Article Text

Abstract
Introduction Patients with interstitial lung disease (ILD) are known to develop an acute exacerbation (AE) after surgery. Previous studies have evaluated the predictors of postoperative AE. However, it remains unclear whether the results of those studies can be generalised to patients with different types of ILD and/or extrapolated to those who undergo non-pulmonary surgery. This study aimed to elucidate the predictors of the development of AE after surgery with general anaesthesia in patients with ILD.
Methods We conducted a nested matched case–control study of 700 patients from an initial cohort of 50 840 patients. We excluded those who underwent solid organ or bone marrow transplantation. The cases were patients with ILD who developed AE within 30 days postoperatively, whereas the controls did not develop AE. Each case (n=28) was matched with four controls (n=112) for sex, year of surgery and multiple operations within 30 days. Furthermore, a multivariable conditional logistic regression analysis was used to identify significant predictors, as indicated by a p value of <0.05.
Results After adjusting for potential confounders, the multivariable conditional logistic regression analysis identified honeycombing on CT (OR 3.09; 95% CI 1.07 to 8.92), a per cent predicted FVC <80% (OR 4.21; 95% CI 1.46 to 12.2) and an ARISCAT score ≥45 (OR 6.14; 95% CI 2.10 to 18.0) significantly associated with the development of postoperative AE.
Conclusions We found that the three factors were independent predictors for the development of postoperative AE in patients with ILD. These predictors are advantageous because they can be readily evaluated before surgery by surgeons and anaesthesiologists even without consulting experienced pulmonologists.
- interstitial fibrosis
- rare lung diseases
- thoracic surgery
- clinical epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What are the predictors of the development of acute exacerbation after surgery with general anaesthesia in patients with interstitial lung disease?
We identified honeycombing on CT, a per cent predicted FVC <80% and an ARISCAT score ≥45 as predictors.
All three predictors can be evaluated by surgeons and anaesthesiologists even without consulting experienced pulmonologists.
Introduction
Patients with interstitial lung diseases (ILDs), including idiopathic interstitial pneumonias (IIPs), are at risk of an acute exacerbation (AE).1–5 Although rare, AE after surgery with general anaesthesia (ie, postoperative AE) may induce a fatal response.6 Accordingly, the ability to predict the likelihood of postoperative AE is crucial during the planning of surgery with general anaesthesia for patients with ILD.
Previous studies of patients with ILD who underwent pulmonary surgery have reported various risk factors for postoperative AE,7–9 among which a usual interstitial pneumonia (UIP) pattern on chest CT scan has been accepted as an important predictor.7 8 The risk factors were derived solely in patients with IIPs who underwent pulmonary surgery (eg, surgery for lung cancer), whereas very few studies have evaluated the risk factors for postoperative AE in patients undergoing non-pulmonary surgery.10 In addition, there were no reports that showed the risk factors for postoperative AE in patients with ILD who underwent surgery that included non-pulmonary surgery (ie, abdominal surgery).
However, interobserver agreement about the UIP pattern on CT was reportedly low.11 Accordingly, more reproducible and consistent radiological criteria are needed.
In this study, we aimed to evaluate whether honeycombing on CT as well as other potential predictors that can be generally obtained preoperatively may be applicable to the prediction of postoperative AE risk in patients with various types of ILD who plan to undergo pulmonary or non-pulmonary surgery. In addition, we developed the risk index of postoperative AE by combining the potential predictors.
Methods
Design, setting and ethical considerations
This study featured a nested matched case–control design and was conducted at a single centre. From an institutional anaesthesia database, we used a patient cohort including nearly all patients who underwent surgery with general anaesthesia at the University of Tokyo Hospital between January 2009 and December 2017. A cumulative total of 50 840 patients who underwent various types of operations were identified. Informed consent was obtained using an opt-out method on the hospital website.
