Article Text

Abstract
Introduction We have previously developed a supported self-management programme (SMP): Self-management Programme of Activity, Coping and Education for chronic obstructive pulmonary disease (COPD), which was successfully delivered on an individual basis. Payers expressed an interest in delivering the intervention in groups.
Aim To explore the feasibility, acceptability and clinical effectiveness of the intervention delivered and supported by healthcare professionals (HCPs) in groups within primary care.
Methods A prospective, single-blinded randomised controlled trial was conducted, with follow-up at 6 and 9 months. Participants were randomly assigned to control (usual care) or intervention (a six-session, group-based SMP delivered over 5 months). The primary outcome was change in COPD Assessment Test (CAT) at 6 months.
Semistructured focus groups were conducted with intervention participants to understand feasibility and acceptability. A focus group was conducted with HCPs who delivered the intervention to gain insight into any potential facilitators/barriers to implementing the intervention in practice. All qualitative data were analysed thematically.
Results 193 participants were recruited, (median Medical Research Council (MRC) grade 2). There was no significant difference between the intervention and control group for the primary outcome (CAT). However, an improvement in self-reported patient activation (at 6 and 9 months), knowledge (at 6 months), mastery (at 6 and 9 months) and fatigue (at 6 months), in the intervention group compared with usual care was demonstrated.
Qualitative results indicated that the intervention was acceptable to patients who took part in the intervention and HCPs valued the intervention, suggesting it might be best delivered early in the disease process.
Conclusions A supported self-management intervention is feasible and acceptable when delivered as a group-based intervention, by HCPs in the community.
- COPD epidemiology
- Pulmonary Rehabilitation
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Self-management Programme of Activity, Coping and Education (SPACE) for chronic obstructive pulmonary disease (COPD) self-management programme (SMP) has previously been successfully delivered on an individual basis. However, payers have expressed an interest in delivering the intervention in groups, within primary care by healthcare professionals (HCPs).
WHAT THIS STUDY ADDS
We delivered a novel SMP that was acceptable (to participants and HCPs) in a group and community-based format. We did not observe a difference in our primary outcome of health status measured at 6 months. However, we did demonstrate an improvement in several secondary outcomes in the intervention group compared with usual care.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
SPACE for COPD as a group-based community intervention could be offered to patients with COPD, with capacity to manage their disease, to bridge the gap between diagnosis and secondary care interventions.
Introduction
Chronic obstructive pulmonary disease (COPD) is the third-leading cause of death worldwide and is associated with considerable disability, impaired quality of life and high utilisation of healthcare resources.1 Symptoms and manifestations of the disease can be modified by adopting appropriate health behaviours including, but not limited to, exercise, physical activity, smoking cessation, anxiety management, breathing control, medication adherence and exacerbation management.2
National and international guidelines for the management of COPD suggest that self-management support should be provided for people with COPD.2 Interventions to support self-management in patients with COPD have been shown to be effective in improving health related quality of life, reducing hospital admissions and reducing COPD specific health costs.3–5 However, trials have mainly recruited people from secondary care and excluded those with mild disease4 despite those with mild dsypnoea representing 38%–54% of diagnosed patients in primary care.6 7 Lahham et al8 explored the impact of home-based pulmonary rehabilitation (PR) in this population, but found no consistent benefits on exercise capacity, symptoms or quality of life compared with standard care. However, standard care comprised attention control, weekly social telephone calls and the provision of the ‘better living with COPD’ book which may go some way to explain similar improvements in both groups, with authors suggesting PR is not well matched to the needs of a milder group.8 A lighter touch self-management strategy may be beneficial. Furthermore, the support from healthcare professionals (HCPs) seems to be key in patients’ maintaining their engagement in self-management activities.9–12
We have previously developed and described SPACE (Self-management Programme of Activity, Coping and Education) for COPD,13–15 which is a structured programme of exercise, education and psychosocial support. The intervention was underpinned by social cognitive theory and motivational interviewing techniques. This was developed by our institution as a collaboration between experts, patients and carers and has been awarded a Crystal Mark for Clarity by the Plain English Campaign. In discussion with payers, there was interest in exploring the delivery of the SPACE for COPD programme as a group-based intervention in the community rather than on a one-to-one basis. The programme has also been used as remote delivery option for PR services throughout the COVID-19 pandemic.16
Objectives were to address the following, using quantitative and qualitative methods:
Examine whether group-based delivery of SPACE for COPD, with sustained support, improves patient outcomes following the intervention compared with a control group.
Explore feasibility, acceptability and efficacy of the intervention to be delivered and supported by HCPs. This will be done by:
Exploring HCP’s experiences of delivering the intervention and identify any barriers to delivery in practice.
