Article Text

Abstract
Introduction The previous data concerning the prevalence of idiopathic pulmonary fibrosis (IPF) and the frequency of antifibrotic drug use in Finland were based on research registries and medical records whereas nationwide data on the number of patients with IPF in specialised care and those on antifibrotic treatment have not been published.
Methods We made an information request to the Finnish National Hospital Discharge Register (Hilmo) covering the whole population of Finland to find out the annual numbers of patients with IPF treated in specialised care in 2016–2021. The numbers of the patients initiating and using pirfenidone and nintedanib were requested from the Social Insurance Institution of Finland (Kela) for the same time period.
Results The estimated prevalence of IPF in specialised care was 36.0 per 100 000 in 2021, having increased since 2016. The number of antifibrotic drug users and their proportion of outpatients with IPF had also risen during the follow-up period. In 2021, 35% of the patients with IPF used pirfenidone or nintedanib. The number of inpatients treated in specialised care because of IPF had declined during 2016−2021.
Conclusions The prevalence of IPF was higher than expected in Finnish specialised care and had increased during the 6-year follow-up time. The increase in the number of patients with IPF using antifibrotic drugs might have diminished the need for IPF-related hospitalisations.
- rare lung diseases
- interstitial fibrosis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Antifibrotic drugs pirfenidone and nintedanib have increased the life expectancy of patients with idiopathic pulmonary fibrosis (IPF). The prevalence of IPF and antifibrotic drug use have been highly variable in previous studies, which are often based on research registries and cohorts, and seldom on nationwide data.
WHAT THIS STUDY ADDS
Based on comprehensive national register data, the prevalence of IPF in specialised care in Finland was higher than expected and had risen during the 6-year follow-up period from 2016 on. Simultaneously, the number of antifibrotic drug users had increased and the number of hospitalisations caused by IPF had declined.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The results suggest that antifibrotic drugs might have decreased the number of IPF-related hospitalisations and increased the life expectancy of patients with IPF, which supports the use of antifibrotic drugs in patients with IPF.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a progressive disease which impairs the quality of life and reduces life expectancy.1–3 Acute exacerbations of IPF (AE-IPF) make the disease course unpredictable and are responsible for a large proportion of hospitalisations and premature deaths of patients with IPF.4 5 The antifibrotic drugs pirfenidone and nintedanib are efficient in slowing down the progression of the disease and have also increased life expectancy in real-world study settings.6–13 However, according to the data based on IPF registries, 25%–77% of patients with IPF do not receive antifibrotic drug treatment.8 9 11 12 14–16 Although research registries of patients with IPF are useful in collecting real-life information related to IPF, the registries may dispose to selection bias and lack generalisability.
The estimated prevalence of IPF based on medical records or health claim data tends to be higher than in studies based on data from IPF registries.17 18 In a Finnish investigation in which the data were collected from medical records, the estimated prevalence for IPF was 16−18/100 000, compared with the prevalence of 8.6/100 000 reported in another study based on Finnish IPF registry data.19 20
The proportion of antifibrotic drug users of all patients with IPF has been higher in IPF registries than in studies based on nationwide data. Less than 10% of the patients with IPF used antifibrotic drugs in a study where the data had been gathered from Swedish population-based registers and electronic medical records, whereas according to the report based on the Swedish IPF registry, the proportion was much higher, namely 54%.9 21 An American study that used data on privately insured and Medicare Advantage beneficiaries revealed that 26.4% of patients with IPF had started antifibrotic medication, whereas the proportion was 49% in the American IPF-PRO registry.15 22 There are no earlier studies evaluating nationwide epidemiological data on IPF in relation to IPF-related hospital treatment periods and antifibrotic drug use.