Participants
We conducted a search of the electronic medical records of patients in the cohort to identify those with pre-existing ILD at the time of operations. We included patients with IIPs, connective tissue disease-related ILDs (CTD-ILDs), ILDs of iatrogenic causes (eg, drug toxicity, radiation), hypersensitivity pneumonitis and pneumoconiosis in this study. We did not include patients with sarcoidosis, cystic lung diseases (eg, lymphangioleiomyomatosis and pulmonary Langerhans cell histiocytosis), or transfusion-related acute lung injury. We additionally excluded patients younger than 18 years of age and those who were undergoing solid organ or bone marrow transplantation.
Furthermore, in this study, we evaluated the occurrence of AEs within 30 postoperative days. According to the ATS/ERS/JRS/ALAT statement, we defined AE as (1) a worsening of dyspnoea within 1 month with (2) evidence of hypoxemia and (3) new radiographic alveolar infiltrates, and (4) the absence of an alternative explanation such as infection, pulmonary embolism, pneumothorax or heart failure.12 The preoperative and postoperative CT images of four representative patients with AE are presented in online supplemental figure S1 and legend.
Supplemental material
The cases and controls in this study were patients with ILD who did and did not develop AE within 30 postoperative days, respectively. Multiple operations within 30 days were considered a single course of surgery, and only the 30-day period after the last operation was evaluated. Two or more operations on the same patient were considered individual surgeries when performed at an interval >30 days. We adopted a case–control matching design in which each AE case was matched with four non-AE controls according to sex, year of surgery (ie, 2009–2011, 2012–2014, 2015–2017) and multiple operations within 30 days; the latter was included to control for the possibility that repeated operations on the same patient might increase the risk of postoperative AE.13
Patient and public involvement
Patients and the public were not involved in the design and conduct of this study, choice of outcome measures, nor recruitment. The results of this study will not be disseminated to the participants and linked communities.
Variables
We evaluated the following variables: sex; age; height; weight; body mass index; smoking status; presence of IIPs, CTD-ILDs, bronchial asthma or chronic obstructive pulmonary disease (COPD); preoperative steroid use; respiratory infection in the last month prior to surgery; preoperative oxygen saturation as measured by pulse oximetry (SpO2); honeycombing on CT; spirometry results, including the per cent predicted FVC and FEV1/FVC; results of preoperative blood tests, namely the haemoglobin (Hb), serum lactate dehydrogenase (LD), serum C reactive protein (CRP) and serum KL-6 levels; year of surgery; surgical site; the American Society of Anesthesiologists physical status (ASA-PS)14; emergency or elective surgery; surgery duration; the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score15; intraoperative blood transfusion; multiple operations within 30 days.
In this study, honeycombing on CT was defined as thick-walled cystic spaces with similar diameters of 3–5 mm (although occasionally up to 25 mm) that comprised several stacked layers of cysts, or a single subpleural layer of three or more contiguous cysts.16 For this study, we included the latest results recorded within 90 days prior to surgery. Reference values for FVC were calculated using the LMS (lambda, mu, sigma) method for the per cent predicted FVC.17 In accordance with previous studies, a cut-off value of 80% for the per cent predicted FVC was used to categorise patients into two groups.18 19 Meanwhile, an FEV1/FVC cut-off value of 0.70 was set according to the GOLD criteria for COPD.20
The ARISCAT score was determined using the following seven factors: age category, preoperative SpO2 category, respiratory infection in the last month, preoperative anaemia, surgical site category, emergency surgery and surgery duration category.15 Patients were categorised into three subgroups each according to age, preoperative SpO2, surgical site and surgery duration. Preoperative anaemia was defined as an Hb level ≤10 g/dL.15 Patients who required oxygen supplementation at rest in our study were considered equivalent to those with an SpO2 ≤90% under room air in the original ARISCAT scoring study. The scores of each of the seven factors were summed to yield the ARISCAT total scores, which were classified into the following three categories: low, <26; intermediate, 26–44; high, ≥45.15
For this study, we used data from the latest blood analyses within 7 days prior to surgery to determine the Hb, LD and CRP levels and the data obtained within 60 days prior to surgery to determine the KL-6 level. Data recorded outside of these limits were regarded as missing. Based on a previous study of postoperative AE, we used a KL-6 cut-off value of 1000 U/mL, which is twice the upper limit of the normal range.7 The cut-off values for LD and CRP were the respective upper limits of the normal ranges (222 IU/L and 0.3 mg/dL).