Understanding, from the participants’ perspective, the feasibility and acceptability of the SPACE for COPD intervention delivered by HCPs in a group-based community setting.
Methods
Trial design
Prospective, single-blinded, randomised controlled trial. We used a mixed-methods design to determine the effectiveness and acceptability of a self-management support intervention for people with COPD, managed in primary care. A separate health economic evaluation of the intervention will be reported elsewhere. Details of the study protocol have previously been published.17 The trial was sponsored by the University Hospitals of Leicester National Health Service (NHS) Trust (study number 152408).
After publication of the protocol, we amended the procedure to allow us to send out questionnaires or for one of the study team to go a participant’s home to complete the primary outcome measure in order to minimise data loss of the primary outcome. This amendment came into place after recruitment started. Prior to this, all patients had to complete questionnaires within in person visits. In addition, a second Endurance Shuttle Walk Test (ESWT) was carried out at all time points if the patient walked for more than 8 min on the initial prescribed speed from the Incremental Shuttle Walk Test (ISWT)
Participants
Participants were recruited from seven general practices (GPs) and from those who responded to poster advertisements displayed at GP and hospitals within Leicester, Leicestershire and Rutland. Participants were also recruited from the NIHR Biomedical Research Centre—Respiratory at University Hospitals of Leicester NHS Trust:
Participants were eligible for the trial if they had an established diagnosis of COPD as defined by The Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.
Patients were excluded from participating in the trial if they were unable to participate in the exercise component of the SPACE for COPD programme due to neurological, locomotive, psychiatric disability, or other comorbidities where exercise would be a contraindication (eg, unstable angina; unable to read/write English to the level of an 8 years old; unwilling to be randomised; previous participants of PR or have received the SPACE for COPD manual in the previous 12 months.
Baseline assessment: Participants who expressed an interest in the study were telephoned by a researcher and invited to a recruitment assessment. Following informed consent, spirometry was undertaken, demographic details were collected and the participant was asked to complete baseline questionnaires. A SenseWear accelerometer was given to them to wear on their dominant arm for 7 days, and pick up was arranged. Participants were also randomised and shuttle walk tests (SWTs) were carried out if the participant was randomised to the intervention group.
Intervention: SPACE for COPD group-based self-management programme
Participants in the intervention group received a SPACE for COPD manual and attended the SPACE for COPD group-based self-management programme (SMP) usually within 1 month of their baseline appointment. The programme was structured around the SPACE for COPD manual, which combines both generic self-management skills and disease-specific tasks. The programme was facilitated by two trained HCPs (eg, physiotherapist, respiratoryspecialist nurse, occupational therapist, health psychologist) to groups of up to 10 participants and delivered through six 2-hour sessions, over a 5-month period. Earlier sessions were delivered closer together in time, allowing group cohesion to take place, an important factor in optimising group dynamics.18 As much as possible, the same facilitators delivered all sessions for each group. Sessions were held at community venues, at times and locations to suit group participants to increase retention and engagement in the intervention. The content of the intervention and accompanying self-management components were described in the published protocol.17 Participants were provided with a contact number for at least one of the facilitators in case they had additional queries/were unable to attend any sessions. The exercise component of the manual was completed by participants at home. A full description of the rationale, development and efficacy of the work underpinning the SPACE for COPD manual is detailed elsewhere.13 14 Twelve HCPs attended a 1-day training course and were given an HCP delivery manual to guide the content of the sessions.
Usual care
Participants in the control group continued with any usual check-ups/reviews—no additional care was provided or removed from their current access. If participants were referred to PR in the duration of their time in the study, they were not denied access to the programme. No additional advice, information or recommendations were provided to participants in this group.
Outcomes
The primary outcome measure was health status at 6 months postbaseline assessment, measured using the COPD Assessment Test (CAT). Scores range from 0 to 40 with higher scores indicating greater clinical impact.
Secondary outcomes were COPD knowledge (using the Bristol COPD Knowledge Questionnaire, BCKQ), health-related quality of life (using the EuroQol 5 dimension, 3 level tool), disease-specific quality of life (using the Chronic Respiratory Questionnaire: CRQ), anxiety and depression (using the Hospital anxiety and Depression Score; HADS), patient motivation (using the patient activation measure: PAM) and exercise capacity (using the ISWT and ESWT—at baseline this was only performed in the intervention group to avoid the test itself acting as an intervention). Outcome measures and details of study clinical assessments and outcome measures at all appointments have previously been described in the study protocol.17 Participants were classed as completers if they completed the primary outcome measure at 6 months.