Finnish healthcare services, which are further described in online supplemental material and in a previous publication by the WHO,23 form a single entity, so that settings are favourable for collecting national data on diseases. Finnish patients with interstitial lung disease (ILD) are treated in specialised care in either central or university hospitals by respiratory physicians. There are no specific ILD centres in Finland; however, each university hospital provides tertiary services in the form of multidisciplinary meetings on ILDs for central hospitals located in their catchment areas. The utilisation of multidisciplinary discussions in the diagnostics of ILDs is a routine practice in all university hospital districts in Finland. Antifibrotic drugs pirfenidone and nintedanib are offered to patients with IPF who meet reimbursement criteria of the Social Insurance Institution of Finland (Kela). These criteria are described in detail in online supplemental material.
Supplemental material
The aim of the study was to find out the annual numbers of patients with IPF in Finnish specialised care recorded with the International Classification of Diseases version 10 (ICD-10) diagnosis code J84.1 from the years 2016 to 2021. Another aim was to study the numbers of antifibrotic drug users in Finland during the past 6 years and to compare the number of pirfenidone or nintedanib users with the number of outpatients and inpatients with IPF in Finnish specialised care. We also wanted to compare these parameters between the five university hospital districts and find out the temporal development in the numbers between 2016 and 2021.
Methods
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Study design
The data for this study were requested from two national sources, namely the Finnish Hospital Discharge Register (Hilmo) and Social Insurance Institution of Finland (Kela). Hilmo, provided by the Finnish Institution of Health and Welfare, includes information on the numbers of patients and their treatment periods either in outpatient clinics or in hospital wards of specialised care where practically all patients with IPF are diagnosed and treated. The Hilmo register data cover the whole population of Finland, and the quality of the register data has been good in earlier studies.24 Kela has its own statistical information service regarding Kela’s benefits, such as medical reimbursement and purchases of medicines.
We made an information request to Hilmo on patients whose first recorded diagnosis code was J84.1. We assumed that the majority of the patients with J84.1 diagnosis code suffered from IPF, and thus, we have used the term IPF when referring to the patients with this diagnosis code. We requested information on the annual numbers of patients with IPF in outpatient clinics or hospital wards in Finnish specialised care according to the five university hospital districts covering all of Finland in 2016–2021.
Another information request was made to Kela to find out the users and initiators of pirfenidone or nintedanib in each university hospital district per year in 2016–2021. Further details on the reimbursement criteria for antifibrotic drugs in Finland are presented in online supplemental material. The data from Kela were based on the numbers of persons who had been prescribed antifibrotic drugs and who had purchased them at least once during the year under review. The specific ATC codes for antifibrotic drugs were used in the search for Kela data, namely L04AX05 for pirfenidone, and L01XE31 or L01X09 (since 2021) for nintedanib.
The demographic data of continental Finland and each university hospital district were received from an open database of Statistics of Finland (online supplemental E-Table 1).25 Åland, the smallest region and hospital district in Finland, located in an archipelago in the Baltic Sea, was excluded from the data because of the small population (about 30 000 inhabitants) and very low number of IPF cases and antifibrotic drug users (less than five per year).
Statistical analysis
The statistical analysis was made with SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, V.27.0. Armonk, New York: IBM Corp) and OriginPro was used for graphs (V.2022. OriginLab Corporation, Northampton, Massachusetts, USA). The prevalence of IPF was estimated by using demographic data as denominators. Prevalence was reported as the number of cases per 100 000 persons.
Ethical issues
The requested register data were anonymous and did not include identifying information. The study was implemented in accordance with Finnish and EU data privacy legislations.
Results
Numbers of patients with IPF in specialised care and antifibrotic drug users in Finland
The annual numbers of outpatients, inpatients with IPF and users of antifibrotic drugs are presented in figure 1, online supplemental E-Tables 2 and 3. The total number of outpatients with IPF had increased during the past 6 years, from 1695 patients to 1986 patients, whereas the number of inpatients had decreased from 375 to 331 patients.

The trends in the numbers of antifibrotic drug users, idiopathic pulmonary fibrosis outpatients and inpatients in Finnish specialised care between 2016 and 2021. IPF, idiopathic pulmonary fibrosis.