Multiple imputation
To account for bias caused by missing data, we used a multiple imputation method21 to address the missing per cent predicted FVC, FEV1/FVC and KL-6 values. During the imputation process, the following 22 variables were used to estimate missing data assumed to be ‘missing at random’: postoperative AE; per cent predicted FVC; FEV1/FVC; KL-6; sex; age; height; weight; body mass index; bronchial asthma; COPD; respiratory infection in the last month; oxygen supplementation at rest; honeycombing on CT; LD; CRP; year of surgery; pulmonary surgery; ASA-PS; emergency surgery; ARISCAT total score; multiple operations within 30 days. Finally, we created 1000 multiple imputation datasets for the analysis, and combined the estimates and standard errors in accordance with Rubin’s rule.21
Statistics
Regarding the patient characteristics, we compared the continuous variables between cases and controls both before and after matching, using Student’s t-test and the Mann-Whitney U test as parametric and non-parametric tests, respectively. The continuous variables are presented as means with standard deviations or medians with interquartile ranges. For binary and categorical variables, associations with the response variable were evaluated using χ2 test or Fisher’s exact test.
After multiple imputation, a multivariable conditional logistic regression analysis was conducted to estimate the adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Binary or categorical variables that were significantly associated with postoperative AE in the univariate analyses of matched cases and controls were included as explanatory variables in the multivariable model. In addition, we conducted a sensitivity analysis of all patients without missing per cent predicted FVC and FEV1/FVC data.
Multicollinearity in the model was evaluated using generalised variance-inflation factor (GVIF).22 For categorical variables, we calculated GVIF(1/2df), in which df are the degrees of freedom of the variable.22 GVIF(1/2df) >2 indicated multicollinearity in the model.23 24
A receiver operating characteristic curve for the per cent predicted FVC was plotted and the area under the curve was measured. The Youden index25 was used to estimate the optimal cut-off value for the prediction of postoperative AE.
We further investigated the prevalence of the positive predictors in the original population before matching and used the Cochran-Mantel-Haenszel test to estimate the sensitivity and specificity of each cut-off value in the cumulative total number of positive predictors. We defined positive predictors as the independent variables that exhibited significantly positive associations with postoperative AE in the multivariable analysis after multiple imputation.
For all analyses, a p value of <0.05 was considered statistically significant. We adopted the Bonferroni adjustment to account for multiple comparisons in univariate analyses. All statistical analyses were conducted using R V.3.5.3 software with the “optmatch” 0.9-11, Multivariate Imputation by Chained Equations26 “mice” 3.4.0, “car” 3.0.2 and “pROC” 1.16.2 packages for matching, multiple imputation, multicollinearity and receiver operating characteristic curve, respectively.