Process outcomes included group characteristics, retention (whole study and intervention group specifically) and intervention adherence. Intervention participants were classed as completers if they attended four out of the six self-management group sessions. Intervention fidelity was also measured (online supplemental appendix 1). Intervention facilitators completed checklists at the end of each self-management group session, and one of the trainers observe one session per self-management group, completing their own checklist.
Supplemental material
Any serious adverse events were reported to the sponsor. A serious adverse event was defined as an acute exacerbation of COPD that resulted in a hospital admission.
Qualitative outcomes
Qualitative focus groups were conducted by SC (see acknowledgements) at the end of the SPACE for COPD intervention and aimed to understand participants’ experiences of the group-based SMP. Those participants allocated to the intervention group were invited to take part in qualitative focus groups at the end of the intervention period. Focus groups were conducted with each SMP group, with between 3 and 10 participants (number dependent on each group size).
HCPs delivering the SPACE for COPD SMP were also invited to participate in a meeting to discuss aspects of feasibility and acceptability, such as gaining insight into any potential facilitators/barriers to implementing the intervention in practice (and derive practical recommendations for doing so). Sample questions are provided in the online supplement.
Acceptability findings from both the focus groups and HCP discussion will be reported here. Additional qualitative findings which may additionally contribute to the design and implementation of this programme moving forward may be reported separately.
Sample size
The power calculation was based on the primary outcome at 6 months.19 20 To detect a mean±SD between-group difference of 2.5±5.0 in the change in CAT with 80% power, 64 people per group are required (α=0.05, two tailed). In anticipation of a possible 25% attrition rate, the total sample size was increased to 86 per group (172 in total). Sample size calculations were carried out using software developed by Machin et al https://onlinelibrary.wiley.com/doi/book/10.1002/9781444300710
Randomisation and blinding
Participants were randomised by an unblinded member of the study team using an online randomisation tool (sealed envelope).21 Individuals were randomised (1:1) to the control group or the intervention group. The system randomises patients in random permuted blocks. This allows for the 1:1 ratio, but due to the random permuted blocks of 2, 4 or 6 ensures full randomisation. Participants were immediately informed of their allocated treatment by an un-blinded member of the study team. Data collection at 6 and 9 months was carried out by the blinded member of the study team, except the ESWT, which was carried out by an un-blinded member of the study team as only intervention participants had a prescribed ESWT speed at baseline.
Statistical methods
Analysis was carried out on an intention-to-treat basis. The main analysis compared primary and secondary outcome measures between treatment groups at 6 months postbaseline to assess the effect of the group-based SMP. Data were also analysed at 9 months to assess the longer-term effect. Data were checked for normality of distribution and multivariate outliers.
Missing data were imputed in Stata (V.15; StataCorp) using multiple imputed chained equations.
Full details of statistical tests are given in online supplemental appendix 2.
Qualitative methods
Focus groups were analysed using Thematic Analysis22 supported by NVivo software (V.9). This approach follows six distinct stages: familiarisation with data; generating initial codes; searching for themes; reviewing themes; defining and naming themes and producing the report. Authors CB and PP carried out initial coding and a sample of interviews were coded by another member of the team to ensure consistency and to enhance interpretive authenticity. Throughout the data analysis, the team met to discuss and review emerging themes and search for accounts that provided contesting views of the same phenomena or identified different phenomena. Our patient representatives were invited to comment on our (anonymised) findings throughout the analysis process to ensure any interpretations made stayed close to the direct experience of patients.23 Finally, member-checking occurred as part of a dissemination event for intervention participants—no changes were made to the acceptability results presented here. A note-based analysis using a constant comparative method was used to analyse notes taken during the HCP discussion.24
Patient involvement
The trial steering committee had two PPI members who contributed throughout the duration of the study. They commented on the initial design of the study, the burden of the trial assessment process, participant facing materials, and on the content and material to support the intervention. In addition, they took part in initial intervention testing and were involved in one of the HCP training days—providing input and answering questions where appropriate. Finally, they input to the qualitative analysis (analysing one transcript each and developing initial themes) with some help and training from the research team. At the end of the study, participants in the intervention group commented on the study findings.
Results
Participant flow
Figure 1 shows the Consolidated Standards of Reporting Trials flow diagram of participant enrolment, allocation, follow-up and analysis. Participant characteristics for both groups are displayed in table 1. There were no differences between groups at baseline for characteristics or the outcomes shown in table 2.

Consolidated Standards of Reporting Trials flow diagram of participant enrolment, allocation, follow-up and analysis. COPD, chronic obstructive pulmonary disease; PR, pulmonary rehabilitation; SPACE, Self-management Programme of Activity, Coping and Education.