The estimated prevalence of IPF in specialised care had increased from 31.0 per 100 000 in 2016 to 36.0 per 100 000 in 2021. In 2021, the highest prevalence was seen in Oulu University Hospital (OUH) District (60.7/100 000) and the lowest in Helsinki University Hospital (HUH) District (32.0/100 000) (figure 2).
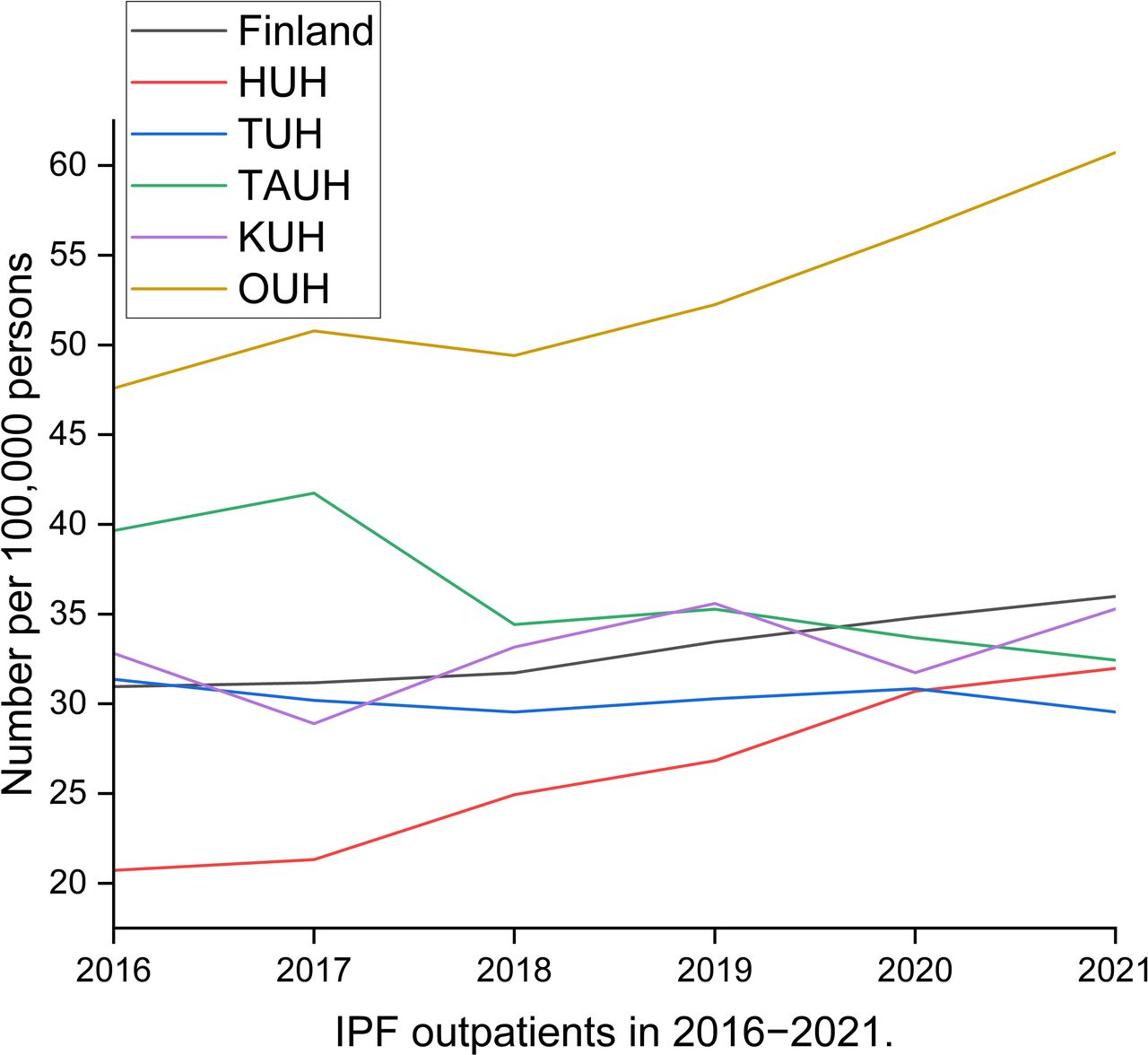
Idiopathic pulmonary fibrosis outpatients in Finnish specialised care according to university hospital district between 2016 and 2021. HUH, Helsinki University Hospital; IPF, idiopathic pulmonary fibrosis; KUH, Kuopio University Hospital; OUH, Oulu University Hospital; TAUH, Tampere University Hospital; TUH, Turku University Hospital.
