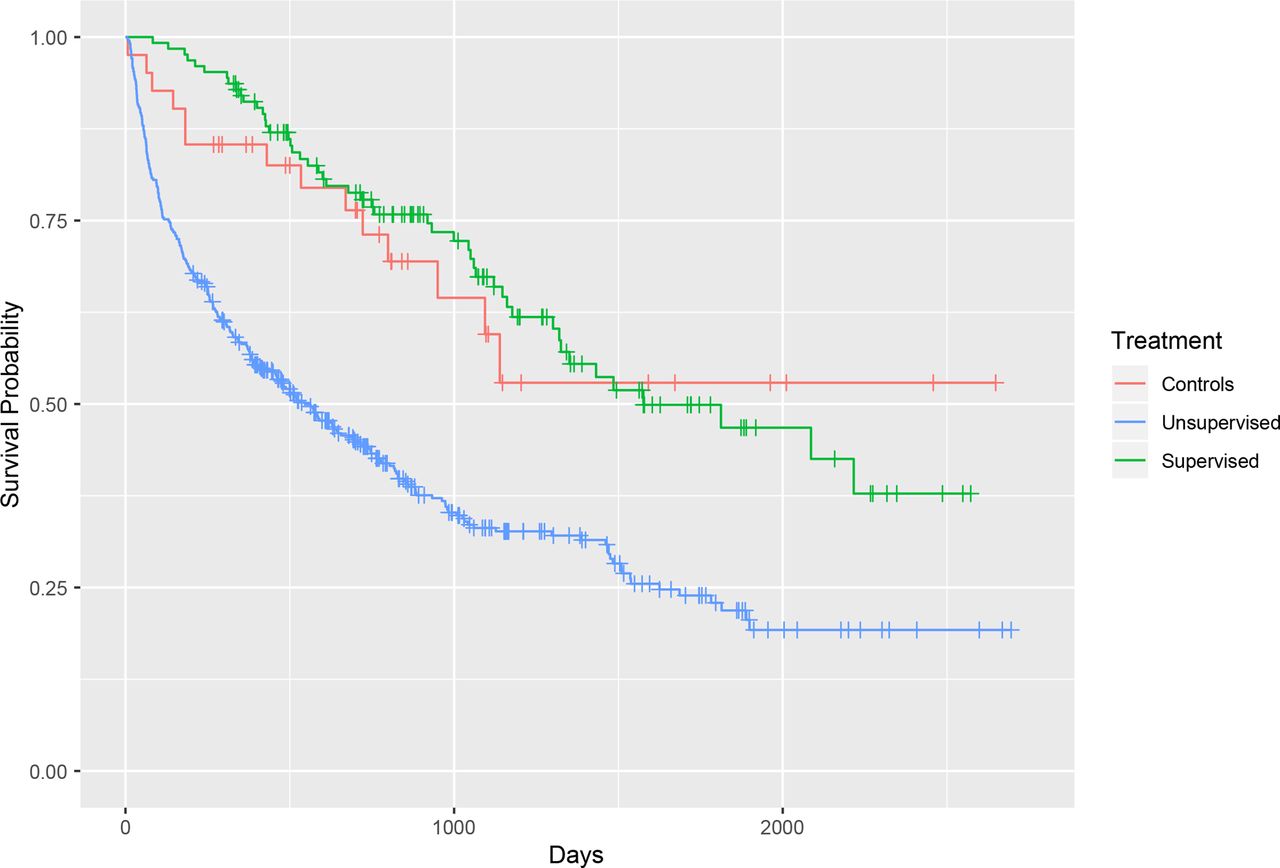
Kaplan-Meier curve of overall survival, stratified by NIV supervision status (controls, supervised cases, unsupervised cases). Unsupervised patients had a poor prognosis compared with controls and supervised cases (univariate HR 2.54, 95% CI 1.48 to 4.33). NIV, non-invasive ventilation.
Overall survival (univariate Cox regression)
In multivariate analysis, a similar pattern of risk factors for mortality was seen (table 3). Although sedative drug use was not a significant factor in multivariate analysis, there was still increased risk of mortality in the unsupervised NIV group, older patients and patients with cardiac failure. Patients with chronic pulmonary disease and obstructive sleep apnoea had a better prognosis.
Overall survival (multivariate Cox regression)
In an unplanned post hoc test, we examined the potential interaction between use of NIV and either cardiac failure, chronic pulmonary disease or obstructive sleep apnoea. In all three cases, we could not determine any interaction between the chronic disease and use of NIV (supervised or not) on survival.
In a second post hoc analysis, we looked at differences in baseline values between the supervised and unsupervised patients. We found that patients in the unsupervised group were significantly older than those who were supervised (77 vs 71 years, respectively, p<0.01) but were otherwise matched on Charlson score and presence of CHF. The supervised NIV group had a higher incidence chronic pulmonary disease (69% supervised vs 51% unsupervised, p=0.02).