Baseline characteristics of all participants
Comparison of primary and secondary outcomes
Sample size
During initial stages of the study, 19 patients were deemed to be ineligible. There were two important implications of this: the overall sample size was lower than expected, and the group sizes had become unequal. As a consequence, the sample size was reassessed and additional participants recruited. The allocation ratio of 1:1 was maintained and as such recruitment was extended to 193 patients (of which 174 would be eligible) in order to maintain 80% power. This number (174) allows for a slightly higher level of attrition, as well as an inequality in the numbers allocated to the two groups.
Numbers analysed
Participants were recruited between March 2015 and October 2016. One hundred and ninety-three participants were randomised. At the end of the trial, data were available for the primary outcome in 65% (n=52) of the intervention group and 93% (n=70) of the usual care group. Missing data rates across variables ranged from 5/193 (2.6%; age/gender) to 101/193 (52.3%; ESWT at 9 months). This large volume of missing data for shuttle walking tests occurred when some participants were unable to attend 9-month appointments. In such circumstances questionnaires were sent by post.
Eighteen serious adverse events were reported by participants; 11 in the intervention arm and 7 in the usual care arm. None were considered to be related to the intervention. No deaths occurred.
Outcomes and estimation
Primary outcome
At 6 months, there was no significant difference between groups in the total CAT score (mean difference 1.70, 95% CI −0.53 to 3.94, p=0.135). When the total CAT score at 9 months was added to the model, there was still no significant difference between groups over time (mean difference .511, 95% CI −1.28 to 2.30, p=0.575) (see figure 2).

COPD Assessment Test (CAT) score. COPD, chronic obstructive pulmonary disease.
Secondary outcomes
The mean difference in PAM score was significant at 6 months, in favour of the intervention group (mean difference −5.66, 95% CI −10.03 to −1.29, p=0.011). This difference was maintained at 9 months (mean difference −6.70, 95% CI −10.85 to −2.56, p=0.002) (see figure 3). The mean difference in PAM level was also significant at 6- (mean difference −0.36, 95% CI −0.69 to −0.03, p=0.031) and 9 months (mean difference −0.57, 95% CI −0.90 to −0.23, p=0.001), in favour of the intervention group (see figure 4).

Patient Activation Measure (PAM) score.