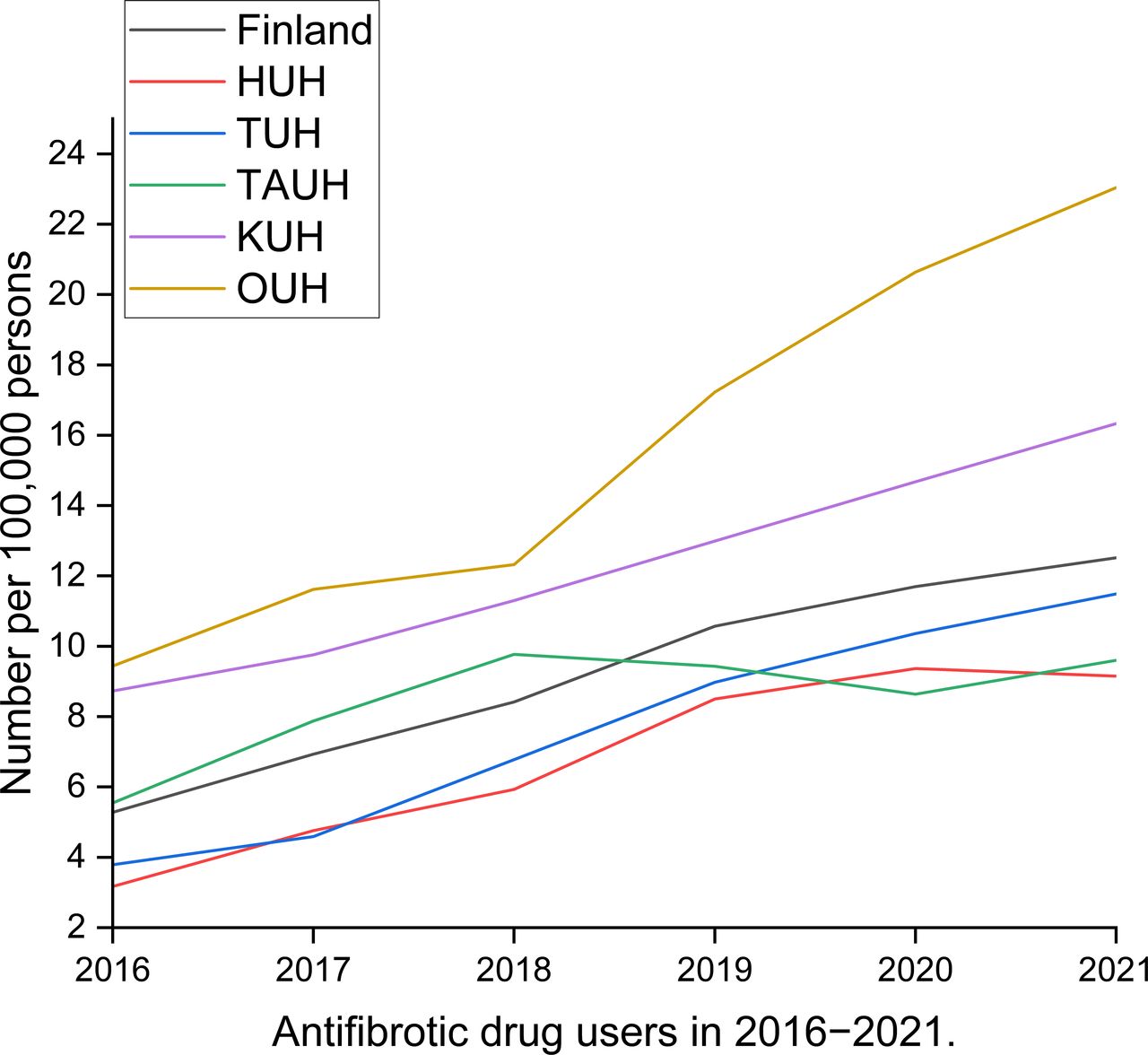
The number of antifibrotic drug users had increased year by year since 2016, but the annual number of persons initiating the use of antifibrotic drugs had remained stable in recent years (online supplemental E-Table 3). The prevalence of antifibrotic drug users in Finland was 12.5 per 100 000 in 2021. In 2021, the highest prevalence was found in OUH District (23.0 per 100 000) and the lowest in HUH District (9.2 per 100 000) (figure 3).

Idiopathic pulmonary fibrosis patients using antifibrotic drugs in Finland according to university hospital district between 2016 and 2021. HUH, Helsinki University Hospital; KUH, Kuopio University Hospital; OUH, Oulu University Hospital; TAUH, Tampere University Hospital; TUH, Turku University Hospital.
The antifibrotic drug users in relation to the numbers of patients with IPF
There was a clear increasing trend in the proportion of antifibrotic drug users in relation to the total number of outpatients with IPF between 2016 and 2021 in Finland (figure 4). Although the prevalence of antifibrotic drug users was highest in OUH District compared with other areas, the proportion of antifibrotic drug users of the total number of outpatients with IPF was near the mean value of Finland in 2021 (38% vs 35%, correspondingly). The number of antifibrotic medication users in relation to the number of outpatients with IPF was highest in Kuopio University Hospital District (46%) and lowest in HUH District (29%) in 2021.

The proportion of antifibrotic drug users from idiopathic pulmonary fibrosis outpatients in Finnish specialised care between 2016 and 2021. HUH, Helsinki University Hospital; IPF, idiopathic pulmonary fibrosis; KUH, Kuopio University Hospital; OUH, Oulu University Hospital; TAUH, Tampere University Hospital; TUH, Turku University Hospital.
The prevalence of patients with IPF-related hospital treatment periods had a decreasing trend in most university hospital districts during the follow-up period (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Idiopathic pulmonary fibrosis inpatients in Finnish specialised care according to university hospital district between 2016 and 2021. HUH, Helsinki University Hospital; IPF, idiopathic pulmonary fibrosis; KUH, Kuopio University Hospital; OUH, Oulu University Hospital; TAUH, Tampere University Hospital; TUH, Turku University Hospital.
Discussion
We have introduced nationwide data on antifibrotic drug users and patients with IPF in Finnish specialised care. These data suggest an increasing prevalence of IPF and rising numbers of antifibrotic drug users during the past 6 years. However, despite the increasing number of outpatients with IPF, there was a decreasing trend in the number of patients with IPF-related hospitalisations.