Readmission
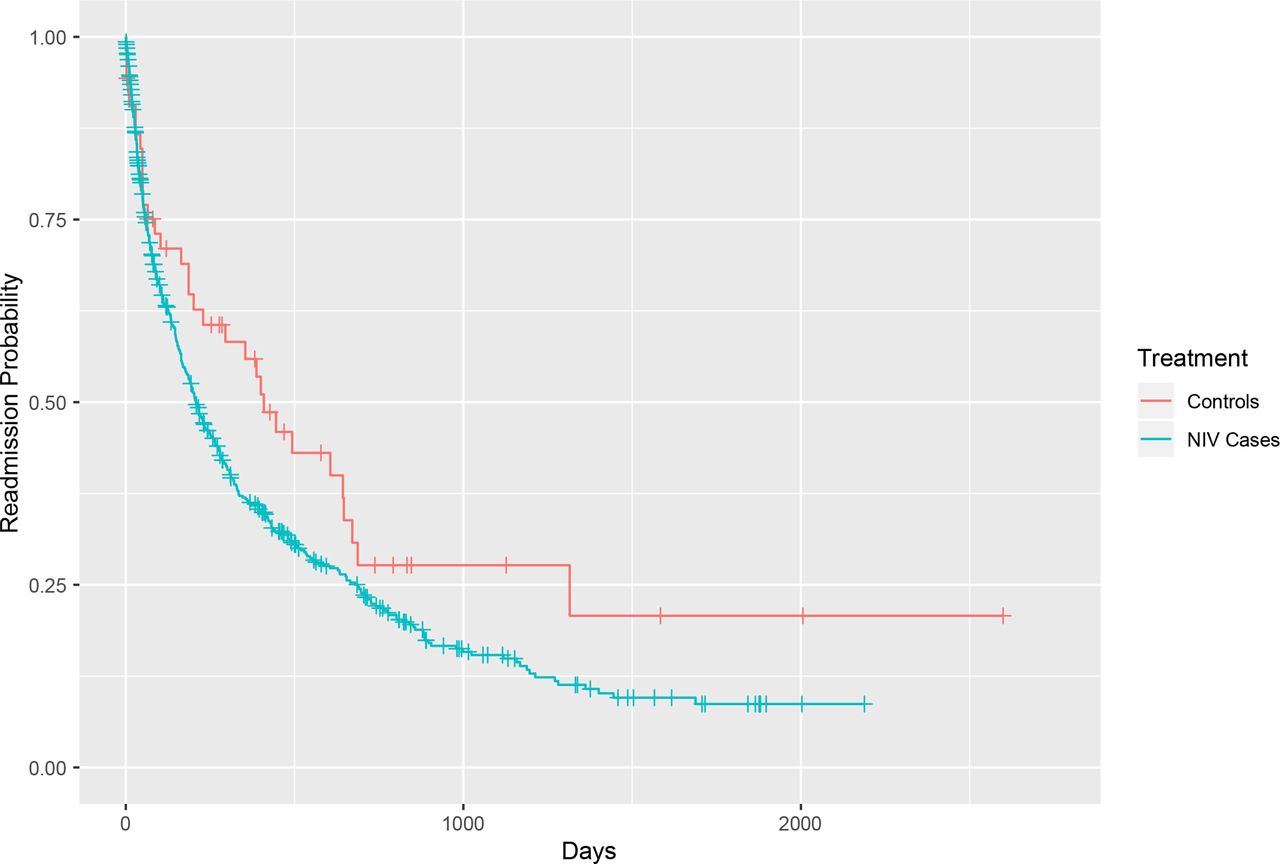
We repeated the above analysis, using time-to-first readmission as the endpoint. During the follow-up, 440 (69%), patients in the cohort experienced at least one readmission, median time to readmission was 870 days (95% CI 744 to 1043). In cases median time to readmission was 854 days (95% CI 732 to 1023) whereas in controls 1837 days (95% CI 796 to 2490). In contrast to overall survival, admission-free survival was not different between the groups who did or did not receive home NIV although there was a trend towards increased risk for readmission in the NIV treated group (HR 1.42 95% CI 0.99 to 2.02) (table 4, figure 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curve of admission-free survival, with stratification by NIV status (cases vs controls). Overall, prescription of NIV was not significantly associated with risk of readmission (HR 1.42, 95% CI 0.99, 2.02). NIV, non-invasive ventilation.
Admission free-survival (univariate)
Risk factors in the univariate analysis for readmission were increasing age (HR 1.01 per year, 95% CI 1.01 to 1.02) and cardiac failure (HR 1.31, 95% CI 1.06 to 1.63). There was no significant impact of supervised NIV therapy as opposed to unsupervised therapy for preventing re-admissions, nor was there any interaction between NIV (whether supervised or not) and either pulmonary disease or cardiac failure (results omitted for clarity).
Discussion
We performed a large retrospective cohort study to evaluate the impact of transitioning patients to home NIV after an acute admission with hypercapnia. The main finding was increased risk of death in the population treated with home NIV compared with those who did not receive NIV. Other risk factors for death were older age, and cardiac failure and ‘unsupervised’ NIV use after discharge. In addition, home NIV did not affect risk for re-admission to hospital overall, although there seems to have been a beneficial effect on patients who either had chronic pulmonary disease or those who attended for the follow-up.