Patient Activation Measure (PAM) level.
The mean difference in BCKQ score was significant at 6 months, in favour of the intervention group (mean difference −2.53, 95% CI −4.59 to −0.47, p=0.016), this difference in both groups was sustained at 9 months but was not significantly different between groups (mean difference −1.88, 95% CI −4.16 to .40, p=0.106) (see figure 5).
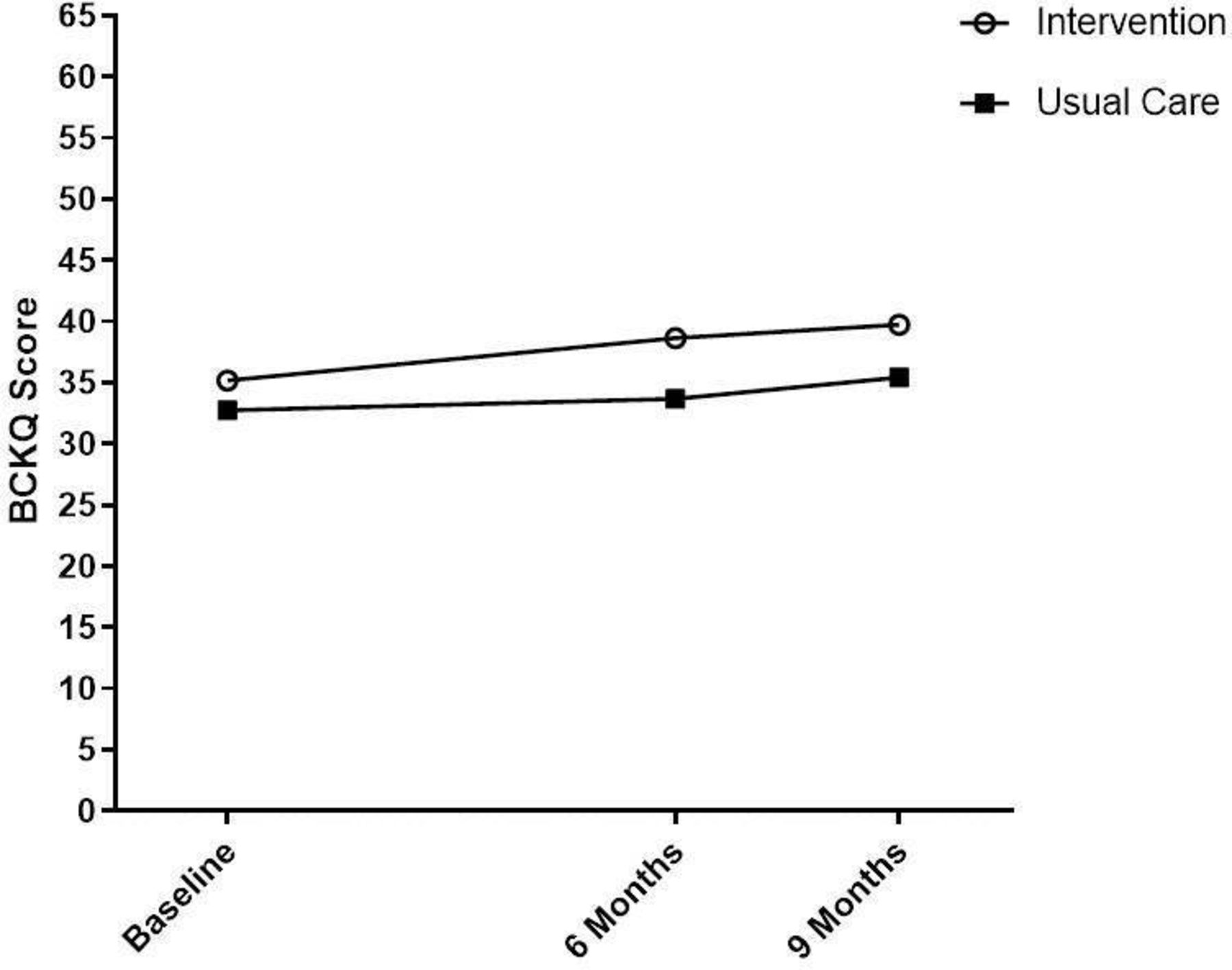
Bristol COPD Knowledge Questionnaire (BCKQ). COPD, chronic obstructive pulmonary disease.
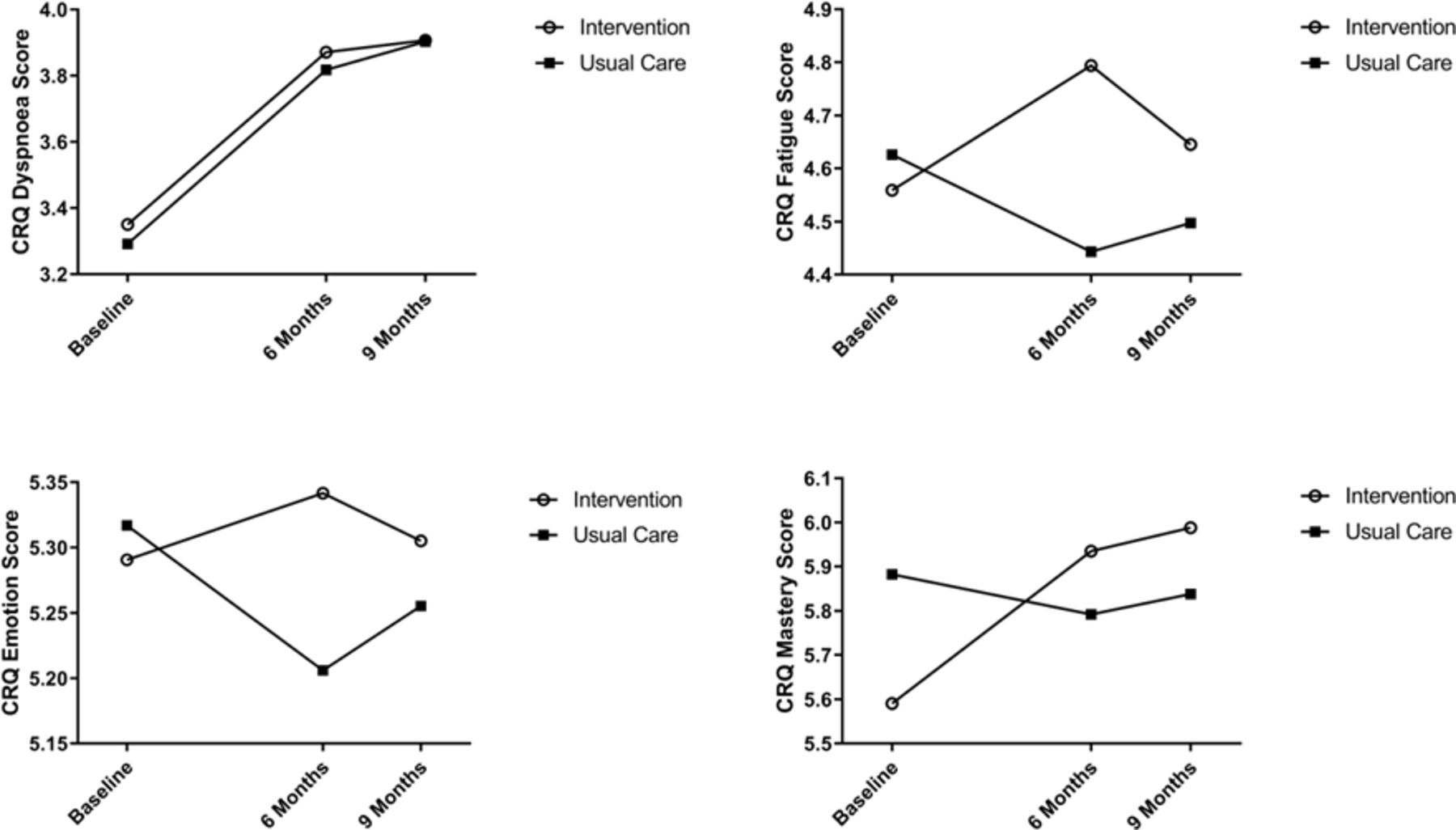
The mean difference in the fatigue (mean difference −0.42, 95% CI −0.81 to −0.03, p=0.035) and mastery (mean difference −0.44, 95% CI −0.78 to −0.09, p=0.015) domains of the CRQ were significant at 6 months, and for the mastery domain this difference was sustained at 9 months (mean difference −0.44, 95% CI −0.78 to −0.10, p=0.011) (see figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chronic respiratory questionnaire (CRQ)—subscales.
There are no significant differences in the CRQ Emotion and Dyspnoea subscales, HADS, ISWT or ESWT at 6 months or 9 months (table 2 and online supplemental appendix 3).
Qualitative results: acceptability of the programme: participants
Data are discussed below; covering delivery practicalities and integration of the SPACE for COPD manual within the SMP (see table 3 for example quotes).
Example quotes from intervention participant focus groups
Were the venues suitable?
Overall, venues and locations were well received. Parking was also important for those driving to venues. For some, venue proximity was more important than venue quality. For others, proximity wasn’t a problem—they could get a lift or share lifts with other group members.
What did they think of the session timings?
Generally, participants were happy with the time of day groups were run, with only a couple saying they would have preferred a different time of day (eg, morning instead of afternoon). Mainly, participants were happy with session length—only one smaller group thought session could be condensed. Finally, everyone was satisfied with length of time between sessions—though one group suggested a month as the longest time between sessions, stating 6 weeks might result in a slight decrease in motivation.
How was the SPACE for COPD manual used?