In this study, the estimated national prevalence of IPF in specialised care was 36.0 per 100 000 in 2021 and it had increased year by year since 2016. In Finland, antifibrotic drugs were used only by patients with IPF when the registry data of this study were collected, because in 2016–2021, the Kela reimbursement for antifibrotic drugs was available only for patients with IPF, not for other types of fibrotic ILDs. Consequently, it can be assumed that the prevalence of patients with IPF must be more than 12.5 per 100 000 persons, which was the prevalence of antifibrotic drug users in Finland in 2021. Thus, the actual prevalence of IPF is higher than presented in a previous study based on Finnish IPF registry (8.6 per 100 000) and might be even higher than in the other earlier Finnish study, which reported a prevalence of 16–18 per 100 000.19 20
The estimated prevalence of IPF has also been variable in other previous studies, namely 3.3–45.1/100 000 worldwide and 3.3–25.1/100 000 in Europe.17 However, the data mentioned above were mostly picked up from IPF registries, which represent only selected populations of patients with IPF, not all of them. The results of the studies reporting the prevalence of IPF based on nationwide databases are well in line with our results showing that the prevalence of IPF was 27 per 100 000 in Japan and 23.4 per 100 000 in women and 39.7 per 100 000 in men in South Korea during the 3-year follow-up time.26 27
In the present study, the annual numbers of outpatients with IPF had increased in three hospital districts out of five during the past 6 years. Simultaneously, the number of antifibrotic drug users had risen year by year in four university hospital districts out of five. It can be speculated that the increase in the prevalence of patients with IPF is not due to a sudden growth in the incidence of IPF but rather a consequence of increased survival due to the use of antifibrotic treatment. This is also supported by the data on underlying causes of deaths provided by statistics of Finland since the annual number of deaths caused by ILDs (coded as J84) has not increased since 2016, when there were 352 deaths, compared with 308 deaths in 2020.28 There are several IPF registry studies demonstrating increased survival time of patients with IPF who use antifibrotic drug treatment, thus supporting the hypothesis of enhanced survival of Finnish patients with IPF, more than a third of whom use antifibrotic drug treatment.6 13 It is also possible that the general knowledge of fibrotic ILDs has improved, which may have increased the clinical suspicion of IPF and the number of cases in specialised care.
We were able to demonstrate a decreasing trend in the number of hospitalised patients with IPF in Finnish specialised care in 2016–2021 simultaneously with an increase in the number of antifibrotic drug users. In HUH district, where antifibrotic drug use was least common compared with other university hospital districts, this decreasing trend could not be observed. It is known that antifibrotic drug use diminishes the progression of IPF, and at least nintedanib has shown some efficacy in the prevention of AE-IPFs.6 7 29 30 AE-IPF or subacute progression of the disease seem to explain about 30%–65% of acute respiratory hospitalisations of patients with IPF.31–34 Mooney et al reported that treatment with antifibrotic drugs improved survival and reduced respiratory-related and all-cause hospitalisations of patients with IPF among Medicare beneficiaries with IPF in the USA.13 According to our results, it could also be speculated that the increase in the numbers of antifibrotic drug users has reduced the number of hospital treatment periods related to IPF during the past 6-year period. This is also supported by our earlier study, in which there were only a few antifibrotic drug users among those patients with IPF who had been hospitalised in North Ostrobothnia Hospital District because of acute respiratory symptoms in 2008–2019.34
To the best of our knowledge, there are no previously published studies presenting nationwide data on temporal development of the numbers of outpatients with IPF, inpatients with IPF and antifibrotic drug users from the years when the adoption of antifibrotic drugs has been in progress. Although the Finnish healthcare system has some unique features, Finnish patients with IPF have been very similar in terms of their clinical features and survival time when compared with patients with IPF from other countries, such as IPF registries in Sweden or Australia.9 11 12 Thus, our results may be generalisable to international patients with IPF as well. Some earlier studies have presented nationwide data on patients with IPF and the prevalence of antifibrotic drug use in the data.21 22 26 However, these studies lack the information on temporal development of these parameters and information on the number of hospital treatment periods. Our results suggest that in a national, unselected study population, the increasing use of antifibrotic drugs has had positive effects at the level of both individual patients and society as a whole in a relatively short time.