Results
Patient recruitment
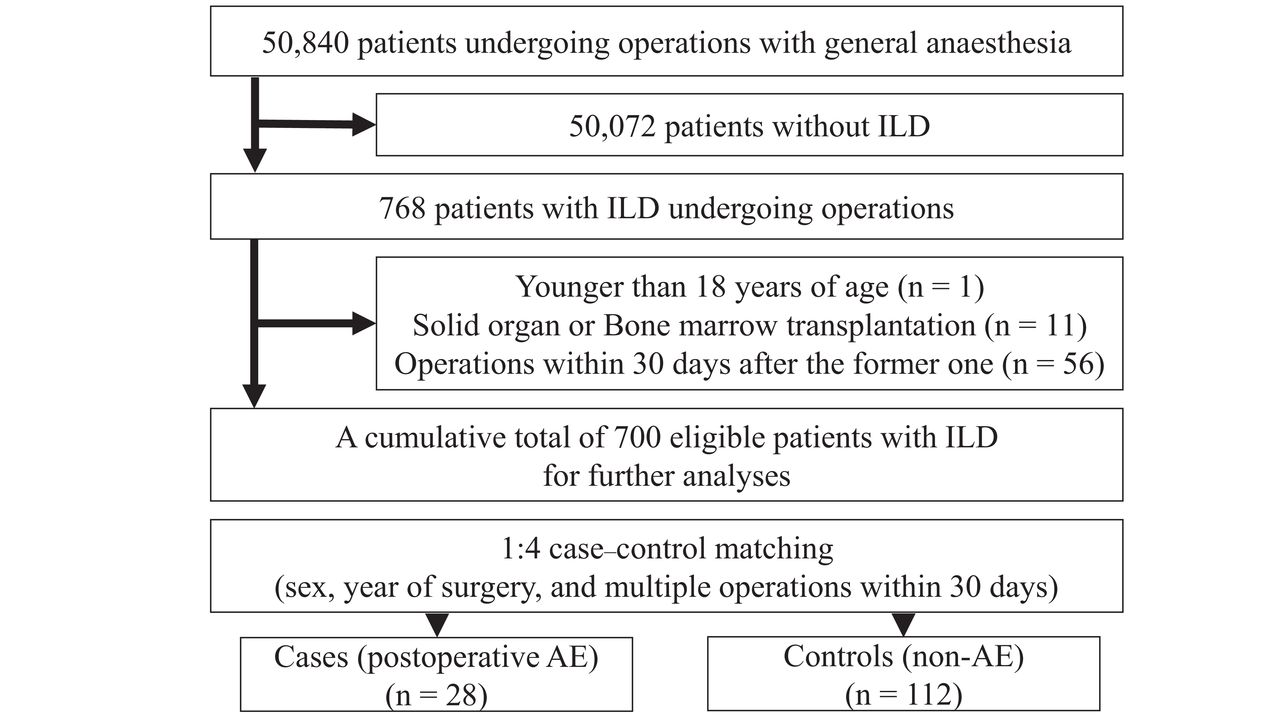
We identified a cumulative total of 768 patients with pre-existing ILD at the time of operations. After excluding a 7-year-old patient, 11 patients who underwent solid organ or bone marrow transplantation, and 56 patients who underwent secondary operations at an interval of less than 30 days after the previous operation, a total of 700 patients remained eligible for further analyses (figure 1).
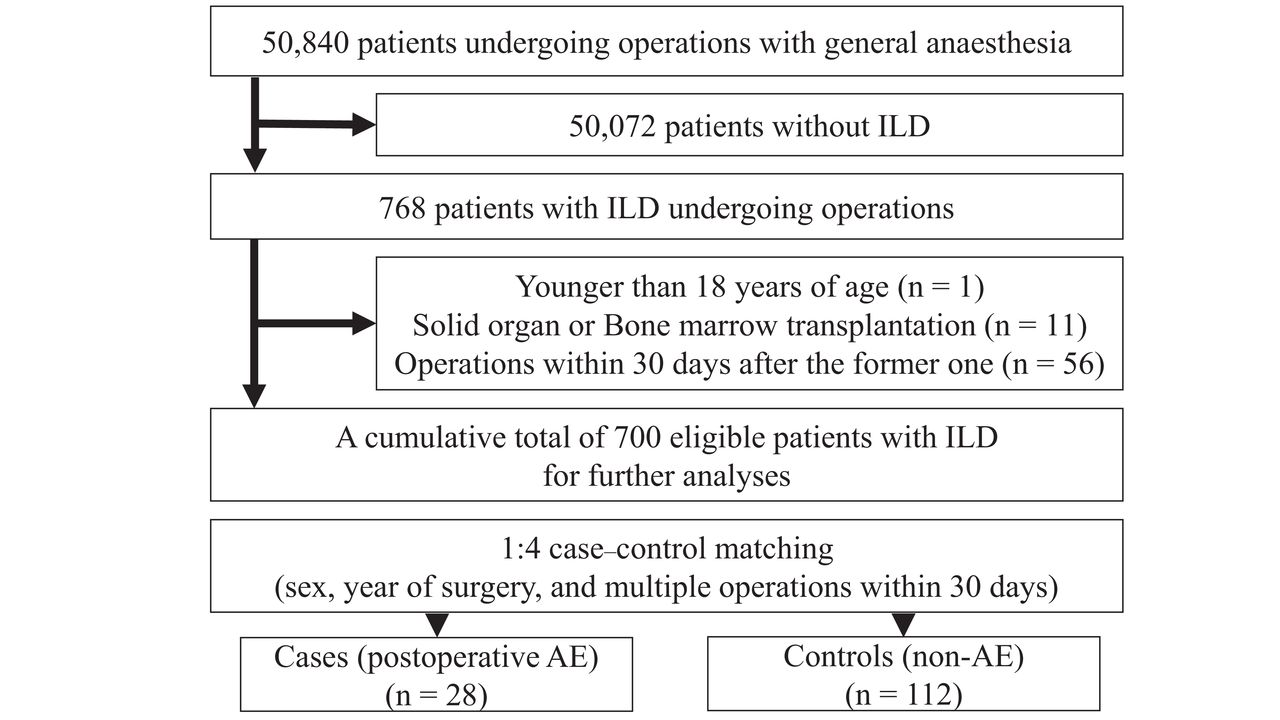
Flow diagram of patient recruitment. AE, acute exacerbation; ILD, interstitial lung disease.
Patient characteristics
Of the 700 patients with ILD, 59% had IIPs in this cohort (see online supplemental table S1). Further, 28 patients (4.0% of patients with ILD) developed postoperative AE, 11 of whom (39% of patients with postoperative AE) died of AE during hospitalisation.
A total of 112 non-AE patients (controls) were matched with the 28 AE patients (cases). Table 1 (table 1a, table 1b, table 1c) presents the results of univariate analyses before and after matching. The numerical variables listed in online supplemental table S2 were used for case–control matching or multiple imputation and were transformed into binary or nominal variables as shown in table 1 (table 1a, table 1b, table 1c). Data were missing for the following three variables: per cent predicted FVC, FEV1/FVC and serum KL-6 (table 1b). Before