Everyone thought that the SPACE for COPD manual complemented group activities in sessions. Positive aspects of the manual included: good reference point for the future, informative, encompasses everyone and did not ‘preach’. Aspects most liked were: exercise charts, breathing techniques and overall advice given. Learning points included: expensive resource that some might not look at again in the future, could be condensed, strength training could be clearer.
Discussion with HCPs
Main themes arising from the HCP discussion are outlined in table 4. These cover learning gained from delivering the SPACE for COPD group-based SMP, how this learning has resulted in a general change in their professional practice and thoughts about future programme implementation.
HCP discussion themes
Discussion
We developed and delivered a novel SMP that was acceptable (to participants and HCPs) in a group and community-based format delivered by those HCPs likely to deliver the intervention in practice. The novelty of our approach included group sessions being spread out further across a longer period than traditional SMPs, with earlier sessions being closer together in time to allow group cohesion to take place.
We did not observe a difference in our primary outcome of health status measured by the CAT. Both groups had an improvement of 1.4 and 1.9 points for the intervention and control groups, respectively (a change of 2 is deemed clinically relevant20). It may be that the intervention was not intense enough to make a difference in this outcome. However, we did demonstrate an improvement in self-reported patient activation (at 6 and 9 months), knowledge (at 6 months), mastery (at 6 and 9 months) and fatigue (at 6 months), in the intervention group compared with usual care. PAM scores improved more than the minimum important difference (MID) of 4 points25 at 6 and 9 months, compared with baseline in the intervention group. This would indicate improved activation and increased self-management skills. There were no statistically significant improvements in anxiety and depression, exercise capacity, dyspnoea or emotion at 6 or 9 months. However, clinically relevant improvements were noted for dyspnoea in both groups (more than the minimal important difference of 0.5 at 6 and 9 months26) and for the ESWT at 6 months in the intervention group this was approaching the MID of 174 s.27 Qualitative results demonstrated that the intervention was acceptable to patients who took part in the intervention and that the SPACE for COPD manual was well received. HCPs also valued the intervention, suggesting it might be best delivered earlier on in the disease process.