There were local differences in the prevalence of patients with IPF since in 2021, the prevalence of IPF in OUH District was 60.7 per 100 000 persons, whereas in HUH District, which covers about 40% of the population of Finland, the prevalence was 32.0 per 100 000. Because IPF is typically diagnosed in people over 60 years of age, the disease should be more prevalent in areas with an elderly population.35 The proportion of at least 65-year-old persons of population was smallest in HUH District compared with other university hospital districts, as seen in online supplemental E-Table 1. This explains partly the lower prevalence of IPF in HUH District compared with other university hospital districts, apart from OUH District, where the age distribution is at the level of the Finnish average. Other explanations for local differences in the prevalence of IPF might be related to the different practices in the use of ICD-10 diagnosis codes, overdiagnostics or underdiagnostics of IPF, and local genetic isolates that predispose to the development of IPF.
The proportion of antifibrotic drug users of all patients with IPF did not vary as much between the university hospital districts as the prevalence of IPF, being 29%–46%. Interestingly, the proportion of antifibrotic drug users of all patients with IPF in this nationwide study was higher, 35%, compared with an earlier Finnish investigation, where the proportion was 27%.12 The study mentioned above by Kaunisto et al12 was based on patients with IPF included in the Finnish IPF Registry during 2011–2015. Because pirfenidone has been available in Finland since 2013 and nintedanib since 2015, all patients in the study by Kaunisto et al could not be offered antifibrotic treatment, which might explain the discrepancies with our results. In IPF registry studies implemented in Germany, USA, Sweden, Central and Eastern Europe, Belgium and Luxembourg, the proportion of patients with IPF using antifibrotic drugs has been higher, namely 49%–69%.8 9 14–16 However, when comparing our results with Swedish or American nationwide data on patients with IPF, the use of antifibrotic drugs was relatively common among Finnish patients with IPF, because less than 10% of Swedish patients with IPF and 26% of American patients used antifibrotic drugs.21 22
There are several limitations of this study. First, the definition for IPF was based on ICD-10 diagnosis code J84.1 and thus, there might be non-IPF pulmonary fibrosis patients included in our material as well. The patients with IPF treated solely in primary care are not found in the Hilmo data, which, in turn, may cause some underestimation of the total numbers of patients with IPF. In Finland, end-of-life treatment is mainly implemented in primary care, so that those patients with IPF who have end-stage pulmonary fibrosis or some other serious disease(s) in terminal phase are not treated in specialised care. However, the data regarding antifibrotic drug use is very specific for IPF and reliable because of the strict medical imbursement criteria of Kela.
In conclusion, our results suggest that the use of antifibrotic drugs might have reduced the need for hospitalisations and increased the survival time of patients with IPF in Finland during the past 6 years. This finding further encourages to improve the diagnostic and treatment practices of IPF to be able to guarantee beneficial antifibrotic treatment for all patients with IPF eligible for treatment.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Authors would like to thank Anna Vuolteenaho for language assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JS made the data requests to Hilmo and Kela, analysed the data, prepared the first draft of the manuscript, prepared the graphs and submitted the study. All authors, JS, RK, UH and MP participated in the study design and in the interpretation of the data. RK managed the study and was responsible for funding aqcuisition. All authors commented on previous versions of the manuscript and read and approved the final manuscript. JS is the guarantor of the study, who accepts full responsibility for the work, had access to the data, and controlled the decision to publish.
Funding This work has been supported by a state subsidy of Oulu University Hospital, the Research Foundation of Pulmonary Diseases, Helsinki, Finland and the Research Foundation of North Finland.
Competing interests JS reports congress/travel costs from Boehringer Ingelheim, GlaxoSmithKline and Novartis Finland Oy, and lecturer’s fees from Chiesi, all outside the submitted work. MP reports personal lecture fee, congress travel cost and advisory board member Boehringer Ingelheim, lecture fee Roche, congress travel cost Orion Pharma, outside the submitted work. UH reports consulting and lecture fees from Johnson and Jonhnson and Boehringer Ingelheim, and congress travel cost from Chiesi and Roche. RK reports consulting and lecture fees from Boehringer Ingelheim, Roche and MSD, and virtual congress cost from Roche and Novartis.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.