and after one-to-four matching, the following five variables were significantly associated with postoperative AE in the univariate analyses: preoperative SpO2 category, honeycombing on CT, per cent predicted FVC category, surgical site category and ARISCAT score category (table 1b, table 1c).
Univariate analyses before and after one-to-four matching
Univariate analyses before and after one-to-four matching
Univariate analyses before and after one-to-four matching
Multivariable conditional logistic regression
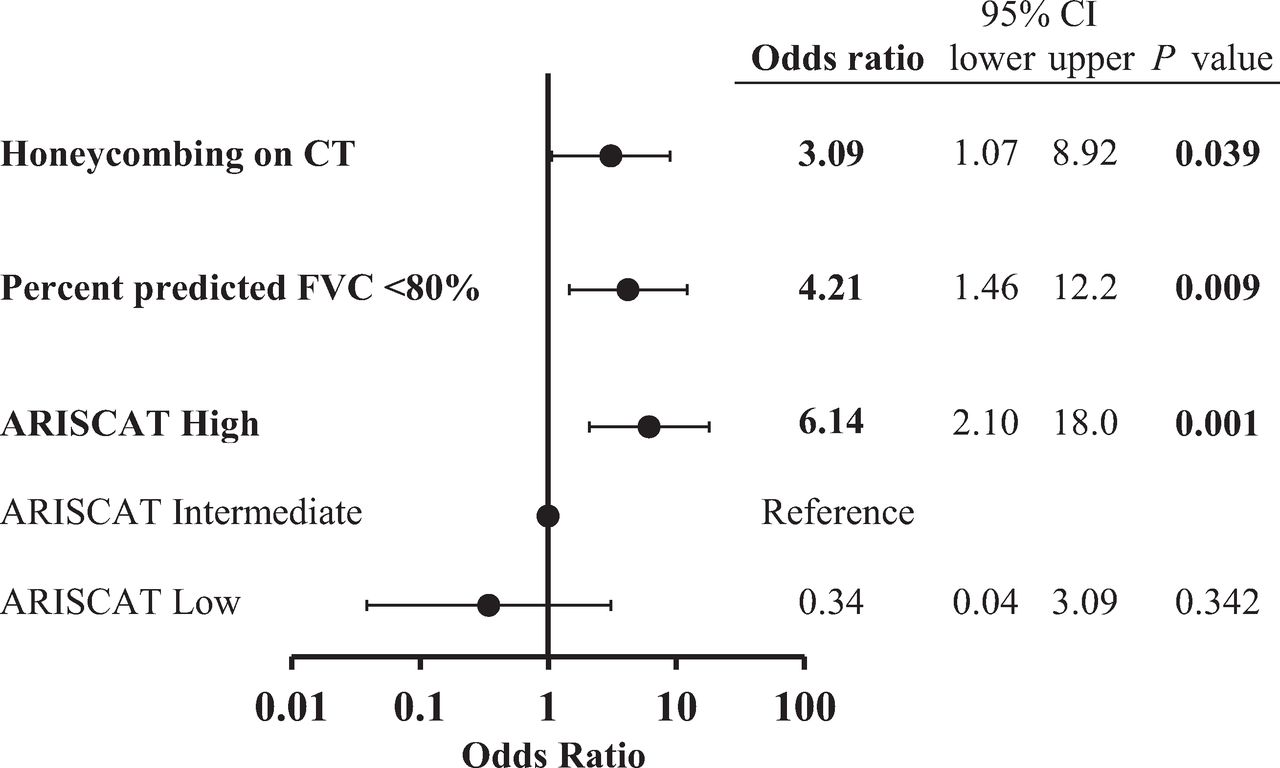
After multiple imputation, we included honeycombing on CT, the per cent predicted FVC category and the ARISCAT score category in our multivariable conditional logistic regression model. We excluded the other significantly different variables because these were components of the ARISCAT score. Subsequently, we determined three factors—honeycombing on CT, a per cent predicted FVC <80% and a high ARISCAT score (reference: intermediate)—to be significantly associated with postoperative AE, with respective adjusted ORs (95% CIs) of 3.09 (1.07 to 8.92; p=0.039), 4.21 (1.46 to 12.2; p=0.009) and 6.14 (2.10 to 18.0; p=0.001; figure 2). The sensitivity analysis yielded similar results (see online supplemental figure S2 and legend).
Supplemental material
{kind=link}
{kind=link}
Multivariable conditional logistic regression after multiple imputation. After one-to-four case–control matching for sex, year of surgery and multiple operations within 30 days, a multivariable conditional logistic regression model was performed using the following variables: honeycombing on CT, per cent predicted FVC <80%, and ARISCAT score category. The model was fitted following multiple imputation for missing values. A p value of <0.05 was considered statistically significant. ARISCAT score categories: low, <26; intermediate, 26–44; high, ≥45. ARISCAT, Assess Respiratory Risk in Surgical Patients in Catalonia; CI, confidence interval; FVC, forced vital capacity.
No multicollinearity was found in the independent variables included in the multivariable logistic regression model (online supplemental table S3).
The area under the receiver operating characteristic curve was 0.690 and the Youden index analysis revealed an optimal cut-off value of 79.58% for per cent predicted FVC (see online supplemental figure S3 and legend).
Supplemental material
We then combined these positive predictors into the Honeycombing-FVC-ARISCAT (H-F-A) index and calculated the cumulative total H-F-A index score for each patient in the unmatched population (see online supplemental table S4-A). We evaluated the probability of postoperative AE by counting the number of patients who received each H-F-A index score. A score cut-off value of ≥1 yielded a sensitivity for postoperative AE of 100% (online supplemental table S4-B).