MRC and CAT scores demonstrated that overall, participants were milder and less symptomatic compared with a typical PR population.28 The median MRC score was 2, and our median baseline CAT score was 14 (IQR 10–20; mean 14.6). As a comparison, a PR audit conducted around the same time as this study29 noted a median CAT score was 22 (IQR 16–28) and 66% of patients were MRC 3 or 4. These numbers are also comparable to participants in the Kon et al study20 determining the MCID for CAT, where the mean CAT score at baseline was 21.4. As our scores are significantly lower, it is possible that we achieved a floor effect in the intervention group whereby change may be unlikely to be achievable. Other studies have also demonstrated similar improvements in intervention and control groups for QoL measures, for example, Chaplin et al.30 As such, it could be hypothesised that attending a specialist respiratory assessment and being part of a research study could increase the likelihood of patients seeking information about, and take a more active role in, self-management of their COPD (including increased confidence to undertake physical activity or training).14 31 Conducting exercise tests as part of this assessment would have further increased confidence to undertake physical activity or training and as such were not included in the baseline assessment for control group participants.32
Patient activation (defined as patients’ knowledge, skills and self-efficacy regarding self-management33) is shown to play a central role in COPD self-management behaviours and is a central component in the Chronic Illness Care Mode.34 It is important to help patients put knowledge and skills into practice in daily life rather than simply telling them what they need to do35—we went some way to doing this with the format of the group sessions. Goal setting was carried out between sessions that were gradually spaced further apart so that participants were implementing these goals in their daily lives for longer, still with the promise of feedback to HCPs on returning to a group session. However, qualitative feedback suggests that 6 weeks may have been too long and that 4 weeks may have been more suitable. In the intervention group, PAM scores increased on average by almost five points, similar to findings in other self-management studies.36 37 Despite this manuscript describing a lighter touch intervention. This is an important finding as activated patients are more likely to report improved health-related behaviours and clinical outcomes, and partake in collaborative decision-making with HCPs.38 39 Furthermore, each point increase in PAM score correlates to a 2% decrease in hospitalisation and 2% increase in medication adherence.40 Therefore, these data indicate that the intervention has the potential to reduce healthcare use.
Disease-specific knowledge increased postintervention supporting the effect of the intervention and at 3 months post intervention, this knowledge was retained (slight increase in scores between 6 and 9 months in both groups). Reduction of disease-specific knowledge in the months following the completion of SMP and rehabilitation programmes is a common finding,41 therefore, we were encouraged to see this outcome maintained at 9 months. New international guidelines could offer some guidance when designing the education component of self-management and rehabilitation programmes in the future.42
Strengths and limitations
Offering a community-based programme, at venues and times more suitable for participants, went some way to remove common barriers to attendance. A high number of intervention participants could be classed as completers of the intervention (mean number of group sessions attended was 3.88 and 62.5% completed four or more sessions)—this, alongside qualitative findings, seems to indicate that conducting sessions in the community, local to the participant, at times suitable to them, better enabled participants to engage with and complete the SMP. It is hard to assess if the adherence rates to the intervention in this study are comparable to that of one-to-one sessions in Mitchell et al14 as this was not measured. However, both studies had high completion for the 6 month assessments from participants in the intervention groups (Mitchell et al14 80%, this study 83%). Our inclusion criteria allowed for recruitment of a wide range of participants, not just those who would usually be suitable for PR. Indeed, the median MRC of our recruited population was grade 2. This group is often excluded from PR programmes.28 The intervention was underpinned by social cognitive theory43 and motivational interviewing techniques.44 It also included other techniques such as goal setting and solution-focused goal feedback that have been shown to be effective in modifying behaviour. Further, it was delivered at an intensity that was possible to incorporate into routine practice. The way in which the group sessions were delivered maximised support from/contact with an HCP and allowed for rapport to develop between participants and HCPs in the initial stages of the intervention, prior to longer breaks between sessions.
For some intervention participants, distance from group venues was a problem, causing withdrawal from the study. This is because they may have had to attend sessions that were outside of their local area as we were recruiting in multiple areas at the same time. For the same reason, other participants were waiting up to a month for group sessions to start. Future studies may wish to consider cluster randomisation over individual participant randomisation to avoid these issues. In practice, this would occur naturally as GP would most likely run SMPs for their patients, ensuring a venue that is suitable for all. While group-based interventions have some advantages in terms of peer-support and likely cost savings; some patients dislike group formats. Also, this study was conducted prior to the start of the COVID-19 pandemic which limited in-person group-based interventions. Future implementation work therefore may need to consider these factors. It is likely that a choice of formats (eg, one to one, group-based, in-person, remote) would help to improve uptake16 and engagement from both patients receiving the intervention and services providing this.