These findings are important and thought-provoking since we do not have good data on the outcomes of transitioning general medical patients to NIV after acute admission. This study is large in size, with 585 cases and 53 controls followed up over several years. The majority of the patients received NIV, which reflected the clinical judgement of the pulmonologists during the period that data were available. It appears from the data that younger patients with chronic lung disease/obstructive sleep apnoea who are able and willing to participate in active follow-up may be good candidates for transitioning to home NIV after a hypercapnic hospital admission. In view of the data presented here, we suggest that elderly patients or those with clinically significant cardiac failure should generally not be candidates for transitioning to home NIV except in special circumstances and if they will be able to attend the follow-up clinics. These matters can clearly only be definitively settled in the framework of randomised clinical trials. Of note, our results are consistent with the SERVE-HF study of CHF patients with central sleep apnoea who had worse prognosis when treated with chronic home Servo-Adaptive ventilation.8 The apparent survival benefit seen for patients with chronic pulmonary disease transitioned to home NIV after an acute hypercapnic hospitalisation is also consistent with current evidence of benefit to patients with COPD, as described in detail in ERS guidelines and two recent meta-analyses.3 6 9 The role of age as an independent factor associated with success or failure of long term home NIV has not been studied as far as we know. The patients in our cohort were older than patients recruited into clinical trials.
The principal limitation in the study is the retrospective design and significant potential for confounding between the different factors. Patient selection was by ‘physician opinion’ rather than by objective criteria. Cases did have slightly higher pCO2 compared with controls, but the differences were not clinically significant (5 mm Hg, table 1) and blood gas values were not predictive of subsequent mortality. Confounding may be present in other factors. For example, we showed that ‘unsupervised’ NIV was associated with increased mortality but we do not know whether this was because of an intervention performed in the clinic which improved prognosis, or because patients attending clinics were more highly motivated, mobile and healthy to attend and presumably were compliant with their therapy. It may be that the ‘unsupervised’ patients were supervised elsewhere or alternatively that their poor prognosis represented non-compliance with the home NIV treatment. We performed several post hoc analyses, which did not reveal significant interactions between the main prognostic factors (use of NIV whether supervised or not with CHF or pulmonary disease). We did show that compliance with follow-up was seen in younger patients and more in those with chronic pulmonary disease. The latter finding could also reflect a selection bias, where patients with pulmonary diseases were invited to follow up in NIV clinic since this reflects the professional interest of the pulmonologist more than a patient with cardiac failure. We also did not have data available for other outcomes such quality of life or sleep in the NIV cases, and these parameters could arguably be as important as survival in a group of mostly elderly patients.17 If hospital readmission can be interpreted loosely as a quality of life indicator, there may also be a trend for poorer outcomes in the cases. As above, clinical trials will be needed to answer these questions. Finally the control group in this study was relatively small in this study compared with the number of cases, which could potentially introduce bias.
Our study findings should be generalisable to other centres, since the study cohort was based on chronically hypercapnic medical patients referred by the internal medicine department for consideration of home NIV. The casemix, demographics and comorbidity scores of these patients, and in Israel as a nation is fairly typical for developed countries. Broadly speaking, the outcomes in terms of mortality and readmission were similar to those reported by Cavalot et al in a Canadian centre.4 We acknowledge that NIV was prescribed widely in our centre for hypercapnic patients in general rather than only for those with chronic pulmonary or neuro-muscular disease or obesity hypoventilation syndrome, which may be at variance with other centres.4 As stated, this represented expert opinion at the time and generation of the data published here was not an a priori intention of treatment policy (ie, this was not a covert interventional study). Therefore, the data presented here represent a frank, if retrospective, assessment of the impact of NIV on a large cohort of hypercapnic patients. We believe that these finding are important and can inform the direction of future clinical trials.
In conclusion, in a large cohort of hospitalised patients who survived an acute hypercapnic hospitalisation, transitioning to home NIV may be effective in reducing mortality in selected patients who are younger and suffer from chronic pulmonary disease or obstructive sleep apnoea and who are co-operative with follow-up. There is evidence of potential harm in older patients or those with cardiac failure who are hypercapnic during their index admission.
Data availability statement
Data are available on reasonable request. Reasonable requests for data to corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Retrospective study was approved by the Shamir Medical Center Research Ethics Committee (ref 0283–18-ASF). The study is reported with reference to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. Due to the retrospective nature of the study, the research ethics committee waived the requirement for informed consent.
Acknowledgments
We thank Natalia Feller from the hospital EMR system for her help in providing the initial dataset.
Footnotes
Contributors All authors made a significant contribution to the research and development of the manuscript, in accordance with ICJME standards. BDF conceived the study, analysed the data and drafted the manuscript. MB extracted data, analyzed the data and edited the manuscript. NN and IS extracted data and edited the manuscript. SP conceived the study, analysed the data and edited the manuscript. The guarantor of the manuscript is BDF, who accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.