Discussion
This nested matched case–control study investigated the predictors of postoperative AE in patients with ILD. Notably, we identified honeycombing on CT, a per cent predicted FVC <80% and an ARISCAT score ≥45 as factors significantly associated with the development of postoperative AE. All three of these factors are advantageous because they can be readily evaluated before surgery by surgeons and anaesthesiologists even without experienced pulmonologists. Each component of the ARISCAT score can be easily determined, and spirometry and chest CT data are generally available for most patients with ILD.
Moreover, our newly defined H-F-A index (shown in online supplemental table S4) may enable patients with ILD to understand their potential risk of postoperative AE, although this index score needs to be validated through external studies. We determined that no patient in the original population with an H-F-A index score of zero developed postoperative AE.
The prediction of postoperative AE based on the diagnosis of UIP patterns may be limited by interobserver disagreement. This process is further complicated by the recently amended classification of UIP patterns on high-resolution CT.27 In contrast, honeycombing on CT, a typical feature of UIP, enables a simpler interpretation of chest CT findings in patients with ILD. Specifically, the observation of a single subpleural layer comprising at least three contiguous cysts on a lung CT image meets the definition of radiological honeycombing16 (eg, online supplemental figure S1-A). In our study, patients with non-IIPs accounted for 93 of the 267 patients who presented with honeycombing on CT (35%). To simplify the radiological analysis, we did not distinguish honeycombing from the similar and difficult-to-distinguish feature of peripheral traction bronchiectasis in subpleural areas,28 as both are recognised as typical CT features of UIP.27 Based on our observations, we believe that honeycombing on CT could enable non-pulmonologists to predict surgical risks in patients with ILD.
For the cut-off value of per cent predicted FVC, we used 80% based on previous studies.18 19 The estimated ORs and 95% CIs using an optimal cut-off value of 79.58%, which was derived from the receiver operating characteristic curve to predict postoperative AE with per cent predicted FVC in our study, were the same as those using a cut-off value of 80% (data not shown). The GAP (gender–age–physiology) model includes the per cent predicted diffusing capacity of lung for carbon monoxide (DLCO) in addition to FVC,29 and both the FVC and DLCO have been reported to reflect the extent of parenchymal abnormalities.30 However, we could not assess the role of DLCO because this parameter does not seem to be a routine preoperative test in many hospitals and was missing for 483 of the 700 eligible patients (69%) in our study.
The ARISCAT score has been validated for the prediction of postoperative pulmonary complications in European cohorts.31 32 However, to the best of our knowledge, no study has reported that an ARISCAT score ≥45 is a significant predictor of postoperative AE. Our study therefore suggests that the ARISCAT score may be useful for predicting AE, as well as other postoperative pulmonary complications.
Our study was limited by the following aspects. First, we did not classify the ILDs through multidisciplinary discussions. Second, we were unable to interview each patient to determine their histories of AE and operations at other hospitals. Therefore, our analysis was based solely on medical records. Third, retrospective observational studies may be biased by undetermined confounders. Finally, this study was conducted at a single centre. A larger prospective multi-centre study of postoperative AE should be conducted to confirm our findings.
In summary, we conducted a nested matched case–control study and identified honeycombing on CT, a decreased FVC, and a high ARISCAT score as significant predictors of postoperative AE in patients with ILD. Given the clinical challenge of clearly distinguishing IIPs from non-IIPs, these three predictors, which are applicable to both IIPs and non-IIPs, are advantageous because they can be readily evaluated before surgery by surgeons and anaesthesiologists even without consulting experienced pulmonologists.
Acknowledgments
We would like to thank Shinichiroh Yokota, Satoshi Kasai and Youichirou Kitagawa for their cooperation in data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KH and TJ had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse effects. YM, HU, KS, GK, KU and TN substantially contributed to the study design, data analysis and interpretation, and the writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KU reports grants from Nihon Kohden Corporation, grants from Nipro Medical Corporation, outside the submitted work. The other authors have no conflict of interest with any companies and/or organisations whose products or services may be discussed in this study.
Patient consent for publication Not required.
Ethics approval This study was approved by the Institutional Review Board of the Graduate School of Medicine at the University of Tokyo (from 27 October 2008; IRB# 2203-(7)) and conducted in accordance with the amended Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.