Results suggest that the CAT may not have been the most suitable primary outcome measure for patients with milder disease.8 It may be that a general self-management measure (eg, HEI-Q45) or the PAM are more suitable. These would also measure the important behaviour change aspects of the SMP.46 While we have not compared the outcomes from this study to those delivering the SPACE for COPD intervention on a one to one basis; we were able to show comparable changes in the CRQ-dyspnoea domain (the primary outcome in the Mitchell et al study14) at 6 months in the intervention groups: 0.5 in the current study and 0.66 when delivered 1:1, both meeting the MCID. The Mitchell et al study did not measure the CAT.
Qualitative results indicate acceptability of the intervention on behalf of the patients’ taking part and the HCPs delivering the sessions. Although the focus groups were only completed in those available at the end of the intervention period, all patients were invited to take part regardless of the number of sessions they attended in total. Despite the qualitative results suggesting that the intervention was acceptable, there were a large number of participants who did not respond to the study invitation (81.5%) and a further 36% who declined to take part. Unfortunately, a number of participants were also withdrawn by the study team that fell within the intervention arm of the study. Although the study was powered for the CAT at 6 months, recruitment was uneven between groups. Reasons for withdrawal were not related to the intervention in the vast majority of cases—many were ineligible (did not have a diagnosis of COPD—as a consequence, the sample size was reassessed and additional participants recruited.) For those who were eligible, social problems and other health problems were often cited as reasons for withdrawal. In many cases participants withdrew from the study before commencing the intervention.
Future implications
The importance of self-management is widely acknowledged in people living with COPD3–5 and opportunities should be maximised from the time of diagnosis through to more severe disease.47 However, there is currently no provision for a structured supported SMP in the UK for those with milder disease. Although mild disease was not an eligibility criterion for this study, we did primarily recruit those in GOLD stages I and II with a median MRC grade if 2. SPACE for COPD as a group-based community situated intervention could therefore be offered to newly diagnosed patients with COPD, with less severe problems and those with capacity to manage their disease, to bridge the gap between diagnosis and offering of PR. For those patients with more severe disease, and may have comorbidities, PR would assume greater importance.47 This prevention model has only recently been adopted in COPD, with calls for interventions to reduce risk in people with early disease48 and potential for considerable health and health service gains if we could facilitate self-management support in patients with early disease and slow their decline.49 In order to establish whether this is possible, long-term follow-up studies are required.
Opportunities to improve self-management skills should also be embedded in PR programmes. In the future, there may be an opportunity to explore the value of the SPACE for COPD programme alongside rehabilitation, or indeed, an alternative for those unwilling or unable to attend. Currently the programme is also being tested as a group based intervention for those who have recently completed PR as a maintenance tool.50 The SPACE for COPD group-based SMP offers patients a choice which may be more convenient for those who may still be working and unable to commit to traditional PR, or for those struggling to travel and are only able to travel in the local area. The nature of the model also allows for patients to access specialist teams for a longer period of time but also encourages the group to meet outside of the scheduled sessions, creating in effect a local COPD community with shared interests. In future, a more intense version of the programme may be warranted to increase gains in the outcomes of interest.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the Hampshire B Research Ethics Committee (REC reference: 14/SC/1169). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the CERS research team, COPD Nursing Team and clinical pulmonary rehabilitation team at the University Hospitals of Leicester who assisted with the study. To Stacey Chantrell who conducted the qualitative focus groups. In addition, thanks go to the community respiratory teams who delivered the intervention at East Leicestershire CCG: Sue Price; Leicestershire Partnership Trust: Karen Moore, Alex Woodward and Gillian Doe; West Leicestershire CCG: Jake Cooke; our Public Involvement group: Patricia Overty and Freda Smart.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LH-W and CB were involved in the development of the intervention, the design and delivery of the trial. CB, PP, LH-W, JB and SS have been involved in drafting the work or revising it critically for important intellectual content and have given the final approval of the version published. JB completed the data analysis. SS is the principal investigator of the study and guarantor of the work.
Funding The research was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East Midlands (CLAHRC EM, now ARC EM) and took place at the University Hospitals of Leicester NHS Trust. Support was also provided by the NIHR Leicester Biomedical Research Centre-Respiratory.
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The funder employed staff to work on the project but had no role in the analysis, interpretation or reporting of the results.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.